

Subscribe to RSS
DOI: 10.1055/s-0045-1807748
Beyond the Lumen: Role of High-Resolution Magnetic Resonance Vessel Wall Imaging in Assessing Intracranial Aneurysms—A Prospective Observational Study from North India
Authors
Funding None.


Abstract
Background
Intracranial aneurysm rupture leading to subarachnoid hemorrhage (SAH) is associated with high morbidity and mortality. While conventional imaging modalities like computed tomography (CT) angiography and digital subtraction angiography (DSA) are commonly employed, they primarily visualize the lumen rather than the vessel wall itself. Recent advancements in magnetic resonance vessel wall imaging present an opportunity to explore the role of inflammation in aneurysm rupture, thus also potentially serving as a predictor for rupture risk.
Aims
This study aimed to assess vessel wall enhancement patterns in ruptured and unruptured intracranial aneurysms, correlating these patterns with aneurysm morphology and evaluate the relationship between the PHASES score and enhancement characteristics.
Materials and Methods
Patients with confirmed intracranial aneurysms on CT angiography and/or DSA underwent plain and contrast-enhanced T1 SPACE (sampling perfection with application-optimized contrasts using different flip angle evolution) images to assess vessel wall enhancement, which was classified as absent, focal, or circumferential termed as grade 0, 1, and 2, respectively.
Results
Out of 60 patients included in the study, 60% presented with ruptured aneurysms. All ruptured aneurysms showed vessel wall enhancement, which was circumferential in 46.7% cases. In contrast, only 30% of unruptured aneurysms showed any form of enhancement, which was predominantly grade 1. Statistical analysis revealed a significant association between enhancement patterns and rupture status, with a p-value of < 0.001.
Conclusion
Vessel wall enhancement was observed in all ruptured aneurysms, thus suggesting a potential role of inflammation in the disruption of aneurysm wall integrity. It may thus also serve as a predictor of aneurysm rupture, enhancing clinical decision-making for patient management.
Introduction
Intracranial aneurysms are focal dilations of cerebral arteries, arising from defects in the arterial wall and are present in approximately 2 to 5% of the general population.[1] Their size can range from small (less than 5 mm) to large (greater than 10 mm), with giant aneurysms exceeding 25 mm.[2] The most common form, saccular or “berry” aneurysms, account for 80 to 90% of cases. They typically occur at arterial branch points in the circle of Willis, where hemodynamic forces are the greatest. The etiology of intracranial aneurysms is multifactorial, involving both genetic predispositions and acquired risk factors.[1] [3] Environmental factors like long-standing hypertension, cigarette smoking, and excessive alcohol consumption are significant contributors to aneurysm formation and growth.[4] [5] [6] [7]
Intracranial aneurysms are either discovered after they rupture leading to subarachnoid hemorrhage (SAH) or incidentally during imaging for unrelated issues.
Imaging modalities such as computed tomography (CT) and digital subtraction angiography (DSA) have been pivotal in diagnosing and treating these aneurysms; however, they primarily visualize the lumen rather than the vessel wall itself.[8] [9] [10] In contrast, magnetic resonance imaging (MRI) vessel wall imaging (VWI) offers a unique opportunity to assess the characteristics of the aneurysm wall, including enhancement patterns that may indicate underlying inflammation or instability.[11] [12] This emerging technique holds promise for predicting rupture risk in intracranial aneurysms, allowing for more tailored and timely interventions.
This study sought to explore the utility of MRI VWI in detecting the presence of and characterizing patterns of vessel wall enhancement in ruptured intracranial aneurysms compared with those in incidentally detected unruptured aneurysms. The study also aimed to correlate vessel wall enhancement with aneurysm morphology. Additionally, it examined the relationship between the PHASES aneurysmal risk score and the pattern of aneurysm wall enhancement. Understanding the implications of aneurysm wall integrity on rupture risk can significantly enhance clinical decision-making, guiding the need for early intervention in vulnerable patients.
Materials and Methods
Study Population
This prospective observational study was conducted at a tertiary care center in North India over a period of 30 months. The study population included patients, irrespective of age and gender, with ruptured and/or unruptured intracranial aneurysms (UIAs), the presence of which was confirmed on CT and/or DSA. Patients with aneurysm clips, contraindications to MRI, or gadolinium-based contrast agents were excluded from the study. The study received approval from the Institutional Ethics Committee. Informed consent was obtained from all patients participating in the study after they were provided with comprehensive information regarding the study's objectives.
Demographic and Clinical Data
The demographic and clinical information, which included the presence or absence of SAH and other symptoms such as due to mass effect like cranial nerve palsies, visual disturbances, or cognitive alterations in unruptured aneurysms, were obtained from the medical records of each patient. The PHASE score (range 0–12) was used to assess the risk of rupture in case of UIAs ([Table 1]).
Abbreviations: ACA, anterior cerebral artery; ICA, internal carotid artery; MCA, middle cerebral artery; PCOM, posterior communicating artery; SAH, subarachnoid hemorrhage.
Imaging Protocol
All patients with confirmed intracranial aneurysms (ruptured as well as unruptured) underwent VWI using contrast-enhanced MRI to assess enhancement patterns and morphology. Imaging was performed on a 1.5 T MR scanner (Magnetom Avanto, Siemens, Erlangen, Germany). Dedicated sequences for VWI included a whole brain sagittal T1 SPACE (sampling perfection with application optimized contrast using different flip angle evolution) sequence acquired before and 3 minutes after the administration of a gadolinium-based contrast agent, gadodiamide at a dose of 0.2 mmol/kg body weight. The imaging parameters were as follows: TR 700 ms, TE 19 ms, field of view 260 × 256, slice thickness 1 mm, number of slices = 44, and flip angle 120 degrees. Routine MRI sequences, which included axial T2, fluid-attenuated inversion recovery, T1, susceptibility- and diffusion-weighted images, as well as a time-of-flight angiogram, were acquired in addition to high-resolution VWI.
Image Analysis
Pre- and postcontrast T1 SPACE images were visualized using multiplanar reformation in syngo.via software. Aneurysm wall enhancement was documented and graded as follows:
-
Grade 0: No enhancement
-
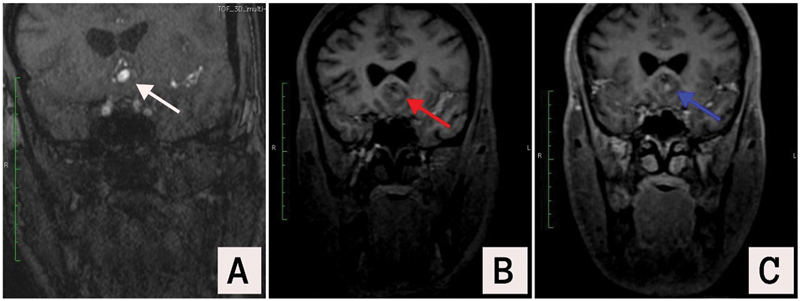
Grade 1: Focal wall enhancement ([Fig. 1])
-
Grade 2: Circumferential wall enhancement ([Figs. 2] and [3])


In case of ruptured intracranial aneurysms, the modified Fisher grading was used to grade the severity of SAH on the noncontrast CT brain acquired at presentation. Aneurysm size, location, width-to-neck ratio, and shape were assessed on CT angiography using volume rendering technique, maximum intensity projections with multiplanar reformation, or three-dimensional digital subtraction angiographic images when available based on standard definitions and technique of measurement.[13] [14]
Statistical Methods
Data analysis was done using the SPSS Version 29.0 data editor (SPSS Inc., Chicago, Illinois, United States). Continuous variables were reported as mean ± standard deviation (SD), while categorical variables were summarized as frequencies and percentages. The chi-square test or Fisher's exact test, as appropriate, was used to compare categorical variables. A p-value of less than 0.05 was deemed statistically significant, and all p-values were two-tailed.
Results
The study included 60 subjects, out of which 34 (56.7%) were females and 49 out of 60 (81.6%) were in the age group of 40 to 60 years.
A total of 73 aneurysms were detected in 60 patients, out of which 13 aneurysms were excluded in view of incomplete data or imaging artifacts. Thus, a total of 60 aneurysms were included in the study. Forty-seven out of 60 patients (78.3%) in this study had a single aneurysm, with 2 aneurysms in 13 (21.7%) patients. None of the patients had more than two aneurysms. Sixty percent of aneurysms were ruptured.
The aneurysm size ranged between 1.1 and 16.2 mm with a mean of 6.14 mm and SD of 4.43 mm (6.14 ± 4.43 mm). Only 12 out of 60 (80%) aneurysms were more than 10 mm in size. The aneurysm location is detailed in [Table 2].
|
Site of aneurysm |
n |
% |
|---|---|---|
|
ICA |
25 |
41.7 |
|
MCA |
13 |
21.7 |
|
ACOM |
9 |
15.0 |
|
ACA |
7 |
11.6 |
|
Posterior circulation |
6 |
10.0 |
|
Total |
60 |
100.0 |
Abbreviations: ACA, anterior cerebral artery; ACOM, anterior communicating artery; ICA, internal carotid artery; MCA, middle cerebral artery.
There was no statistically significant difference in the grade of enhancement between risk groups stratified on the basis of the PHASES aneurysm risk score ([Table 3]).
p values which are significant have been shown in bold.
All the ruptured aneurysms showed vessel wall enhancement with circumferential enhancement ([Figs. 2] and [3]) in 63.9%. No wall enhancement was seen in 11 out of 24 (45.8%) unruptured aneurysms. Among unruptured aneurysms with wall enhancement, grade 1 enhancement (focal) prevailed over grade 2 (circumferential) ([Table 4]).
Abbreviation: SAH, subarachnoid hemorrhage.
p values which are significant have been shown in bold.
There was a statistically significant higher proportion of wall enhancement among aneurysms with a width-to-neck ratio of ≥ 1.5 compared with those with smaller ratios. There was, however, no influence of shape on aneurysm wall enhancement ([Table 4]).
Discussion
Intracranial aneurysm rupture is a significant cause of mortality and morbidity worldwide. The development of intracranial aneurysms is associated with several acquired and genetic factors. However, there is a significant proportion of these aneurysms, which are incidentally detected and stay stable over time without undergoing rupture. Although aneurysm size, location, and shape have been found to be contributory factors, in the recent past aneurysm wall inflammation has been proposed as a possible pathophysiologic mechanism in initiating aneurysm rupture. High-resolution magnetic resonance VWI allows visualization of enhancement within the aneurysm wall. This enhancement may be a surrogate marker for inflammation in ruptured and unruptured aneurysms.
Wall enhancement was seen in all the ruptured aneurysms on postcontrast T1 SPACE images in our study suggesting that enhancement is an indicator of aneurysm instability. This enhancement was circumferential in more than half of the ruptured aneurysms. Our findings are consistent with the existing literature.[15] [16] Histological studies have correlated circumferential wall enhancement with infiltration by inflammatory cells whereas focal wall enhancement is usually seen at areas of local thrombus formation and atherosclerotic changes.
The study's findings on enhancement patterns, particularly the prevalence of circumferential enhancement, are consistent with prior research. Edjlali et al noted that circumferential aneurysmal wall enhancement was significantly more common in unstable aneurysms.[16] Supporting this, our study observed circumferential enhancement in 63.9% of ruptured aneurysms versus 20.8% of unruptured cases. This robust association between wall enhancement and aneurysm rupture represents a clinically significant aspect of our findings, corroborated by Wang et al, who demonstrated a strong association between wall enhancement and rupture (odds ratio = 34.26).[17] Collectively, these results suggest that wall enhancement could serve as a valuable imaging biomarker for identifying high-risk aneurysms.
Among the unruptured aneurysms studied, vessel wall enhancement was observed in 54.2% of cases, with 33.3% exhibiting focal enhancement and 20.8% displaying circumferential enhancement. Although our study did not specifically focus on symptomatic cases, vessel wall enhancement patterns can serve as important indicators of the stability and risk associated with UIAs. The observed pattern of vessel wall enhancement may help distinguish high-risk aneurysms that could benefit from closer monitoring or intervention. Fu et al found that symptomatic UIAs were more likely to show circumferential adventitial wall enhancement and had a higher wall enhancement index compared with asymptomatic UIAs.[18] Additionally, Xu et al noted that both qualitative and quantitative wall enhancements moderately predict unstable intracranial aneurysms.[19] Similarly, Fu et al reported that circumferential enhancement was more prevalent in symptomatic unruptured aneurysms.[20]
The moderate correlation between enhancement patterns and aneurysm type (ruptured vs. unruptured), coupled with a strong association with SAH grade, suggests that wall enhancement effectively integrates with existing risk stratification methods. Additionally, the relationship between aneurysm morphology—specifically, the width-to-neck ratio—and wall enhancement underscores the link between enhancement and established risk factors for instability and rupture. Our findings regarding the association between aneurysm morphology and enhancement resonate with those of Lv et al, who identified that morphological parameters like size ratio and nonsphericity index were independently associated with wall enhancement.[21]
PHASES aneurysm risk score did not correlate with the enhancement patterns observed in the vessel walls of the unruptured aneurysms (p-value = 0.99), which suggests that the PHASES score, which is designed to assess the risk of aneurysm rupture, cannot be used to predict the degree or type of vessel wall enhancement in these patients. Furthermore, since the grade and pattern of enhancement are directly related, the conclusion reinforces that the PHASES aneurysm risk score is not a reliable indicator of enhancement characteristics, thereby limiting its utility in predicting aneurysm stability based on imaging features. This is in contrast to the study by Lv et al who observed a correlation between wall enhancement in unruptured aneurysms and higher PHASES scores, indicating an increased risk of rupture.[22] The contrasting findings may stem from differences in sample size, demographics, clinical characteristics of the populations studied, and methodological variations, such as imaging techniques and criteria for measuring enhancement. Additionally, differences in assessment criteria for vessel wall enhancement and underlying pathophysiological factors may play a role. These factors highlight the complexity of aneurysm assessment and the need for further research to clarify the relationship between imaging features and risk scores.
While our study primarily employed qualitative assessments of wall enhancement, the literature indicates the potential utility of quantitative measures. Notably, studies by Wu et al and Fu et al utilized quantitative methods such as contrast ratios between the aneurysm wall and pituitary stalk.[18] [23] Future iterations of this research could benefit from incorporating such quantitative assessments to allow for more precise comparisons, potentially enhancing the accuracy and reproducibility of wall enhancement evaluations.
A meta-analysis by Wang et al highlighted a particular association between circumferential enhancement and rupture in small aneurysms (< 7 mm).[17] Given that the mean aneurysm size in our study was 6.14 mm, the findings regarding enhancement patterns are especially pertinent for this size group. The correlation between circumferential enhancement and rupture risk in small aneurysms further underscores the value of vessel wall enhancement in evaluating rupture risk, even for smaller aneurysms that might otherwise be considered lower risk based solely on size.
There were a few limitations of our study. With only 60 patients, the sample size limits the generalizability of the findings. Larger studies are needed to validate these results. While the study focuses on qualitative assessments of wall enhancement, it does not incorporate quantitative measures, which could have provided more precise and reproducible data. A size-wise subgroup analysis was not performed in view of small aneurysm numbers in each size category. However, only 20% of the aneurysms were larger than 10 mm. Long-term follow-up of the patients with intracranial aneurysms may help in understanding the changes in enhancement pattern and morphology of aneurysm, which in turn may help in identifying aneurysms with high risk of rupture.
Conclusion
This study provides compelling evidence for the value of vessel wall enhancement as an imaging biomarker in the assessment of intracranial aneurysms. Vessel wall enhancement was observed in all ruptured aneurysms, thus suggesting a potential role of inflammation in the disruption of aneurysm wall integrity. The strong association between enhancement and rupture status, along with its relationships to other established risk factors, suggests that wall enhancement could play a crucial role in risk stratification, particularly for unruptured aneurysms. However, further research is needed to standardize assessment methods, particularly in quantitative measures, and to validate the predictive value of wall enhancement through larger prospective studies.
Conflict of Interest
None declared.
Note
This study has not been presented at any previous meeting or conference.
-
References
- 1 Xu Z, Rui Y-N, Hagan JP, Kim DH. Intracranial aneurysms: pathology, genetics, and molecular mechanisms. Neuromolecular Med 2019; 21 (04) 325-343
- 2 Merritt WC, Berns HF, Ducruet AF, Becker TA. Definitions of intracranial aneurysm size and morphology: a call for standardization. Surg Neurol Int 2021; 12: 506
- 3 Alg VS, Sofat R, Houlden H, Werring DJ. Genetic risk factors for intracranial aneurysms: a meta-analysis in more than 116,000 individuals. Neurology 2013; 80 (23) 2154-2165
- 4 Bakker MK, Ruigrok YM. Genetics of intracranial aneurysms. Stroke 2021; 52 (09) 3004-3012
- 5 Kleinloog R, de Mul N, Verweij BH, Post JA, Rinkel GJE, Ruigrok YM. Risk factors for intracranial aneurysm rupture: a systematic review. Neurosurgery 2018; 82 (04) 431-440
- 6 Wang H, Wang L, Wang J, Zhang L, Li C. The biological effects of smoking on the formation and rupture of intracranial aneurysms: a systematic review and meta-analysis. Front Neurol 2022; 13: 862916
- 7 Zhao L, Cheng C, Peng L. et al. Alcohol abuse associated with increased risk of angiographic vasospasm and delayed cerebral ischemia in patients with aneurysmal subarachnoid hemorrhage requiring mechanical ventilation. Front Cardiovasc Med 2022; 9: 825890
- 8 Khatri GD, Sarikaya B, Cross NM, Medverd JR. The role of imaging in the management of non-traumatic subarachnoid hemorrhage: a practical review. Emerg Radiol 2021; 28 (04) 797-808
- 9 Kato Y, Sano H, Katada K. et al. Application of three-dimensional CT angiography (3D-CTA) to cerebral aneurysms. Surg Neurol 1999; 52 (02) 113-121 , discussion 121–122
- 10 van Rooij WJ, Sprengers ME, de Gast AN, Peluso JP, Sluzewski M. 3D rotational angiography: the new gold standard in the detection of additional intracranial aneurysms. AJNR Am J Neuroradiol 2008; 29 (05) 976-979
- 11 Santarosa C, Cord B, Koo A. et al. Vessel wall magnetic resonance imaging in intracranial aneurysms: principles and emerging clinical applications. Interv Neuroradiol 2020; 26 (02) 135-146
- 12 Lehman VT, Brinjikji W, Mossa-Basha M. et al. Conventional and high-resolution vessel wall MRI of intracranial aneurysms: current concepts and new horizons. J Neurosurg 2018; 128 (04) 969-981
- 13 Sanchez S, Hickerson M, Patel RR. et al. Morphological characteristics of ruptured brain aneurysms: a systematic literature review and meta-analysis. Stroke Vasc Intervent Neurol 2023; 3 (02) e000707
- 14 Park HS, Kwon SC, Park ES, Park JB, Kim MS. A new definition for wide-necked cerebral aneurysms. J Cerebrovasc Endovasc Neurosurg 2019; 21 (04) 193-198
- 15 Nagahata S, Nagahata M, Obara M. et al. Wall enhancement of the intracranial aneurysms revealed by magnetic resonance vessel wall imaging using three-dimensional turbo spin-echo sequence with motion-sensitized driven-equilibrium: a sign of ruptured aneurysm?. Clin Neuroradiol 2016; 26 (03) 277-283
- 16 Edjlali M, Gentric J-C, Régent-Rodriguez C. et al. Does aneurysmal wall enhancement on vessel wall MRI help to distinguish stable from unstable intracranial aneurysms?. Stroke 2014; 45 (12) 3704-3706
- 17 Wang X, Zhu C, Leng Y, Degnan AJ, Lu J. Intracranial aneurysm wall enhancement associated with aneurysm rupture: a systematic review and meta-analysis. Acad Radiol 2019; 26 (05) 664-673
- 18 Fu Q, Wang Y, Zhang Y. et al. Qualitative and quantitative wall enhancement on magnetic resonance imaging is associated with symptoms of unruptured intracranial aneurysms. Stroke 2021; 52 (01) 213-222
- 19 Xu G, Luo N, Deng Y. Qualitative and quantitative wall enhancement associated with unstable intracranial aneurysms: a meta-analysis. Acta Radiol 2023; 64 (05) 1974-1984
- 20 Fu Q, Guan S, Liu C, Wang K, Cheng J. Clinical significance of circumferential aneurysmal wall enhancement in symptomatic patients with unruptured intracranial aneurysms: a high-resolution MRI study. Clin Neuroradiol 2018; 28 (04) 509-514
- 21 Lv N, Tang H, Chen S. et al. Morphological parameters related to aneurysm wall enhancement in patients with multiple intracranial aneurysms. World Neurosurg 2018; 114: e338-e343
- 22 Lv N, Karmonik C, Chen S. et al. Relationship between aneurysm wall enhancement in vessel wall magnetic resonance imaging and rupture risk of unruptured intracranial aneurysms. Neurosurgery 2019; 84 (06) E385-E391
- 23 Wu XB, Zhong JL, Wang SW. et al. Circumferential wall enhancement with contrast ratio measurement in unruptured intracranial aneurysm for aneurysm instability. Brain Behav 2022; 12 (05) e2568
Address for correspondence
Publication History
Article published online:
04 June 2025
© 2025. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Xu Z, Rui Y-N, Hagan JP, Kim DH. Intracranial aneurysms: pathology, genetics, and molecular mechanisms. Neuromolecular Med 2019; 21 (04) 325-343
- 2 Merritt WC, Berns HF, Ducruet AF, Becker TA. Definitions of intracranial aneurysm size and morphology: a call for standardization. Surg Neurol Int 2021; 12: 506
- 3 Alg VS, Sofat R, Houlden H, Werring DJ. Genetic risk factors for intracranial aneurysms: a meta-analysis in more than 116,000 individuals. Neurology 2013; 80 (23) 2154-2165
- 4 Bakker MK, Ruigrok YM. Genetics of intracranial aneurysms. Stroke 2021; 52 (09) 3004-3012
- 5 Kleinloog R, de Mul N, Verweij BH, Post JA, Rinkel GJE, Ruigrok YM. Risk factors for intracranial aneurysm rupture: a systematic review. Neurosurgery 2018; 82 (04) 431-440
- 6 Wang H, Wang L, Wang J, Zhang L, Li C. The biological effects of smoking on the formation and rupture of intracranial aneurysms: a systematic review and meta-analysis. Front Neurol 2022; 13: 862916
- 7 Zhao L, Cheng C, Peng L. et al. Alcohol abuse associated with increased risk of angiographic vasospasm and delayed cerebral ischemia in patients with aneurysmal subarachnoid hemorrhage requiring mechanical ventilation. Front Cardiovasc Med 2022; 9: 825890
- 8 Khatri GD, Sarikaya B, Cross NM, Medverd JR. The role of imaging in the management of non-traumatic subarachnoid hemorrhage: a practical review. Emerg Radiol 2021; 28 (04) 797-808
- 9 Kato Y, Sano H, Katada K. et al. Application of three-dimensional CT angiography (3D-CTA) to cerebral aneurysms. Surg Neurol 1999; 52 (02) 113-121 , discussion 121–122
- 10 van Rooij WJ, Sprengers ME, de Gast AN, Peluso JP, Sluzewski M. 3D rotational angiography: the new gold standard in the detection of additional intracranial aneurysms. AJNR Am J Neuroradiol 2008; 29 (05) 976-979
- 11 Santarosa C, Cord B, Koo A. et al. Vessel wall magnetic resonance imaging in intracranial aneurysms: principles and emerging clinical applications. Interv Neuroradiol 2020; 26 (02) 135-146
- 12 Lehman VT, Brinjikji W, Mossa-Basha M. et al. Conventional and high-resolution vessel wall MRI of intracranial aneurysms: current concepts and new horizons. J Neurosurg 2018; 128 (04) 969-981
- 13 Sanchez S, Hickerson M, Patel RR. et al. Morphological characteristics of ruptured brain aneurysms: a systematic literature review and meta-analysis. Stroke Vasc Intervent Neurol 2023; 3 (02) e000707
- 14 Park HS, Kwon SC, Park ES, Park JB, Kim MS. A new definition for wide-necked cerebral aneurysms. J Cerebrovasc Endovasc Neurosurg 2019; 21 (04) 193-198
- 15 Nagahata S, Nagahata M, Obara M. et al. Wall enhancement of the intracranial aneurysms revealed by magnetic resonance vessel wall imaging using three-dimensional turbo spin-echo sequence with motion-sensitized driven-equilibrium: a sign of ruptured aneurysm?. Clin Neuroradiol 2016; 26 (03) 277-283
- 16 Edjlali M, Gentric J-C, Régent-Rodriguez C. et al. Does aneurysmal wall enhancement on vessel wall MRI help to distinguish stable from unstable intracranial aneurysms?. Stroke 2014; 45 (12) 3704-3706
- 17 Wang X, Zhu C, Leng Y, Degnan AJ, Lu J. Intracranial aneurysm wall enhancement associated with aneurysm rupture: a systematic review and meta-analysis. Acad Radiol 2019; 26 (05) 664-673
- 18 Fu Q, Wang Y, Zhang Y. et al. Qualitative and quantitative wall enhancement on magnetic resonance imaging is associated with symptoms of unruptured intracranial aneurysms. Stroke 2021; 52 (01) 213-222
- 19 Xu G, Luo N, Deng Y. Qualitative and quantitative wall enhancement associated with unstable intracranial aneurysms: a meta-analysis. Acta Radiol 2023; 64 (05) 1974-1984
- 20 Fu Q, Guan S, Liu C, Wang K, Cheng J. Clinical significance of circumferential aneurysmal wall enhancement in symptomatic patients with unruptured intracranial aneurysms: a high-resolution MRI study. Clin Neuroradiol 2018; 28 (04) 509-514
- 21 Lv N, Tang H, Chen S. et al. Morphological parameters related to aneurysm wall enhancement in patients with multiple intracranial aneurysms. World Neurosurg 2018; 114: e338-e343
- 22 Lv N, Karmonik C, Chen S. et al. Relationship between aneurysm wall enhancement in vessel wall magnetic resonance imaging and rupture risk of unruptured intracranial aneurysms. Neurosurgery 2019; 84 (06) E385-E391
- 23 Wu XB, Zhong JL, Wang SW. et al. Circumferential wall enhancement with contrast ratio measurement in unruptured intracranial aneurysm for aneurysm instability. Brain Behav 2022; 12 (05) e2568