

Subscribe to RSS
DOI: 10.1055/s-0044-1788257
Long-Term Outcomes of Thymoma Treated at a Single Institute
Authors

Abstract
Introduction
Thymomas are uncommon tumors that originate from epithelial cells of thymus and may have varying clinical course.
Materials and Methods
A retrospective review of medical records of thymoma patients treated between January 2012 and April 2022 at our institute was conducted.
Results
There were a total of 23 patients (12 males and 11 females) with median age of 52 years (range, 33–77 years). Eleven patients (47.8%) had associated paraneoplastic syndromes of which 10 (43.5%) had myasthenia gravis and 1 (4.3%) had pure red cell aplasia. Average maximal tumor diameter was 62 mm (28–160 mm). Masaoka-Koga stage distribution was as follows: stage I (n = 2, 8.7%), IIA (n = 4, 17.4%), IIB (n = 1, 4.3%), IIIA (n = 2, 8.7%), IIIB (n = 4, 17.4%), IVA (n = 7, 30.4%), and IVB (n = 3, 13.1%). The World Health Organization type B2 was the commonest histology (n = 12, 52.17%), followed by B3 (n =7, 30.4%), B1 (n = 2, 8.7%), AB (n = 1,4.3%), and A (n = 1, 4.3%). Six patients received neoadjuvant chemotherapy with cyclophosphamide regimen, 22 (95.6%) underwent surgery, and 1 patient received adjuvant chemotherapy. R0 resection was attained in 20 (91%) patients, R1 resection in 1 (4.5%) patient, and R2 in 1 (4.5%) patient. All operated patients underwent postoperative radiotherapy (45–60 Gy in 25–30 fractions). Four patients relapsed at a median duration of 14 months (2–26 months). At a median follow-up of 6 years, 5-year overall survival was 67.1% and 5-year progression-free survival was 66.6%. Local control at 5 years was 86.6%.
Conclusion
Despite majority of our patients presenting at an advanced stage, the local control rates are encouraging and reinforce multimodality approach.
Keywords
thymoma - thymic epithelial tumors - myasthenia gravis - paraneoplastic syndromes - radiation - thymusIntroduction
Thymomas belong to a spectrum of thymic epithelial tumors (TETs) classified by the World Health Organization (WHO), wherein the other subtypes comprise thymic carcinomas, carcinoid, small cell carcinoma, and large cell neuroendocrine carcinoma.[1] Together, these subtypes constitute less than 1% of all neoplasms and up to 30% of all anterior mediastinal neoplasms in adults.[2] They are further classified into type A (including an atypical variant), AB, B (B1, B2, and B3), micronodular with lymphoid stroma, and metaplastic thymoma depending on histologic features and immunohistochemistry.[1] The tumors originate from the epithelial cells of the thymus, a lymphoid gland composed of two lobes involved in the maturation of T lymphocytes, critical to the adaptive immune system.[3]
Thymomas are the most common type of TET with an annual incidence of 0.13 to 0.32 cases per 100,000 people[4] and typically occur in adults aged 40 to 70 years with increased incidence in African Americans and Pacific Islanders, hinting at a genetic predisposition.[5] Paraneoplastic syndromes (PNSs) may antedate the diagnosis of thymoma or be diagnosed concurrently, with myasthenia gravis (MG) being the commonest PNS. Up to 20% of MG patients have thymoma and 30 to 50% of thymoma patients have thymoma-associated MG.[6]
Although known to exhibit local invasion (pleural, pericardial),[7] [8] thymomas seldom spread to draining lymphatics, owing to lack of afferent lymphatics.[9] The mainstay of treatment is surgery (total thymectomy and excision of tumor) for operable patients, and completeness of resection is considered a key predictor of outcome.[10] Indications of adjuvant radiotherapy (RT) depend on a combination of factors such as Masaoka-Koga stage, resection status, and WHO subtype. According to the National Comprehensive Cancer Network (NCCN) guidelines,[11] adjuvant RT is indicated in microscopic residual tumor (R1) and macroscopic residual tumor (R2) resections, R0 with capsular invasion, and stages II to IV. The European Society of Medical Oncology guidelines[12] mention that adjuvant RT is recommended in R1 and R2 resections (any stage), R0 (if stage IIA with type B3 histology, stage IIB with type B2–B3 histology), anhd stages III to IVA (irrespective of resection status or WHO type). Definitive RT with concurrent chemotherapy is recommended in unresectable cases. Recommended doses of RT in adjuvant setting are 45 to 50 Gy (if R0), 50 to 54 Gy (if R1), and 60 to 70 Gy in definitive setting. The role of neoadjuvant chemotherapy is to downstage potentially resectable tumors,[13] [14] [15] with the preferred regimen being cisplatin/doxorubicin/cyclophosphamide (CAP).[16] [17] Patients with poor tolerance to anthracyclines may be offered cisplatin/etoposide with or without ifosfamide or paclitaxel/carboplatin combination.[18] [19]
Considering the relative rarity of this tumor and limited data on incidence and treatment outcomes in Indian patients, we aimed to analyze the clinical profiles, treatment outcomes, and patterns of relapse of patients treated at a tertiary care institute.
Materials and Methods
This is a retrospective study of prospectively maintained database of thymoma patients treated consecutively between January 2012 to June 2022. Patients with thymic carcinoma were excluded. Clinical records were captured in a predesigned proforma derived from the electronic health information system database. Clinical details (age, sex, symptoms, tumor size, Masaoka-Koga stage, WHO type, and PNSs), treatment details (surgery, RT, and chemotherapy), outcomes (alive and well, alive with disease, and dead due to disease/other cause), and last follow-up were entered into Microsoft Excel. All patients had baseline staging evaluation with either a contrast-enhanced computed tomography (CECT) of the thorax and abdomen or whole body fluorodeoxyglucose positron emission tomography CT scan. Baseline pulmonary function tests were carried out for all patients. Surgery consisted of total thymectomy, with resection of adjacent structures. Patients with pericardial involvement underwent pericardial resection followed by reconstruction, and those with pleural disease underwent pleural resection. Patients with lung metastasis or tumor adherent to lung underwent lobectomy of the involved lobe or wedge resection of lung. Surgical clips were placed at the time of surgery to aid in radiation target volume delineation. Intraoperatively, one patient was found to have pleura studded with multiple tiny pleural nodules and additionally underwent pleurectomy.
Patients were immobilized in supine position with Vac-Lok or thoracic cast and RT planning scans acquired at 3 mm slice thickness. RT was delivered either by tomotherapy or by volumetric modulated arc therapy (VMAT) using 6 MV photons. Response assessment with CECT of the thorax was at 3 months posttreatment according to Response Evaluation Criteria in Solid Tumors version 1.1 and thereafter at 6 monthly intervals till 5 years, followed by annual imaging. Metabolic response was also recorded, if available. Results were analyzed using the Statistical Package for the Social Sciences software (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0 Armonk, New York, United States: IBM Corp). Descriptive statistics such as mean and median were used to summarize the qualitative variables. Local control, overall survival (OS), and progression-free survival (PFS) were estimated using the Kaplan–Meier method.
Local control was defined as freedom from local progression. PFS was calculated as the time from the initiation of treatment to disease progression. OS was calculated from the date of diagnosis to the date of death from any cause or the date of last follow-up. Acute and late toxicities were scored according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE v5). The study was conducted according to the ethical guidelines outlined in the Declaration of Helsinki, Good Clinical Practice guidelines, and the Indian Council of Medical Research guidelines. The study was presented in the ethics committee and was granted approval (MICR: 1532/2023).
Results
Patient and treatment characteristics are shown in [Tables 1] and [2], respectively.
Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; WHO, World Health Organization.
Abbreviations: CAP, cyclophosphamide; NACT, neoadjuvant chemotherapy; VMAT, volumetric modulated arc therapy.
There were a total of 23 patients (12 males and 11 females) with median age of 52 years (range, 33–77 years). Majority (86.9%) had Eastern Cooperative Oncology Group performance status 1. Eleven patients (47.8%) had associated PNSs of which 10 (43.5%) had history of myasthenia gravis (MG) and 1 (4.3%) had pure red cell aplasia. Twelve patients had associated comorbidities. The commonest symptoms at presentation were cough (n = 6, 26%), dyspnea (n = 4, 17.4%), chest pain (n = 3, 13%), drooping of eyelids (n = 3, 13%), and generalized fatigue (n = 3, 13%). All patients were evaluated with baseline CECT of the thorax and had an average maximal tumor diameter of 62 mm (28–160 mm). Masaoka-Koga stage distribution was as follows: stage I (n = 2, 8.7%), IIA (n = 4, 17.4%), IIB (n = 1, 4.3%), IIIA (n = 2, 8.7%), IIIB (n = 4, 17.4%), IVA (n = 7, 30.4%), and IVB (n = 3, 13.1%). Three patients with metastatic disease had lung metastases. WHO type B2 was the commonest histology (n = 12, 52.17%), followed by B3 (n = 7, 30.4%), B1 (n = 2, 8.7%), AB (n = 1, 4.3%), and A (n = 1, 4.3%). Six patients received neoadjuvant chemotherapy (NACT) (six cycles of CAP regimen), 22 (95.6%) underwent surgery, and 1 patient received adjuvant chemotherapy. R0 resection was attained in 20 patients (91%), R1 resection in 1 patient (4.5%), and R2 in 1 patient (4.5%). All operated patients underwent postoperative RT (PORT) (45–60 Gy in 25–30 fractions, at 1.8–2 Gy per fraction). The indications for adjuvant RT included a combination of stage and WHO histology subtype. Early stages (I–II) with B2 histology and above, and stages III to IVA irrespective of histology received adjuvant RT. Both patients with stage I disease had type B2 histology. Five patients had stage II disease (two with B2 histology and three with B3 histology).
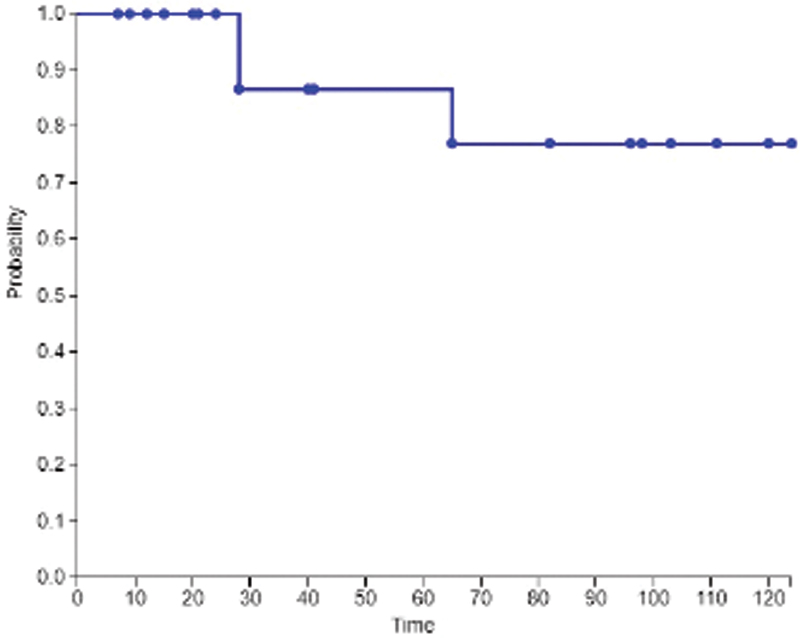
The lone nonoperated patient (due to multiple comorbidities) underwent definitive RT. RT was delivered by tomotherapy in 8 patients (34.7%) and VMAT in remaining 15 patients (65.3%). Four patients relapsed at a median duration of 14 months (2–26 months). Of the four patients who relapsed, three had pleural/lung metastases (out-of-field recurrence), one developed brain metastasis and one patient had liver metastasis. All patients who relapsed died within 6 months. A total of seven deaths occurred—four due to relapses, one due to myasthenia crisis, one due to grade 3 thrombocytopenia following adjuvant chemotherapy, and one due to unknown cause. At a median follow-up of 6 years, 5-year OS was 67.1% ([Fig. 1]) and 5-year PFS was 66.6% ([Fig. 2]). At the last follow-up, 13 patients (56.5%) are alive without disease, of which 4 had grade 2 pneumonitis (late toxicity). Local control at 5 years was 86.6% ([Fig. 3]).


Discussion
Thymomas have a varying clinical course and a better understanding of this heterogeneous disease is a requisite for achieving excellent clinical outcomes. Adults with a median age of 50 years are typically affected and the tumors are rarely seen in the pediatric/adolescent age. A higher risk of distant metastasis has been reported in a population-based study of more than 4,400 patients among the young adults.[20] The median age in the current study was 52 years, similar to previously reported outcomes of largest series of 62 patients from India by Rathod et al.[21] ([Table 3]) However, another report by Kumar et al reported median age of 40.8 years, a decade younger than our study.[22] There is no consistent gender predilection in thymomas; however, a slight female preponderance has been reported for types A, AB, and B1 and male predominance in carcinomas.[23] [24] In the present study, males and females were equally affected.
Given the critical role of thymus in immune function, it is unsurprising that TETs are associated with autoimmune conditions such as MG and pure red cell aplasia, as disruption in the balance of T-cells in both peripheral blood and tumor microenvironment are seen in these syndromes. In our study, almost half (48%) had associated PNS, with myasthenia being the commonest. This is consistent with available literature from India.[22]
The size of thymoma has prognostic implications, as demonstrated by a large national analysis of 1,849 patients that reported worse 5-year survival rate (84.6 vs. 89.4%) for tumor size 8 cm or larger, and deemed it as a risk factor for recurrence postresection.[25] The median size in our study was 62 mm, which was 14 to 18 mm smaller than other previous published data from India.[21] [22] Another report from the Surveillance, Epidemiology, and End Results (SEER) database of 1,272 thymoma patients reported larger rates of metastases and recurrence if tumors were more than 90 mm in size.[26]
The International Thymic Malignancy Group (ITMIG) worldwide database of 4,221 thymomas reported B2 as the commonest histology.[27] However, higher incidence of types AB and B3 and lower incidences of A and B2 were noted for Asians. Contrary to the worldwide database, a large retrospective study on histotyping of Indian thymomas revealed B2 as the commonest histology.[28] In the present study, B2 was the commonest subtype, followed by B3, consistent with findings from another Indian study.[22] Together, B2 and B3 subtypes constituted more than 80% of our patient population. In our study, Masaoka-Koga stages IIIB, IVA, and IVB constituted 60% of the patient population, with IIIB being the commonest stage, similar to previous reported studies from India[29] [30] but contrary to Rathod et al where stages I to II were the commonest.[21] The sites of metastases in our cohort included pleura and lung in two patients and lung in one patient. Pleural/lung and lymph nodes have previously been reported to be the commonest sites of metastases, and less commonly to liver and brain.[31]
The treatment of thymoma is complex and not without controversy, mainly due to the heterogeneous nature of this disease. In our series of 23 patients, all except one underwent surgery, with R0 resection achieved in 90% of the patients. The lone case deemed medically inoperable underwent definitive radiation to a dose of 60 Gy. All of the 22 operated cases underwent adjuvant radiation to a dose of 45 to 60 Gy. The role of PORT in thymoma is mired with conflicting reports. In one of the largest retrospective series to address the role of PORT for both thymoma and thymic carcinomas done by the Japanese Association for Research on the Thymus, of 1,265 patients with stages II and III, no benefit in RFS and OS was seen in patients with thymoma.[32] Contrary to this study, a survival benefit with PORT for thymoma has been seen in multiple retrospective analyses. In a study of 1,263 patients with stages II and III registered in database by the ITMIG (55% of whom received PORT), PORT was associated with improved 5-year OS specially in stage IIB or III or with margin positive status.[33]
In another study of 529 patients with thymoma in the SEER database, when compared with who did not receive PORT, the 345 patients (65%) who received PORT had superior OS rate (76 vs. 66%) and DFS (91 vs. 81%) at 7 years. Subgroup analysis suggested the OS benefit was limited to patients with stage III or IV disease.[34] The first and only available guidelines for optimal clinical target volume (CTV) delineation highlighted the importance of a multidisciplinary approach and the variability between the volumes marked by radiation oncologists (larger volumes) as compared with thoracic surgeons. A collaborative delineation led to significantly smaller volumes thereby emphasizing the need for the surgeons' inputs while defining the CTV.[35] In the present study, RT target volumes were delineated after fusing the baseline imaging and reconstructing the pre-resection gross tumor volume. Postoperative CTV included entire surgical bed mapped with the aid of surgical clips as well as areas of prior tumor contact with pleura/pericardium/mediastinum and areas of doubtful disease. CTV was delineated after consensus with the operating thoracic surgeon. Planning treatment volume was generated by expanding the CTV by 5 mm. The evolution of radiation techniques allows the delivery of advanced techniques that can reduce dose to critical thoracic organs at risk. Among photon-based RT techniques, dosimetric parameters for VMAT are superior to those obtained by three-dimensional conformal RT, while tomotherapy achieves best target volume coverage.[36] Majority of our patients were treated by VMAT (65.3%), while remaining were by tomotherapy.
In our study, four patients relapsed at a median duration of 14 months. Three developed pleural/lung metastases (out-of-field recurrence), one developed brain metastasis and one relapsed in liver and abdominal lymph nodes. Majority of relapses among thymoma patients reported in the literature occur intrathoracic, most being pleural based, up to 77%.[37] [38] Locoregional recurrences have been reported in up to 79% in another study.[39] All four relapses occurred in patients with higher stage (IVA in two and IVB in two) and more aggressive WHO subtype (B2 in two and B3 in two). The lone inoperable case in our cohort underwent NACT followed by radical RT, and eventually developed brain metastases. All patients who relapsed died within 6 months. A total of seven deaths occurred—four due to relapses, one due to myasthenia crisis, one due to grade 3 thrombocytopenia following adjuvant chemotherapy, and one due to unknown cause. At a median follow-up of 6 years, our 5-year OS was 67.1% and 5-year DFS was 66.6%. The 5-year OS in our study is considerably lower to that reported by Alothaimeen and Memon (88.6%),[40] Bruni et al (90.2%),[41] Yuan et al (91%),[39] and Chowdhary et al (75.7%),[42] but comparable to Zhu et al (56.5%).[43] Two series from India have reported 3-year OS rates of 83 and 90%.[21] [22] The lower OS rates in our study may be attributed to the advanced stage of our study population. However, our local control at 5 years was 86.6% which is higher compared with other series (68–77.8%).[40] [42] [43] [44] Local control can be considered a surrogate for effectiveness of local treatment. The high local control rates in the present study may be attributed to R0 resection status in more than 90% of our patients and adjuvant RT in all patients, irrespective of stage and histology. Considering most patients with thymoma receive thoracic/mediastinal radiation ([Figs. 4] and [5]), increased lung dose is inevitable. We observed grade 2 pneumonitis in four patients at long-term follow-up, all of whom had been treated by VMAT technique. None of these patients required admission for management of pneumonitis. [Fig. 6] shows postradiation fibrosis in a patient who received thoracic/mediastinal RT for stage IVA disease.



|
Author (year of publication) |
No. of patients |
Associated PNS (no. of patients) |
Mean age (y) |
Commonest Masaoka-Koga stage |
Commonest WHO subtype |
Primary surgery (%) |
Adjuvant RT |
Mortality |
Outcomes |
|---|---|---|---|---|---|---|---|---|---|
|
Myojin et al (2000)[38] |
32 |
– |
57 |
III (29%) |
C (60%) |
78% |
92% |
– |
5 y OS 71% |
|
Zhu et al (2004)[43] |
175 |
MG (40) |
50 |
I (27%) |
– |
100% |
169 (96.5%) |
– |
5 y OS (86.4%) |
|
Kumar et al (2013)[22] |
36 |
MG (17) Cushing (3) |
57 |
IVA (36.1%) |
B2 (33.3%) |
27 (75%) |
20 (74%) |
– |
3 y PFS (60%) 3 y OS (83%) |
|
Lim et al (2015), SEER[34] |
529 |
– |
57 |
– |
B3 (27%) |
100% |
65% |
– |
PORT favorable for stages III and IV |
|
Rimner et al (2016), ITMIG[33] |
1,263 |
MG (478) |
54 |
II (69%) |
B1/B2/B3 (70%) |
100% |
55% |
– |
10 y OS (86%) |
|
Rathod et al (2014)[21] |
62 |
MG (9) |
51.5 |
I–II (57%) |
B (49%) |
44 (71%) |
76% |
– |
3 y OS (90%) |
|
Yuan et al (2017)[39] |
307 |
MG (58) |
50.5 |
II (55.4%) |
AB (32.2%) |
100% |
46.3% |
12.4% |
10 y OS 74% |
|
Alothaimeen and Memon (2020)[40] |
56 |
MG (20) |
39 |
– |
– |
75% |
75% |
– |
5 y OS (90.1%) |
|
Bruni et al (2020)[41] |
183 |
MG (63) |
58.5 |
I (39.3%) |
B3 (24%) |
100% |
61.7% |
– |
10 y OS (69.7%) |
|
Chowdhary et al (2023)[42] |
88 |
MG (16) Pure red cell aplasia (5) |
52.17 |
II (44.3%) |
B2 (43.2%) |
64 (72.7%) |
34 (53.1%) |
22 (25%) |
5 y OS (75.7%) |
Abbreviations: ITMIG, International Thymic Malignancy Group; MG, myasthenia gravis; OS, overall survival; PFS, progression-free survival; PNS, paraneoplastic syndrome; PORT, postoperative RT; RT, radiotherapy; SEER, Surveillance, Epidemiology, and End Results; WHO, World Health Organization.
Our study was limited by its inherent retrospective nature and relatively small sample size.
Future Directions
Advances in RT planning and delivery may potentially permit the administration of higher doses safely, with lesser potential for toxicities. Using proton beam therapy (PBT), some of the known toxicities associated with radiation may be minimized. NCCN states that it can be considered for selected patients given that it has superior dosimetry compared with intensity modulated RT (IMRT) and favorable results with regard to local control. Dosimetric differences between PBT and IMRT was reported by Parikh et al where mean doses to lung, esophagus, and heart were considerably reduced with PBT.[45] Reduced mean doses to heart and lung using PBT have been reported in recent literature.[46] [47]
The entry of immunotherapy has stormed the medical world and its potential benefit in thymomas may be a reality as recent reports have shown programmed cell death ligand 1 (PD-L1) expression ranging from 23 to 70% depending on the subtype of TET.[48] The frequent PD-L1 association (particularly in B3 subtype) and its potential benefit with immunotherapy (nivolumab) is being investigated in a phase II European Organisation for Research and Treatment (EORTC) study, likely paving the way for immunotherapy in TET. However, concerns regarding treatment of TET patients with an active autoimmune disorder with immunotherapy remain unanswered.[49]
Conclusion
Majority of our patients present with advanced stage and B2/B3 histology. Despite the advanced stage, the local control rates are encouraging and reinforce multimodality approach in a disease that is technically challenging to treat.
Corrigendum: The author byline for this article has been corrected as per corrigendum published on September 26, 2024. (DOI: 10.1055/s-0044-1791272).
Conflict of Interest
None declared.
Acknowledgments
We thank the technical and nursing staff of Division of Radiation Oncology, Medanta The Medicity for assistance in treatment delivery.
Previous Presentation
This study was presented as a proffered paper presentation at the 37th AROICON 2022 held in New Delhi, India, December 3, 2022.
-
References
- 1 Marx A, Chan JKC, Chalabreysse L. et al. The 2021 WHO classification of tumors of the thymus and mediastinum: what is new in thymic epithelial, germ cell, and mesenchymal tumors?. J Thorac Oncol 2022; 17 (02) 200-213
- 2 Rico M, Flamarique S, Casares C. et al. GOECP/SEOR radiotherapy guidelines for thymic epithelial tumours. World J Clin Oncol 2021; 12 (04) 195-216
- 3 Thapa P, Farber DL. The role of the thymus in immune response. Thorac Surg Clin 2019; 29 (02) 123-131
- 4 Rich AL. Epidemiology of thymoma. J Thorac Dis 2020; 12 (12) 7531-7535
- 5 Engels EA. Epidemiology of thymoma and associated malignancies. J Thorac Oncol 2010; 5 (10, suppl 4): S260-S265
- 6 Marx A, Strobel P, Weis C-A. The pathology of the thymus in myasthenia gravis. Mediastinum 2018; •••: 2-66
- 7 Bläker H, Dragoje S, Laissue J-A, Otto HF. Pericardial involvement by thymomas. Entirely intrapericardial thymoma and a pericardial metastasis of thymoma with glomeruloid vascular proliferations. Pathol Oncol Res 1999; 5 (02) 160-163
- 8 Picchi E, Di Giuliano F, Ferrari D, Pistolese CA, Garaci F, Floris R. Pleural thymoma: radiological and histological findings. Eur J Radiol Open 2018; 5: 147-152
- 9 Engels EA, Pfeiffer RM. Malignant thymoma in the United States: demographic patterns in incidence and associations with subsequent malignancies. Int J Cancer 2003; 105 (04) 546-551
- 10 Zhao Y, Shi J, Fan L, Hu D, Yang J, Zhao H. Surgical treatment of thymoma: an 11-year experience with 761 patients. Eur J Cardiothorac Surg 2016; 49 (04) 1144-1149
- 11 Ettinger DS, Wood DE, Riely GJ, Aisner DL, Akerley W, Bauman JR. et al; National Comprehensive Cancer Network. Thymomas and thymic carcinomas: clinical practice guidelines in oncology. J Natl Compr Canc Netw 2022
- 12 Girard N, Ruffini E, Marx A, Faivre-Finn C, Peters S. ESMO Guidelines Committee. Thymic epithelial tumours: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2015; 26 (Suppl. 05) v40-v55
- 13 Ruffini E, Guerrera F, Brunelli A. et al. Report from the European Society of Thoracic Surgeons prospective thymic database 2017: a powerful resource for a collaborative global effort to manage thymic tumours. Eur J Cardiothorac Surg 2019; 55 (04) 601-609
- 14 Kanzaki R, Kanou T, Ose N. et al. Long-term outcomes of advanced thymoma in patients undergoing preoperative chemotherapy or chemoradiotherapy followed by surgery: a 20-year experience. Interact Cardiovasc Thorac Surg 2019; 28 (03) 360-367
- 15 Riely GJ, Huang J. Induction therapy for locally advanced thymoma. J Thorac Oncol 2010; 5 (10, suppl 4): S323-S326
- 16 Kondo K. Optimal therapy for thymoma. J Med Invest 2008; 55 (1-2): 17-28
- 17 Okuma Y, Saito M, Hosomi Y, Sakuyama T, Okamura T. Key components of chemotherapy for thymic malignancies: a systematic review and pooled analysis for anthracycline-, carboplatin- or cisplatin-based chemotherapy. J Cancer Res Clin Oncol 2015; 141 (02) 323-331
- 18 Loehrer Sr PJ, Jiroutek M, Aisner S. et al. Combined etoposide, ifosfamide, and cisplatin in the treatment of patients with advanced thymoma and thymic carcinoma: an intergroup trial. Cancer 2001; 91 (11) 2010-2015
- 19 Lemma GL, Lee JW, Aisner SC. et al. Phase II study of carboplatin and paclitaxel in advanced thymoma and thymic carcinoma. J Clin Oncol 2011; 29 (15) 2060-2065
- 20 Liu M, Wang C, Gao L, Lv C, Fu X. Clinical significance of age at diagnosis among patients with thymic epithelial tumors: a population-based study. Aging (Albany NY) 2020; 12 (06) 4815-4821
- 21 Rathod S, Munshi A, Paul S, Ganesh B, Prabhash K, Agarwal JP. Thymoma: first large Indian experience. Indian J Cancer 2014; 51 (02) 109-112
- 22 Kumar N, Kumar R, Bera A. et al. Thymoma: clinical experience from a tertiary care institute from North India. J Cancer Res Ther 2013; 9 (02) 235-239
- 23 Hsu C-H, Chan JK, Yin CH, Lee CC, Chern CU, Liao CI. Trends in the incidence of thymoma, thymic carcinoma, and thymic neuroendocrine tumor in the United States. PLoS One 2019; 14 (12) e0227197
- 24 Marx A, Ströbel P, Badve SS. et al. ITMIG consensus statement on the use of the WHO histological classification of thymoma and thymic carcinoma: refined definitions, histological criteria, and reporting. J Thorac Oncol 2014; 9 (05) 596-611
- 25 Liou DZ, Ramakrishnan D, Lui NS, Shrager JB, Backhus LM, Berry MF. Does size matter? A national analysis of the utility of induction therapy for large thymomas. J Thorac Dis 2020; 12 (04) 1329-1341
- 26 Bian D, Zhou F, Yang W. et al. Thymoma size significantly affects the survival, metastasis and effectiveness of adjuvant therapies: a population based study. Oncotarget 2018; 9 (15) 12273-12283
- 27 Weis C-A, Yao X, Deng Y. et al; Contributors to the ITMIG Retrospective Database. The impact of thymoma histotype on prognosis in a worldwide database. J Thorac Oncol 2015; 10 (02) 367-372
- 28 Guleria P, Parshad R, Malik PS, Ray R, Pandey RM, Jain D. Histotyping of Indian thymomas: a clinicopathologic study from north India. Indian J Med Res 2019; 150 (02) 153-160
- 29 Arjunan R, Kurpad V, Vimalathithan V, Prakash P, Althaf S, Kumar V. Thymoma: a retrospective review of 55 cases of thymoma treated at a regional cancer center. J Cancer Prev Curr Res 2015; 2 (01) 8-10
- 30 Tirumala V, Suresh Babu MC, Govind Babu K. et al. Treatment experience of thymoma and thymic carcinoma in tertiary cancer institute in India. Ann Oncol 2018; 29 (Suppl. 09) IX149
- 31 Cheng G, Gu C, Song Z. Impact of metastasis site for survival of patients with advanced thymic epithelial tumors. Transl Cancer Res 2016; 5 (05) 546-551
- 32 Omasa M, Date H, Sozu T. et al; Japanese Association for Research on the Thymus. Postoperative radiotherapy is effective for thymic carcinoma but not for thymoma in stage II and III thymic epithelial tumors: the Japanese Association for Research on the Thymus Database Study. Cancer 2015; 121 (07) 1008-1016
- 33 Rimner A, Yao X, Huang J. et al. Postoperative radiation therapy is associated with longer overall survival in completely resected stage II and III thymoma- an analysis of the International Thymic Malignancies Interest Group Retrospective Database. J Thorac Oncol 2016; 11 (10) 1785-1792
- 34 Lim YJ, Kim HJ, Wu H-G. Role of postoperative radiotherapy in nonlocalized thymoma: propensity-matched analysis of Surveillance, Epidemiology, and End Results database. J Thorac Oncol 2015; 10 (09) 1357-1363
- 35 Marcuse F, Peeters S, Herman K. et al. Optimal delineation of the clinical target volume for thymomas in the post-resection setting: a multi-center study. Radiother Oncol 2021; 165: 8-13
- 36 Haefner MF, Verma V, Bougatf N. et al. Dosimetric comparison of advanced radiotherapy approaches using photon techniques and particle therapy in the postoperative management of thymoma. Acta Oncol 2018; 57 (12) 1713-1720
- 37 Gomez D, Komaki R, Yu J, Ikushima H, Bezjak A. Radiation therapy definitions and reporting guidelines for thymic malignancies. J Thorac Oncol 2011; 6 (7, suppl 3): S1743-S1748
- 38 Myojin M, Choi NC, Wright CD. et al. Stage III thymoma: pattern of failure after surgery and postoperative radiotherapy and its implication for future study. Int J Radiat Oncol Biol Phys 2000; 46 (04) 927-933
- 39 Yuan Z-Y, Gao S-G, Mu J-W. et al. Long-term outcomes of 307 patients after complete thymoma resection. Chin J Cancer 2017; 36 (01) 46
- 40 Alothaimeen HS, Memon MA. Treatment outcomes and prognostic factors of malignant thymoma – a single institution experience. Asian Pac J Cancer Prev 2020; 21 (03) 653-661
- 41 Bruni A, Stefani A, Perna M. et al. The role of postoperative radiotherapy for thymomas: a multicentric retrospective evaluation from three Italian centers and review of the literature. J Thorac Dis 2020; 12 (12) 7518-7530
- 42 Chowdhary RL, Chufal KS, Ismail M. et al. Intuitive evaluation of contemporary management strategies in thymoma - the largest Indian experience. Rep Pract Oncol Radiother 2023; 28 (04) 454-462
- 43 Zhu G, He S, Fu X, Jiang G, Liu T. Radiotherapy and prognostic factors for thymoma: a retrospective study of 175 patients. Int J Radiat Oncol Biol Phys 2004; 60 (04) 1113-1119
- 44 Tomaszek S, Wigle DA, Keshavjee S, Fischer S. Thymomas: review of current clinical practice. Ann Thorac Surg 2009; 87 (06) 1973-1980
- 45 Parikh RR, Rhome R, Hug E. et al. Adjuvant proton beam therapy in the management of thymoma: a dosimetric comparison and acute toxicities. Clin Lung Cancer 2016; 17 (05) 362-366
- 46 McGunigal M, Margolis M, Forsthoefel M. et al. Thymic malignancies treated with active scanning proton beam radiation and Monte Carlo planning: early clinical experience. Acta Oncol 2021; 60 (05) 649-652
- 47 Zhu HJ, Hoppe BS, Flampouri S. et al. Rationale and early outcomes for the management of thymoma with proton therapy. Transl Lung Cancer Res 2018; 7 (02) 106-113
- 48 Katsuya Y, Fujita Y, Horinouchi H, Ohe Y, Watanabe S, Tsuta K. Immunohistochemical status of PD-L1 in thymoma and thymic carcinoma. Lung Cancer 2015; 88 (02) 154-159
- 49 Jakopovic M, Bitar L, Seiwerth F, Marusic A, Krpina K, Samarzija M. Immunotherapy for thymoma. J Thorac Dis 2020; 12 (12) 7635-7641
Address for correspondence
Publication History
Received: 27 September 2023
Accepted: 11 June 2024
Article published online:
08 July 2024
© 2024. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Marx A, Chan JKC, Chalabreysse L. et al. The 2021 WHO classification of tumors of the thymus and mediastinum: what is new in thymic epithelial, germ cell, and mesenchymal tumors?. J Thorac Oncol 2022; 17 (02) 200-213
- 2 Rico M, Flamarique S, Casares C. et al. GOECP/SEOR radiotherapy guidelines for thymic epithelial tumours. World J Clin Oncol 2021; 12 (04) 195-216
- 3 Thapa P, Farber DL. The role of the thymus in immune response. Thorac Surg Clin 2019; 29 (02) 123-131
- 4 Rich AL. Epidemiology of thymoma. J Thorac Dis 2020; 12 (12) 7531-7535
- 5 Engels EA. Epidemiology of thymoma and associated malignancies. J Thorac Oncol 2010; 5 (10, suppl 4): S260-S265
- 6 Marx A, Strobel P, Weis C-A. The pathology of the thymus in myasthenia gravis. Mediastinum 2018; •••: 2-66
- 7 Bläker H, Dragoje S, Laissue J-A, Otto HF. Pericardial involvement by thymomas. Entirely intrapericardial thymoma and a pericardial metastasis of thymoma with glomeruloid vascular proliferations. Pathol Oncol Res 1999; 5 (02) 160-163
- 8 Picchi E, Di Giuliano F, Ferrari D, Pistolese CA, Garaci F, Floris R. Pleural thymoma: radiological and histological findings. Eur J Radiol Open 2018; 5: 147-152
- 9 Engels EA, Pfeiffer RM. Malignant thymoma in the United States: demographic patterns in incidence and associations with subsequent malignancies. Int J Cancer 2003; 105 (04) 546-551
- 10 Zhao Y, Shi J, Fan L, Hu D, Yang J, Zhao H. Surgical treatment of thymoma: an 11-year experience with 761 patients. Eur J Cardiothorac Surg 2016; 49 (04) 1144-1149
- 11 Ettinger DS, Wood DE, Riely GJ, Aisner DL, Akerley W, Bauman JR. et al; National Comprehensive Cancer Network. Thymomas and thymic carcinomas: clinical practice guidelines in oncology. J Natl Compr Canc Netw 2022
- 12 Girard N, Ruffini E, Marx A, Faivre-Finn C, Peters S. ESMO Guidelines Committee. Thymic epithelial tumours: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2015; 26 (Suppl. 05) v40-v55
- 13 Ruffini E, Guerrera F, Brunelli A. et al. Report from the European Society of Thoracic Surgeons prospective thymic database 2017: a powerful resource for a collaborative global effort to manage thymic tumours. Eur J Cardiothorac Surg 2019; 55 (04) 601-609
- 14 Kanzaki R, Kanou T, Ose N. et al. Long-term outcomes of advanced thymoma in patients undergoing preoperative chemotherapy or chemoradiotherapy followed by surgery: a 20-year experience. Interact Cardiovasc Thorac Surg 2019; 28 (03) 360-367
- 15 Riely GJ, Huang J. Induction therapy for locally advanced thymoma. J Thorac Oncol 2010; 5 (10, suppl 4): S323-S326
- 16 Kondo K. Optimal therapy for thymoma. J Med Invest 2008; 55 (1-2): 17-28
- 17 Okuma Y, Saito M, Hosomi Y, Sakuyama T, Okamura T. Key components of chemotherapy for thymic malignancies: a systematic review and pooled analysis for anthracycline-, carboplatin- or cisplatin-based chemotherapy. J Cancer Res Clin Oncol 2015; 141 (02) 323-331
- 18 Loehrer Sr PJ, Jiroutek M, Aisner S. et al. Combined etoposide, ifosfamide, and cisplatin in the treatment of patients with advanced thymoma and thymic carcinoma: an intergroup trial. Cancer 2001; 91 (11) 2010-2015
- 19 Lemma GL, Lee JW, Aisner SC. et al. Phase II study of carboplatin and paclitaxel in advanced thymoma and thymic carcinoma. J Clin Oncol 2011; 29 (15) 2060-2065
- 20 Liu M, Wang C, Gao L, Lv C, Fu X. Clinical significance of age at diagnosis among patients with thymic epithelial tumors: a population-based study. Aging (Albany NY) 2020; 12 (06) 4815-4821
- 21 Rathod S, Munshi A, Paul S, Ganesh B, Prabhash K, Agarwal JP. Thymoma: first large Indian experience. Indian J Cancer 2014; 51 (02) 109-112
- 22 Kumar N, Kumar R, Bera A. et al. Thymoma: clinical experience from a tertiary care institute from North India. J Cancer Res Ther 2013; 9 (02) 235-239
- 23 Hsu C-H, Chan JK, Yin CH, Lee CC, Chern CU, Liao CI. Trends in the incidence of thymoma, thymic carcinoma, and thymic neuroendocrine tumor in the United States. PLoS One 2019; 14 (12) e0227197
- 24 Marx A, Ströbel P, Badve SS. et al. ITMIG consensus statement on the use of the WHO histological classification of thymoma and thymic carcinoma: refined definitions, histological criteria, and reporting. J Thorac Oncol 2014; 9 (05) 596-611
- 25 Liou DZ, Ramakrishnan D, Lui NS, Shrager JB, Backhus LM, Berry MF. Does size matter? A national analysis of the utility of induction therapy for large thymomas. J Thorac Dis 2020; 12 (04) 1329-1341
- 26 Bian D, Zhou F, Yang W. et al. Thymoma size significantly affects the survival, metastasis and effectiveness of adjuvant therapies: a population based study. Oncotarget 2018; 9 (15) 12273-12283
- 27 Weis C-A, Yao X, Deng Y. et al; Contributors to the ITMIG Retrospective Database. The impact of thymoma histotype on prognosis in a worldwide database. J Thorac Oncol 2015; 10 (02) 367-372
- 28 Guleria P, Parshad R, Malik PS, Ray R, Pandey RM, Jain D. Histotyping of Indian thymomas: a clinicopathologic study from north India. Indian J Med Res 2019; 150 (02) 153-160
- 29 Arjunan R, Kurpad V, Vimalathithan V, Prakash P, Althaf S, Kumar V. Thymoma: a retrospective review of 55 cases of thymoma treated at a regional cancer center. J Cancer Prev Curr Res 2015; 2 (01) 8-10
- 30 Tirumala V, Suresh Babu MC, Govind Babu K. et al. Treatment experience of thymoma and thymic carcinoma in tertiary cancer institute in India. Ann Oncol 2018; 29 (Suppl. 09) IX149
- 31 Cheng G, Gu C, Song Z. Impact of metastasis site for survival of patients with advanced thymic epithelial tumors. Transl Cancer Res 2016; 5 (05) 546-551
- 32 Omasa M, Date H, Sozu T. et al; Japanese Association for Research on the Thymus. Postoperative radiotherapy is effective for thymic carcinoma but not for thymoma in stage II and III thymic epithelial tumors: the Japanese Association for Research on the Thymus Database Study. Cancer 2015; 121 (07) 1008-1016
- 33 Rimner A, Yao X, Huang J. et al. Postoperative radiation therapy is associated with longer overall survival in completely resected stage II and III thymoma- an analysis of the International Thymic Malignancies Interest Group Retrospective Database. J Thorac Oncol 2016; 11 (10) 1785-1792
- 34 Lim YJ, Kim HJ, Wu H-G. Role of postoperative radiotherapy in nonlocalized thymoma: propensity-matched analysis of Surveillance, Epidemiology, and End Results database. J Thorac Oncol 2015; 10 (09) 1357-1363
- 35 Marcuse F, Peeters S, Herman K. et al. Optimal delineation of the clinical target volume for thymomas in the post-resection setting: a multi-center study. Radiother Oncol 2021; 165: 8-13
- 36 Haefner MF, Verma V, Bougatf N. et al. Dosimetric comparison of advanced radiotherapy approaches using photon techniques and particle therapy in the postoperative management of thymoma. Acta Oncol 2018; 57 (12) 1713-1720
- 37 Gomez D, Komaki R, Yu J, Ikushima H, Bezjak A. Radiation therapy definitions and reporting guidelines for thymic malignancies. J Thorac Oncol 2011; 6 (7, suppl 3): S1743-S1748
- 38 Myojin M, Choi NC, Wright CD. et al. Stage III thymoma: pattern of failure after surgery and postoperative radiotherapy and its implication for future study. Int J Radiat Oncol Biol Phys 2000; 46 (04) 927-933
- 39 Yuan Z-Y, Gao S-G, Mu J-W. et al. Long-term outcomes of 307 patients after complete thymoma resection. Chin J Cancer 2017; 36 (01) 46
- 40 Alothaimeen HS, Memon MA. Treatment outcomes and prognostic factors of malignant thymoma – a single institution experience. Asian Pac J Cancer Prev 2020; 21 (03) 653-661
- 41 Bruni A, Stefani A, Perna M. et al. The role of postoperative radiotherapy for thymomas: a multicentric retrospective evaluation from three Italian centers and review of the literature. J Thorac Dis 2020; 12 (12) 7518-7530
- 42 Chowdhary RL, Chufal KS, Ismail M. et al. Intuitive evaluation of contemporary management strategies in thymoma - the largest Indian experience. Rep Pract Oncol Radiother 2023; 28 (04) 454-462
- 43 Zhu G, He S, Fu X, Jiang G, Liu T. Radiotherapy and prognostic factors for thymoma: a retrospective study of 175 patients. Int J Radiat Oncol Biol Phys 2004; 60 (04) 1113-1119
- 44 Tomaszek S, Wigle DA, Keshavjee S, Fischer S. Thymomas: review of current clinical practice. Ann Thorac Surg 2009; 87 (06) 1973-1980
- 45 Parikh RR, Rhome R, Hug E. et al. Adjuvant proton beam therapy in the management of thymoma: a dosimetric comparison and acute toxicities. Clin Lung Cancer 2016; 17 (05) 362-366
- 46 McGunigal M, Margolis M, Forsthoefel M. et al. Thymic malignancies treated with active scanning proton beam radiation and Monte Carlo planning: early clinical experience. Acta Oncol 2021; 60 (05) 649-652
- 47 Zhu HJ, Hoppe BS, Flampouri S. et al. Rationale and early outcomes for the management of thymoma with proton therapy. Transl Lung Cancer Res 2018; 7 (02) 106-113
- 48 Katsuya Y, Fujita Y, Horinouchi H, Ohe Y, Watanabe S, Tsuta K. Immunohistochemical status of PD-L1 in thymoma and thymic carcinoma. Lung Cancer 2015; 88 (02) 154-159
- 49 Jakopovic M, Bitar L, Seiwerth F, Marusic A, Krpina K, Samarzija M. Immunotherapy for thymoma. J Thorac Dis 2020; 12 (12) 7635-7641

