

Subscribe to RSS
DOI: 10.1055/s-0044-1790223
Clinical Profile and Outcomes of Childhood Wilms Tumors Treated in a Tertiary Cancer Center from North India
Authors

Abstract
In India and other lower-middle-income countries, the progress in the management of Wilms tumor (WT) has lagged behind when compared to the developed countries. In the current study, we highlight the outcomes of 61 children with WT treated at an oncological center in northern India. Our study found that the patient demographics, including age and gender distribution, closely paralleled other Indian studies. Notably, 24% of patients had distant metastasis at diagnosis. An upfront biopsy was performed in majority of the patient with a remarkable concordance rate of over 90%, with no significant complications associated with the procedure. Our surgical approach, guided by image-defined risk factors, resulted in 84% of patients undergoing delayed surgery after chemotherapy. Notably, the incidence of intraoperative complications, including tumor spill, was minimal. Treatment abandonment and toxic death due to sepsis emerged as significant challenges, affecting 22% and 7% of our patient cohort, respectively. The 3-year event-free survival (EFS) and overall survival were 70% and 84%, respectively. The age group of 6 to 8 years and stage V disease emerged as adverse factors influencing EFS. In summary, our study highlights the multifaceted nature of WT management in resource-constrained settings with survival rates promising but still lagging behind high-income countries. Addressing challenges such as treatment abandonment and reducing toxic death is imperative to enhance outcomes of WT in India.
Keywords
chemotherapy - India - lower-middle-income countries - nephrectomy - toxicity - Wilms tumorIntroduction
Renal tumors account for 5% of all pediatric cancers with Wilms tumor (WT) being the most common.[1] [2] Over the past five decades, two major international multidisciplinary cooperative consortia, namely, the Children's Oncology Group (COG) and International Society of Paediatric Oncology Renal Tumor Study Group (SIOP-RTSG), have conducted successive studies that have yielded remarkable advancements in outcomes, surpassing 90% in developed countries. However, the progress achieved in WT in lower middle-income countries (LMICs) and low-income countries has been notably disparate, with outcomes consistently lagging behind those in developed nations.[3] [4] [5] [6] A recent systematic review highlighted the overall survival (OS) of WT in India to range between 48 and 89%.[7] The disparity in outcomes can be attributed to certain unique challenges, including a high disease burden, treatment-related mortality, limited access to surgical expertise, and treatment abandonment, all of which contribute to poor outcomes among pediatric WT in LMICs. In the current study, we report on our experience of treating children less than 15 years of age with WT over a 3-year period from a single center in northern India.
Materials and Methods
This was a retrospective study, approved by the Institutional Ethics Committee (Approval ID-11000520). Data related to patients with WT, aged less than 15 years, who were treated at our institute between May 1, 2018 and November 2, 2020 were collected from the electronic medical record and followed up till December 31, 2022. Staging procedure included contrast-enhanced computed tomography (CECT) of the thorax-abdomen-pelvis. The three-dimensional images (coronal, sagittal, and axial planes) of the renal mass were evaluated and following features were documented by the radiologists: (1) the tumor extension in relation to the midline (imaginary line going through the midline of the vertebral body); (2) planes (smooth, indistinct, or lobulated) between the tumor and surrounding structures; (3) presence of tumor thrombus (in renal vein, inferior vena cava [IVC], or in ureter); and (4) retroperitoneal lymphadenopathy, whether encasing the vessels or not. The decision of upfront versus delayed nephrectomy was guided by predefined image-defined risk factors such as large size of the tumor, extent of tumor thrombus, and retroperitoneal lymphadenopathy encasing vessels, as described previously by Qureshi et al.[8] In the absence of the above mentioned high-risk features, patient underwent upfront nephrectomy while those with high-risk features, received 4 to 6 weeks of chemotherapy followed by reassessment using CECT thorax-abdomen-pelvis followed by surgery. Liver and lung lesions on CECT scans which were radiologically characteristics as per UMBRELLA SIOP-RTSG 2016 protocol, were considered metastases.[9] Response Evaluation Criteria in Solid Tumors criteria was used to assess metastatic response in post-neoadjuvant chemotherapy wherein complete response was defined as disappearance of all lesions and partial response was defined as ≥ 30% decrease in sum of the longest diameters of the target lesions with no new lesions in the response assessment scan.
Subsequent treatment was tailored based on tumor histology and local stage as per SIOP strategy.[9] Image-guided biopsy was reserved for patients with atypical findings on imaging. Biopsy was offered in cases where the bulk of the tumor was in the suprarenal fossa with adrenal gland infiltration and not showing positive claw sign with the ipsilateral kidney which was indicative of the organ from which the tumor was arising, thus, posing an imaging dilemma of a likely differential diagnosis of a neuroblastoma. For patients in the upfront nephrectomy group, histological classification was as per COG (favorable and unfavorable), while the SIOP classification (low, intermediate, high risk) was employed for the delayed nephrectomy group.[10] Patients who were upfront operated at another center and histological diagnosis confirmed at our institute were also included in this study. If the surgical details (spill or rupture, lymph node [LN] sampling) of these referred patients were unavailable, they were managed as local stage III and treated with three-drug regimen with whole abdomen irradiation (WAI) at a dose of 10.8 gray (Gy) over 6 fractions. Patients with unfavorable histology with local stage II and stage III of any other histology without spillage were treated with flank radiotherapy (RT) at a dose of 10.8 Gy over 6 fractions. All the patients with upfront lung metastasis and complete response post-induction chemotherapy received additional whole lung irradiation (WLI) at a dose of 12 Gy over 8 fractions. Patients with bilateral WT received 6 to 12 weeks of three-drug chemotherapy, followed by response assessment for nephron-sparing surgery.
The primary objective of this study was to assess the event-free survival (EFS) and overall survival (OS) of patients with WT. Secondary objectives were to assess the treatment abandonment rates, relapse patterns, prognostic factors influencing survival, impact of radiation therapy timing on outcomes, and chemotherapy-related toxicity. OS was calculated from the date of diagnosis to date of death due to any cause or last follow-up and EFS was calculated from the date of diagnosis to the date of abandonment, relapse, disease progression, death, or last follow-up whichever occurred earlier. EFS and OS analysis were presented as Kaplan–Meier curves. All demographic data were summarized as descriptive statistics, and continuous data as median (range). Conventional univariate and multivariate analyses were performed by Cox proportional-hazard model using R Statistical Software (v4.1.2; R Core Team 2021).
Results
Eight-four patients with renal masses were registered during the aforementioned time period. Out of these, 23 (27%) were excluded due to the following reasons, presented with relapse WT after taking treatment outside (n = 10), second opinion (n = 3), and non-WT histology (n = 10). Consequently, 61 children met the inclusion criteria for the purpose of this study ([Fig. 1]).
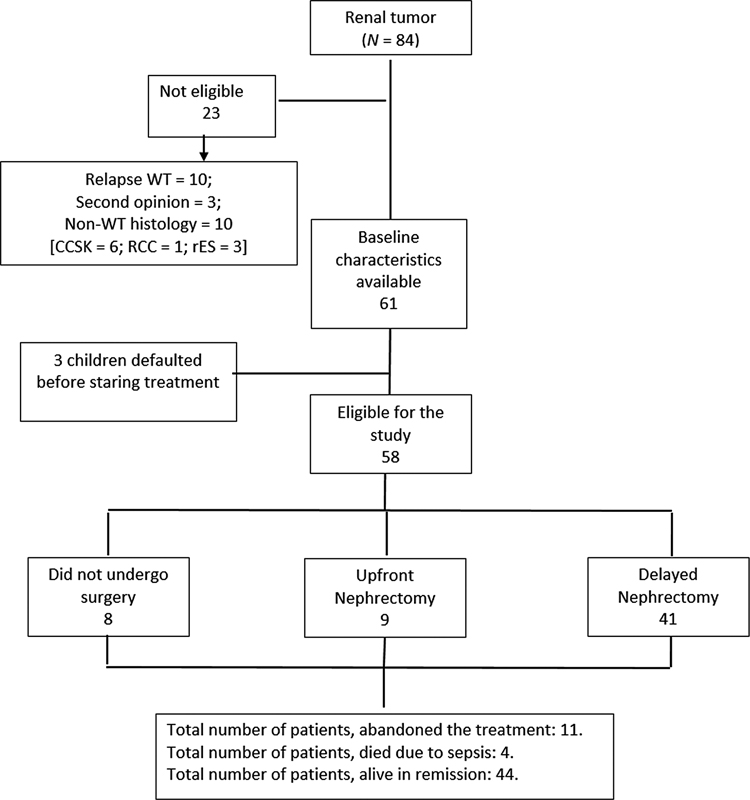
The median age of the cohort was 42.2 (range: 5–120) months with a male-to-female ratio of 1.5:1. Three children were syndromic of which 2 had WAGR syndrome (WT, aniridia, genitourinary malformation, and mental retardation) and 1 had WT along with microcephaly and developmental delay. After initial evaluation, 3 children defaulted before commencement of therapy.
Among the 58 patients who underwent treatment, 25 (43%) had right-sided tumors, 28 (48%) had left-sided tumors, and 5(8%) had bilateral tumors. Distant metastasis was present in 14 (24%) patients. Sites of metastasis included lung only, liver only, and both lung and liver in 11 (79%), 1 (7%), and 2 (14%) patients, respectively. Post-neoadjuvant chemotherapy, complete and partial metastatic response were achieved in 3 and 7 children, respectively, but there was no response in 1 child.
Nine (16%) of 58 patients underwent upfront nephrectomy; Local stage I: 1 (11%), stage II: 3 (33%), and stage III: 5 (56%). Among them, 4 received two-drug and 5 received three-drug adjuvant chemotherapy (AC). The remaining 49 (84%) received upfront chemotherapy. Twenty-three (47%) of 49 patients in the delayed nephrectomy group underwent ultrasonography-guided core needle biopsy prior to therapy. No complications were attributed to biopsy. Biopsy was consistent with WT in 21 (91%) patients while 2 (9%) yielded inconclusive results. These 2 patients subsequently received neoadjuvant chemotherapy (NACT) for WT. Among 49 children of delayed nephrectomy group, 30 children received two-drug and remaining 19 children received three-drug nonadjuvant chemotherapy (NACT). Cumulative dose of anthracycline used in the three-drug regimen was 300 mg/m2.
Within the delayed nephrectomy group, 8 children did not undergo surgery: 2 with unilateral WT succumbed to sepsis during chemotherapy, 1 with unilateral WT died at home due to unknown reasons, 1 with unilateral WT had disease progression during chemotherapy, and 4 of 5 children with bilateral WT abandoned treatment during the various phases of chemotherapy (after 1st, 3rd, 7th, and 11th week of therapy). The remaining 41 children in the delayed nephrectomy group underwent open transperitoneal nephrectomy as per protocol. In the delayed nephrectomy group, 26 children had data with respect to tumor volume at the baseline as well as before surgery. This analysis showed a significant reduction of average tumor volume (707.43 vs. 360.31 mL). Detailed staging and histological information are provided in [Table 1].
Abbreviations: COG, Children's Oncology Group; SIOP, International Society of Paediatric Oncology; WT, Wilms tumor.
A total of 50 children underwent nephrectomy and LN samplings (9 upfront, 41 delayed). LNs sampling was done from the five different stations as an institutional policy and 6 children had LN involvement. For the right-sided tumor, LNs were sampled from hilar, supra- and infrahilar paracaval, as well as interaortocaval supra- and infrahilar stations ([Fig. 2A]). Similarly, for left-sided tumor, LNs were sampled from hilar, supra- and infrahilar paraaortic, as well as interaortocaval supra- and infrahilar stations ([Fig. 2B]).[11] Among 50 cases, 8 had infrahepatic intravascular tumor thrombus and 1 had suprahepatic extension till right atrium, for which child had been put under cardiopulmonary bypass at the time of thrombectomy. There were no intraoperative mortalities. One child with bilateral WT, underwent left nephrectomy and right nephron-sparing surgery died due to sepsis in the immediate postoperative period. Another child in the upfront group and 4 children in the delayed nephrectomy group developed intestinal obstruction. All of them underwent laparotomy and adhesiolysis.

During adjuvant chemotherapy, one child with stage III disease succumbed to sepsis while another child died at home for unknown reasons. Eight children could not complete the prescribed adjuvant chemotherapy due to nationwide lockdown due to coronavirus disease 2019 (COVID-19) and other social issues.
Adjuvant RT was administered to 21 children. Among them, 10 (48%) received flank RT at a dose of 10.8 Gy over 6 fractions, and an additional 4 (19%) patients underwent WAI with the same dose. In addition, 2 (9.5%) received WLI at a dose of 12 Gy over 8 fractions, 3 received both WLI and WAI, 1 (4.8%) received liver RT, and 1 (4.8%) received RT without documented reason. The median time to commence radiation following nephrectomy was available for 18 patients and was 44 days (range: 12–72 days), with only 1 patient receiving RT within 14 days of surgery.
After a median follow-up of 32.4 months, 13 (22%) children abandoned therapy, 4 (7%) expired due to sepsis, 3 (5%) had relapse of disease, and 3 (5%) died due to unknown reasons. The 3-year EFS and OS of the entire cohort were 70.13 ± 8.71 and 84.30 ± 8.27%, respectively ([Figs. 3] and [4]). Excluding patient who abandoned treatment, the 3-year EFS and OS were 78 ± 0.06% and 82.1 ± 0.05%, respectively.


The 3-year EFS of stage I, II, III, and IV patients were 92.3 ± 7.4%, 81.8 ± 11.6%, 82.3 ± 11.7%, and 70.7 ± 14.3%, respectively. While the respective 3-year OS according to stage was 100% for stage I and II, 91.7 ± 8.0% and 80.8.5 ± 12.2% for stage III and IV, respectively. There were no survivors among patients with stage V disease.
Cox proportional-hazard model analysis revealed that the age group of 6 to 8 years and stage V disease negatively influenced EFS, both on univariate and multivariate analysis ([Table 2] and [Fig. 5]). Among long-term sequelae, 2 nonsyndromic children of unilateral WT (3%) developed chronic renal failure and 1 child (1.5%) developed secondary leukemia. Notably, no cases of cardiotoxicity were reported in patient who received anthracyclines.

Abbreviations: CI, confidence interval; HR, hazard ratio.
Discussion
Our hospital stands as one of the largest tertiary care oncological center in northern India, annually catering to approximately 300 children afflicted with cancer. The demographic characteristics observed in our study, including age and gender distribution, align with other studies from India.[7] Additionally, in the current study about quarter of the patients had distant metastasis. This rate is higher in comparison to approximately 10% incidence found in developed countries but is consistent with several reports from India.[7] [8] [11] In an LMIC setting, upfront biopsy for suspected WT is a common practice.[12] In our study, about half of the patients in the delayed nephrectomy group underwent a biopsy before the initiation of therapy, yielding a high concordance rate of over 90%. While apprehensions surrounding biopsy include procedure-related risks, potential recurrence of tumor at the biopsy track, and delay in initiation of therapy, none of which were present in our study population.[1] [13] Our surgical approach for WT mirrors that proposed by Qureshi et al, with upfront surgery reserved for a selected group of patients lacking certain image-defined risk factors as described previously while remaining patients offered chemotherapy before surgery as per SIOP.[8] This hybrid approach resulted in 84% of patients in the current study undergoing delayed surgery following chemotherapy. Notably, the incidence of intraoperative complications including tumor spill was minimal (0.12%) among these patients. The utilization of preoperative chemotherapy may also contribute to improved surgical outcomes, facilitating better resection of the tumor mass from the surrounding structures and aiding the separation of the tumor thrombus from the intimal wall of IVC.[8] [14] While a small proportion of patients in the current study experienced intestinal obstruction requiring surgical reexploration, these cases were resolved without major complications.
Our study highlighted a high abandonment rate of 22%, a concerning issue in the treatment of childhood cancer in LMICs.[5] [6] [7] These high abandonment rates happened during the formative years of our hospital and particularly during the COVID-19 pandemic when we witnessed a nationwide lockdown. To address this challenge, we have since implemented various measures, including financial support for therapy, provision of accommodation for patient and their families during active treatment, transportation services to hospital, and monthly ration provisions for malnourished children in association with several nongovernmental organizations. Another major concern in the current study was the toxic deaths due to microbiologically proven sepsis, accounting for approximately 7% of cases. This figure is relatively high for a disease that is typically treated with a relatively less intensive chemotherapy. Our efforts have thus focused on bolstering the nutritional status of children with cancer and educating caregivers about infection control measures, aiming to curtail sepsis-related complications. Our study demonstrated a 3-year EFS of 70%, encompassing all risk groups. These results are similar or slightly better in comparison to other reports from India,[7] [15] [16] but inferior to data from high-income- countries (HICs).[17] [18] It is worth noting that the estimated age-standardized mortality rate for renal tumor in the age group of 0 to 14 years is 0.2 per million in India as against 0.05 per million in the United States of America.[19] [20] Discrepancies in EFS and OS within our study could be attributed to a small subset of patients who abandoned treatment toward the later stages of adjuvant chemotherapy, predominantly due to the COVID-19 lockdown restrictions, but continue to be in remission. One of notable observations in our study was the age-dependent impact on survival, with the age group of 6 to 8 years adversely affecting the EFS. Similar to our study, older age at diagnosis was found to be an independent risk factor for relapse in a retrospective review of a pooled analysis of two successive studies by the SIOP group which included over 5,000 patients.[21] These findings might be attributed to variations in tumor biology, treatment responses, or physiological factors across different age groups. Another crucial determinant of outcomes in our study was the stage of the disease at diagnosis. Multivariate analysis reinforced the adverse effect of stage V disease on outcomes. In the current study, 5 (8%) patients had stage V disease, of whom 4 defaulted therapy and 1 succumbed to sepsis. Though the outcomes of bilateral WT in HIC have improved over the years with the use of preoperative chemotherapy and subsequent nephron sparing surgery, it still continues to be a challenge in LMICs due to the need of surgical expertise and extensive posttreatment rehabilitation. Such patients are often at an increased risk of end-stage renal disease.[22] [23]
In summary, our study's insights underscore the multifaceted nature of WT management in resource-constrained settings. The survival rates of our WT patients are comparable to other reports from LMICs, although lagging behind HICs. Notably, advanced age and bilateral disease were identified as factors adversely influencing survival. Further improvement in survival can be achieved through a holistic approach that addresses treatment abandonment and adapting comprehensive infection control measures and enhanced caregiver education.
Conflict of Interest
None declared.
Acknowledgments
We would like to thank Tahamina Bano from Medical and Social Worker Department and Saket Kumar for meticulous data collection.
-
References
- 1 Jackson TJ, Williams RD, Brok J. et al; Children's Cancer and Leukaemia Group (CCLG) Renal Tumours Group. The diagnostic accuracy and clinical utility of pediatric renal tumor biopsy: report of the UK experience in the SIOP UK WT 2001 trial. Pediatr Blood Cancer 2019; 66 (06) e27627
- 2 Nakata K, Colombet M, Stiller CA, Pritchard-Jones K, Steliarova-Foucher E. IICC-3 Contributors. Incidence of childhood renal tumours: an international population-based study. Int J Cancer 2020; 147 (12) 3313-3327
- 3 Cunningham ME, Klug TD, Nuchtern JG. et al. Global disparities in Wilms tumor. J Surg Res 2020; 247: 34-51
- 4 Asfour HY, Khalil SA, Zakaria AS, Ashraf ES, Zekri W. Localized Wilms' tumor in low-middle-income countries (LMIC): how can we get better?. J Egypt Natl Canc Inst 2020; 32 (01) 32
- 5 Njuguna F, Martijn HA, Kuremu RT. et al. Wilms tumor treatment outcomes: perspectives from a low-income setting. J Glob Oncol 2016; 3 (05) 555-562
- 6 Arora RS, Challinor JM, Howard SC, Israels T. Improving care for children with cancer in low-and middle-income countries-a SIOP PODC initiative. Pediatr Blood Cancer 2016; 63 (03) 387-391
- 7 Srinivasan S, Ramanathan S, Prasad M. Wilms tumor in India: a systematic review. South Asian J Cancer 2022; 12 (02) 206-212
- 8 Qureshi SS, Kembhavi SA, Bhagat M. et al. Customized approach for upfront or delayed resection using radiological criteria in unilateral, nonmetastatic pediatric renal tumors: a prospective study. Pediatr Blood Cancer 2019; 66 (Suppl. 03) e27815
- 9 van den Heuvel-Eibrink MM, Hol JA, Pritchard-Jones K. et al; International Society of Paediatric Oncology—Renal Tumour Study Group (SIOP–RTSG). Position paper: rationale for the treatment of Wilms tumour in the UMBRELLA SIOP-RTSG 2016 protocol. Nat Rev Urol 2017; 14 (12) 743-752
- 10 Irtan S, Ehrlich PF, Pritchard-Jones K. Wilms tumor: “State-of-the-art” update, 2016. In: Seminars in Pediatric Surgery. WB Saunders; ; October 1, 2016;25(5):250–256
- 11 Qureshi SS, Bhagat M, Kazi M. et al. Standardizing lymph nodal sampling for Wilms tumor: a feasibility study with outcomes. J Pediatr Surg 2020; 55 (12) 2668-2675
- 12 Vu MT, Shalkow J, Naik-Mathuria B. et al. Wilms' tumor in low- and middle-income countries: survey of current practices, challenges, and priorities. Ann Pediatr Surg 2022; 18 (01) 28
- 13 Vujanić GM, Kelsey A, Mitchell C, Shannon RS, Gornall P. The role of biopsy in the diagnosis of renal tumors of childhood: results of the UKCCSG Wilms tumor study 3. Med Pediatr Oncol 2003; 40 (01) 18-22
- 14 Qureshi SS, Bhagat M, Smriti V. et al. Intravascular extension of Wilms tumor: characteristics of tumor thrombus and their impact on outcomes. J Pediatr Urol 2021; 17 (01) 69.e1-69.e8
- 15 Rahiman EA, Trehan A, Jain R. et al. A higher tumor volume and undernutrition at diagnosis adversely affect the survival of children with Wilms tumor: a study of 200 patients. Pediatr Blood Cancer 2022; 69 (11) e29880
- 16 John R, Kurian JJ, Sen S. et al. Clinical outcomes of children with Wilms tumor treated on a SIOP WT 2001 protocol in a tertiary care hospital in south India. J Pediatr Urol 2018; 14 (06) 547.e1-547.e7
- 17 Pritchard-Jones K, Bergeron C, de Camargo B. et al; SIOP Renal Tumours Study Group. Omission of doxorubicin from the treatment of stage II-III, intermediate-risk Wilms' tumour (SIOP WT 2001): an open-label, non-inferiority, randomised controlled trial. Lancet 2015; 386 (9999) 1156-1164
- 18 Oue T, Fukuzawa M, Okita H. et al; Japan Wilms Tumor Study (JWiTS) Group. Outcome of pediatric renal tumor treated using the Japan Wilms Tumor Study-1 (JWiTS-1) protocol: a report from the JWiTS group. Pediatr Surg Int 2009; 25 (11) 923-929
- 19 Sung H, Ferlay J, Siegel RL. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 20 Accessed august 17, 2024 at: https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=population&mode_population=countries&population=900&populations=900&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&group_cancer=1&include_nmsc=0&include_nmsc_other=1
- 21 Hol JA, Lopez-Yurda MI, Van Tinteren H. et al. Prognostic significance of age in 5631 patients with Wilms tumour prospectively registered in International Society of Paediatric Oncology (SIOP) 93-01 and 2001. PLoS One 2019; 14 (08) e0221373
- 22 Ehrlich P, Chi YY, Chintagumpala MM. et al. Results of the first prospective multi-institutional treatment study in children with bilateral Wilms tumor (AREN0534): a report from the Children's Oncology Group. Ann Surg 2017; 266 (03) 470-478
- 23 Agarwala S, Mittal D, Bhatnagar V. et al. Management and outcomes in massive bilateral Wilms' tumors. J Indian Assoc Pediatr Surg 2014; 19 (04) 208-212
Address for correspondence
Publication History
Received: 21 September 2023
Accepted: 29 July 2024
Article published online:
03 September 2024
© 2024. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Jackson TJ, Williams RD, Brok J. et al; Children's Cancer and Leukaemia Group (CCLG) Renal Tumours Group. The diagnostic accuracy and clinical utility of pediatric renal tumor biopsy: report of the UK experience in the SIOP UK WT 2001 trial. Pediatr Blood Cancer 2019; 66 (06) e27627
- 2 Nakata K, Colombet M, Stiller CA, Pritchard-Jones K, Steliarova-Foucher E. IICC-3 Contributors. Incidence of childhood renal tumours: an international population-based study. Int J Cancer 2020; 147 (12) 3313-3327
- 3 Cunningham ME, Klug TD, Nuchtern JG. et al. Global disparities in Wilms tumor. J Surg Res 2020; 247: 34-51
- 4 Asfour HY, Khalil SA, Zakaria AS, Ashraf ES, Zekri W. Localized Wilms' tumor in low-middle-income countries (LMIC): how can we get better?. J Egypt Natl Canc Inst 2020; 32 (01) 32
- 5 Njuguna F, Martijn HA, Kuremu RT. et al. Wilms tumor treatment outcomes: perspectives from a low-income setting. J Glob Oncol 2016; 3 (05) 555-562
- 6 Arora RS, Challinor JM, Howard SC, Israels T. Improving care for children with cancer in low-and middle-income countries-a SIOP PODC initiative. Pediatr Blood Cancer 2016; 63 (03) 387-391
- 7 Srinivasan S, Ramanathan S, Prasad M. Wilms tumor in India: a systematic review. South Asian J Cancer 2022; 12 (02) 206-212
- 8 Qureshi SS, Kembhavi SA, Bhagat M. et al. Customized approach for upfront or delayed resection using radiological criteria in unilateral, nonmetastatic pediatric renal tumors: a prospective study. Pediatr Blood Cancer 2019; 66 (Suppl. 03) e27815
- 9 van den Heuvel-Eibrink MM, Hol JA, Pritchard-Jones K. et al; International Society of Paediatric Oncology—Renal Tumour Study Group (SIOP–RTSG). Position paper: rationale for the treatment of Wilms tumour in the UMBRELLA SIOP-RTSG 2016 protocol. Nat Rev Urol 2017; 14 (12) 743-752
- 10 Irtan S, Ehrlich PF, Pritchard-Jones K. Wilms tumor: “State-of-the-art” update, 2016. In: Seminars in Pediatric Surgery. WB Saunders; ; October 1, 2016;25(5):250–256
- 11 Qureshi SS, Bhagat M, Kazi M. et al. Standardizing lymph nodal sampling for Wilms tumor: a feasibility study with outcomes. J Pediatr Surg 2020; 55 (12) 2668-2675
- 12 Vu MT, Shalkow J, Naik-Mathuria B. et al. Wilms' tumor in low- and middle-income countries: survey of current practices, challenges, and priorities. Ann Pediatr Surg 2022; 18 (01) 28
- 13 Vujanić GM, Kelsey A, Mitchell C, Shannon RS, Gornall P. The role of biopsy in the diagnosis of renal tumors of childhood: results of the UKCCSG Wilms tumor study 3. Med Pediatr Oncol 2003; 40 (01) 18-22
- 14 Qureshi SS, Bhagat M, Smriti V. et al. Intravascular extension of Wilms tumor: characteristics of tumor thrombus and their impact on outcomes. J Pediatr Urol 2021; 17 (01) 69.e1-69.e8
- 15 Rahiman EA, Trehan A, Jain R. et al. A higher tumor volume and undernutrition at diagnosis adversely affect the survival of children with Wilms tumor: a study of 200 patients. Pediatr Blood Cancer 2022; 69 (11) e29880
- 16 John R, Kurian JJ, Sen S. et al. Clinical outcomes of children with Wilms tumor treated on a SIOP WT 2001 protocol in a tertiary care hospital in south India. J Pediatr Urol 2018; 14 (06) 547.e1-547.e7
- 17 Pritchard-Jones K, Bergeron C, de Camargo B. et al; SIOP Renal Tumours Study Group. Omission of doxorubicin from the treatment of stage II-III, intermediate-risk Wilms' tumour (SIOP WT 2001): an open-label, non-inferiority, randomised controlled trial. Lancet 2015; 386 (9999) 1156-1164
- 18 Oue T, Fukuzawa M, Okita H. et al; Japan Wilms Tumor Study (JWiTS) Group. Outcome of pediatric renal tumor treated using the Japan Wilms Tumor Study-1 (JWiTS-1) protocol: a report from the JWiTS group. Pediatr Surg Int 2009; 25 (11) 923-929
- 19 Sung H, Ferlay J, Siegel RL. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 20 Accessed august 17, 2024 at: https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=population&mode_population=countries&population=900&populations=900&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&group_cancer=1&include_nmsc=0&include_nmsc_other=1
- 21 Hol JA, Lopez-Yurda MI, Van Tinteren H. et al. Prognostic significance of age in 5631 patients with Wilms tumour prospectively registered in International Society of Paediatric Oncology (SIOP) 93-01 and 2001. PLoS One 2019; 14 (08) e0221373
- 22 Ehrlich P, Chi YY, Chintagumpala MM. et al. Results of the first prospective multi-institutional treatment study in children with bilateral Wilms tumor (AREN0534): a report from the Children's Oncology Group. Ann Surg 2017; 266 (03) 470-478
- 23 Agarwala S, Mittal D, Bhatnagar V. et al. Management and outcomes in massive bilateral Wilms' tumors. J Indian Assoc Pediatr Surg 2014; 19 (04) 208-212
