
RSS-Feed abonnieren
DOI: 10.1055/s-0045-1803580
Results in the Endoscopic Management of Tuberculum Sellae and Planum Sphenoidale Meningiomas: Experience of Two Specialized Teams

Objective: Tuberculum sellae and planum sphenoidale meningiomas (TSM, PSM) are rare anterior skull base lesions, traditionally treated through various transcranial approaches. Recently, the extended endoscopic endonasal approach (EEA) has become an alternative for resection, offering early lesion devascularization and wide optic canals decompression, while avoiding brain manipulation. We present a 13-year retrospective, double-institutional experience using extended EEA approach, discussing the impact of tumor size, optic canal involvement, vascular encasement, and tumor consistency on TSM and PSM resection.
Methods: This collaborative study analyzed patients, who underwent extended EEA surgery for TSMs or PSMs removal between 2010 and 2022. Conducted by the Naples team at Division of Neurosurgery, Università degli Studi di Napoli Federico II, Italy, and the Columbus team at Department of Neurological Surgery, The Ohio State University Wexner Medical Center, USA, the study evaluated demographic data, preoperative assessments, tumor features, prior treatments, surgical results, complications, follow-up, and recurrence. Meningiomas were also categorized using the Sekhar-Mortazavi classification.
Results: A total of 95 patients (71 with TSM and 24 with PSM) were included. Visual impairment was the most common symptom at presentation, occurring in 83% (n:79) of patients. Among those with TSMs, 62 patients had visual deficits, with 52 of them having optic canal involvement. For PSMs, visual symptoms and headache were onset symptom in 20 patients, with optic canal involvement in 13. Based on the Sekhar-Mortazavi classification, 86 meningiomas were categorized into three classes. We enrolled 54 class I tumors, 31 class II, and 1 class III tumor. Gross-total resection (GTR) was achieved in 77.8% (n:74) of cases, reaching 81.8% for class I tumors. GTR rates were inversely proportional to tumor size, visual pathway involvement and vascular encasement. Moreover, fibrous and fibro-elastic consistencies were strongly related to a lower rate of resection. A decreasing trend in CSF leak was observed, from 32% in 2010 to 2014 to 10% in 2018 to 2022. Vision function improved in 75.9% (n:60) of patients. The overall rate of endocrinological issues (SIADH/DI) was 4.2%.
Conclusion: The extended EEA is a secure and efficient method for removing TSMs and PSMs, preserving vascularization of the optic apparatus while facilitating gross-total resection and enhancing visual outcomes.



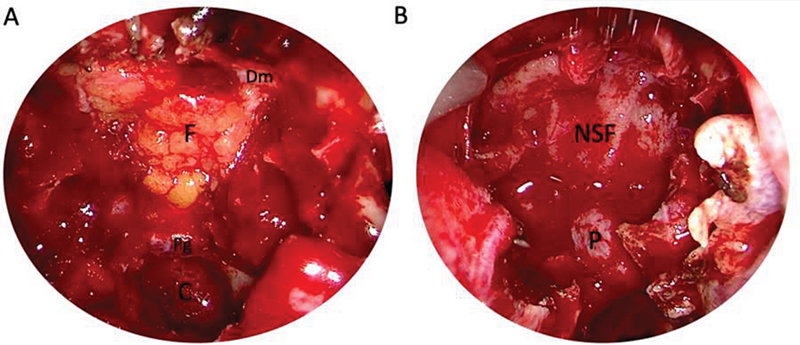
ICA, internal carotid artery; OC, optic chiasm; SHb, superior hypophyseal branches; T, tumor; FL, frontal lobe; A1/A2, precommunicating and postcommunicating anterior cerebral artery; ACoA, anterior communicating artery.
Die Autoren geben an, dass kein Interessenkonflikt besteht.
Publikationsverlauf
Artikel online veröffentlicht:
07. Februar 2025
© 2025. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany