
Subscribe to RSS
DOI: 10.1055/s-0045-1806941
Percutaneous Transsplenic Balloon-Assisted Transjugular Intrahepatic Portosystemic Shunt Placement for Chronic Noncirrhotic Obliterative Portal Vein Thrombus
Funding None.


Abstract
Portal vein recanalization-transjugular intrahepatic portosystemic shunt (PVR-TIPS) has become an accepted minimally invasive therapeutic option for alleviating symptoms of portal hypertension refractory to medical and endoscopic therapy in patients with chronic portal vein thrombosis. The transsplenic approach for PVR-TIPS has shown excellent results with acceptable complication rates. Traditionally, endovascular snares are used as fluoroscopic target for accessing the recanalized portal vein from the hepatic vein. Here, we report our experience with contrast-filled balloon catheter as a fluoroscopic target for the same in a noncirrhotic patient with extrahepatic portal venous obstruction and recurrent variceal bleeding.
Introduction
Chronic noncirrhotic obliterative portal vein obstruction, also known as extrahepatic portal vein obstruction (EHPVO), is an important cause of prehepatic portal hypertension.[1] Recurrent, well-tolerated episodes of variceal bleeding are the usual presentation.[1] In patients not responding to medical and endoscopic management, portal vein recanalization with or without transjugular intrahepatic portosystemic shunt (PVR-TIPS) has become an accepted minimally invasive alternative therapeutic option that has found its way into recent guidelines as well.[2] Since the conventional approach to TIPS often fails in these cases, transsplenic antegrade recanalization of the portal vein has become the preferred technique.[3] Traditionally, endovascular snares introduced via transsplenic access are used as the fluoroscopic target for puncturing the recanalized portal vein from the transjugular route.[3] One disadvantage of this method is that the snare may not fully open in a diminutive or partially thrombosed portal vein. Some recent studies have described the use of contrast-filled balloons for the same purpose, instead of a snare.[4] [5] Herein, we describe our technique of balloon-assisted transsplenic PVR-TIPS.
Case Report
A 44-year-old gentleman presented to our outpatient department with a history of multiple episodes of upper gastrointestinal bleeding in the form of hematemesis and melena for the past 12 years for which repeated sessions of endoscopic variceal ligation had been done elsewhere. He was diagnosed to have EHPVO during his index presentation at the outside institute based on imaging findings. At presentation to us, he appeared malnourished and cachexic and complained of constant fatigue and palpitations.
Basic laboratory investigations revealed a hemoglobin level of 5.6 g/dL and a total count of 7,500 cells/mm3. The rest of the investigations including renal and liver function tests were within normal limits. Upper gastrointestinal endoscopy showed large esophageal varices.
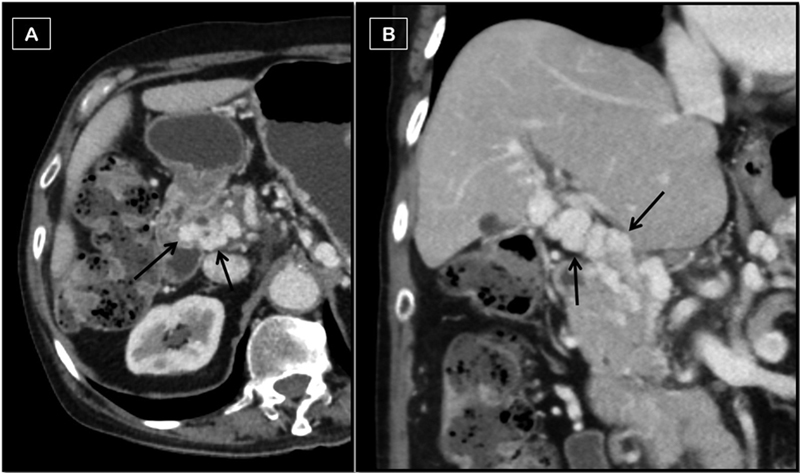
A contrast-enhanced computed tomography (CT) study revealed a completely obliterated native main portal vein, which could not be made out separately from multiple periportal collaterals ([Fig. 1]). The splenic and superior mesenteric veins were patent.
To ascertain the cause of EHPVO, hematological workup was done, including factor V Leiden mutation, JAK2 mutation, and protein C and protein S. However, all the tests were negative or within normal limits. The patient refused bone marrow biopsy, which was suggested to rule out myeloproliferative neoplasms.
TIPS was attempted elsewhere from the conventional transjugular approach but failed as the native portal vein could not be accessed. Hence, after a multidisciplinary team meeting, PVR-TIPS from the transsplenic approach was planned for secondary prophylaxis of variceal bleeding.
Technique
The procedure was done under general anesthesia with the patient in the supine position. One of the intraparenchymal branches of the splenic vein was accessed using the Neff percutaneous access set (Cook Medical, Bloomington, IN, United States) and a 5-Fr, 11-cm vascular access sheath (Avanti, Cordis, Miami Lakes, FL, United States) was placed. A combination of 5-Fr Kumpe catheter (Cook Medical) and a 0.035-inch hydrophilic guidewire (Radifocus, Terumo Corporation, Tokyo, Japan) was now used to advance further within the splenic vein toward the cavernoma and intermittent venograms taken to serve as a roadmap ([Fig. 2]). One of the venograms revealed an attenuated straight vascular channel going toward the hepatic hilum, which corroborated with the expected position of the native portal vein on CT images ([Fig. 3]). This vein was now cannulated with the help of a 5-Fr Cobra catheter (C2, Cook Medical) and the anterior segmental branch of the right portal vein was identified ([Fig. 4]). The hydrophilic guidewire was now exchanged for a 260-cm, 0.035-inch Amplatz Ultrastiff guidewire (Cook Medical) and the C2 catheter removed. Over the Amplatz guidewire, an 8 × 40 mm sized balloon catheter (Mustang, Boston Scientific, United States) was threaded into the right anterior segmental portal venous branch and inflated with contrast media to serve as a target for puncture from the transjugular approach.



The right internal jugular vein was now accessed using the standard technique and a 10-Fr, 11-cm vascular access sheath was placed (Avanti, Cordis). The right hepatic vein was then cannulated and the 10-Fr short sheath exchanged for the Rösch-Uchida Transjugular Liver Access set (RUPS-100, Cook Medical) over the ultrastiff guidewire. This was followed by introduction of the trocar stylet and catheter set from RUPS-100. The stiffening cannula was now rotated anticlockwise so that it wedges against the right hepatic venous wall and gets directed toward the balloon. Under combined ultrasound and fluoroscopic guidance, the trocar stylet and catheter set was now advanced to puncture the contrast-filled balloon catheter. Balloon puncture was confirmed on fluoroscopy by indentation over the balloon by the advancing trocar stylet followed by a sudden loss of resistance and leakage of contrast from the balloon into the portal vein ([Fig. 5]). At this point, the trocar stylet was unscrewed and removed while keeping the 5-Fr catheter in place. A 0.035-inch, 260-cm hydrophilic guidewire (Radifocus, Terumo) was then passed through the 5-Fr catheter into the partially collapsed balloon and allowed to coil within it. This was followed by simultaneous advancement of the guidewire from the jugular end and withdrawal of the balloon catheter from the splenic end under continuous fluoroscopic guidance in such a way that the guidewire advances into the main portal vein and then into the splenic vein ([Fig. 6]). The 5-Fr catheter was now replaced with a multipurpose angiographic (MPA) catheter, which was advanced into the splenic vein over the guidewire. The balloon catheter was now removed and a venogram taken from the MPA catheter to confirm its position. The rest of the steps were the same as those of the standard TIPS procedure. A hybrid TIPS stent (Niti, Taewoong, South Korea) with a graft length of 10 cm was finally placed with its upper end at the right hepatic vein–inferior vena cava junction and lower end at the splenoportal confluence ([Fig. 7]). The splenic parenchymal tract was closed with two pushable coils of 4-mm diameter. Anticoagulation with unfractionated heparin was initiated during the procedure, which was changed to low-molecular-weight heparin to prevent thrombotic stent occlusion. He was started on apixaban at a dose of 2.5 mg twice daily at discharge and was asked to come for follow-up every 3 months for Doppler study and laboratory investigations. He has completed 18 months of follow-up and remains asymptomatic.



Discussion
In patients with EHPVO and patent splenic vein, the transsplenic approach has become the preferred option for creating a TIPS to alleviate portal hypertension.[3] Through the antegrade approach via the splenic vein, the thrombosed and often fibrotic, thread-like native portal vein can be accessed and recanalized.[3] After recanalization of the main portal vein, puncture from the hepatic vein to the portal vein with a TIPS needle must be performed. Traditionally, this critical step is performed using an endovascular snare as the fluoroscopic target.[3] The biggest advantage of using a snare is that the operator can grasp the wire and pull it through the splenic route, thus establishing a stable through-and-through access for the remainder of the case. However, one practical disadvantage of the snare technique is that the snare may not fully open in a small or thrombosed intrahepatic portal vein, making the puncture difficult. Use of contrast-filled balloons introduced via a splenic access as an alternative target was proposed by Jeong et al in a case report and has shown reasonably good results in a subsequent larger case series.[4] [5] Since the balloon provides a visual and haptic feedback while puncturing, overall procedural fluoroscopic time has been reported to be lesser than that for the snare-assisted technique.[5] By using additional transabdominal ultrasound guidance, radiation exposure can be further reduced, as demonstrated by our case.
In conclusion, percutaneous transsplenic balloon-assisted PVR-TIPS is a feasible, safe, and effective technique in patients with EHPVO and has the potential to improve the long-term outcomes of these patients.
Conflict of Interest
None declared.
-
References
- 1 Khanna R, Sarin SK. Non-cirrhotic portal hypertension: diagnosis and management. J Hepatol 2014; 60 (02) 421-441
- 2 de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C. Baveno VII Faculty. Baveno VII: renewing consensus in portal hypertension. J Hepatol 2022; 76 (04) 959-974
- 3 Swersky A, Borja-Cacho D, Deitch Z, Thornburg B, Salem R. Portal vein recanalization-transjugular intrahepatic portosystemic shunt (PVR-TIPS) facilitates liver transplantation in cirrhotic patients with occlusive portal vein thrombosis. Semin Intervent Radiol 2023; 40 (01) 38-43
- 4 Jeong SY, Park AW, Wilkins L. Transjugular intrahepatic portosystemic shunt using transsplenic access with balloon-assisted puncture technique in a patient with chronic and complete occlusion of portal vein. Int J Gastrointest Interv 2015; 4: 127-129
- 5 Meine TC, Becker LS, Dewald CLA. et al. Percutaneous transsplenic balloon-assisted transjugular intrahepatic portosystemic shunt placement in patients with portal vein obliteration for portal vein recanalization: feasibility, safety and effectiveness. Cardiovasc Intervent Radiol 2022; 45 (05) 696-702
Address for correspondence
Publication History
Article published online:
28 March 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Khanna R, Sarin SK. Non-cirrhotic portal hypertension: diagnosis and management. J Hepatol 2014; 60 (02) 421-441
- 2 de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C. Baveno VII Faculty. Baveno VII: renewing consensus in portal hypertension. J Hepatol 2022; 76 (04) 959-974
- 3 Swersky A, Borja-Cacho D, Deitch Z, Thornburg B, Salem R. Portal vein recanalization-transjugular intrahepatic portosystemic shunt (PVR-TIPS) facilitates liver transplantation in cirrhotic patients with occlusive portal vein thrombosis. Semin Intervent Radiol 2023; 40 (01) 38-43
- 4 Jeong SY, Park AW, Wilkins L. Transjugular intrahepatic portosystemic shunt using transsplenic access with balloon-assisted puncture technique in a patient with chronic and complete occlusion of portal vein. Int J Gastrointest Interv 2015; 4: 127-129
- 5 Meine TC, Becker LS, Dewald CLA. et al. Percutaneous transsplenic balloon-assisted transjugular intrahepatic portosystemic shunt placement in patients with portal vein obliteration for portal vein recanalization: feasibility, safety and effectiveness. Cardiovasc Intervent Radiol 2022; 45 (05) 696-702