

Subscribe to RSS
DOI: 10.1055/s-0045-1809423
Iodine-Negative Rare Gluteal Muscle Metastasis of Papillary Thyroid Cancer: Detected by 68Ga-DOTATATE PET/MRI and 18F-FDG PET/CT
Authors


Abstract
The case presents a 57-year-old male with metastatic papillary thyroid carcinoma (PTC) to the lymph nodes, lung, and mediastinum. Despite receiving multiple high-dose radioactive iodine (RAI) therapies, the patient's serum thyroglobulin levels continued to rise. The patient, who was unresponsive to RAI therapy, was being evaluated for suitability for 177Lu-DOTATATE therapy. Therefore, after the third high-dose treatment, simultaneous 68Ga-DOTATATE PET/MRI and 18F FDG PET/CT imaging were performed, revealing a painless mass in the left gluteal region. The gluteal mass was excised, and histopathology confirmed it as metastatic PTC. Muscle metastases are extremely rare for PTC. This case exemplifies the different levels of tumoral affinity shown by aggressive variants of PTC across three distinct imaging modalities: 68Ga-DOTATATE PET/MRI, 18F FDG PET/CT, and whole-body iodine scintigraphy.
Keywords
papillary thyroid carcinoma - gluteal muscles - RAI-refractory - 68Ga-DOTATATE PET/MRI - 18F-FDG PET/CTIntroduction
Papillary thyroid carcinoma (PTC) is the most common cancer of the thyroid gland.[1] While cervical lymph node metastasis appears more frequently, the rate of distant metastasis is low. Distant metastases frequently occur in the lungs and bones and to a lesser extent in brain and liver tissue.[2] In our case, we aimed to present a rare metastasis of PTC to the gluteal muscles.[3] [4]
Case Report
A 57-year-old male patient presented with complaints of neck swelling, shortness of breath, and difficulty swallowing. During his examinations, an approximately 5 cm solid nodule in the left thyroid lobe was found. Fine-needle aspiration biopsy suggested PTC, associated with pathological lymph nodes in the left cervical lymphatic stations. Consequently, he underwent a total thyroidectomy with central neck dissection and left modified lateral neck dissection. Histopathological examination revealed diffuse sclerosing variant papillary thyroid cancer with a partial tall cell variant in the left lobe, with the largest tumor size being 5 cm.
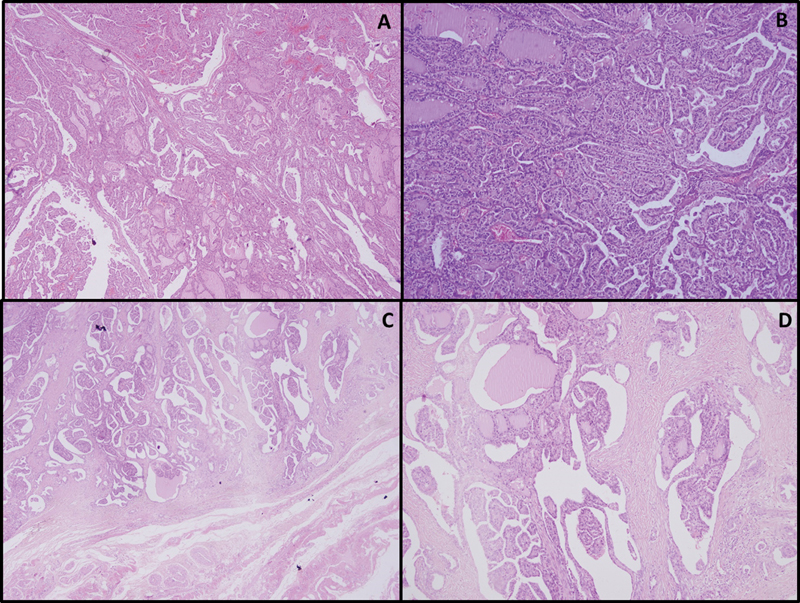
After the surgery, serum thyroglobulin (Tg) levels were above 500 ng/mL, suggesting distant metastasis. The patient received high-dose 131I therapy based on the aggressive histological subtype and radiological evidence of distant metastases, as per institutional practice. Radioiodine therapy was administered following recombinant human thyroid-stimulating hormone stimulation, in accordance with institutional protocol. Whole-body iodine scintigraphy performed after radioactive iodine (RAI) treatment showed intense increased activity of three foci in the bilateral thyroid beds and multiple masses in the mediastinum and lungs ([Fig. 1A, B]). RAI therapy with the same dose was repeated three times at 6-month intervals. A 68Ga-DOTATATE PET/MRI (positron emission tomography/magnetic resonance imaging) scan revealed a 7-cm soft tissue mass adjacent to the left gluteal muscle with moderate uptake ([Fig. 1C–E]). 18F-FDG PET/CT (computed tomography) images showed intense focal 18F-FDG uptake in the mediastinum (SUVmax: 6.6), lungs (SUVmax: 4.5), and the left gluteal muscle (SUVmax: 6.2; [Fig. 2A–C]). The soft tissue mass was excised. Histopathological findings were consistent with metastasis of primary PTC ([Fig. 3]). Immunohistochemical analysis confirmed Tg, TTF-1, and PAX8 positivity in the gluteal lesion, while PSA and PSAP were negative, supporting thyroidal origin and excluding a neuroendocrine neoplasm. The gluteal lesion showed no uptake on post-therapy 131I whole-body scintigraphy, despite being clearly visualized on both 68Ga-DOTATATE PET/MRI and 18F-FDG PET/CT. Combined with persistently elevated Tg levels, these findings fulfill the American Thyroid Association (ATA) 2015 criteria for RAI-refractory disease.


Discussion
This case stands out by illustrating a rare gluteal muscle metastasis of PTC, confirmed histopathologically and characterized through triple-imaging correlation. While RAI-refractoriness is a well-documented phenomenon in aggressive PTC variants, gluteal muscle involvement is exceedingly uncommon and poses significant diagnostic challenges.
The gluteal lesion was not visualized on post-therapy 131I whole-body scintigraphy, despite being clearly detected on both 68Ga-DOTATATE PET/MRI and 18F-FDG PET/CT. Persistently elevated Tg levels supported the diagnosis. According to the 2015 ATA guidelines, lack of iodine uptake in metastatic lesions with progression or biochemical activity confirms RAI-refractory disease.[5]
This case also offered a unique opportunity to compare three functional imaging modalities in a single patient. Notably, all metastatic lesions were visualized on 68Ga-DOTATATE PET/MRI, while both 131I-WBS and 18F-FDG PET/CT failed to capture all sites. Moreover, the degree of uptake varied between modalities, suggesting heterogeneity in somatostatin receptor expression and glucose metabolism. Such variability underscores the importance of complementary imaging strategies in patients with aggressive or atypical disease behavior.
PET/MRI was chosen over PET/CT for its superior soft-tissue contrast and lower radiation dose—especially relevant in a patient with prior cumulative high-dose RAI exposure. It provided both anatomical precision and functional insight, which were essential in delineating the infiltrative gluteal lesion extending from the gluteus medius toward the gluteus minimus.
Although skeletal muscle metastases from PTC have been previously described, gluteal muscle involvement remains a rare entity.[6] [7] Most reports focus on FDG PET/CT, while our case demonstrates the added diagnostic value of 68Ga-DOTATATE PET/MRI, particularly for anatomical clarity and lesion extent.
Almeida et al recently compared 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT in patients with TENIS (thyroglobulin-elevated negative iodine scintigraphy) syndrome under both suppressed and stimulated thyroid-stimulating hormone (TSH) conditions. They found DOTATATE PET/CT detected more locoregional and distant lymph node metastases regardless of TSH level, although stimulation led to decreased specificity.[8] In our case, DOTATATE PET/MRI performed under TSH suppression still demonstrated clinically significant uptake, reinforcing its potential value even in nonstimulated settings.
Furthermore, Binse et al demonstrated that 68Ga-DOTATOC PET/CT identified tumor lesions in 33% of patients with elevated Tg despite negative RAI and FDG scans—primarily in poorly differentiated carcinomas.[9] Only one of five papillary carcinoma patients in their cohort had a positive scan. In contrast, our case represents a rare example of 68Ga-DOTATATE PET/MRI successfully detecting all metastatic sites in an aggressive variant of PTC, emphasizing the evolving role of somatostatin receptor imaging even in selected papillary subtypes.
Conclusion
Beyond the well-known phenomenon of iodine-negativity in aggressive PTC, this case contributes an uncommon anatomical presentation and emphasizes the role of multimodal imaging in the early identification of extra-axial muscle metastases.
Conflict of Interest
None declared.
-
References
- 1 Cabanillas ME, McFadden DG, Durante C. Thyroid cancer. Lancet 2016; 388 (10061): 2783-2795
- 2 Hirsch D, Levy S, Tsvetov G. et al. Long-term outcomes and prognostic factors in patients with differentiated thyroid cancer and distant metastases. Endocr Pract 2017; 23 (10) 1193-1200
- 3 Herbowski L. Skeletal muscle metastases from papillary and follicular thyroid carcinomas: an extensive review of the literature. Oncol Lett 2018; 15 (05) 7083-7089
- 4 Bruglia M, Palmonella G, Silvetti F. et al. Skin and thigh muscle metastasis from papillary thyroid cancer. Singapore Med J 2009; 50 (02) e61-e64
- 5 Haugen BR, Alexander EK, Bible KC. et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016; 26 (01) 1-133
- 6 Hitu L, Cainap C, Apostu D. et al. Skeletal muscle metastasis in papillary thyroid microcarcinoma evaluated by F18-FDG PET/CT. Diagnostics (Basel) 2020; 10 (02) 10
- 7 Yang J, Li LF, Zhang XM. et al. Unusual synchronous skeletal muscle and lung metastasis in papillary thyroid cancer: a case report and review of the literature. Oncol Lett 2015; 9 (02) 727-730
- 8 Almeida LS, Araújo MC, Zantut-Wittmann DE. et al. Effect of thyroid-stimulating hormone in 68Ga-DOTATATE PET/CT of radioiodine-refractory thyroid carcinoma: a pilot study. Nucl Med Commun 2018; 39 (05) 441-450
- 9 Binse I, Poeppel TD, Ruhlmann M. et al. 68Ga-DOTATOC PET/CT in patients with iodine- and 18F-FDG-negative differentiated thyroid carcinoma and elevated serum thyroglobulin. J Nucl Med 2016; 57 (10) 1512-1517
Address for correspondence
Publication History
Article published online:
03 June 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Cabanillas ME, McFadden DG, Durante C. Thyroid cancer. Lancet 2016; 388 (10061): 2783-2795
- 2 Hirsch D, Levy S, Tsvetov G. et al. Long-term outcomes and prognostic factors in patients with differentiated thyroid cancer and distant metastases. Endocr Pract 2017; 23 (10) 1193-1200
- 3 Herbowski L. Skeletal muscle metastases from papillary and follicular thyroid carcinomas: an extensive review of the literature. Oncol Lett 2018; 15 (05) 7083-7089
- 4 Bruglia M, Palmonella G, Silvetti F. et al. Skin and thigh muscle metastasis from papillary thyroid cancer. Singapore Med J 2009; 50 (02) e61-e64
- 5 Haugen BR, Alexander EK, Bible KC. et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016; 26 (01) 1-133
- 6 Hitu L, Cainap C, Apostu D. et al. Skeletal muscle metastasis in papillary thyroid microcarcinoma evaluated by F18-FDG PET/CT. Diagnostics (Basel) 2020; 10 (02) 10
- 7 Yang J, Li LF, Zhang XM. et al. Unusual synchronous skeletal muscle and lung metastasis in papillary thyroid cancer: a case report and review of the literature. Oncol Lett 2015; 9 (02) 727-730
- 8 Almeida LS, Araújo MC, Zantut-Wittmann DE. et al. Effect of thyroid-stimulating hormone in 68Ga-DOTATATE PET/CT of radioiodine-refractory thyroid carcinoma: a pilot study. Nucl Med Commun 2018; 39 (05) 441-450
- 9 Binse I, Poeppel TD, Ruhlmann M. et al. 68Ga-DOTATOC PET/CT in patients with iodine- and 18F-FDG-negative differentiated thyroid carcinoma and elevated serum thyroglobulin. J Nucl Med 2016; 57 (10) 1512-1517