

Subscribe to RSS
DOI: 10.1055/s-0045-1809414
Fixing the “Oops” Moment: Glueing Up Pulmonary Artery Pseudoaneurysm after a Lung Biopsy
Authors


Abstract
Computed tomography-guided lung biopsy is a common procedure performed to obtain adequate tissue not just for diagnosis but also for molecular typing. Hemothorax is a rare yet serious complication of percutaneous lung biopsies with reported incidence of 0.092%. This is most commonly due to the injury to the intercostal artery or internal mammary artery. However, bleeding due to pulmonary artery involvement is rare and we report one such case which was managed by percutaneous glue embolization.
Introduction
Computed tomography (CT)-guided lung biopsy is a common procedure performed to obtain adequate tissue not just for diagnosis but also for molecular typing. Hemothorax is a rare yet serious complication of percutaneous lung biopsies with reported incidence of 0.092%.[1] This is most commonly due to the injury to the intercostal artery or internal mammary artery. However, bleeding due to pulmonary artery involvement is rare and we report one such case which was managed by percutaneous glue embolization.
Case Report
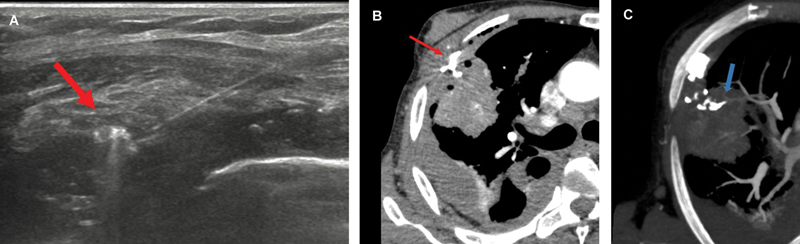
A 67-year-old man with chronic kidney disease, anemia, chronic obstructive pulmonary disease, and weight loss presented with a 5.5 × 4 cm mass with spiculated margins in the right upper lobe on the CT chest ([Fig. 1]). CT-guided biopsy was performed using a coaxial system of 18G 16-cm long and 2-cm throw. Postbiopsy CT showed mild hemothorax. The patient started complaining of mild pain with a gradual increase, and the need for oxygenation increased from 2 to 5 L. A noncontrast CT performed after 1 hour showed an increase in hemothorax occupying half of the right hemithorax ([Fig. 2A]). The patient did not have any episodes of hemoptysis. Ultrasound (USG) screening revealed a peripheral pulmonary artery pseudoaneurysm adjacent to the pleura measuring approximately 15 × 14 mm, confirmed with CT angiography ([Fig. 2B–D]).


Given the peripheral location and visibility on USG, it was decided to treat the pseudoaneurysm percutaneously under USG and CT guidance. Under USG guidance, the pseudoaneurysm sac was percutaneously punctured with a 22G lumbar puncture needle and injection of glue: lipiodol mixture (1:5 dilution) was performed after carefully positioning the needle within the neck of the pseudoaneurysm ([Fig. 3A]). USG and CT angiography confirmed complete thrombosis of the pseudoaneurysm with glue cast seen along the peripheral pulmonary artery ([Fig. 3B]). Postprocedure, his oxygen requirement came down subsequently with no further increase in hemothorax and the patient was discharged after 2 days in stable condition. Serial USG thorax was performed for monitoring the hemothorax. As the patient was stable with no increase in hemothorax, he was managed conservatively.
Discussions
Lung biopsies have become an increasingly common procedure for the diagnosis of thoracic lesions, particularly those suspected of being malignant. Pneumothorax and pulmonary hemorrhage are the most common complications.[2] One of the less common but potentially life-threatening complications is injury to the pulmonary artery, leading to hemothorax. In such cases, rapid recognition and appropriate management are crucial, as hemothorax can rapidly lead to hemodynamic instability and respiratory compromise. Pulmonary artery aneurysms (PAAs) can be further classified into two types: proximal (or central) and peripheral PAAs.[3] Central PAAs involve the pulmonary trunk and the main right and left pulmonary arteries, while peripheral PAAs involve intrapulmonary arteries. Low pressure, low resistance, and increased fragility are characteristic of the pulmonary vasculature, and thus, transection of this can lead to massive hemorrhage and even death.[4]
In our case, a well-demarcated peripheral pseudoaneurysm was seen on USG and hence it was percutaneously embolized with glue. Successful percutaneous glue embolization of pseudoaneurysm in the thoracic region has been extensively described in the studies by Lal et al and Shin et al.[4] [5]
Glue has better control and is visible when mixed with lipiodol as compared with thrombin. Real-time visualization with USG and fluoroscopic guidance is advantageous compared with CT. Nontarget embolization of the glue, though described in literature, can be reduced by using high concentration resulting in earlier solidification.[6] Percutaneous injection of liquid embolic whenever possible can go a long way in being cost-effective and less time-consuming compared with the endovascular approach.
Conclusion
This case report shows that percutaneous glue embolization is safe and cost-effective approach in the management of a rare complication of lung biopsy, pulmonary artery pseudoaneurysm.
Conflict of Interest
None declared.
Acknowledgments
The authors would like to express their sincere gratitude to all authors that contributed to this case report. The authors also would like to thank the patient for consenting to the publication of their case, allowing them to contribute to the medical community's understanding of percutaneous glue embolization in pulmonary artery pseudoaneurysm.
Patients' Consent
Patient consent has been obtained.
-
References
- 1 Tomiyama N, Yasuhara Y, Nakajima Y. et al. CT-guided needle biopsy of lung lesions: a survey of severe complication based on 9783 biopsies in Japan. Eur J Radiol 2006; 59 (01) 60-64
- 2 Baratella E, Cernic S, Minelli P. et al. Accuracy of CT-guided core-needle biopsy in diagnosis of thoracic lesions suspicious for primitive malignancy of the lung: a five-year retrospective analysis. Tomography 2022; 8 (06) 2828-2838
- 3 Fontana F, Piacentino F, Curti M. et al. Pulmonary artery pseudoaneurysms embolization: bicentric experience and review of the literature. J Clin Med 2023; 12 (11) 3796
- 4 Lal A, Bansal A, Chaluvashetty SB, Sandhu MS, Gorsi U. Percutaneous transthoracic embolisation for massive haemoptysis secondary to peripheral pulmonary artery pseudoaneurysms. Eur Radiol 2021; 31 (04) 2183-2190
- 5 Shin S, Shin TB, Choi H. et al. Peripheral pulmonary arterial pseudoaneurysms: therapeutic implications of endovascular treatment and angiographic classifications. Radiology 2010; 256 (02) 656-664
- 6 Garg A, Chandrasekaran K, Jadhav S, Chandok G, Ringe A, Sankhe A. Intra-aneurysmal glue embolisation of a giant pulmonary artery pseudoaneurysm after left upper lobe lobectomy: case report. Korean J Radiol 2013; 14 (03) 455-459
Address for correspondence
Publication History
Article published online:
11 June 2025
© 2025. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Tomiyama N, Yasuhara Y, Nakajima Y. et al. CT-guided needle biopsy of lung lesions: a survey of severe complication based on 9783 biopsies in Japan. Eur J Radiol 2006; 59 (01) 60-64
- 2 Baratella E, Cernic S, Minelli P. et al. Accuracy of CT-guided core-needle biopsy in diagnosis of thoracic lesions suspicious for primitive malignancy of the lung: a five-year retrospective analysis. Tomography 2022; 8 (06) 2828-2838
- 3 Fontana F, Piacentino F, Curti M. et al. Pulmonary artery pseudoaneurysms embolization: bicentric experience and review of the literature. J Clin Med 2023; 12 (11) 3796
- 4 Lal A, Bansal A, Chaluvashetty SB, Sandhu MS, Gorsi U. Percutaneous transthoracic embolisation for massive haemoptysis secondary to peripheral pulmonary artery pseudoaneurysms. Eur Radiol 2021; 31 (04) 2183-2190
- 5 Shin S, Shin TB, Choi H. et al. Peripheral pulmonary arterial pseudoaneurysms: therapeutic implications of endovascular treatment and angiographic classifications. Radiology 2010; 256 (02) 656-664
- 6 Garg A, Chandrasekaran K, Jadhav S, Chandok G, Ringe A, Sankhe A. Intra-aneurysmal glue embolisation of a giant pulmonary artery pseudoaneurysm after left upper lobe lobectomy: case report. Korean J Radiol 2013; 14 (03) 455-459