

Subscribe to RSS
DOI: 10.1055/s-0044-1792160
Bow–Hunter Syndrome Due to Tandem Lesions; A Case Report
Authors
Funding None.

Abstract
Bow–Hunter syndrome (BHS) includes a form of stroke caused by dynamic factors affecting the extracranial vertebral artery (VA), such as rotation-induced flow disturbance at the atlantoaxial level. BHS is a rare condition that can result from a variety of factors, including abnormal bone compression and vertebral instability. So far, there have been no reports in which both vertebral instability and osteophytes compress the VA at different sites, leading to stroke. Herein, we present a rare case of stroke attributed to BHS involving thrombosis formation due to osteophyte compression at C3/4 and VA occlusion due to vertebral instability at the C4/5 overlapped. A 72-year-old male presented with rotational vertigo and vomiting associated with a cerebellar infarction. Digital subtraction angiography revealed severe stenosis of the left VA with an intra-arterial thrombus. Percutaneous transluminal angioplasty improved the stenosis; however, intravascular ultrasound revealed compression of the VA by osteophytes at C3/4. Additionally, left VA occlusion at C4/5 was confirmed because of vertebral instability. The osteophyte was removed via the anterolateral approach, and the VA was decompressed. The patient's postoperative course was uneventful, with no recurrence for more than 2 years. BHS can occur in the lower cervical spine when vertebral instability coincides with intimal arterial damage caused by osteophytes at other sites.
Keywords
Bow–Hunter syndrome - vertebral artery - intravascular ultrasound - osteophytes - vertebral instabilityIntroduction
Bow–Hunter syndrome (BHS) is a rare condition in which head rotation causes vertebral artery (VA) flow disturbance at the atlantoaxial level, leading to vertebrobasilar insufficiency.[1] Due to its anatomical course through the transverse foramen, the second segment of the VA can be compressed by abnormal bones such as osteophytes, leading to cerebral ischemia or embolism.[2] [3] [4] [5] [6] [7] [8] Additionally, the VA can be stenosed or occluded due to vertebral instability, further complicating the diagnosis and treatment. However, to our knowledge, there have been no reported cases in which vertebral instability and osteophytes separately compress the VA at different sites, leading to stroke.
We encountered a rare case in which two abnormalities overlapped, leading to a stroke attributed to BHS. Specifically, these abnormalities included thrombosis formation due to intimal injury of the VA at the C3/4 osteophyte and cervical instability causing VA occlusion at C4/5.
Case Description
A 72-year-old male presented to our hospital with persistent rotational vertigo and vomiting upon awakening. He had a history of hypertension, hyperlipidemia, and left internal carotid artery stenosis, and was taking statins, aspirin, and antihypertensive medications. He had a smoking history of 20 to 40 cigarettes per day for > 30 years. On admission, his consciousness level was assessed as 15 on the Glasgow Coma Scale, with saccadic eye movements and horizontal gaze nystagmus. The patient presented with dysarthria, mild dysmetria, and mild decomposition. His National Institutes of Health Stroke Scale (NIHSS) score was 3, with left upper- and lower-limb ataxia and speech disorders. Magnetic resonance imaging revealed acute cerebellar infarction ([Fig. 1A]).
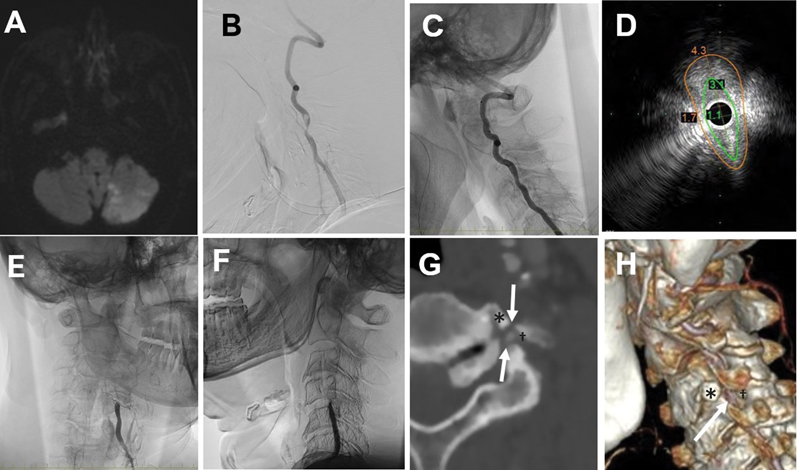
Digital subtraction angiography (DSA) revealed severe stenosis with an intra-arterial thrombus in the left VA ([Fig. 1B]). After 2 weeks of heparinization, percutaneous transluminal angioplasty (PTA) was performed to treat the symptomatic left VA stenosis using Shiden 3.0 × 20 mm (Kaneka, Osaka, Japan) at 6 atm/2 minute and Genity 3.0 × 25 mm (Kaneka) at 6 atm/2 minute, resulting in stenosis improvement, with good blood flow in the neutral and right rotation head positions ([Fig. 1C]). However, intravascular ultrasonography (IVUS) using the VOLCANO system (Volcano Japan Corp., Tokyo, Japan) and an IVUS catheter (Eagle Eye Platinum; Volcano Japan Corp.) indicated compression of the left VA by the osteophytes ([Fig. 1D]). Furthermore, with the head in flexion and left rotation, left VA occlusion at the C4/5 was confirmed ([Fig. 1E, F]). Considering the risk of stent breakage due to osteophytes, a stent was not placed, and the procedure was ended only when PTA was performed.
We diagnosed symptomatic VA stenosis occurring as a result of the simultaneous occurrence of two abnormalities: intimal damage due to compression at the left C3/4 osteophytes and VA occlusion due to vertebral instability of C4/5 ([Fig. 1G, H]). The anterolateral approach was used to decompress the VA for osteophyte removal. The patient's head was rotated to the right while confirming the left VA blood flow with ultrasound ([Fig. 2A]). Exposure of the osteophytes and the C3/4 anterior tubercle revealed compression of the VA ([Fig. 2B]), and osteophytes were removed. In addition, the base of the C3/4 anterior tubercle was drilled to expose the VA. Further, we removed the hypertrophic osteophyte that arose from the intervertebral foramen of C4, as it compressed the VA from behind ([Fig. 2C]). Finally, the relief of tension on the VA was confirmed ([Fig. 2D]). Postoperatively, computed tomography angiography confirmed the removal of the C3/4 osteophyte and complete decompression of the VA ([Fig. 2E]).

DSA obtained on the 7th postoperative day revealed no significant stenosis at C3/4 or C4/5 in the neutral position ([Fig. 2F]). However, residual severe stenosis of the left VA with delayed flow in left head rotation was observed ([Fig. 2G]). Minimal stenosis at C3/4 was observed in head flexion compared with the neutral position, but no VA occlusion occurred at C4/5 ([Fig. 2H]). The patient was discharged on postoperative day 10 with a modified Rankin Scale score of 0 and an NIHSS score of 0. The patient has remained recurrence-free for 2 years.
Discussion
Herein, we presented a case of BHS in which the left VA was compressed by osteophytes between the C3 and C4 intervertebral foramen, causing intimal damage and stenosis of the VA. Additionally, vertebral instability at the C4/5 level was resulting in an abnormal VA course, causing occlusion of the left VA during left rotation or extension of the head. These abnormalities caused thrombosis at the C3/4 level, leading to cerebellar infarction when the thrombus was scattered. In the present case, we aimed to prevent recurrent stroke by removing the obvious thrombotic causes of the osteophytes. Although the lesions occurred at separate sites at the C3/4 and C4/5 levels due to overlapping causes of osteophyte and vertebral instability, resection of the osteophyte led to a favorable outcome.
This case report has several clinical implications. First, this experience shows that VA cryptogenic occlusion due to vertebral instability, VA latent stenosis, and/or intimal damage caused by osteophytes at different sites can cause cerebellar infarction when these two events occur simultaneously. To the best of our knowledge, no similar cases have been reported thus far.
In the present case, we determined that the osteophytes at the C3/4 directly caused compression of the VA and led to occlusion during rotation. Furthermore, we inferred from preoperative DSA imaging that the presence of vertebral instability caused occlusion of the VA at C4/5 during extension. Additionally, we hypothesized that the formation of these abnormal osteophytes demonstrates vertebral instability.
There are no specific treatment guidelines for BHS, which leads to difficulty in determining the treatment approach. Approximately half of all patients treated with antiplatelet agents experience recurrence within several months to years, suggesting that some form of surgical intervention is recommended.[9] In cases presenting with abnormalities at two sites, such as ours, it is essential to clearly understand the pathogenesis of cerebellar infarction as two separate entities. Although most individuals with vertebral instability remain asymptomatic due to dynamic effects, the addition of other pathological factors can lead to cerebellar infarction. Therefore, personalized treatment approaches are required. In our case, we aimed to remove the pathological factor of intimal damage by decompressing the osteophyte, thereby limiting the impact to only dynamic effects.
In addition, BHS can occur at the lower cervical spine, although it is typically associated with VA occlusion of the upper cervical spine (C1/2) during head rotation. Reports of BHS in the lower cervical spine are rare; however, when they do occur, they are often associated with osteophytes.[2] [4] [5] [10] [11] [12] [13] Prior case reports of vertebral instability have shown that the upper vertebral body on the affected intervertebral segment slides backward on the side where it has rotated, while the VA in the transverse foramen is subjected to overstretching, leading to compression of the VA. Furthermore, in the presence of osteophytes, the VA is more strongly compressed and prone to occlusion.[3] Therefore, when a BHS is found at the lower cervical spine, it is necessary to actively check for vertebral instability to make an accurate diagnosis and decide on an appropriate treatment strategy.
Finally, IVUS can provide clues for the diagnosis of BHS. In this case, we used IVUS to confirm the presence or absence of VA dissection or thrombus, the measurement of the vessel diameter, and the nature of the VA stenosis, finding that the osteophyte surrounding the VA caused arterial compression. To the best of our knowledge, which is similar to our case, only one reported case has shown that IVUS is useful for diagnosing BHS.[14]
Conclusion
BHS may occur in the lower cervical spine. Further, this phenomenon can be caused by two coinciding factors: vertebral instability and intimal damage due to osteophyte at a different site.
Conflict of Interest
None declared.
Note
This manuscript was presented at the 53rd Annual Meeting of the Japanese Society on Surgery for Cerebral Stroke on March 9, 2024.
Authors' Contributions
All authors contributed to the conception and design of the study. Material preparation and data collection were performed by all the authors. Data analysis was performed by S.Y. and J.N,. The first draft of the manuscript was written by S.Y., and all authors commented on the previous versions of the manuscript. All the authors have read and approved the final manuscript.
Ethical Approval
All procedures in this study were performed in accordance with the 1964 Declaration of Helsinki. A series of treatments were performed after obtaining appropriate written informed consent from the patient. The requirement for additional written consent for inclusion in this study was waived by the Ethics Committee of Saiseikai Shiga Hospital because of the retrospective and observational nature of the study (Permission Number; 646).
-
References
- 1 Sorensen BF. Bow Hunter's stroke. Neurosurgery 1978; 2 (03) 259-261
- 2 Bulsara KR, Velez DA, Villavicencio A. Rotational vertebral artery insufficiency resulting from cervical spondylosis: case report and review of the literature. Surg Neurol 2006; 65 (06) 625-627
- 3 Kawaguchi T, Fujita S, Hosoda K, Shibata Y, Iwakura M, Tamaki N. Rotational occlusion of the vertebral artery caused by transverse process hyperrotation and unilateral apophyseal joint subluxation. Case report. J Neurosurg 1997; 86 (06) 1031-1035
- 4 Citow JS, Macdonald RL. Posterior decompression of the vertebral artery narrowed by cervical osteophyte: case report. Surg Neurol 1999; 51 (05) 495-498 , discussion 498–499
- 5 Yamaguchi S, Sakata K, Nakayama K, Shigemori M. A case of embolic infarction originating from extracranial vertebral artery stenosis by cervical spondylosis at C5/6: its pathogenesis and surgical treatment [in Japanese]. No Shinkei Geka 2003; 31 (10) 1111-1116
- 6 Shimizu S, Ishigaki T, Murata H, Kubo Y, Toma N, Morooka Y. Vertebral artery dissection due to a bone anomaly of the superior facet of C6: a rare cause of embolic stroke [in Japanese]. No Shinkei Geka 2008; 36 (08) 725-730
- 7 Spetzler RF, Hadley MN, Martin NA, Hopkins LN, Carter LP, Budny J. Vertebrobasilar insufficiency. Part 1: microsurgical treatment of extracranial vertebrobasilar disease. J Neurosurg 1987; 66 (05) 648-661
- 8 Sullivan HG, Harbison JW, Vines FS, Becker D. Embolic posterior cerebral artery occlusion secondary to spondylitic vertebral artery compression. Case report. J Neurosurg 1975; 43 (05) 618-622
- 9 Sato M, Yamahata H, Yasuda M. et al. Treatment of rotational/positional vertebral artery occlusion due to degenerative changes in the cervical vertebrae: a case report and review of the literature. J Orthop Sci 2023; 28 (06) 1614-1619
- 10 Fleming JB, Vora TK, Harrigan MR. Rare case of bilateral vertebral artery stenosis caused by C4-5 spondylotic changes manifesting with bilateral bow hunter's syndrome. World Neurosurg 2013; 79 (5-6): E1-E5
- 11 Velat GJ, Reavey-Cantwell JF, Ulm AJ, Lewis SB. Intraoperative dynamic angiography to detect resolution of Bow Hunter's syndrome: technical case report. Surg Neurol 2006; 66 (04) 420-423 , discussion 423
- 12 Ohsaka M, Takgami M, Koyanagi I, Kim S, Houkin K. Cerebral ischemia originating from rotational vertebral artery occlusion caused by C5/6 spondylotic changes: a case report [in Japanese]. No Shinkei Geka 2009; 37 (08) 797-802
- 13 Lee V, Riles TS, Stableford J, Berguer R. Two case presentations and surgical management of Bow Hunter's syndrome associated with bony abnormalities of the C7 vertebra. J Vasc Surg 2011; 53 (05) 1381-1385
- 14 Takafumi S, Hojo R, Tsuchiyama T, Fukamizu S. A case report of Bow Hunter's syndrome with intravascular ultrasound showing changing significant severe stenosis of the left vertebral artery associated with turning left. Eur Heart J Case Rep 2023; 8 (01) ytad639
Address for correspondence
Publication History
Article published online:
04 November 2024
© 2024. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sorensen BF. Bow Hunter's stroke. Neurosurgery 1978; 2 (03) 259-261
- 2 Bulsara KR, Velez DA, Villavicencio A. Rotational vertebral artery insufficiency resulting from cervical spondylosis: case report and review of the literature. Surg Neurol 2006; 65 (06) 625-627
- 3 Kawaguchi T, Fujita S, Hosoda K, Shibata Y, Iwakura M, Tamaki N. Rotational occlusion of the vertebral artery caused by transverse process hyperrotation and unilateral apophyseal joint subluxation. Case report. J Neurosurg 1997; 86 (06) 1031-1035
- 4 Citow JS, Macdonald RL. Posterior decompression of the vertebral artery narrowed by cervical osteophyte: case report. Surg Neurol 1999; 51 (05) 495-498 , discussion 498–499
- 5 Yamaguchi S, Sakata K, Nakayama K, Shigemori M. A case of embolic infarction originating from extracranial vertebral artery stenosis by cervical spondylosis at C5/6: its pathogenesis and surgical treatment [in Japanese]. No Shinkei Geka 2003; 31 (10) 1111-1116
- 6 Shimizu S, Ishigaki T, Murata H, Kubo Y, Toma N, Morooka Y. Vertebral artery dissection due to a bone anomaly of the superior facet of C6: a rare cause of embolic stroke [in Japanese]. No Shinkei Geka 2008; 36 (08) 725-730
- 7 Spetzler RF, Hadley MN, Martin NA, Hopkins LN, Carter LP, Budny J. Vertebrobasilar insufficiency. Part 1: microsurgical treatment of extracranial vertebrobasilar disease. J Neurosurg 1987; 66 (05) 648-661
- 8 Sullivan HG, Harbison JW, Vines FS, Becker D. Embolic posterior cerebral artery occlusion secondary to spondylitic vertebral artery compression. Case report. J Neurosurg 1975; 43 (05) 618-622
- 9 Sato M, Yamahata H, Yasuda M. et al. Treatment of rotational/positional vertebral artery occlusion due to degenerative changes in the cervical vertebrae: a case report and review of the literature. J Orthop Sci 2023; 28 (06) 1614-1619
- 10 Fleming JB, Vora TK, Harrigan MR. Rare case of bilateral vertebral artery stenosis caused by C4-5 spondylotic changes manifesting with bilateral bow hunter's syndrome. World Neurosurg 2013; 79 (5-6): E1-E5
- 11 Velat GJ, Reavey-Cantwell JF, Ulm AJ, Lewis SB. Intraoperative dynamic angiography to detect resolution of Bow Hunter's syndrome: technical case report. Surg Neurol 2006; 66 (04) 420-423 , discussion 423
- 12 Ohsaka M, Takgami M, Koyanagi I, Kim S, Houkin K. Cerebral ischemia originating from rotational vertebral artery occlusion caused by C5/6 spondylotic changes: a case report [in Japanese]. No Shinkei Geka 2009; 37 (08) 797-802
- 13 Lee V, Riles TS, Stableford J, Berguer R. Two case presentations and surgical management of Bow Hunter's syndrome associated with bony abnormalities of the C7 vertebra. J Vasc Surg 2011; 53 (05) 1381-1385
- 14 Takafumi S, Hojo R, Tsuchiyama T, Fukamizu S. A case report of Bow Hunter's syndrome with intravascular ultrasound showing changing significant severe stenosis of the left vertebral artery associated with turning left. Eur Heart J Case Rep 2023; 8 (01) ytad639