

Subscribe to RSS
DOI: 10.1055/s-0044-1790289
Multicenter Clinical Randomized Controlled Trial and Network Pharmacology Analysis of Zhenzhu Qingyuan Granules for the Treatment of Gastroesophageal Reflux Disease
Authors
Funding National Administration of Traditional Chinese Medicine Evidence-Based Capacity Building Project (2019XZZX-XH005), Special Project on Traditional Chinese Medicine Scientific Research of Health Commission of Henan Province (2022ZY2022), Henan Provincial Top Talents Cultivation Project in Traditional Chinese Medicine Discipline of Henan Provincial Traditional Chinese Medicine Inheritance and Innovation Talents Project (Zhongjing Project) (Henan Health Traditional Medicine Letter [2021] No. 15), and Special Project on Traditional Chinese Medicine Scientific Research of Health Commission of Henan Province (2023ZY2062).

Abstract
Objective To evaluate the clinical efficacy and safety of Zhenzhu Qingyuan Granules through a clinical randomized controlled trial and to analyze the potential action targets and pathways of this formula using network pharmacology.
Methods Patients with gastroesophageal reflux disease (GERD) of liver–stomach stagnant heat pattern who met the inclusion and exclusion criteria were randomly divided into the control group and the observation group. The control group received oral rabeprazole, whereas the observation group were given Zhenzhu Qingyuan Granules in addition to the rabeprazole. The treatment duration was 8 weeks. Clinical efficacy was observed in both groups after 8 weeks. Network pharmacology was used to analyze the action targets of Zhenzhu Qingyuan Granules and the genes related to GERD, and core targets were inferred. Gene Ontology and Kyoto Encyclopedia of Genes and Genomes enrichment analyses were conducted to explore the potential mechanisms of this formula.
Results The clinical research results showed that the total effective rate in the treatment group was 92.68%, compared with 70.00% in the control group, with a statistically significant difference (p < 0.05). After treatment, both Chinese medicine syndrome score and endoscopic score improved in both groups compared with before treatment (p < 0.05), and the treatment group showed greater improvement than the control group (p < 0.05). Network pharmacology identified effective components of Zhenzhu Qingyuan Granules for treating GERD, including quercetin, luteolin, and β-sitosterol, with potential action targets such as tumor protein 53 (TP53), protein kinase B (AKT1), and tumor necrosis factor.
Conclusion Zhenzhu Qingyuan Granules can significantly improve clinical symptoms in patients with GERD of liver–stomach stagnated heat pattern, enhance clinical efficacy, and have high safety. This formula may exert therapeutic effects through multiple targets and pathways.
Keywords
gastroesophageal reflux disease - Zhenzhu Qingyuan Granules - liver–stomach stagnated heat syndrome - randomized controlled trial - network pharmacologyIntroduction
Gastroesophageal reflux disease (GERD) is one of the common diseases in gastroenterology, primarily characterized by symptoms such as acid reflux, heartburn, burning sensation, and retrosternal pain, and with high recurrence tendency. The incidence of GERD in the Asia-Pacific region is lower than in Western countries, but there has been an increasing trend in the past decade.[1] Currently, besides lifestyle modifications, Western medicine mainly relies on proton pump inhibitor (PPI), prokinetic agents, endoscopic treatment, and surgical options,[2] although the effectiveness of these interventions is limited. Traditional Chinese medicine (TCM) emphasizes a holistic approach, using syndrome differentiation and treatment to address both the symptoms and root causes of the disease. This method aims to restore normal spleen and stomach function and has shown definite clinical efficacy with a low recurrence rate.[3] [4] Clinically, some patients experience high life stress, resulting in liver qi stagnation, which in turn affects the spleen and stomach, leading to digestive weakness and subsequent heat accumulation due to long-term improper diet. Based on tongue and pulse diagnosis, these patients were identified as having the liver–stomach stagnated heat pattern. Zhenzhu Qingyuan granules, an empirical formula for treating GERD, have demonstrated significant efficacy in addressing the liver–stomach stagnated heat pattern. This study aims to conduct a randomized controlled trial to observe the clinical efficacy of Zhenzhu Qingyuan granules in treating GERD with liver–stomach stagnated heat pattern and to preliminarily explore its mechanism through network pharmacology.
Clinical Data
General Information
This study employed a prospective, multicenter, randomized, parallel-controlled trial design. A total of 88 outpatients diagnosed with GERD and identified with the liver–stomach stagnated heat pattern according to TCM from the Henan Provincial Hospital of Chinese Medicine, the Fifth Affiliated Hospital of Zhengzhou University, and Zhengzhou People's Hospital between August 2020 and March 2022 were selected. Participants were randomly divided into an observation group and a control group, with 44 patients in each group. During the study, three patients dropped out from the observation group and four from the control group. Ultimately, 41 patients were included in the observation group, consisting of 28 males and 13 females, with an average age of 52.71 ± 9.86 years and an average disease duration of 3 ± 0.49 years. The control group comprised 40 patients, with 29 males and 11 females, an average age of 51.69 ± 10.17 years, and an average disease duration of 3 ± 0.72 years. The baseline data of both groups were comparable (p > 0.05). The study was approved by the Ethics Committee of Henan Provincial Hospital of Chinese Medicine (approval number: Hospital Ethics Approval No. [1150-01]).
Diagnostic Criteria
The diagnostic criteria for GERD and the TCM syndrome differentiation for liver–stomach stagnated heat syndrome refer to the Consensus on the Diagnosis and Treatment of Gastroesophageal Reflux Disease by Combining Traditional Chinese and Western Medicine.[5]
Western medicine diagnostic criteria for GERD: (1) presence of typical symptoms such as heartburn and acid reflux; (2) atypical symptoms including chest pain, upper abdominal pain, burning sensation in the upper abdomen, and belching; (3) exclusion of cardiac chest pain in patients with chest pain; (4) possible association with extraesophageal symptoms including cough, throat symptoms, asthma, and dental erosion; (5) positive in esophageal reflux monitoring; (6) positive in upper gastrointestinal endoscopy; (7) effective PPI test can be used as a preliminary diagnostic method for GERD. Diagnosis of GERD can be made if criteria (1) and any one of criteria (2)–(4) or criteria (5)–(7) are met.
TCM syndrome differentiation criteria for liver–stomach qi stagnated heat syndrome: primary symptoms—(1) acid reflux; (2) burning pain behind the sternum; (3) stomach upset. Secondary symptoms—(1) dysphoria and irritability; (2) hypochondriac distension and fullness; (3) dry mouth with bitter taste; (4) constipation. Tongue and pulse: red tongue with yellow coating, wiry, and slippery pulse. Diagnosis requires the presence of two primary symptoms and one or two secondary symptoms, with reference to the tongue and pulse characteristics.
Inclusion Criteria
(1) Age between 18 and 65 years; (2) diagnosis of GERD with liver–stomach stagnated heat pattern and TCM syndrome differentiation as described above; (3) willingness to participate in the study and sign informed consent.
Exclusion Criteria
(1) History of severe peptic ulcers or gastrointestinal surgery, digestive tract space-occupying lesion, or other serious complications; (2) pregnant or breastfeeding women; (3) severe liver or kidney dysfunction, malignant tumor, or cardiovascular diseases assessed by an anesthesiologist as unsuitable for general anesthesia; (4) other autoimmune or organ failure diseases; (5) severe mental illness that could harm others; (6) other serious infectious diseases; (7) participation in other clinical trials within the past 3 months.
Elimination Criteria
Elimination of participants who have poor compliance during the study, use other medications that may affect the study results, develop other diseases requiring a change in treatment, have missing or incomplete clinical data, or experience serious adverse events during the treatment process.
Clinical Research Methods
Treatment Methods
Control Group
Oral administration of rabeprazole sodium enteric-coated tablets (China, Jiangsu Hansoh Pharmaceutical Co., Ltd.), 2 tablets each time, once daily, taken on an empty stomach. All groups will take this for 8 weeks, constituting one treatment course.
Observation Group
Rabeprazole sodium enteric-coated tablets combined with Zhenzhu Qingyuan Granules. Prescription: Chinese medicine; Zhenzhu Qingyuan Granules (China Resources Sanjiu Medical & Pharmaceutical Co., Ltd.), including 30 g of Zhenzhumu (Margaritifera Concha), 6 g of Qingpi (Citri Reticulatae Pericarpium Viride), 10 g of Yuanhu (Corydalis Rhizoma), 6 g of Zhishi (Aurantii Fructus Immaturus), 20 g of Zhebeimu (Fritillariae Thunbergii Bulbus), 20 g of Wuzeigu (Sepiae Endoconcha), 6 g of Huanglian (Coptidis Rhizoma), and 3 g of Wuzhuyu (Euodiae Fructus). Take one dose daily, add 200 mL of warm boiled water, and take in two divided doses. The treatment cycle is 8 weeks. Follow-up for both the observation and control groups will be conducted 4 weeks after stopping the medication.
Observation Indicators and Methods
Traditional Chinese Medicine Syndrome Score[6]
Observation of symptoms like acid reflux, retrosternal burning pain, stomach upset, dysphoria and irritability, dry mouth with bitter taste. Symptoms are graded according to the Guidelines for Clinical Research of New Chinese Herbs, with scores of 0, 2, 4, or 6 for none, mild, moderate, or severe symptoms.
Traditional Chinese Medicine Syndrome Efficacy Standard
Efficacy index is calculated using the nimodipine method. Efficacy index = [(Pretreatment score − Posttreatment score)/Pretreatment score] × 100%. According to the Guidelines for Clinical Research of New Chinese Herbs,[7] the efficacy is categorized into four levels: (1) clinical cured (symptom of reflux disappears, efficacy index ≥ 95%); (2) significantly effective (symptoms mostly disappear, occasional symptoms while quickly resolve, 70% ≤ efficacy index < 95%); (3) effective (symptoms remain but are alleviated, 30% ≤ efficacy index < 70%); (4) ineffective (symptoms persist or worsen, efficacy index < 30%).
Improvement in Esophageal Mucosal Inflammation under Endoscopy
Endoscopic grading of esophageal mucosa: according to the Los Angeles Classification for GERD, graded as normal, A, B, C, D with scores of 0, 1, 2, 3, 4 respectively.[5] [6]
Reflux Disease Questionnaire Efficacy Score
Reflux Disease Questionnaire (RDQ) scores were assessed before and after treatment,[6] with symptoms of heartburn, regurgitation, noncardiac chest pain, and acid reflux being measured weekly. The total score ranges from 0 to 40, with higher scores indicating more severe and frequent symptoms.
Adverse Event Records and Safety Indicators
Blood routine, urine routine, stool routine + occult blood, electrocardiogram, liver function, and kidney function tests were conducted before treatment and at 4 and 8 weeks of treatment. Adverse reactions such as diarrhea, nausea, and vomiting were recorded.
Statistical Methods
Statistical analysis was conducted using SPSS 25.0 software. Measurement data were expressed as (xˉ ± S), with independent samples t-test for intergroup comparisons and paired samples t-test for intragroup comparisons. Count data were expressed as (cases [%]), with χ 2 test used. p < 0.05 indicated statistical significance.
Clinical Research Results
Comparison of Clinical Traditional Chinese Medicine Syndrome Scores Before and After Treatment in Both Groups
Compared with before treatment, the observation group showed significant improvement in symptoms such as acid reflux, retrosternal burning pain, stomach upset, dysphoria and irritability, dry mouth with bitter taste, hypochondriac distension and fullness, constipation, and total TCM syndrome scores, with statistically significant differences (p < 0.05). The control group also showed significant improvement in the symptoms such as acid reflux, retrosternal burning pain, stomach upset, dysphoria and irritability, dry mouth with bitter taste and total TCM syndrome scores, with statistically significant differences (p < 0.05). Additionally, compared with the control group after treatment, the observation group had significantly better results in the mentioned TCM syndrome scores and total TCM syndrome scores, with statistically significant differences (p < 0.05), as shown in [Table 1].
Note: For intragroup comparisons, a p < 0.05, b p < 0.01; for intergroup comparisons, c p < 0.05, d p < 0.01.
Comparison of Clinical Efficacy of Traditional Chinese Medicine Syndromes between Two Groups
The number of patients with good clinical efficacy in the observation group and control group was 38 and 28, respectively, with total effective rates of 92.68 and 70.00%, showing a statistically significant difference (p < 0.05), as shown in [Table 2].
Note: Compared with the control group, a p < 0.05.
Comparison of Reflux Disease Questionnaire Scores and Endoscopic Esophageal Mucosal Scores Before and After Treatment between Two Groups
Compared with before treatment, the observation and treatment groups showed significant decreases in endoscopic esophageal mucosal scores and RDQ scores after treatment, with statistically significant differences (p < 0.05). Compared with the control group after treatment, the observation group also showed significant decreases in endoscopic esophageal mucosal scores and RDQ scores, with statistically significant differences (p < 0.05), as shown in [Table 3]. Endoscopic mucosal findings before and after treatment for both groups are shown in [Fig. 1].
Abbreviation: RDQ, Reflux Disease Questionnaire.
Note: Compared with before treatment in the same group, a p < 0.05, b p < 0.01; compared with the control group after treatment, c p < 0.05, d p < 0.01.
Safety Evaluation and Adverse Reaction Observation
Routine tests of blood, urine, and stool, as well as liver and kidney functions, were normal before and after treatment for both groups; no significant adverse reactions were observed in either group, indicating good drug safety.
Network Pharmacology Study of Zhenzhu Qingyuan Granules for the Treatment of Gastroesophageal Reflux Disease
Materials and Methods
Active Ingredients and Targets of Zhenzhu Qingyuan Granules
From the Traditional Chinese Medicine System Pharmacology Database, chemical components of the 8 herbs in Zhenzhu Qingyuan Granules: Huanglian (Coptidis Rhizoma), Wuzhuyu (Euodiae Fructus), Zhishi (Aurantii Fructus Immaturus), Qingpi (Citri Reticulatae Pericarpium Viride), Yanhusuo (Corydalis Rhizoma), Zhenzhumu (Margaritifera Concha), Zhebeimu (Fritillariae Thunbergii Bulbus), and Haipiaoxiao (Sepiae Endoconcha) were obtained. Set drug-likeness (DL) and oral bioavailability (OB) as screening parameters, select those with DL ≥ 0.18 and OB ≥ 30% to compile an active ingredient library. Organize the targets of the active ingredients and annotate target genes using the Uniprot database.
Selection of Gastroesophageal Reflux Disease-Related Genes
To search Human Genome Annotation and Online Mendelian Inheritance in Man databases to filter GERD-related genes. To compare GERD genes with targets of Zhenzhu Qingyuan Granules to identify common genes and create a Venn diagram using R software.
Construction of Effective Component–Target–Disease Network
The relationships between drug active components and common genes were imported into the network visualization software Cytoscape 3.8.0 to draw the Zhenzhu Qingyuan Granules effective active component–target–GERD network diagram.
Construction of Protein–Protein Interaction Network and Analysis of Core Targets
Common genes were imported into the STRING database, select “homo sapiens,” and draw the PPI network interaction diagram for GERD targets treated with Zhenzhu Qingyuan Granules. Set high confidence = 0.7 as the minimum interaction score. Use R to calculate the interaction frequency of major proteins, identify core targets, and generate a barplot of core targets.
Gene ontology Functional Enrichment and Kyoto Encyclopedia of Genes and Genomes Pathway Enrichment Analysis
Use R software for Gene Ontology (GO) functional enrichment and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis of common targets related to Zhenzhu Qingyuan Granules and GERD. Identify the main molecular functions and signaling pathways involved in treating GERD with Zhenzhu Qingyuan Granules.
Results
Active Components and Potential Targets of Zhenzhu Qingyuan Granules
Identify 14 active components from Huanglian (Coptidis Rhizoma), 30 from Wuzhuyu (Euodiae Fructus), 5 from Qingpi (Citri Reticulatae Pericarpium Viride), 22 from Zhishi (Aurantii Fructus Immaturus), 49 from Yanhusuo (Corydalis Rhizoma), 16 from Zhebeimu (Fritillariae Thunbergii Bulbus), 3 from Zhenzhumu (Margaritifera Concha), and 2 from Haipiaoxiao (Sepiae Endoconcha). After removing duplicates like Berberine, Quercetin, Coptisine, Sinensetin, and Naringenin, a total of 128 active components were obtained. After aggregating and deduplicating potential targets, 423 targets were identified. Using “gastroesophageal reflux disease” as the search term in the Genecards database, 4,120 disease-related genes were found, with 199 common genes compared with the potential targets of Zhenzhu Qingyuan Granules.[8]
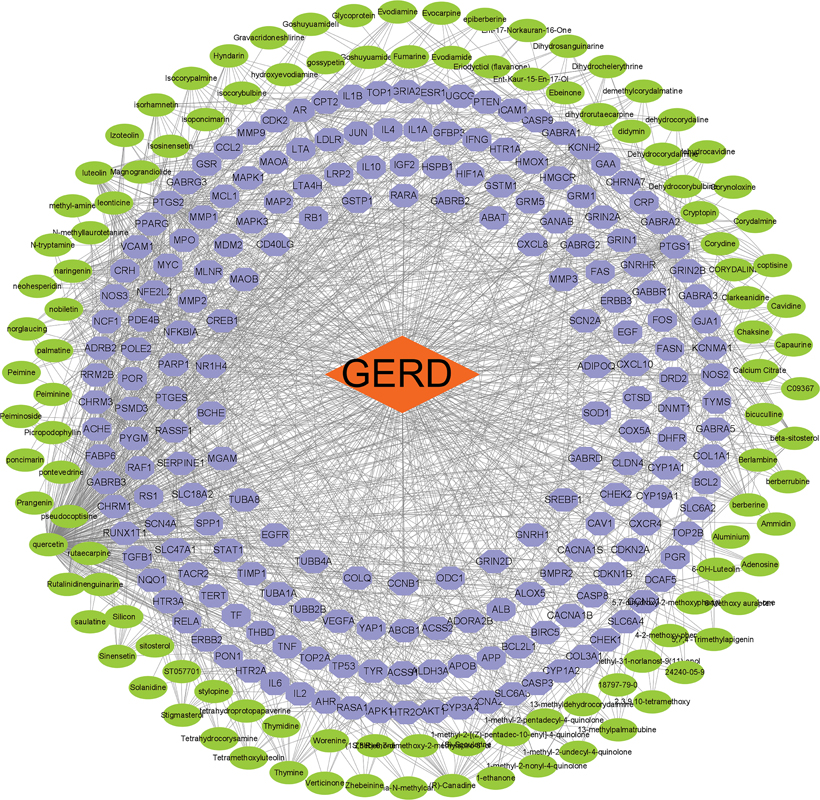
Effective Component–Target–Disease Network of Zhenzhu Qingyuan Granules
Draw the network relationship diagram of effective component–target–disease for Zhenzhu Qingyuan Granules. The diagram shows 199 common genes in purple and 111 effective active components for treating GERD in green. The component with the most treatment targets is Quercetin from Huanglian (Coptidis Rhizoma), Wuzhuyu (Euodiae Fructus), and Yanhusuo (Corydalis Rhizoma) (95 targets), followed by Luteolin from Zhishi (Aurantii Fructus Immaturus) (38 targets), β-Sitosterol from Wuzhuyu (Euodiae Fructus) (20 targets), Naringenin and Nobiletin from Qingpi (Citri Reticulatae Pericarpium Viride), and Zhishi (Aurantii Fructus Immaturus) (18 and 17 targets, respectively), Isorhamnetin from Wuzhuyu (Euodiae Fructus) (16 targets), and Hyndarin and Leonticine from Yanhusuo (Corydalis Rhizoma) (13 targets each), and Rutaecarpine from Wuzhuyu (Euodiae Fructus) (13 targets). Detailed information is in [Fig. 1].
Core Targets Interaction Diagram
Import the 199 common targets into the STRING database to obtain the protein interaction diagram, as shown in [Fig. 2]. Using R language, the top 30 targets by interaction rank were identified. The barplot ([Fig. 3]) shows that proteins such as TP53, AKT1, tumor necrosis factor (TNF), interleukin-6, jun proto-oncogene (JUN), mitogen-activated protein kinase 3, epidermal growth factor receptor, and vascular endothelial growth factor A rank highly as core targets.


Gene Ontology Functional Enrichment Analysis
Using R software, GO functional enrichment analysis of common targets related to Zhenzhu Qingyuan Granules and GERD was conducted, identifying 203 enriched GO functions. Thirty key molecular functions were selected based on enrichment protein numbers, as shown in [Fig. 4].

Kyoto Encyclopedia of Genes and Genomes Pathway Enrichment Analysis
KEGG pathway enrichment analysis was performed using R software on common targets of Zhenzhu Qingyuan Granules and GERD. A total of 170 signaling pathways were screened, with prominent pathways including AGE–RAGE signal pathway, lipid and atherosclerosis, and TNF signal pathway, as detailed in [Fig. 5].

Discussion
Currently, the treatment for GERD primarily involves medication, with acid suppression being the first-line treatment approach. Both domestic and international guidelines recommend PPI as the first-line drug, with a treatment course lasting from 4 to 8 weeks. For GERD patients with poor response to medication or those unwilling to use PPI long-term, antireflux surgery can be considered. While short-term efficacy is often good, there is generally a lack of long-term evidence supporting its efficacy. Long-term PPI therapy may lead to a series of adverse effects, including bacterial overgrowth and an increased risk of Clostridium difficile infections. The American College of Gastroenterology guidelines note that PPI may increase the risk of intestinal infections. Additionally, PPI may be less effective for refractory GERD patients.[9] [10] In contrast to Western medicine, TCM focuses on overall regulation while reducing gastric acid reflux. TCM employs multicomponent, multitarget interventions to help alleviate clinical symptoms, improve patient quality of life, reduce adverse effects from Western treatments, and lower recurrence rates.[11] According to clinical manifestations, GERD can be classified in TCM under categories such as “Caoza (stomach upset)” and “Tusuan (acid regurgitation),” with its etiology being heat-related. In the Supplements to the Diagnosis and Treatment (Zheng Zhi Hui Bu), it says: “Generally, stagnation in the middle energizer that persists and turns into heat leads to the transformation of wood into fire, causing acid due to heat.” Zhenzhu Qingyuan Granules is an empirical formula for treating GERD of liver–stomach stagnated heat pattern. In this formula, Zhenzhumu (Margaritifera Concha) can clear liver heat and has strong acid-neutralizing and pain-relieving effects, serving as the king drug. Qingpi (Citri Reticulatae Pericarpium Viride) disperses liver qi and resolves stagnation, whereas Huanglian (Coptidis Rhizoma) clears heat, dries dampness, purges fire, and removes toxicity, which is effective in clearing liver and stomach fire. If the liver fire is purged, it would not attack the stomach qi, and elimination of stomach heat ensures harmonized ascending and descending. The combination of these two act as the minister herbs to alleviate liver qi stagnation and clear hidden fire. Yanhusuo (Corydalis Rhizoma) activates blood and qi flow and relieves pain; Zhishi (Aurantii Fructus Immaturus) relieves qi stagnation and reduces accumulation, resolves phlegm and dissipates fullness, working with Qingpi (Citri Reticulatae Pericarpium Viride) to regulate overall qi movement. Zhebeimu (Fritillariae Thunbergii Bulbus) resolves phlegm, dissipates masses, reduces carbuncles. Haipiaoxiao (Sepiae Endoconcha) astringes and stops bleeding, suppresses acidity, and relieves pain. The combination of these two forms Wubei Powder, which is effective for stomachache, acid regurgitation, stomach upset, and hunger-like sensations. Wuzhuyu (Euodiae Fructus) disperses liver qi stagnation and descends upward flow of stomach qi, and when paired with Huanglian (Coptidis Rhizoma), it can form Zuojin Pill, which clears the liver, harmonizes the stomach, and descends reversed flow of qi. It also guides other herbs into the liver meridian, acting as a conductant herb. The overall formula works to disperse the liver, relieve qi stagnation, purge heat and harmonize the middle energizer, suppress acid, and stop pain. The results of this study show that Zhenzhu Qingyuan Granules can effectively improve symptoms and mucosal findings in GERD patients, with results superior to the use of rabeprazole alone.
To further explore its action mechanism, this study employed network pharmacology to identify potential therapeutic targets. The results showed that the active components in the Zhenzhu Qingyuan Granules include quercetin, luteolin, and β-sitosterol. Quercetin, one of the flavonoid dietary antioxidants,[12] can inhibit gastric acid secretion, reduce oxidative stress in gastric ulcers, and protect the gastric mucosa.[13] Research has demonstrated that quercetin can protect against experimental reflux esophagitis in rats by inhibiting lipid peroxidation and increasing catalase levels.[14] Luteolin, a flavonoid compound, can promote the expression and nuclear translocation of antioxidant-related nuclear factors such as nuclear factor-erythroid 2 related factor 2 (Nrf2) and heme oxygenase-1 (HO-1), while reducing the enzymatic activity of HO-1 in cells, thus exerting antioxidant effects.[15] [16] Studies have shown that luteolin can reduce prostaglandin production by affecting the arachidonic acid pathway, inhibit the toll-like receptor 4 (TLR4)/MyD88 signaling pathway and the expression of its downstream inflammatory factors, and modulate the polarization of bone marrow-derived macrophages by regulating phosphorylated signal transducers and activators of transcription (p-STAT), thereby adjusting the expression of inflammatory mediators.[17] [18] [19] β-sitosterol, a plant sterol, has anti-inflammatory, antioxidant, and antimicrobial effects.[20] It can inhibit the activation of the nucleotide-binding oligomerization domain, leucine-rich repeat, and pyrin domain-containing 3 (NLRP3) inflammasome in macrophages, thereby inhibiting the generation of CRISPR-associated protein 1 (CAS1) and reducing the production of TNF-α, interleukin-1β (IL-1β), and IL-6, which contributes to its anti-inflammatory effect.[21] Additionally, β-sitosterol and its derivatives can inhibit the overexpression of TLR4 and nuclear transcription factor-κB to reduce liver damage, and enhance the expression of NRF-2 and HO-1 to suppress oxidative stress.[22] These findings suggest that Zhenzhu Qingyuan Granules may exert its acid-suppressing and anti-inflammatory effects by modulating inflammatory responses. Further analysis of the action targets of Zhenzhu Qingyuan Granules revealed that the effective components and potential targets for treating GERD include TP53, AKT1, TNF, etc. TP53, a tumor suppressor gene located on chromosome 17p13,[23] is mutated in most esophageal adenocarcinomas and serves as a potential biomarker for Barrett's esophagus progression to adenocarcinoma.[24] Studies show that acidic reflux can inhibit TP53 activity through free radical-induced lipid peroxidation and cyclooxygenase-2 (COX2) responses in GERD patients.[25] AKT, also known as PKB, plays a crucial role in various signal transduction pathways related to cell growth, division, apoptosis inhibition, and angiogenesis, particularly closely related to in inflammation, with AKT1 being one of its important subtypes.[26] [27] Gastroesophageal reflux upregulates COX2 expression and prostaglandin synthesis by activating AKT, and further promotes Barrett's esophagus transformation to adenocarcinoma, with closer relation with AKT1.[28] TNF, commonly secreted by macrophages or activated T lymphocytes, includes TNF-α and TNF-β as the common TNF subtypes, and is involved in killing tumor cells, enhancing neutrophil phagocytosis, and anti-infection function.[29] Research has confirmed that serum inflammatory biomarkers were elevated in patients with achalasia of cardia, and TNF-α may be related to the pathogenesis of achalasia.[30] Additionally, regulating TNF-α expression can improve the inflammatory response in acute reflux esophagitis in rats to reduce esophageal mucosal damage.[31]
Conclusion
Clinical multicenter randomized controlled trial has shown that Zhenzhu Qingyuan Granules are more effective than using rabeprazole alone in treating GERD of liver–stomach stagnated heat pattern, with better improvements in patient symptoms and endoscopic mucosal appearance. Network pharmacology analysis reveals that Zhenzhu Qingyuan Granules act on multiple targets in treating GERD, with main targets of TP53, AKT1, and TNF, providing new targets for further research on Chinese medicine treatment of GERD. However, this study has limitations: it only assessed the liver–stomach stagnated heat pattern and did not evaluate other patterns. Future research will progressively refine clinical studies on different TCM syndromes. Regarding the action mechanism, this study only performed preliminary analysis of potential targets, and further in vivo and in vitro experiments will be conducted to validate the results.
Conflict of Interest
The authors declare no conflict of interest.
CRediT Authorship Contribution Statement
Mengge Li: methodology, investigation, and writing-original draft. Zhibo Dang: methodology and writing-original draft. Peiguo Qian: project administration, investigation, and resources. Zhenhuan Yang and Lei Luo: formal analysis. Bo Li, Xingzhou Xia, and Yingjie Ma: investigation and resources. Zhongqin Dang and Yuliang Wang: conceptualization, resources, and writing-review and editing.
-
References
- 1 Zheng Z, Shang Y, Wang N. et al. Current advancement on the dynamic mechanism of gastroesophageal reflux disease. Int J Biol Sci 2021; 17 (15) 4154-4164
- 2 Smith W, Davila N. Gastroesophageal reflux disease: 2021 guideline updates and clinical pearls. Nurse Pract 2023; 48 (07) 24-25
- 3 Wang P, Wang FY, Lan Y. et al. Exploration of clinical advantages of traditional Chinese medicine in gastroesophageal reflux disease. Chin J Exp Tradit Med Formul 2023; 29 (12) 199-208
- 4 Zhang HB, Zhou BT, Tang XD. Consensus of traditional Chinese medicine diagnosis and treatment experts on gastroesophageal reflux disease (2023). J Tradit Chin Med 2023; 64 (18) 1935-1944
- 5 Li JX, Chen J, Li Y. Consensus on the diagnosis and treatment of gastroesophageal reflux disease by combining traditional Chinese and western medicine. Chin J Integr Tradit Chin West Med Dig Med 2018; 3: 221-232
- 6 Zhang SS, Zhu SL, Wang HW. et al. Consensus opinion of traditional Chinese medicine diagnosis and treatment experts on gastroesophageal reflux disease. Chin J Integr Tradit Chin West Med Dig Med 2017; 05: 321-326
- 7 State Food and Drug Administration. Guiding Principles for Clinical Research of New Traditional Chinese Medicine Drugs. Beijing: China Medical Technology Press; 2002: 366-367
- 8 Yang ZH, Jia ZJ, Suo FY. et al. Research on the mechanism of Huanglian Jiedu Tang in treating ulcerative colitis based on network pharmacology. Mod J Integr Tradit Chin West Med 2022; 03: 359-367
- 9 Xiao YL. Comparison of consensus or guideline interpretations on gastroesophageal reflux disease in multiple parts of the world. Shanghai Med 2022; 45 (11) 745-749
- 10 Peng RL, Zhang ZY. Comparative interpretation of consensus and guidelines on gastroesophageal reflux disease between the east and the west. Gastroenterology 2022; 27 (10) 596-600
- 11 Li NN, Zhao S. Research progress in the treatment of gastroesophageal reflux disease with traditional Chinese medicine. Chin For Med Res 2024; 22 (06) 151-154
- 12 Wang YR, Yuan M, Zhang L. et al. Research progress on the antioxidant effect and related mechanisms of quercetin. J Nutr 2022; 44 (02) 204-208
- 13 Gupta SS, Azmi L, Mohapatra PK. et al. Flavonoids from whole plant of Euphorbia hirta and their evaluation against experimentally induced gastroesophageal reflux disease in rats. Pharmacogn Mag 2017; 13 (49, Suppl 1): S127-S134
- 14 Rao CV, Vijayakumar M. Effect of quercetin, flavonoids and alpha-tocopherol, an antioxidant vitamin, on experimental reflux oesophagitis in rats. Eur J Pharmacol 2008; 589 (1–3): 233-238
- 15 Jiang YL, Li WY, Feng S. et al. Research progress on structural modification and biological activity of luteolin. Chin Herb Med 2023; 54 (20) 6889-6902
- 16 Wang W, He P, Jiang XM. The anti-inflammatory and antioxidant effects of luteolin and its flavonoid glycosides. Shipin Kexue 2020; 41 (17) 208-215
- 17 Yu Q, Wu GZ. Research progress on the anti-inflammatory mechanism of luteolin. Pharm Res 2019; 38 (02) 108-119
- 18 Zhang SR, Zhang QY. The regulatory effect of luteolin on rat Aspergillus fumigatus keratitis through the TLR4/MyD88 signaling pathway. J Jilin Univ 2021; 47 (02) 315-322
- 19 Shi JF, Wang SX, Cao M. et al. The effect of luteolin on the polarity and expression of inflammatory factors in BMDM. Chin J Nosocom 2020; 30 (23) 3568-3573
- 20 Chen YK, Zeng A, Luo ZH. et al. β- Research progress on the pharmacological effects of sitosterol. J Guangdong Pharmac Univ 2021; 37 (01) 148-153
- 21 Liao PC, Lai MH, Hsu KP. et al. Identification of β-sitosterol as in vitro anti-inflammatory constituent in Moringa oleifera . J Agric Food Chem 2018; 66 (41) 10748-10759
- 22 Yin Y, Liu X, Liu J. et al. Beta-sitosterol and its derivatives repress lipopolysaccharide/d-galactosamine-induced acute hepatic injury by inhibiting the oxidation and inflammation in mice. Bioorg Med Chem Lett 2018; 28 (09) 1525-1533
- 23 Dong MM, Chai XK, Liu XC. et al. Research progress in molecular biology of gastroesophageal reflux disease. Chin J Comp Med 2022; 32 (10) 148-154
- 24 Li S, Chung DC, Mullen JT. Screening high-risk populations for esophageal and gastric cancer. J Surg Oncol 2019; 120 (05) 831-846
- 25 Majka J, Wierdak M, Szlachcic A. et al. Interaction of epidermal growth factor with COX-2 products and peroxisome proliferator-activated receptor-γ system in experimental rat Barrett's esophagus. Am J Physiol Gastrointest Liver Physiol 2020; 318 (03) G375-G389
- 26 Li Q, Li Z, Luo T. et al. Targeting the PI3K/AKT/mTOR and RAF/MEK/ERK pathways for cancer therapy. Mol Biomed 2022; 3 (01) 47
- 27 Manning BD, Toker A. AKT/PKB signaling: navigating the network. Cell 2017; 169 (03) 381-405
- 28 Buttar SN, Falk WG, DeMars JC. et al. Abstract PR-03: Aspirin mediated downregulation of Warburg kinase AKT1 in patients with Barrett's esophagus: implications in neoplastic transformation. Cancer Prev Res (Phila) 2012; 5 (Suppl 11): 5
- 29 van Loo G, Bertrand MJM. Death by TNF: a road to inflammation. Nat Rev Immunol 2023; 23 (05) 289-303
- 30 Clayton S, Cauble E, Kumar A. et al. Plasma levels of TNF-α, IL-6, IFN-γ, IL-12, IL-17, IL-22, and IL-23 in achalasia, eosinophilic esophagitis (EoE), and gastroesophageal reflux disease (GERD). BMC Gastroenterol 2019; 19 (01) 28
- 31 Nam HH, Nan L, Choo BK. Anti-inflammation and protective effects of Anethum graveolens L. (Dill Seeds) on esophageal mucosa damages in reflux esophagitis-induced rats. Foods 2021; 10 (10) 2500
Address for correspondence
Publication History
Received: 11 April 2024
Accepted: 19 June 2024
Article published online:
30 September 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Zheng Z, Shang Y, Wang N. et al. Current advancement on the dynamic mechanism of gastroesophageal reflux disease. Int J Biol Sci 2021; 17 (15) 4154-4164
- 2 Smith W, Davila N. Gastroesophageal reflux disease: 2021 guideline updates and clinical pearls. Nurse Pract 2023; 48 (07) 24-25
- 3 Wang P, Wang FY, Lan Y. et al. Exploration of clinical advantages of traditional Chinese medicine in gastroesophageal reflux disease. Chin J Exp Tradit Med Formul 2023; 29 (12) 199-208
- 4 Zhang HB, Zhou BT, Tang XD. Consensus of traditional Chinese medicine diagnosis and treatment experts on gastroesophageal reflux disease (2023). J Tradit Chin Med 2023; 64 (18) 1935-1944
- 5 Li JX, Chen J, Li Y. Consensus on the diagnosis and treatment of gastroesophageal reflux disease by combining traditional Chinese and western medicine. Chin J Integr Tradit Chin West Med Dig Med 2018; 3: 221-232
- 6 Zhang SS, Zhu SL, Wang HW. et al. Consensus opinion of traditional Chinese medicine diagnosis and treatment experts on gastroesophageal reflux disease. Chin J Integr Tradit Chin West Med Dig Med 2017; 05: 321-326
- 7 State Food and Drug Administration. Guiding Principles for Clinical Research of New Traditional Chinese Medicine Drugs. Beijing: China Medical Technology Press; 2002: 366-367
- 8 Yang ZH, Jia ZJ, Suo FY. et al. Research on the mechanism of Huanglian Jiedu Tang in treating ulcerative colitis based on network pharmacology. Mod J Integr Tradit Chin West Med 2022; 03: 359-367
- 9 Xiao YL. Comparison of consensus or guideline interpretations on gastroesophageal reflux disease in multiple parts of the world. Shanghai Med 2022; 45 (11) 745-749
- 10 Peng RL, Zhang ZY. Comparative interpretation of consensus and guidelines on gastroesophageal reflux disease between the east and the west. Gastroenterology 2022; 27 (10) 596-600
- 11 Li NN, Zhao S. Research progress in the treatment of gastroesophageal reflux disease with traditional Chinese medicine. Chin For Med Res 2024; 22 (06) 151-154
- 12 Wang YR, Yuan M, Zhang L. et al. Research progress on the antioxidant effect and related mechanisms of quercetin. J Nutr 2022; 44 (02) 204-208
- 13 Gupta SS, Azmi L, Mohapatra PK. et al. Flavonoids from whole plant of Euphorbia hirta and their evaluation against experimentally induced gastroesophageal reflux disease in rats. Pharmacogn Mag 2017; 13 (49, Suppl 1): S127-S134
- 14 Rao CV, Vijayakumar M. Effect of quercetin, flavonoids and alpha-tocopherol, an antioxidant vitamin, on experimental reflux oesophagitis in rats. Eur J Pharmacol 2008; 589 (1–3): 233-238
- 15 Jiang YL, Li WY, Feng S. et al. Research progress on structural modification and biological activity of luteolin. Chin Herb Med 2023; 54 (20) 6889-6902
- 16 Wang W, He P, Jiang XM. The anti-inflammatory and antioxidant effects of luteolin and its flavonoid glycosides. Shipin Kexue 2020; 41 (17) 208-215
- 17 Yu Q, Wu GZ. Research progress on the anti-inflammatory mechanism of luteolin. Pharm Res 2019; 38 (02) 108-119
- 18 Zhang SR, Zhang QY. The regulatory effect of luteolin on rat Aspergillus fumigatus keratitis through the TLR4/MyD88 signaling pathway. J Jilin Univ 2021; 47 (02) 315-322
- 19 Shi JF, Wang SX, Cao M. et al. The effect of luteolin on the polarity and expression of inflammatory factors in BMDM. Chin J Nosocom 2020; 30 (23) 3568-3573
- 20 Chen YK, Zeng A, Luo ZH. et al. β- Research progress on the pharmacological effects of sitosterol. J Guangdong Pharmac Univ 2021; 37 (01) 148-153
- 21 Liao PC, Lai MH, Hsu KP. et al. Identification of β-sitosterol as in vitro anti-inflammatory constituent in Moringa oleifera . J Agric Food Chem 2018; 66 (41) 10748-10759
- 22 Yin Y, Liu X, Liu J. et al. Beta-sitosterol and its derivatives repress lipopolysaccharide/d-galactosamine-induced acute hepatic injury by inhibiting the oxidation and inflammation in mice. Bioorg Med Chem Lett 2018; 28 (09) 1525-1533
- 23 Dong MM, Chai XK, Liu XC. et al. Research progress in molecular biology of gastroesophageal reflux disease. Chin J Comp Med 2022; 32 (10) 148-154
- 24 Li S, Chung DC, Mullen JT. Screening high-risk populations for esophageal and gastric cancer. J Surg Oncol 2019; 120 (05) 831-846
- 25 Majka J, Wierdak M, Szlachcic A. et al. Interaction of epidermal growth factor with COX-2 products and peroxisome proliferator-activated receptor-γ system in experimental rat Barrett's esophagus. Am J Physiol Gastrointest Liver Physiol 2020; 318 (03) G375-G389
- 26 Li Q, Li Z, Luo T. et al. Targeting the PI3K/AKT/mTOR and RAF/MEK/ERK pathways for cancer therapy. Mol Biomed 2022; 3 (01) 47
- 27 Manning BD, Toker A. AKT/PKB signaling: navigating the network. Cell 2017; 169 (03) 381-405
- 28 Buttar SN, Falk WG, DeMars JC. et al. Abstract PR-03: Aspirin mediated downregulation of Warburg kinase AKT1 in patients with Barrett's esophagus: implications in neoplastic transformation. Cancer Prev Res (Phila) 2012; 5 (Suppl 11): 5
- 29 van Loo G, Bertrand MJM. Death by TNF: a road to inflammation. Nat Rev Immunol 2023; 23 (05) 289-303
- 30 Clayton S, Cauble E, Kumar A. et al. Plasma levels of TNF-α, IL-6, IFN-γ, IL-12, IL-17, IL-22, and IL-23 in achalasia, eosinophilic esophagitis (EoE), and gastroesophageal reflux disease (GERD). BMC Gastroenterol 2019; 19 (01) 28
- 31 Nam HH, Nan L, Choo BK. Anti-inflammation and protective effects of Anethum graveolens L. (Dill Seeds) on esophageal mucosa damages in reflux esophagitis-induced rats. Foods 2021; 10 (10) 2500