

Subscribe to RSS
DOI: 10.1055/s-0045-1809035
Evaluation of Two-Point Compression Ultrasound as a Screening Tool for Lower Extremity Deep Venous Thrombosis in a Neurocritical Care Unit: Insights from a Single-Center Study
Authors


Abstract
Background
Deep venous thrombosis (DVT) is an important cause of morbidity and mortality in the intensive care unit (ICU) and it is often missed in the neurocritical care unit (NCCU) as patients might not manifest with obvious symptomatology. Screening of these patients may provide a preventive benefit. The routine use of formal lower extremity venous Doppler (LEVD) scan, which is done by a vascular laboratory technician and comprises the imaging of the entire lower extremity venous system plus Doppler imaging, can be resource intensive. Alternatively, the two-point compression ultrasound (2-CUS), which consists of the imaging and compression at the common femoral vein and popliteal fossa, is quick and can be done by the clinician at bedside with minimal training. The aim of this study is to evaluate the use of 2-CUS as a screening tool for all patients in the NCCU.
Methods
We performed a retrospective analysis of prospectively collected data for consecutive patients admitted to the NCCU at Baylor College of Medicine between August 2020 and February 2021. A 2-CUS scan was performed by neurocritical care fellows, evaluating the bilateral common femoral veins and popliteal veins without color Doppler, on admission and every third day. An LEVD scan was performed in all NCCU patients every 7 days and sooner if 2-CUS scan was positive. The inclusion criteria were patients admitted to the neurocritical care service and age ≥18 years. The exclusion criteria were expected length of stay (LOS) of less than 48 hours, known recent DVT, or positive test for COVID-19.
Results
A total of 298 patients were admitted to the NCCU. 2-CUS was done in 256 patients, while 64 patients underwent both 2-CUS and an LEVD scan. The overall incidence rate of lower extremity DVTs was 10.1%. Nine patients undergoing 2-CUS were positive, of whom six were confirmed by LEVD, and three were false positives (positive predictive value = 66.7%). Two patients had false-negative 2-CUS (negative predictive value = 96.6%). When compared with LEVD, the sensitivity of 2-CUS was 75% (6/8) and the specificity was 95% (57/60). The sensitivity for proximal DVTs was 100%. The two DVTs missed were in the posterior tibial veins not scanned with 2-CUS.
Conclusion
This is the first study to evaluate the use of 2-CUS as a screening tool for lower extremity DVTs. An incidence of 10.6% was found on patients with a LOS ≥7 days. With a sensitivity of 100% for proximal DVT, a specificity of 95%, and a diagnostic accuracy of 95%, the authors conclude that 2-CUS is a feasible, easily learnt, quick and cost-effective tool for screening DVT in NCCU patients.
Introduction
Venous thromboembolism (VTE), which includes deep venous thrombosis (DVT) and pulmonary embolism (PE), is an important cause of morbidity and mortality in the intensive care units (ICUs).[1] [2] Studies have shown that the incidence of DVTs in the ICU is somewhere between 13% to 21% in patients not receiving chemical prophylaxis[3] [4] [5] [6] and 5% to 23% in patients receiving chemical prophylaxis.[1] [7] [8] In neurocritical care units (NCCUs), no reliable population-based estimates are available; however, the incidence is perceived to be higher. For instance, the incidence of DVTs in traumatic brain injury patients has been reported to be as high as 40%.[9] DVTs are often asymptomatic in ICU patients.[10] [11] [12] [13] [14] Screening of these asymptomatic patients can lead to a higher rate of DVT detection.[8] [15] [16] This may help in preventing life-threatening complications such as PE and in turn reduce morbidity and mortality, although the evidence supporting this hypothesis is inconsistent.[17] [18] [19] [20] [21]
A typical lower extremity venous Doppler (LEVD) scan combines compression study, color Doppler, and pulse wave Doppler along the entire length of the venous system. Its routine use can be resource intensive and requires experienced ultrasound technicians. In contrast, a two-point compression ultrasound (2-CUS) examination focuses on the highest probability sites for DVTs instead of scanning the whole leg.[22] The shortened examination can be performed with minimal training and has been shown to be a fast and reliable alternative for the diagnosis of DVTs in symptomatic ICU patients with a diagnostic accuracy of 95%.[23] The examination relies solely on compression at two points and cuts down the total scan time by skipping the Doppler exam and evaluation for calf DVTs which are of uncertain clinical significance. The 2-CUS examination can be valuable in critically ill patients with urgent need for evaluation of DVTs, which would otherwise be dependent on availability of an ultrasound technician and an interpreting radiologist.[23] In NCCUs, the technique can be used for frequent screening of high-risk patients such as those with paraplegia or patients unable to receive DVT prophylaxis due to a contraindication. However, the feasibility and accuracy of the 2-CUS have not been well established for screening of asymptomatic patients, particularly in the NCCUs. The aim of this study is to evaluate the use of 2-CUS as surveillance for patients in this patient population.
Methods
Study Design and Patient Population
We performed a retrospective analysis of prospectively collected data for quality improvement purposes of consecutive patients admitted to the NCCU at Baylor College of Medicine between August 2020 and February 2021. All patients admitted to the NCCU older than 18 years were screened for inclusion. The exclusion criteria included an expected length of stay (LOS) of less than 48 hours, based on the perceived lower risk of DVTs with shorter hospital stays. Patients with a positive COVID-19 test were excluded to minimize unnecessary exposure. Additionally, individuals with a preexisting DVT diagnosis were excluded to reduce potential bias associated with a known DVT diagnosis.
Ultrasound Procedure
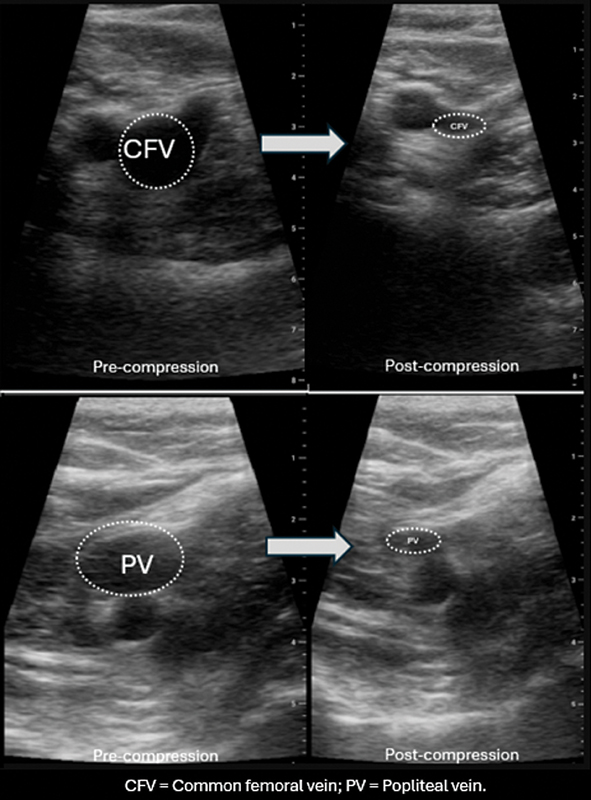
Clinical fellows of the Neurocritical Care Fellowship program (n = 4) at Baylor College of Medicine with no prior experience in lower extremity venous ultrasonography received training to perform 2-CUS. The training included a video lecture, which included both normal and abnormal cases, and a single practical demonstration in human subjects following which the fellows were allowed to do the 2-CUS screening examinations per protocol. There was no prespecified requirement for the fellows to perform a minimum number of practice scans before screening the patients. The ultrasound was performed in the supine position with the patients' hips slightly abducted and externally rotated and the knees flexed as needed to approach the popliteal fossa. We used Philips Sparq (Philips Ultrasound, Bothell, WA, United States) linear array transducer (L12–4) or Fujifilm SonoSite Edge II Total (Fujifilm Ultrasound, Bothell, WA, United States) linear array transducer (L10–5) to visualize lower extremity veins at two sites. The common femoral vein (CFV) was insonated in the inguinal area below the inguinal crease and the popliteal vein (PoV) was imaged in the popliteal fossa along their transverse axis. The examination was limited to these two points and was not aided by Doppler augmentation. Color Doppler was used at the operator's discretion to aid in the identification of the vein but was not required for thrombus evaluation. The criteria for positive test for DVT on 2-CUS included the visualization of an echogenic focus inside the vein (consistent with a thrombus) and inability to compress the vein completely (so the superior and inferior walls of the vein touch and the vein is completely collapsed; see [Fig. 1]). The scans were interpreted by the fellow performing the ultrasound. The screening 2-CUS examination was done on admission, every third day and when there was a clinical suspicion of DVT until detection of a DVT, death, or discharge of the patient from the ICU.
An LEVD scan was requested by the treating team in patients based on a positive 2-CUS, clinical suspicion of DVT, or on all patients on every seventh day of their NCCU admission. This scan was done using Philips Epic (Philips Ultrasound) linear array transducer (L9–3) or Philips iU22 (Philips Ultrasound) linear array transducer (L9–3) by a certified vascular ultrasound technician and interpreted by a radiologist. It involved a more extensive evaluation of both proximal and distal lower extremity venous system including the CFV, femoral vein (FV), deep femoral vein (DFV), PoV, anterior tibial vein (ATV), posterior tibial vein (PTV), and peroneal veins (PrV). The veins were visualized in both transverse and longitudinal axes. The examination included compressibility, evaluation for echogenic material within the vein, color flow, pulse wave Dopplers, and flow augmentation.
Statistical Analysis
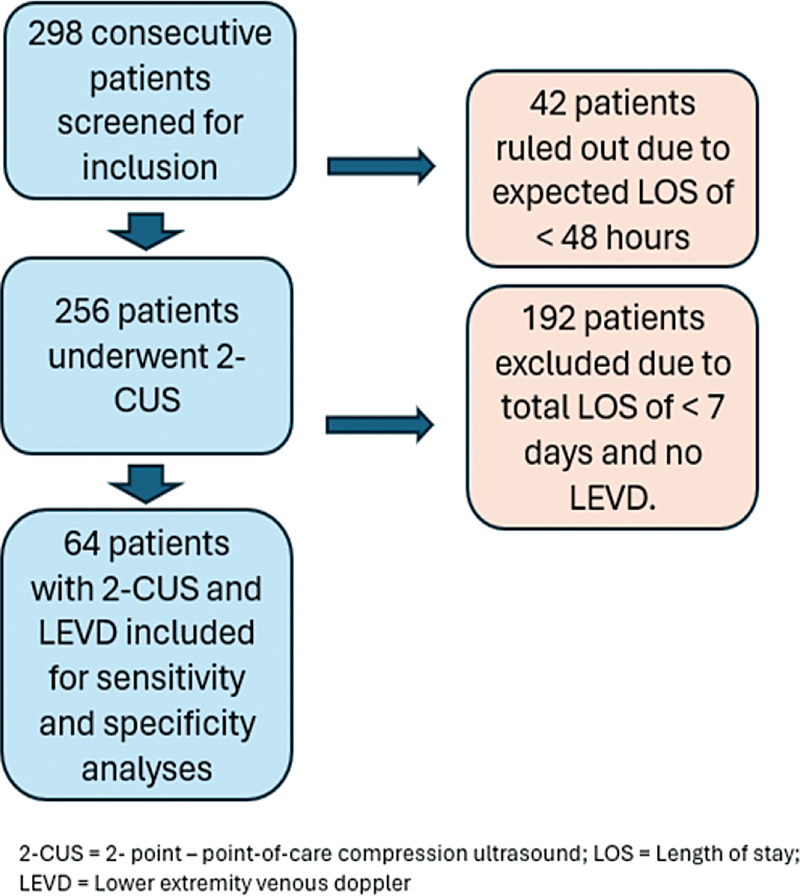
Statistical analysis was performed using SPSS 21 (Armonk, NY, United States). Descriptive statistics were performed for baseline characteristics. Categorical variables were expressed as percentages, while continuous variables were expressed as means and standard deviations. We calculated the overall sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy for lower extremity DVT detection using protocolized 2-CUS scans. Only patients who completed both 2-CUS scans and LEVD were included in these analyses. Wilson score intervals were used to calculate 95% confidence intervals (CIs). Since the calculations involved diagnostic metrics such as sensitivity and specificity based on categorical variables, that is, positive or negative 2-CUS or LEVD scans, patients who were missing either of these scans were excluded without any data imputation ([Fig. 2]). There were no missing data for baseline characteristics reported in the manuscript.
Results
A total of 298 patients were admitted to the NCCU. Forty-two patients were screened out as 2-CUS was not performed either due to anticipated LOS of less than 48 hours (n = 2) or due to patients' refusal or agitation (n = 2). Of the remaining 256 patients, 192 patients were excluded as no LEVD was done due to LOS of between 2 and 6 days. Sixty-four patients underwent both 2-CUS and an LEVD ([Fig. 2]). The baseline characteristics of the studied cohort are detailed in [Table 1]. Briefly, the study population had a mean age of 62.34 years and comprised 40.9% females and 59.1% males. The majority of the patients identified as White (55.2%), followed by African American (26.3%) and Hispanic (13.9%). Most common admission diagnosis was acute ischemic stroke (35%), followed by intracerebral hemorrhage (15.6%), subdural hemorrhage (11%), status epilepticus/seizures (9.8%), and subarachnoid hemorrhage (9.8%).
|
Age (y), mean (SD) |
62.34 (17.67) |
|---|---|
|
Female, n (%) Male, n (%) |
122 (40.9%) 176 (59.1) |
|
White, n (%) African American, n (%) Hispanic, n (%) Asian, n (%) |
155 (55.2) 74 (26.3) 39 (13.9) 13 (4.6) |
|
ICU LOS in days, mean (SD) |
5.31 (5.44) |
|
Obesity, n (%) |
103 (34.6) |
|
History of smoking, n (%) |
49 (16.4) |
|
History of malignancy, n (%) |
47 (15.7) |
|
History of DVT, n (%) |
5 (1.7) |
|
Limb paresis, n (%) |
70 (23.5) |
|
Recent surgery, n (%) |
116(38.8) |
|
Admission diagnosis, n (%) |
|
|
AIS SAH SDH ICH SCI SE/seizures TBI Postneurosurgery Other[a] |
87 (35) 25 (9.8) 28 (11) 40 (15.6) 11 (4.3) 25 (9.8) 8 (3.1) 29 (11.3) 32 (12.5) |
Abbreviations: AIS, acute ischemic stroke; DVT, deep vein thrombosis; ICH, intracranial hemorrhage; ICU, intensive care unit; LOS, length of stay; SAH, subarachnoid hemorrhage; SCI, spinal cord injury; SD, standard deviation; SDH, subdural hematoma; SE, status epilepticus; TBI, traumatic brain injury.
a Other includes encephalopathy and neuromuscular, infectious/inflammatory, and neoplastic processes.
The incidence of DVT in patients who underwent LEVD was 8 (10.6%). 2-CUS was done in 256 patients; 9 patients were positive, of whom 6 were confirmed by LEVD and 3 were false positives. Two patients had false-negative 2-CUS. When compared with LEVD, the sensitivity of 2-CUS was 75% (95% CI: 0.41–0.93) and specificity was 93.1% (95% CI: 0.84–0.97). The positive predictive value was 66.7% (95% CI: 0.35–0.88) and the negative predictive value was 96.4% (95% CI: 0.88–0.99; see [Table 2]). Among the nine patients with DVT, 5 had a diagnosis of acute ischemic stroke, 2 patients had subarachnoid hemorrhage, 1 was status post neurosurgery, and 1 had spinal cord pathology. The diagnostic accuracy increased from 82.6% during the first month to 97.6% after the first month of the study with an overall diagnostic accuracy of 92.6% (95% CI: 0.83–0.97), suggesting a learning curve. The sensitivity for proximal above-knee DVTs, that is, CFV and PoV, was 100%. The two DVTs missed on 2-CUS were located in the PTVs, which were not scanned with 2-CUS.
Abbreviations: CI, confidence interval; FN, false positive; NPV, negative predictive value; PPV, positive predictive value; TP, true positive.
Discussion
To our knowledge, this is the first study evaluating the use of serial 2-CUS as a screening tool for DVTs in NCCUs. The sensitivity for all DVTs in this study was 75% as it missed two distal PTV DVTs. Our study was able to capture 100% of all proximal DVTs, which are typically associated with higher risk of life-threatening VTE or PE.[24] [25] [26] The clinical significance of distal DVTs is unclear as data suggest that they may not extend proximally, remain uneventful, and might not benefit from anticoagulation.[24] [25] [26] Specificity for all DVTs reported in our study was 95%. The three false positives occurred in the first month of the study, indicating a learning curve and a better diagnostic accuracy with time and experience with this diagnostic tool. It should also be noted that 2-CUS and LEVDs were not performed simultaneously and the differences in the result might be secondary to a new clot formation, clot propagation, or clot migration.[23]
The diagnostic accuracy measures reported in our study are similar to the three previously reported ICU studies that compared the performance of point-of-care ultrasound with LEVD for the detection of DVTs. Kory et al performed a three-point compression ultrasound (CFV, SFV, and PV) in medical, surgical, and cardiothoracic ICUs and reported a sensitivity of 86% and specificity of 96%.[23] Caronia et al reported a lower sensitivity of 63% and comparable specificity of 97% for 2-CUS ultrasound scans (CFV and PV) performed by a medical resident. Although residents showed 97% agreement with LEVDs, a higher incidence of FV DVTs that were not scanned by 2-CUS resulted in a much lower sensitivity.[27] It should be noted that in our study, no FV DVTs were identified, which resulted in a higher sensitivity for proximal DVTs. Recently, a prospective observational study reported sensitivity of 69% (95% CI: 41.3–89) and specificity of 99% (95% CI: 96.7–100) with an intensivist-performed three-point CUS (CFV, FV, and PV) in trauma patients. The false-negative scans were reported for nonocclusive DVTs and a single false-positive scan was due to misinterpretation of the femoral artery as a vein.[28] The first two studies were done in patients with a clinical suspicion of DVT[23] [27] and the last study utilized routine twice-weekly surveillance for high-risk trauma patients.[28] Please see [Table 3] for a comparison of these studies with our study.
|
Study |
Imaging protocol |
Reason for examination |
Incidence of lower extremity DVTs |
Sensitivity |
Specificity |
Accuracy |
|---|---|---|---|---|---|---|
|
Kory et al[23] (N = 128) |
3 compressions along the CFV, 2 compressions along the PoV, and sequential compression along the FV in 2-cm increments if the CFV and PoV sites were fully compressible |
Clinical suspicion. No routine surveillance |
20% |
86% |
96% |
95% |
|
Caronia et al[27] (N = 75) |
Compression at the CFV and popliteal veins |
Clinical suspicion. No routine surveillance |
16% |
63% |
97% |
n/a |
|
Roberts et al[28] (N = 117) |
3 compressions along the CFV, 2 compressions along the PoV, and sequential compression along the FV in 2-cm increments if the CFV and PoV sites were fully compressible |
Twice weekly screening in prespecified high-risk patient population |
22.2 |
69% (95% CI: 41.3–89) |
99% (95% CI: 96.7–100) |
n/a |
|
Current study (N = 64) |
Compression at the CFV and popliteal veins |
Clinical suspicion and routine surveillance twice weekly |
10.1% |
75% (95% CI: 41–93) |
94.6% (95% CI: 85–98) |
92.2% (95 CI: 83–97 |
Abbreviations: CFV, common femoral vein; CI, confidence interval; FV, femoral vein; n/a, not applicable; PoV, popliteal vein.
The incidence of 10.6% for DVTs in our study is comparable to the previously reported incidence by Dickerson et al in NCCU patients when weekly LEVDs were used for surveillance.[21] However, other studies report a significant variation in the incidence of DVTs ranging from 2.5% in neurosurgical patients[29] to 40% in traumatic brain injury patients.[9] Both studies used LEVDs twice weekly as a surveillance method.[9] [29] There is also a notable variation in the incidence of DVTs in non-neurological critical care patients, ranging from 2.8 to 23% with different surveillance screening protocols.[1] [3] [4] [5] [6] [7] [8] [20] [28] This variation can be explained by the heterogenous patient population, smaller cohort sizes, differences in the surveillance protocols, and frequency of screening examinations in these studies.[28] [29]
DVT surveillance is not the standard of practice and more studies are needed to evaluate its benefits and appropriate protocols. Studies looking at routine surveillance of DVTs have shown increased rates of detection for DVTs, but have failed to consistently show a decrease in life-threatening PE, LOS, morbidity, or mortality.[9] [18] [19] [20] [21] [29] [30] [31] Surveillance studies have been done with LEVD in a twice-weekly or every 3 days frequency.[9] [19] [29] [30] Recently, Arabi et al in a preplanned substudy of the Pneumatic Compression for Preventing Venous Thrombo-embolism Trial (PREVENT) compared a surveilled group with LEVD (n = 1,682) with standard of care showing an increase in DVT detection (n = 383), an earlier diagnosis (4 vs. 20 days, respectively), and a lower 90-day mortality.[19] The overall frequency of PE detection was similar in both groups; however, surveillance was associated with a quicker diagnosis of PE by 4 days.[19] Another similar study in an ICU population (n = 128) showed that surveillance was associated with increased DVT diagnosis (2.8 vs. 1.3% in nonsurveilled patients) and a decrease in the incidence of PE (0.7 vs. 1.5% in nonsurveilled patients).[20] Surveillance was found to be an independent predictor of higher DVT and lower PE incidence. In the mentioned study, the associated cost increment was $509,091 per life saved, suggesting the use of 2-CUS instead of LEVD could lower the associated cost significantly.[20] Among neurosurgical patients, Dickerson et al[21] (n = 485) and Samuel et al[18] (n = 147) failed to demonstrate a reduction in PE and mortality rate when routine surveillance was performed through LEVDs. Larger multicentric and randomized controlled studies are warranted to investigate if 2-CUS surveillance scans can lead to earlier detection of DVTs, prevent clinically significant VTEs and PEs, and affect the overall morbidity and mortality associated with these events.
The notable strength of this study is evaluation of 2-CUS as a screening tool in neurocritical care patient population, which has previously been not well studied. The study emphasizes that 2-CUS scans are feasible in NCCU with relatively quick training of previously unexperienced practitioners and can be used for faster screening and surveillance. The technique can be quickly learnt, is faster, and is cost-effective. However, the technique does not necessarily replace the need for LEVD when a strong clinical suspicion is present as it carries a risk of detecting false positives and can have false negatives. A positive 2-CUS should be followed up with LEVD to avoid overtreatment. Although this study detected proximal DVTs with 100% sensitivity, the technique still has a potential to miss out on proximal DVTs that are typically not insonated with the 2-CUS such as FV and DFVs.[27] In addition, it can miss out on distal DVTs as seen in our study. Thus, a strong clinical suspicion should prompt LEVD despite a negative 2-CUS study.
The study has several limitations. The single-center design of the study with a small sample size consisting of a specific patient population limits the generalizability of this study. Certain patient populations such as patients with traumatic brain injury are under-represented in our study. The study was done in an academic center where a large treatment team comprising attending physicians, neurocritical care fellows, and residents were responsible for taking care of the patients. The routine screening examinations may not be feasible for a smaller team taking care of a high volume of patients. The study does not explore the metrics for the individual operators and the impact of inter-rater variability. The small sample size can lead to potentially imprecise estimates of sensitivity and specificity. However, the overall diagnostic accuracy of this study is similar to the previously reported literature.[19] [20] [21] The neurocritical care fellows, ultrasound technicians, and interpreting radiologists were not strictly blinded to other's sonographic findings. However, the 2-CUS scans were generally performed before the LEVDs and the results of 2-CUS scans were not communicated to the ultrasound technicians or radiologists. Another limitation is that the 2-CUS scans and LEVDs were not performed simultaneously. Per protocol, a positive 2-CUS examination led to an immediate request for LEVD, which was performed within a day. However, for negative screening examinations, the time interval between 2-CUS and LEVD ranged from 0 to 3 days. This introduces a potential bias as clot formation between the two examinations could have potentially impacted the false-negative rate. However, in our study, the two observed false-negative scans were for distal PTVs not scanned during 2-CUS examination. Finally, the study did not address if the routine surveillance with 2-CUS leads to a more rapid detection of DVTs and how it can affect the overall morbidity and mortality of the patients.
Conclusion
2-CUS is a quick bedside tool to screen for DVTs and can be quickly learnt by providers with no formal training in ultrasonography. Our study supports that 2-CUS is feasible, quick, and cost-effective tool for screening clinically significant lower extremity proximal DVTs in NCCU patients. Future studies are needed to validate these findings in larger cohorts and to assess if such screening protocols can effectively increase the rate of DVT detection and lower the life-threatening thromboembolic complications such as PE and overall mortality in this patient population.
Conflict of Interest
None declared.
* All authors were affiliated with Baylor College of Medicine when this work was conducted. Muhammad U. Hafeez is currently affiliated with the Department of Neurology, University of Texas Medical Branch, Galveston, Texas. Ivan Cuesta is affiliated with the Department of Neurology, Advocate General Lutheran Hospital, Chicago, Illinois. Aaron A. Desai is currently affiliated with the Department of Neurology, University of South Florida, Tampa, Florida.
# Muhammad U. Hafeez and Ivan Cuesta are the first co-authors.
-
References
- 1 Cook D, Crowther M, Meade M. et al. Deep venous thrombosis in medical-surgical critically ill patients: prevalence, incidence, and risk factors. Crit Care Med 2005; 33 (07) 1565-1571
- 2 Attia J, Ray JG, Cook DJ, Douketis J, Ginsberg JS, Geerts WH. Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med 2001; 161 (10) 1268-1279
- 3 Moser KM, LeMoine JR, Nachtwey FJ, Spragg RG. Deep venous thrombosis and pulmonary embolism. Frequency in a respiratory intensive care unit. JAMA 1981; 246 (13) 1422-1424
- 4 Cade JF. High risk of the critically ill for venous thromboembolism. Crit Care Med 1982; 10 (07) 448-450
- 5 Kapoor M, Kupfer YY, Tessler S. Subcutaneous heparin prophylaxis significantly reduces the incidence of venous thromboembolic events in the critically ill. Crit Care Med 1999; 27 (12) A69
- 6 Fraisse F, Holzapfel L, Couland JM. et al; The Association of Non-University Affiliated Intensive Care Specialist Physicians of France. Nadroparin in the prevention of deep vein thrombosis in acute decompensated COPD. Am J Respir Crit Care Med 2000; 161 (4, Pt 1): 1109-1114
- 7 Ibrahim EH, Iregui M, Prentice D, Sherman G, Kollef MH, Shannon W. Deep vein thrombosis during prolonged mechanical ventilation despite prophylaxis. Crit Care Med 2002; 30 (04) 771-774
- 8 Cook D, Meade M, Guyatt G. et al; PROTECT Investigators for the Canadian Critical Care Trials Group and the Australian and New Zealand Intensive Care Society Clinical Trials Group. Dalteparin versus unfractionated heparin in critically ill patients. N Engl J Med 2011; 364 (14) 1305-1314
- 9 Yang T, Wei G, Zhu C, Pan A. Incidence and risk factor analysis of deep venous thrombosis in patients with severe traumatic brain injury. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2019; 31 (02) 182-186
- 10 Eck RJ, Hulshof L, Wiersema R. et al. Incidence, prognostic factors, and outcomes of venous thromboembolism in critically ill patients: data from two prospective cohort studies. Crit Care 2021; 25 (01) 27
- 11 Schultz DJ, Brasel KJ, Washington L. et al. Incidence of asymptomatic pulmonary embolism in moderately to severely injured trauma patients. J Trauma 2004; 56 (04) 727-731 , discussion 731–733
- 12 Ciuti G, Grifoni E, Pavellini A. et al. Incidence and characteristics of asymptomatic distal deep vein thrombosis unexpectedly found at admission in an internal medicine setting. Thromb Res 2012; 130 (04) 591-595
- 13 Shimabukuro N, Mo M, Hashiyama N. et al. Clinical course of asymptomatic isolated distal deep vein thrombosis of the leg: a single-institution study. Ann Vasc Dis 2019; 12 (04) 487-492
- 14 Rose SC, Zwiebel WJ, Miller FJ. Distribution of acute lower extremity deep venous thrombosis in symptomatic and asymptomatic patients: imaging implications. J Ultrasound Med 1994; 13 (04) 243-250
- 15 De Martino RR, Beck AW, Edwards MS. et al. Impact of screening versus symptomatic measurement of deep vein thrombosis in a national quality improvement registry. J Vasc Surg 2012; 56 (04) 1045-51.e1
- 16 Skrifvars MB, Bailey M, Presneill J. et al; EPO-TBI investigators and the ANZICS Clinical Trials Group. Venous thromboembolic events in critically ill traumatic brain injury patients. Intensive Care Med 2017; 43 (03) 419-428
- 17 Allen CJ, Murray CR, Meizoso JP. et al. Surveillance and early management of deep vein thrombosis decreases rate of pulmonary embolism in high-risk trauma patients. J Am Coll Surg 2016; 222 (01) 65-72
- 18 Samuel S, Patel N, McGuire MF, Salazar M, Nguyen T. Analysis of venous thromboembolism in neurosurgical patients undergoing standard versus routine ultrasonography. J Thromb Thrombolysis 2019; 47 (02) 209-215
- 19 Arabi YM, Burns KEA, Alsolamy SJ. et al; Saudi Critical Care Trials Group. Surveillance or no surveillance ultrasonography for deep vein thrombosis and outcomes of critically ill patients: a pre-planned sub-study of the PREVENT trial. Intensive Care Med 2020; 46 (04) 737-746
- 20 Malhotra AK, Goldberg SR, McLay L. et al. DVT surveillance program in the ICU: analysis of cost-effectiveness. PLoS One 2014; 9 (09) e106793
- 21 Dickerson JC, Harriel KL, Dambrino RJ. et al. Screening duplex ultrasonography in neurosurgery patients does not correlate with a reduction in pulmonary embolism rate or decreased mortality. J Neurosurg 2019; 132 (05) 1589-1597
- 22 Kearon C, Julian JA, Newman TE, Ginsberg JS. Noninvasive diagnosis of deep venous thrombosis. McMaster Diagnostic Imaging Practice Guidelines Initiative. Ann Intern Med 1998; 128 (08) 663-677
- 23 Kory PD, Pellecchia CM, Shiloh AL, Mayo PH, DiBello C, Koenig S. Accuracy of ultrasonography performed by critical care physicians for the diagnosis of DVT. Chest 2011; 139 (03) 538-542
- 24 Palareti G, Cosmi B, Lessiani G. et al. Evolution of untreated calf deep-vein thrombosis in high risk symptomatic outpatients: the blind, prospective CALTHRO study. Thromb Haemost 2010; 104 (05) 1063-1070
- 25 Utter GH, Dhillon TS, Salcedo ES. et al. Therapeutic anticoagulation for isolated calf deep vein thrombosis. JAMA Surg 2016; 151 (09) e161770
- 26 Robert-Ebadi H, Righini M. Management of distal deep vein thrombosis. Thromb Res 2017; 149: 48-55
- 27 Caronia J, Sarzynski A, Tofighi B. et al. Resident performed two-point compression ultrasound is inadequate for diagnosis of deep vein thrombosis in the critically III. J Thromb Thrombolysis 2014; 37 (03) 298-302
- 28 Roberts L, Rozen T, Murphy D. et al. A preliminary study of intensivist-performed DVT ultrasound screening in trauma ICU patients (APSIT study). Ann Intensive Care 2020; 10 (01) 122-122
- 29 Misra M, Roitberg B, Ebersole K, Charbel FT. Prevention of pulmonary embolism by combined modalities of thromboprophylaxis and intensive surveillance protocol. Neurosurgery 2004; 54 (05) 1099-1102 , discussion 1102–1103
- 30 Shackford SR, Cipolle MD, Badiee J. et al. Determining the magnitude of surveillance bias in the assessment of lower extremity deep venous thrombosis: a prospective observational study of two centers. J Trauma Acute Care Surg 2016; 80 (05) 734-739 , discussion 740–741
- 31 Haut ER, Noll K, Efron DT. et al. Can increased incidence of deep vein thrombosis (DVT) be used as a marker of quality of care in the absence of standardized screening? The potential effect of surveillance bias on reported DVT rates after trauma. J Trauma 2007; 63 (05) 1132-1135 , discussion 1135–1137
Address for correspondence
Publication History
Article published online:
12 May 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Cook D, Crowther M, Meade M. et al. Deep venous thrombosis in medical-surgical critically ill patients: prevalence, incidence, and risk factors. Crit Care Med 2005; 33 (07) 1565-1571
- 2 Attia J, Ray JG, Cook DJ, Douketis J, Ginsberg JS, Geerts WH. Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med 2001; 161 (10) 1268-1279
- 3 Moser KM, LeMoine JR, Nachtwey FJ, Spragg RG. Deep venous thrombosis and pulmonary embolism. Frequency in a respiratory intensive care unit. JAMA 1981; 246 (13) 1422-1424
- 4 Cade JF. High risk of the critically ill for venous thromboembolism. Crit Care Med 1982; 10 (07) 448-450
- 5 Kapoor M, Kupfer YY, Tessler S. Subcutaneous heparin prophylaxis significantly reduces the incidence of venous thromboembolic events in the critically ill. Crit Care Med 1999; 27 (12) A69
- 6 Fraisse F, Holzapfel L, Couland JM. et al; The Association of Non-University Affiliated Intensive Care Specialist Physicians of France. Nadroparin in the prevention of deep vein thrombosis in acute decompensated COPD. Am J Respir Crit Care Med 2000; 161 (4, Pt 1): 1109-1114
- 7 Ibrahim EH, Iregui M, Prentice D, Sherman G, Kollef MH, Shannon W. Deep vein thrombosis during prolonged mechanical ventilation despite prophylaxis. Crit Care Med 2002; 30 (04) 771-774
- 8 Cook D, Meade M, Guyatt G. et al; PROTECT Investigators for the Canadian Critical Care Trials Group and the Australian and New Zealand Intensive Care Society Clinical Trials Group. Dalteparin versus unfractionated heparin in critically ill patients. N Engl J Med 2011; 364 (14) 1305-1314
- 9 Yang T, Wei G, Zhu C, Pan A. Incidence and risk factor analysis of deep venous thrombosis in patients with severe traumatic brain injury. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2019; 31 (02) 182-186
- 10 Eck RJ, Hulshof L, Wiersema R. et al. Incidence, prognostic factors, and outcomes of venous thromboembolism in critically ill patients: data from two prospective cohort studies. Crit Care 2021; 25 (01) 27
- 11 Schultz DJ, Brasel KJ, Washington L. et al. Incidence of asymptomatic pulmonary embolism in moderately to severely injured trauma patients. J Trauma 2004; 56 (04) 727-731 , discussion 731–733
- 12 Ciuti G, Grifoni E, Pavellini A. et al. Incidence and characteristics of asymptomatic distal deep vein thrombosis unexpectedly found at admission in an internal medicine setting. Thromb Res 2012; 130 (04) 591-595
- 13 Shimabukuro N, Mo M, Hashiyama N. et al. Clinical course of asymptomatic isolated distal deep vein thrombosis of the leg: a single-institution study. Ann Vasc Dis 2019; 12 (04) 487-492
- 14 Rose SC, Zwiebel WJ, Miller FJ. Distribution of acute lower extremity deep venous thrombosis in symptomatic and asymptomatic patients: imaging implications. J Ultrasound Med 1994; 13 (04) 243-250
- 15 De Martino RR, Beck AW, Edwards MS. et al. Impact of screening versus symptomatic measurement of deep vein thrombosis in a national quality improvement registry. J Vasc Surg 2012; 56 (04) 1045-51.e1
- 16 Skrifvars MB, Bailey M, Presneill J. et al; EPO-TBI investigators and the ANZICS Clinical Trials Group. Venous thromboembolic events in critically ill traumatic brain injury patients. Intensive Care Med 2017; 43 (03) 419-428
- 17 Allen CJ, Murray CR, Meizoso JP. et al. Surveillance and early management of deep vein thrombosis decreases rate of pulmonary embolism in high-risk trauma patients. J Am Coll Surg 2016; 222 (01) 65-72
- 18 Samuel S, Patel N, McGuire MF, Salazar M, Nguyen T. Analysis of venous thromboembolism in neurosurgical patients undergoing standard versus routine ultrasonography. J Thromb Thrombolysis 2019; 47 (02) 209-215
- 19 Arabi YM, Burns KEA, Alsolamy SJ. et al; Saudi Critical Care Trials Group. Surveillance or no surveillance ultrasonography for deep vein thrombosis and outcomes of critically ill patients: a pre-planned sub-study of the PREVENT trial. Intensive Care Med 2020; 46 (04) 737-746
- 20 Malhotra AK, Goldberg SR, McLay L. et al. DVT surveillance program in the ICU: analysis of cost-effectiveness. PLoS One 2014; 9 (09) e106793
- 21 Dickerson JC, Harriel KL, Dambrino RJ. et al. Screening duplex ultrasonography in neurosurgery patients does not correlate with a reduction in pulmonary embolism rate or decreased mortality. J Neurosurg 2019; 132 (05) 1589-1597
- 22 Kearon C, Julian JA, Newman TE, Ginsberg JS. Noninvasive diagnosis of deep venous thrombosis. McMaster Diagnostic Imaging Practice Guidelines Initiative. Ann Intern Med 1998; 128 (08) 663-677
- 23 Kory PD, Pellecchia CM, Shiloh AL, Mayo PH, DiBello C, Koenig S. Accuracy of ultrasonography performed by critical care physicians for the diagnosis of DVT. Chest 2011; 139 (03) 538-542
- 24 Palareti G, Cosmi B, Lessiani G. et al. Evolution of untreated calf deep-vein thrombosis in high risk symptomatic outpatients: the blind, prospective CALTHRO study. Thromb Haemost 2010; 104 (05) 1063-1070
- 25 Utter GH, Dhillon TS, Salcedo ES. et al. Therapeutic anticoagulation for isolated calf deep vein thrombosis. JAMA Surg 2016; 151 (09) e161770
- 26 Robert-Ebadi H, Righini M. Management of distal deep vein thrombosis. Thromb Res 2017; 149: 48-55
- 27 Caronia J, Sarzynski A, Tofighi B. et al. Resident performed two-point compression ultrasound is inadequate for diagnosis of deep vein thrombosis in the critically III. J Thromb Thrombolysis 2014; 37 (03) 298-302
- 28 Roberts L, Rozen T, Murphy D. et al. A preliminary study of intensivist-performed DVT ultrasound screening in trauma ICU patients (APSIT study). Ann Intensive Care 2020; 10 (01) 122-122
- 29 Misra M, Roitberg B, Ebersole K, Charbel FT. Prevention of pulmonary embolism by combined modalities of thromboprophylaxis and intensive surveillance protocol. Neurosurgery 2004; 54 (05) 1099-1102 , discussion 1102–1103
- 30 Shackford SR, Cipolle MD, Badiee J. et al. Determining the magnitude of surveillance bias in the assessment of lower extremity deep venous thrombosis: a prospective observational study of two centers. J Trauma Acute Care Surg 2016; 80 (05) 734-739 , discussion 740–741
- 31 Haut ER, Noll K, Efron DT. et al. Can increased incidence of deep vein thrombosis (DVT) be used as a marker of quality of care in the absence of standardized screening? The potential effect of surveillance bias on reported DVT rates after trauma. J Trauma 2007; 63 (05) 1132-1135 , discussion 1135–1137