

Subscribe to RSS
DOI: 10.1055/s-0044-1801588
Enhancing Anticoagulation Monitoring and Therapy in Patients Undergoing Microvascular Reconstruction in Maxillofacial Surgery: results from the interims analysis of the prospective study
Authors

Introduction: In reconstructive surgery, a serious complication is loss of a microvascular free flap due to perfusion disorders, especially thrombosis. In recent years, viscoelastic testing (VET) has become increasingly important in point-of-care (POC) anticoagulation monitoring. The aim of this ongoing prospective management study (planned sample size 200 pts.) is to analyze the predictive value of POC devices for flap perfusion disorders due to thrombosis or bleeding.
Method: All Patients undergoing reconstructive surgery using microvascular free flaps provide blood samples for viscoelastic testing and standard laboratory testing (SLT) at defined time points. The primary outcome is defined as free flap loss until 30 days after hospital discharge (short-term follow-up). Patient characteristics and outcomes are assessed descriptively. Correlation will be analyzed using Mann-Whitney-U test. This study was approved by the Ethics Committee of the Technical University of Dresden, Germany (BO-EK- BO-EK-22012022) and registered with German Clinical Trials Register DRKS00028193. The study is performed according to the published study protocol [1].
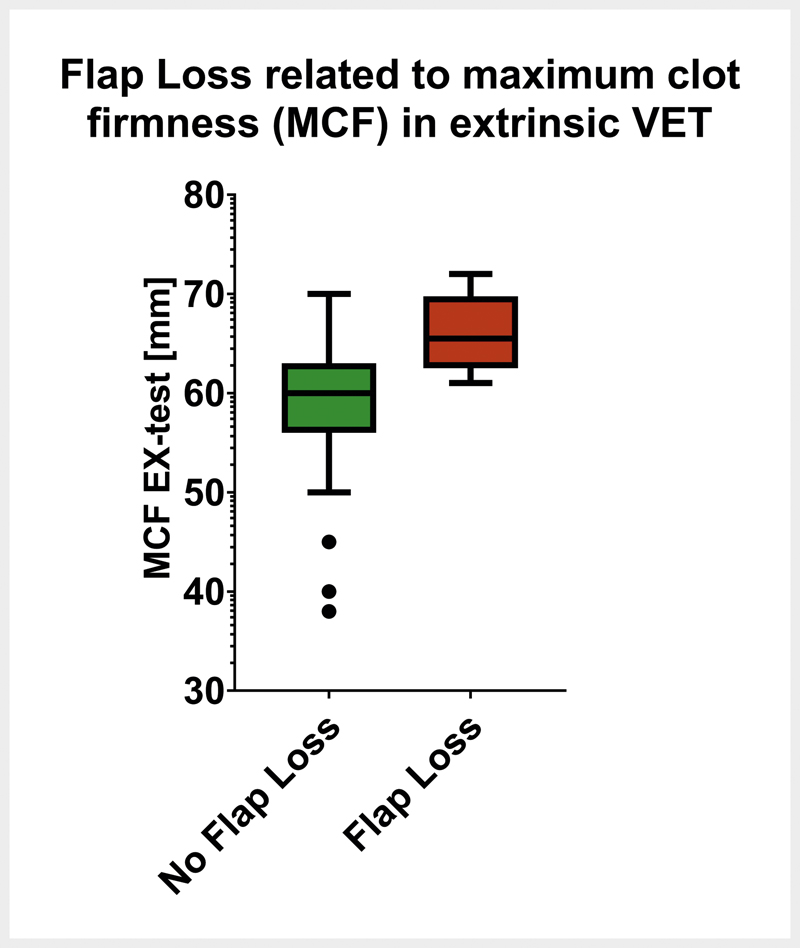
Results: So far, 100 consecutive patients were enrolled between February 2022 and March 2023. Free-flap perfusion deficiency occurred in 8 patients (8%), and in 10 patients (10%) a venous congested flap was observed (2 patients presented both perfusion deficits and venous congestion). In 8 patients with perfusion deficiency re-operation was performed in 5 (63%), whereby 4 flaps could be saved. In 10 patients with venous congestion, skin pricking was performed in 7 patients (70%), whereby 5 flaps could be saved. Overall free-flap loss from any etiology occurred in 6 patients (6%). Parameters for extrinsic VET (EX-test) at 5 (A5) and 10 (A10) minutes as well at maximum clot firmness (MCF) were significantly higher in patients with free-flap loss ([Fig. 2]), indicating hypercoagulability, while on the other hand none of the SLT could predict free-flap loss. Although antithrombin levels were higher at baseline in patients with free-flap loss, this did not seem to prevent free-flap loss. ([Fig. 1]). Interestingly values for MCF in EX-test decreased in both groups (with and without flap lost) during and dircetly after surgery. Patients with flap loss showed not only significantly higher MCF at baseline, but also after 3-10 days after surgery, when flap loss typically occurs, indicating an upregulated metabolism leading to hypercoagulability ([Fig. 3]).


Conclusion: In our interim-analysis, overall free-flap loss was as high as expected with 6%. Only VET (performed within several minutes after induction of anesthesia) was able to predict overall free-flap loss. We conclude that whole blood testing with VET is more appropriate to detect hypercoagulability and to predict free-flap loss than SLT. Whether VTE can be used to guide anticoagulant therapy for better flap survival remains to be tested in dedicated RCTs.
Conflict of Interest:
LH received honoraria for lectures from AstraZeneca, CSL Behring, Werfen and Octapharma.
-
References
- 1 Schröder TA. et al. Enhancing Anticoagulation Monitoring and Therapy in Patients Undergoing Microvascular Reconstruction in Maxillofacial Surgery: A Prospective Observational Trial. J Pers Med 2022; 12 (08) 1229
Publication History
Article published online:
13 February 2025
© 2025. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Schröder TA. et al. Enhancing Anticoagulation Monitoring and Therapy in Patients Undergoing Microvascular Reconstruction in Maxillofacial Surgery: A Prospective Observational Trial. J Pers Med 2022; 12 (08) 1229