

Subscribe to RSS
DOI: 10.1055/s-0045-1804498
A Delayed Post-COVID-19 Silent Thyroiditis
Authors
Funding None.

Abstract
Background
Although respiratory symptoms are the predominant manifestations of coronavirus disease 2019 (COVID-19) infection, thyroid dysfunction is a commonly recognized sequela. We report a case of delayed silent thyroiditis that manifested 3 months following COVID-19 infection in a 14-year-old female.
Case Description
A 14-year-old female presented with palpitations, tremors, and sweating that started around 3 months after the resolution of COVID-19 infection.
Her presentation, thyroid function tests, along with ultrasonographic pictures and radioiodine uptake scan of the thyroid were consistent with a diagnosis of silent thyroiditis. She was managed symptomatically with propranolol, after which her symptoms improved, and thyroid function tests returned to normal.
Conclusion
COVID-19 is a possible trigger for delayed silent thyroiditis that health care providers should recognize for accurate diagnosis and management.
Introduction
In January of 2020, the World Health Organization declared the coronavirus disease 2019 (COVID-19) outbreak a “health emergency of international concern.”[1] Thus far, the virus caused an unparalleled global health crisis, with over 2 million deaths reported worldwide.[2] COVID-19 infection has a versatile spectrum of clinical presentations ranging from asymptomatic infection to death due to respiratory failure.[3]
Much remains to be understood about the complete range of impacts of COVID-19 on autoimmune endocrine diseases. However, a growing number of reports indicate the involvement of the endocrine system.[4] Here, we present a case of silent thyroiditis in a 14-year-old female following a COVID-19 infection.
Case Description
A previously healthy 14-year-old female was referred to the endocrinology outpatient clinic due to grossly abnormal thyroid function tests (TFTs) associated with tremors, palpitations, sweating, and chest pain of 3 months duration. Upon further questioning, the history revealed that the patient's symptoms started approximately 3 months after contracting a COVID-19 infection, which presented with mild flu-like symptoms and fever. Infection was confirmed by polymerase chain reaction (PCR) testing and its symptoms resolved promptly within a few days. Following the resolution of COVID-19 symptoms, the patient did not experience any other respiratory illnesses or symptoms. The patient did not receive any COVID-19 vaccines during this time either. Her family history was negative for any thyroid illnesses.
General physical examination revealed an anxious female who was conscious, alert, and oriented. She was afebrile, with a blood pressure of 129/73 mm Hg, tachycardic with a heart rate of 106 beats per minute, and a respiratory rate of 18 breaths per minute. Examination of the neck revealed a nonenlarged, smooth, soft, nontender neck with no associated lymphadenopathy. General examination revealed no signs of thyroid eye disease.
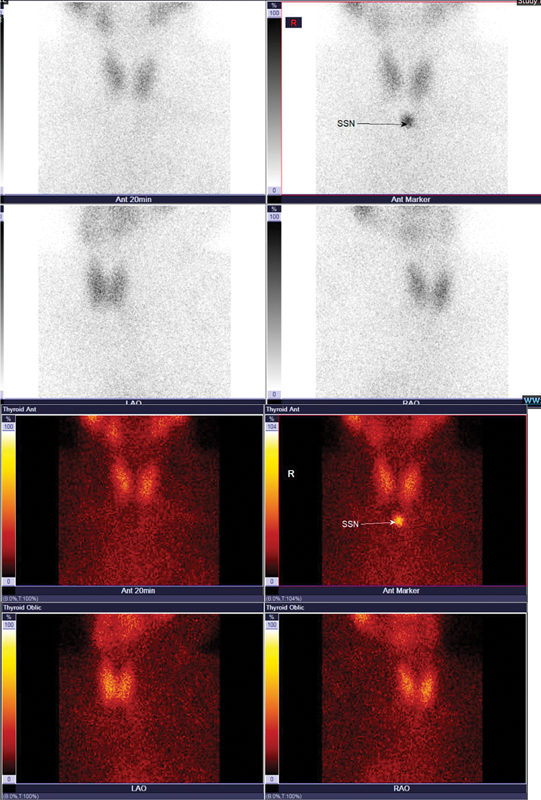
Laboratory investigations revealed a suppressed thyroid-stimulating hormone (TSH) level, elevated free T4 and free T3, along with negative thyroid peroxidase antibody, and negative thyroid-stimulating immunoglobulin ([Table 1]). Ultrasound of the neck ([Fig. 1]) revealed an inhomogeneous thyroid gland with two small subcentimetric hypoechoic solid nodules in the left thyroid lobe and isthmus. A radioiodine uptake scan ([Fig. 2]), done 3 weeks after the initial presentation to the clinic, revealed a mildly enlarged thyroid gland with homogeneous low normal radiotracer uptake of 0.5% (normal being 0.3–3.33%), a picture suggestive of resolving thyroiditis. The reason for the delay in the radioiodine uptake imaging study was related to logistics as the scan was not available in our facility. The patient was initiated on propranolol 10 mg three times a day and was given a 4-week follow-up visit in the endocrine outpatient clinic.

Abbreviations: TPO, thyroid peroxidase; TSH, thyroid-stimulating hormone.
Within 2 weeks of initiating therapy, the patient experienced an acute worsening of symptoms despite compliance with medications. The patient developed recurrent palpitations, episodes of profuse sweating, and tremors, prompting her to present to the emergency department. She was found to be tachycardic, an electrocardiogram showed sinus tachycardia and lab results revealed an even higher thyroid hormone levels with further suppression of TSH ([Table 2]). After symptomatic treatment of intravenous metoprolol to manage the tachycardia, she was discharged and advised to follow-up sooner with her endocrinologist.
Abbreviations: ED, emergency department; TFT, thyroid function test; TSH, thyroid-stimulating hormone.
Subsequently, after a few weeks, follow-up TFTs revealed a hypothyroid picture ([Table 2]) and thus the medications were discontinued. The patient was advised to follow-up regularly to monitor TFTs. Eventually, after multiple follow-up clinic visits, the final TFT revealed the normalization of all values ([Table 2]).
Discussion
COVID-19 was primarily considered a respiratory illness caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus. It is known to affect the respiratory system, leading to symptoms such as cough, fever, and difficulty breathing. However, it is true that over time, researchers have observed that COVID-19 can have systemic effects, impacting various organs and systems beyond the respiratory system. The development of a COVID-19 infection begins when the virus enters the body through the respiratory system and settles in the lung parenchyma. The virus then uses angiotensin-converting enzyme 2 (ACE2) as a receptor to invade the host's lung cells. Additionally, viral ribonucleic acid has been found in the plasma of COVID-19 patients, indicating viremia. This suggests that, beyond lung cells, the virus can interact with ACE2 present in other tissues, namely, several endocrine organs, including the pancreas, thyroid, testis, ovary, adrenal glands, and pituitary. Although one might anticipate potential endocrine effects due to SARS-CoV-2's interaction with ACE2 in these organs, there is currently no data to confirm this.[5] [6]
Thyroiditis is often associated with viral infections, such as the mumps virus, Coxsackievirus, and, in some cases, respiratory viruses such as COVID-19 infection.[7] It is characterized by an inflammation of the thyroid gland with the release of preformed thyroid hormones, most commonly occurring in female patients during or after viral infection. Both silent and subacute thyroiditis following SARS-CoV-2 infection have been reported in the literature. Subacute thyroiditis and silent thyroiditis are characterized by the recent onset of symptoms in a patient with a normal to fairly enlarged thyroid gland along with a markedly reduced radioiodine uptake. However, the distinguishing feature between the two conditions is the absence of thyroid pain or tenderness, as well as the lack of systemic manifestations such as fever or myalgia.[8] The patient we describe did not complain of any neck pain, and had a nontender thyroid upon examination, making the diagnosis of silent thyroiditis more likely. While there are no known pathogenetic factors, the disease is thought to have an autoimmune basis,[8] which in this case seems to reflect a delayed reaction to the COVID-19 infection.
While we acknowledge that the absence of a documented viral screen in our report may raise questions about the exclusion of other viral etiologies, but the patient presented to our facility with symptoms approximately 3 months after a confirmed COVID-19 infection, diagnosed via PCR testing. During this period, the patient did not experience symptoms of other infections, and there was no clinical evidence suggesting concurrent or subsequent viral illnesses. While a viral screen could provide additional clarity, the timing of the patient's thyroid dysfunction relative to the resolution of COVID-19 symptoms strongly suggests a post-COVID etiology. Silent thyroiditis in this context has been increasingly recognized as a sequela of SARS-CoV-2 infection, as highlighted by emerging literature.
A review of the literature highlights the uniqueness of this case. While silent thyroiditis has been documented in a 48-year-old male occurring 3 weeks after a COVID-19 infection,[9] our patient is significantly younger and exhibited a delayed presentation of silent thyroiditis. Numerous case reports have described instances of silent thyroiditis and subacute thyroiditis following COVID-19 vaccinations,[10] [11] typically presenting 2 to 4 weeks postvaccination; however, our patient had not received the vaccine during that time. One case featured a 16-year-old male presenting primarily with psychiatric symptoms,[12] but although our patient is of a similar age, she displayed more typical symptoms such as tremors, sweating, and palpitations. It is also noteworthy that silent thyroiditis is observed more frequently in the postpartum period, which was not the case for our patient. While there are reports of cases in the literature describing silent thyroiditis in nonpostpartum patients, particularly after a COVID infection, most reported cases involve older males, with symptoms appearing within 2 to 6 weeks after the triggering event. What adds interest to our case is the delayed onset of her symptoms, where the symptoms developed 3 months after the viral illness in a young female patient.
Conclusion
Silent thyroiditis should be identified as one of the potentially late presenting extrapulmonary manifestations and sequelae of COVID-19 infection. Its early identification allows clinicians to manage and reassure their patients accordingly. Meanwhile, this case report emphasizes the importance of asking about history of infections especially with COVID-19 in patients presenting with thyroid dysfunction symptoms.
Conflict of Interest
None declared.
Authors' Contribution
All the authors contributed to the drafting and revising of the manuscript and approved its final version.
Confirmation of Consent for Publications
The authors confirm that they have obtained the consent of the patient's guardian for publication of the case report on a totally anonymous basis.
Compliance with Ethical Principles
Approval of the institutional review board is not required for single case reports or small case series provided patients give consent and reporting is completely anonymous.
-
References
- 1 Li L, Qin L, Xu Z. et al. Using artificial intelligence to detect COVID-19 and community-acquired pneumonia based on pulmonary CT: evaluation of the diagnostic accuracy. Radiology 2020; 296 (02) E65-E71
- 2 Lodigiani C, Iapichino G, Carenzo L. et al; Humanitas COVID-19 Task Force. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res 2020; 191: 9-14
- 3 Huang C, Wang Y, Li X. et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395 (10223): 497-506
- 4 Dworakowska D, Grossman AB. Thyroid disease in the time of COVID-19. Endocrine 2020; 68 (03) 471-474
- 5 Liu F, Long X, Zhang B, Zhang W, Chen X, Zhang Z. ACE2 expression in pancreas may cause pancreatic damage after SARS-CoV-2 infection. Clin Gastroenterol Hepatol 2020; 18 (09) 2128-2130.e2
- 6 Li MY, Li L, Zhang Y, Wang XS. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect Dis Poverty 2020; 9 (01) 45
- 7 Trimboli P, Cappelli C, Croce L, Scappaticcio L, Chiovato L, Rotondi M. COVID-19-associated subacute thyroiditis: evidence-based data from a systematic review. Front Endocrinol (Lausanne) 2021; 12: 707726
- 8 Walker P. Silent thyroiditis. Can Fam Physician 1984; 30: 1337-1339
- 9 Quaytman J, Gollamudi U, Bass N, Suresh S. Reactive arthritis and silent thyroiditis following SARS-CoV-2 infection: case report and review of the literature. Clin Case Rep 2022; 10 (02) e05430
- 10 Capezzone M, Tosti-Balducci M, Morabito EM. et al. Silent thyroiditis following vaccination against COVID-19: report of two cases. J Endocrinol Invest 2022; 45 (05) 1079-1083
- 11 Bornemann C, Woyk K, Bouter C. Two cases of subacute thyroiditis following SARS-COV-2 vaccination. Front Med (Lausanne) 2021; 8: 737142
- 12 Furuta Y, Masuoka T, Narishige R, Tateno A. Delayed diagnosis of painless thyroiditis in an adolescent presenting with aggression and disruptive behavior initially attributed to worsening of a psychiatric disorder. J Nippon Med Sch 2024; ;•••:
Address for correspondence
Publication History
Article published online:
09 April 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Li L, Qin L, Xu Z. et al. Using artificial intelligence to detect COVID-19 and community-acquired pneumonia based on pulmonary CT: evaluation of the diagnostic accuracy. Radiology 2020; 296 (02) E65-E71
- 2 Lodigiani C, Iapichino G, Carenzo L. et al; Humanitas COVID-19 Task Force. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res 2020; 191: 9-14
- 3 Huang C, Wang Y, Li X. et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395 (10223): 497-506
- 4 Dworakowska D, Grossman AB. Thyroid disease in the time of COVID-19. Endocrine 2020; 68 (03) 471-474
- 5 Liu F, Long X, Zhang B, Zhang W, Chen X, Zhang Z. ACE2 expression in pancreas may cause pancreatic damage after SARS-CoV-2 infection. Clin Gastroenterol Hepatol 2020; 18 (09) 2128-2130.e2
- 6 Li MY, Li L, Zhang Y, Wang XS. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect Dis Poverty 2020; 9 (01) 45
- 7 Trimboli P, Cappelli C, Croce L, Scappaticcio L, Chiovato L, Rotondi M. COVID-19-associated subacute thyroiditis: evidence-based data from a systematic review. Front Endocrinol (Lausanne) 2021; 12: 707726
- 8 Walker P. Silent thyroiditis. Can Fam Physician 1984; 30: 1337-1339
- 9 Quaytman J, Gollamudi U, Bass N, Suresh S. Reactive arthritis and silent thyroiditis following SARS-CoV-2 infection: case report and review of the literature. Clin Case Rep 2022; 10 (02) e05430
- 10 Capezzone M, Tosti-Balducci M, Morabito EM. et al. Silent thyroiditis following vaccination against COVID-19: report of two cases. J Endocrinol Invest 2022; 45 (05) 1079-1083
- 11 Bornemann C, Woyk K, Bouter C. Two cases of subacute thyroiditis following SARS-COV-2 vaccination. Front Med (Lausanne) 2021; 8: 737142
- 12 Furuta Y, Masuoka T, Narishige R, Tateno A. Delayed diagnosis of painless thyroiditis in an adolescent presenting with aggression and disruptive behavior initially attributed to worsening of a psychiatric disorder. J Nippon Med Sch 2024; ;•••: