Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is expansively used to manage
several disorders of the biliopancreatic system. However, currently there are no data
regarding the number of procedures performed or the current rate of complication associated
with them in our country. It is estimated that over 411,409 ERCPs were performed from
2002 to 2013 in the United States.[1] The growing list of ERCP indications includes obstructive jaundice, pancreatic or
biliary ductal system pathology, its treatment or tissue sampling, any pancreatitis
of unknown cause, biliary stenting for strictures and leakage, endoscopic drainage
of pancreatic pseudocysts, and balloon dilation of the duodenal papilla and ductal
strictures.[2]
A systematic survey of 21 prospective clinical studies between 1977 and 2006 involving
16,885 subjects reported an overall post-ERCP complication rate of 6.85% with a 0.33%
mortality.[3] Acute pancreatitis is the most common complication encountered post-procedure with
an incidence rate of 3 to 10%.[4] Other complications include hemorrhage (0.3–2.0%), duodenal perforation (DP; 0.08–0.6%),
and cholangitis (0.5–3%).
Uncommon complications such as air embolism, pneumothorax, splenic injury, and bowel
perforation have also been recognized.[5]
[6]
[7]
[8] Mortality is unusual (0.3–1%) and is mostly associated with surgical procedures.
The utilization trends of ERCP show that the number of procedures performed for therapeutic
indications will see a rise.[9] There is an urgent need to recognize and appropriately manage potential complications
to reduce morbidity and mortality associated with this procedure. Imaging is indispensable
in the early diagnosis of these complications, and it is vital that the radiologist
is familiar with the imaging findings and further management implications of these
conditions.
While occasional case reports and short case series exist on this subject, there is
paucity of literature specifically reviewing the imaging findings of these complications
from our country. We thus conducted a retrospective study of the post-ERCP complications
to bring out the imaging spectrum of these complications.
Materials and Methods
The descriptive study was carried out at the department of radiology at a tertiary
care referral center. A retrospective analysis of 5 years (2018–2022) of cases of
post-ERCP complications diagnosed at our hospital was performed. A search engine of
medical terms was used, and a database of all positive cases in the department of
the hospital was made. The radiological reports containing both the words “post-ERCP”
and a term from a collated list of complications compiled after review of literature
such as “pancreatitis” were searched to identify potential cases. After a careful
review by two radiologists, 41 patients were identified as post-ERCP cases with complications
(exclusively procedure related) according to their clinical and radiological records.
Patients with prior complications like bowel obstruction, prior history of pancreatitis,
bleeding diathesis, prothrombotic tendencies, or those caused by trauma were excluded
from this series because the positive findings were not exclusive to the procedure.
All the patients who underwent an ERCP prior to imaging were included in this study.
All the cases were imaged on a 256-slice multidetector scanner (Philips brilliance
ICT Philips Medical Systems, Eindhoven, Netherlands) using a standardized institutional
protocol comprising basal noncontrast images and after an intravenous bolus injection
of a nonionic iodinated contrast agent (300 mg of iodine/mL with a dose of 1 mL/kg
bodyweight at a rate of 3–4 mL/s) using different phases depending on the cases. A
portal phase with a fixed delay of 70 seconds was obtained in all the patients. Arterial
bolus-tracking techniques were performed or added according to clinical suspicion.
Nonenhanced computed tomography (CT) was used in identifying hyperattenuating fresh
blood or hematoma. Late arterial phase between 25 and 35 seconds was used to demonstrate
any vascular injuries defined as active contrast extravasation. In 33 patients, positive
oral nonionic water-soluble contrast agent (300 mg of iodine/mL) was given as follows:
30 mL in 1,000 mL of water. In eight patients, no oral contrast could be given due
to poor clinical condition of the patient. All the CT scan images were retrospectively
evaluated by two radiologists, one with 5 years and another with 15 years of experience
in consensus.
Results
The mean age of the patients was 50.8 years (range: 04–79 years); 26 patients (63.4%)
were females and 15 patients (36.5%) were males. The clinical features and results
of CT findings are summarized in [Table 1].
Table 1
Clinical and radiological findings of patients included in the study
|
Case no.
|
Age/sex
|
Presentation
|
CT finding
|
|
1
|
46/F
|
Abdominal pain
|
Pancreatitis modified CTSI 6/10, ileus, thrombus in the RHV, collection in head of
the pancreas
|
|
2
|
38/M
|
Abdominal pain
|
Pancreatitis: modified CTSI 4/10
|
|
3
|
22/F
|
Abdominal pain, breathlessness, tachycardia
|
Pancreatitis: modified CTSI 8/10, pulmonary thromboembolism, sealed GB perforation
|
|
4
|
30/F
|
Abdominal pain, fever, tachycardia
|
D2 perforation, MPD injury, multiple intrabdominal collections
|
|
5
|
62/F
|
Jaundice
|
Displaced ERCP stent
|
|
6
|
69/F
|
Abdominal pain, abdominal distention
|
D2 perforation, small bowel obstruction
|
|
7
|
41/F
|
Jaundice, abdominal pain
|
GB perforation
|
|
8
|
51/M
|
Abdominal pain, fever
|
Pancreatitis: CTSI 8/10, liver abscess
|
|
9
|
67/F
|
Abdominal pain
|
Liver abscess, intrabdominal collection
|
|
10
|
79/M
|
Jaundice, fever, abdominal pain
|
Cholangitis, thrombus in RPV
|
|
11
|
66/M
|
Abdominal pain, fever, ARDS
|
Pancreatitis: CTSI 8/10, air foci in collection
|
|
12
|
48/F
|
Jaundice
|
Duodenitis
|
|
13
|
58/F
|
Abdominal pain
|
Sealed GB perforation
|
|
14
|
66/M
|
Abdominal pain
|
Pancreatitis: CTSI 6/10
|
|
15
|
51/M
|
Fever, tachycardia, Abdominal pain, distention
|
Pancreatitis: CTSI 10/10, liver abscess, intra-abdominal collection
|
|
16
|
66/M
|
Abdominal pain, abdominal distention
|
Acute pancreatitis: CTSI 6/10
|
|
17
|
60/F
|
Abdominal pain, breathlessness, fever
|
Consolidation and pleural effusion bilateral, ileus
|
|
18
|
66/M
|
Abdominal pain, abdominal distention
|
Acute pancreatitis: CTSI 4/10
|
|
19
|
47/F
|
Abdominal pain, abdominal distention, fever
|
Multiple cholangitic abscesses, subcapsular collection, thrombus in MPV, RPV, and
LPV
|
|
20
|
53/F
|
Jaundice
|
Acute cholangitis
|
|
21
|
54/F
|
Abdominal pain, tachycardia
|
Hepatic abscesses with possible pleural communication
|
|
22
|
75/M
|
Hypotension, bleeding
|
Displaced CBD stent, acute pancreatitis: CTSI 4/10
|
|
23
|
60/M
|
Jaundice
|
Acute cholangitis, acute pancreatitis: CTSI 6/10
|
|
24
|
76/F
|
Abdominal pain
|
Acute pancreatitis 2/10
|
|
25
|
65/F
|
Abdominal pain
|
Duodenal perforation
|
|
26
|
51/F
|
Abdominal pain, abdominal distention
|
Bowel perforation, thrombus SMV
|
|
27
|
61/M
|
Abdominal pain
|
Acute pancreatitis CTSI 4/10
|
|
28
|
50/F
|
Fever, abdominal pain
|
Acute pancreatitis: CTSI 8/10, contained duodenal perforation, acute cholangitis,
cholangitic abscesses
|
|
29
|
25/F
|
Abdominal pain
|
Acute pancreatitis: CTSI 4/10
|
|
30
|
62/F
|
Abdominal pain
|
Groove pancreatitis: CTSI 6/10
|
|
31
|
65/F
|
Abdominal pain
|
Acute pancreatitis: CTSI 4/10
|
|
32
|
32/F
|
Dyspnea, tachycardia
|
PTE
|
|
33
|
42/F
|
Abdominal pain, vomiting
|
Duodenal perforation
|
|
34
|
33/F
|
Jaundice
|
Displaced stent
|
|
35
|
25/F
|
Hypotension, abdominal pain
|
Sealed duodenal perforation
|
|
36
|
37/F
|
Abdominal pain
|
Colonic perforation
|
|
37
|
37/F
|
Abdominal pain
|
Acute pancreatitis: CTSI 6/10
|
|
38
|
49/F
|
Abdominal pain
|
Acute pancreatitis: CTSI 8/10
|
|
39
|
35/M
|
Abdominal pain, jaundice
|
GB perforation
|
|
40
|
4/M
|
Suspicion of perforation during procedure
|
Gross intraperitoneal, retroperitoneal and subcutaneous air—perforation
|
|
41
|
72/M
|
Hypotension, fall in Hb
|
Pseudoaneurysm in RHA
|
Abbreviations: ARDS, acute respiratory distress syndrome; CBD, common bile duct; CTSI,
computed tomography severity index; ERCP, endoscopic retrograde cholangiopancreatography;
GB, gallbladder; LPV, left portal vein; MPD, main pancreatic duct; PTE, pulmonary
thromboembolism; RHA, right hepatic artery; RHV, right haptic vein; RPV, right portal
vein; SMV, superior mesenteric vein.
Clinical Features
Of the 41 patients, abdominal pain was the most common symptom, which was observed
in 34 patients (82.9%). The second most common symptom was sudden-onset jaundice,
which was seen in eight patients (19.5%). Other common clinical signs observed included
abdominal distention, fever, and tachycardia in 7 patients each (17%), dyspnea in
6 patients (14.6%), hypotension in 3 patients (7.3%), bleeding in 2 patients (4.8%),
and clinical features of acute respiratory distress syndrome (ARDS) in 1 patient (2.4%).
Radiological Findings
Collections: The most common complication detected in CT post-ERCP was presence of intra-abdominal
collections, seen in 21 patients (51.2%). The collections were mostly commonly seen
in association with pancreatitis. The most common location of these collections was
peripancreatic, which was seen in 13 patients (31.7%). The rest were pericholecystic
in three patients (7.3%), perihepatic in three patients (7.3%), and peritoneal in
two patients (4.8%). All the collections were hypodense having a density varying from
8 to 32 Hounsfield Units (HU). In one case, there was increase of HU in subsequent
phases of study suggestive of contrast extravasation (24–46). However, no point source
of contrast extravasation could be identified.
Pancreatitis: The next most common complication detected by imaging was pancreatitis, which was
seen in 20 of 41 patients (48.7%). The most common type of pancreatitis among these
patients was acute interstitial edematous pancreatitis (IEP), seen in 13 patients
(31.7%). The average modified computed tomography severity index (M-CTSI) score in
these subsets of patients was 4.7. Acute necrotizing pancreatitis (NP) was seen in
seven patients (17%). The average M-CTSI score was 8.
Bowel perforation: The radiological impression of perforation was given in nine patients. The most common
finding was that of paraduodenal collection, which was seen in eight patients, followed
by free or loculated air loculi in either paraduodenal, peritoneal, or retroperitoneal
location. Active contrast extravasation was not seen in any patient. Only one patient
showed a paraduodenal collection, which increased in HU on subsequent phases of study.
Duodenal site perforation was the most likely impression given in eight patients.
Pleural effusion: It was present in eight patients (19.5%). It was bilateral in 50% of the patients
and right sided in three patients.
Infections: Liver abscess was detected in six patients (14.6%). The segments involved varied
involving both lobes of the liver including the caudate lobe and segments 2, 3, and
6 to 8. The most common associated imaging finding seen in all cases was intrahepatic
biliary dilatation. Cholangitis was present in four patients (9.7%).
Procedure related: Gallbladder (GB) perforation was present four patients (9.7%), displaced common bile
duct (CBD) stent was seen in three patients (7.3%), and possibility of main pancreatic
duct (MPD) cannulation was given in two patients. Vascular injury resulting in right
hepatic artery pseudoaneurysm was seen in one patient (2.4%).
Others: Thrombosis of the portal vein or its branches was seen in two patients (4.8%), superior
mesenteric vein thrombosis was seen in one patient (2.4%), and right hepatic vein
thrombosis was seen in one patient (2.4%). Pulmonary thromboembolism was present in
2 patients (4.8%), duodenal inflammation in one patient (2.4%), bowel ileus in 4 patients
(9.6%), and bowel obstruction in 1 patient (2.4%).
Discussion
General Concept: Clinical Indications for Imaging, Role of CT, and Normal Imaging
Findings Post-ERCP
A combination of symptoms, clinical signs, intraoperative procedural findings, and
laboratory results often states the requirement for imaging. A difficult or precut
sphincterotomy, multiple cannulation attempts, suspected DP during stenting, abrupt
onset of post-procedural abdominal pain, abdominal distension, fever, unexplained
and persisting tachycardia, significant hypotension, elevated leukocyte count, raised
acute phase reactants, increase in serum lipase or amylase, and decreasing hemoglobin
are some of the factors that form the clinical indications for imaging.[10] In the acute setting, contrast-enhanced CT (CECT) is the imaging modality of choice
for evaluation of complications in the post-ERCP setting.[11] At our center, we recommend a multiphasic CT protocol that includes a nonenhanced
scan followed by scans in the late arterial (25–30 seconds) and portal venous phases
(60–70 seconds) scans after ingestion of oral contrast. Nonenhanced CT is useful for
identification of stent locations and visualization of hyperattenuating collections
of fresh blood. The late arterial phase reveals any vascular injuries in the form
of active contrast extravasation and pseudoaneurysms. Extravasation of oral contrast
from the bowel lumen is helpful in identifying the site of DP.
Some of the normal imaging findings post-ERCP includes the presence of intra- and
extrahepatic pneumobilia, as shown in [Fig. 1], which should not be confused for any pathology. Pneumobilia may even persist for
months in case of sphincterotomy or stent placement. Retained contrast in the biliary
system may be seen on imaging immediately following ERCP having a characteristic striated
appearance,[12] as shown in [Fig. 1]. Post-ERCP acute duodenitis may be visible as edematous wall thickening and is a
reversible condition.
 Fig. 1 A 25-year-old male patient 1 day after endoscopic retrograde cholangiopancreatography
(ERCP). (A) Noncontrast computed tomography (NCCT) axial image showing pneumobilia (arrow) and (B) contrast-enhanced computed tomography (CECT) and (C) maximum intensity projection (MIP) images show stents in the bile duct and the main
pancreatic duct (MPD; curved arrow). Normal appearance post-ERCP.
Fig. 1 A 25-year-old male patient 1 day after endoscopic retrograde cholangiopancreatography
(ERCP). (A) Noncontrast computed tomography (NCCT) axial image showing pneumobilia (arrow) and (B) contrast-enhanced computed tomography (CECT) and (C) maximum intensity projection (MIP) images show stents in the bile duct and the main
pancreatic duct (MPD; curved arrow). Normal appearance post-ERCP.
Pancreatitis
Patients usually present within a few hours with severe epigastric pain, often radiating
to the back, nausea, and mild fever with raised pancreatic enzyme levels.[13] Pancreatitis is diagnosed if two of the following three criteria are present: epigastric
pain consistent with acute pancreatitis, raised serum amylase or lipase levels more
than three times the normal limit, and (or) typical imaging findings.[14] The incidence of PEP (post-ERCP pancreatitis) ranges from 3 to 10% in several studies.[4]
[11]
[15] In our study, the percentage of patients among those sent for imaging and who were
diagnosed to have PEP based on imaging findings was 48.7.
Revised Atlanta classification does not recommend early imaging in acute pancreatitis;
in cases of PEP, imaging (<24–48 hours) may be necessary to exclude other complications
having similar manifestations (especially DP).[15] The type of PEP may be IEP or NP. Due to early imaging, most patients have subtle
findings. In IEP, the pancreas is bulky and homogeneously enhanced with peripancreatic
fat stranding and fluid collections ([Fig. 2]).[16] In NP, there is necrosis of the pancreatic parenchyma or peripancreatic tissue,
which is seen as a hypoenhancing area. They may form nonencapsulated liquefied areas
(acute necrotic collections), which may later (usually after 4 weeks) become organized
and encapsulated to form walled-off necrosis ([Fig. 3]). Early scans, done in the setting of PEP, can underestimate the severity of pancreatitis
and often underdiagnose necrosis.[17] Hence, a repeat CT is often required at a later time frame.
 Fig. 2 A 66-year-old male patient presenting with epigastric pain 1 day after endoscopic
retrograde cholangiopancreatography (ERCP). (a,b) Contrast-enhanced computed tomography (CECT) axial images show bulky pancreas (p)
with fat stranding and fluid in the peripancreatic regions (straight white arrows). The stent is seen in the bile duct (curved arrow) and a calculus in the gallbladder (hollow arrow).
Fig. 2 A 66-year-old male patient presenting with epigastric pain 1 day after endoscopic
retrograde cholangiopancreatography (ERCP). (a,b) Contrast-enhanced computed tomography (CECT) axial images show bulky pancreas (p)
with fat stranding and fluid in the peripancreatic regions (straight white arrows). The stent is seen in the bile duct (curved arrow) and a calculus in the gallbladder (hollow arrow).
 Fig. 3 A 66-year-old male patient presenting with diffuse abdominal pain and fever 3 days
after endoscopic retrograde cholangiopancreatography (ERCP). Axial contrast-enhanced
computed tomography (CT) scan shows focal necrosis (hollow white arrow) of the pancreas (p) with inflammation in the peripancreatic region and fluid collections
in the mesentery (straight white arrow). The stent seen in the bile duct and the duodenum (thick white arrows).
Fig. 3 A 66-year-old male patient presenting with diffuse abdominal pain and fever 3 days
after endoscopic retrograde cholangiopancreatography (ERCP). Axial contrast-enhanced
computed tomography (CT) scan shows focal necrosis (hollow white arrow) of the pancreas (p) with inflammation in the peripancreatic region and fluid collections
in the mesentery (straight white arrow). The stent seen in the bile duct and the duodenum (thick white arrows).
M-CTSI may be used to grade the severity of acute pancreatitis.[18] In a large single-center study conducted by Woods et al, PEP was graded as mild
(≤2 points) in 53.6%, moderate (4–6 points) in 42.8%, and severe (≥8 points) in 3.6%
of cases.[19] In our study, 65% of the cases were of acute IEP and the rest were NP. The severity
of PEP was graded as mild (≤2 points) in 5%, moderate (4–6 points) in 65%, and severe
(≥8 points) in 30% of cases. This difference may be explained as probably only moderate
to severe cases are usually sent for imaging. All mild cases who self-recover may
not undergo any imaging.
Bowel Perforation
Bowel perforation is rare, with an incidence of approximately 0.08 to 0.6%, but it
is one of the most fatal complications with a mortality rate of 9 to 18%.[20] Stapfer et al[7] created a classification system for DPs to predict the need for surgery, based on
mechanism, anatomical location, and descending order of severity. Type I perforations
include duodenoscope-induced perforations of the medial or lateral duodenal wall.
Type II perforations were those seen in the periampullary region of the D2 segment
duodenal wall by sphincterotomy or papillotomy of the bile duct or pancreas. Type
III perforation involves injury to the bile or pancreatic ducts. Type IV perforation
is a minor retroperitoneal insignificant perforation due to excessive endoscopic insufflations
only indicated by the presence of retroperitoneal air.[7] Risk factors include repeated dilatation of CBD, stricture dilatation, sphincter
of Oddi dysfunction, presence of paraduodenal diverticula, and previous surgery.[10] DP after ERCP often mimics PEP, and delayed diagnosis can be fatal. Therefore, a
lower threshold for imaging is required.
CT scan with a water-soluble oral contrast agent has the highest sensitivity to assess
the presence of perforation.[21] The presence of extraluminal air is a hallmark of imaging of DP. Air may be present
in the duodenal wall, retroperitoneum, or intraperitoneal compartment ([Fig. 4]). Air may be present normally for 24 hours post-procedure due to insufflation or
accidental direction of the catheter tip into the submucosa of the duodenum.[7] The imaging findings should be interpreted with the clinical features of the case
in mind. In type II DP, free air usually collects behind the head of the pancreas
and duodenum. It may also be found around the inferior vena cava and in the right
perinephric and anterior pararenal space ([Fig. 5]). Rarely, air may spread around the portal vein and splanchnic vessels, sometimes
across the midline and into the posterior mediastinum. Volume of air detected has
no correlation with patient outcome nor does it indicate the need for surgery as it
depends upon the amount insufflated during the procedure.[22]
[23]
 Fig. 4
(A) Axial noncontrast computed tomography (CT) scan of a 65-year-old female patient post
endoscopic retrograde cholangiopancreatography (ERCP) shows multiple air loculi in
the mesentery with fat stranding and fluid collections (straight white arrows). Common bile duct (CBD) stent is seen in situ with oral contrast in the duodenum
(hollow white arrow). (B,C) Axial contrast CT scan of a 51-year-old woman presenting with abdominal pain during
ERCP shows air in the retroperitoneum, around the right kidney, and the inferior vena
cava (straight white arrows). (D) Axial contrast-enhanced CT (CECT) image of a 22-year-old man post-ERCP shows air
in the duodenal wall (straight white arrow). Duodenostomy tube in situ (curved white arrows).
Fig. 4
(A) Axial noncontrast computed tomography (CT) scan of a 65-year-old female patient post
endoscopic retrograde cholangiopancreatography (ERCP) shows multiple air loculi in
the mesentery with fat stranding and fluid collections (straight white arrows). Common bile duct (CBD) stent is seen in situ with oral contrast in the duodenum
(hollow white arrow). (B,C) Axial contrast CT scan of a 51-year-old woman presenting with abdominal pain during
ERCP shows air in the retroperitoneum, around the right kidney, and the inferior vena
cava (straight white arrows). (D) Axial contrast-enhanced CT (CECT) image of a 22-year-old man post-ERCP shows air
in the duodenal wall (straight white arrow). Duodenostomy tube in situ (curved white arrows).
 Fig. 5 A 51-year-old female patient presenting with pain in the epigastrium 1 day after
endoscopic retrograde cholangiopancreatography (ERCP). (A) Axial and (B) coronal contrast-enhanced computed tomography (CECT) images in the soft-tissue window
and (C) coronal CT lung window image show extensive pneumo-retroperitoneum (straight white arrows) and fluid collection (curved white arrow) around the D2 and D3 segments of the duodenum. (D) Type II perforation.
Fig. 5 A 51-year-old female patient presenting with pain in the epigastrium 1 day after
endoscopic retrograde cholangiopancreatography (ERCP). (A) Axial and (B) coronal contrast-enhanced computed tomography (CECT) images in the soft-tissue window
and (C) coronal CT lung window image show extensive pneumo-retroperitoneum (straight white arrows) and fluid collection (curved white arrow) around the D2 and D3 segments of the duodenum. (D) Type II perforation.
The second most sensitive imaging finding for perforation was fluid collections adjacent
to bowel loops. Delayed imaging of these collections may show progressive increase
in HU values even if the actual site of perforation could not be identified on scans
([Fig. 6]). A large perforation may result in the formation of intra- or retroperitoneal collections
that are often bilious and may be infected ([Fig. 7]). The most specific but least sensitive imaging sign is oral extraluminal contrast
extravasation, and it was not seen in any of our positive cases. This is probably
because small perforations usually seal off by themselves.
 Fig. 6 A 69-year-old female patient presenting with epigastric pain and abdominal distention
1 day after endoscopic retrograde cholangiopancreatography (ERCP). (A) Noncontrast computed tomography (NCCT) and (B) contrast-enhanced computed tomography (CECT) axial images with oral contrast illustrate
an ill-defined dependent collection (straight white arrows) inferior to the D2/D3 segments of the duodenum, which shows an increase in Hounsfield
unit (HU) in subsequent images with layered hyperdense contents within it suggestive
of leaked contrast subsequent to perforation; however, the exact site of perforation
is not delineated. Pneumo-retroperitoneum in the anterior pararenal space (curved white arrow).
Fig. 6 A 69-year-old female patient presenting with epigastric pain and abdominal distention
1 day after endoscopic retrograde cholangiopancreatography (ERCP). (A) Noncontrast computed tomography (NCCT) and (B) contrast-enhanced computed tomography (CECT) axial images with oral contrast illustrate
an ill-defined dependent collection (straight white arrows) inferior to the D2/D3 segments of the duodenum, which shows an increase in Hounsfield
unit (HU) in subsequent images with layered hyperdense contents within it suggestive
of leaked contrast subsequent to perforation; however, the exact site of perforation
is not delineated. Pneumo-retroperitoneum in the anterior pararenal space (curved white arrow).
 Fig. 7 A 51-year-old male patient presenting with abdominal pain and fever. (A,B) Axial contrast-enhanced computed tomography (CECT) images showing subhepatic collection
with air (hollow white arrow), suggesting biloma. Stent noted in the bile duct (white arrow). Straight yellow arrow indicates caudate lobe hepatic abscess.
Fig. 7 A 51-year-old male patient presenting with abdominal pain and fever. (A,B) Axial contrast-enhanced computed tomography (CECT) images showing subhepatic collection
with air (hollow white arrow), suggesting biloma. Stent noted in the bile duct (white arrow). Straight yellow arrow indicates caudate lobe hepatic abscess.
Infections
Cholangitis
Cholangitis is seen in 0.5 to 3% of patients following ERCP.[24]
[25] Classic clinical presentation includes fever, jaundice, and abdominal pain (Charcot's
triad).[11] In the presence of systemic sepsis, additional symptoms of hypotension and altered
mental status (Reynold's pentad) may develop. The primary role of imaging in a case
of clinically suspected cholangitis is to identify the etiology. Ultrasound is the
first modality useful for identifying intrahepatic biliary dilatation and biliary
abscesses. Subsequent CT or magnetic resonance (MR) imaging may demonstrate nonspecific
findings such as thickened enhancing bile duct walls ([Fig. 8]), enlarged hyperenhancing bulging papilla, and periportal T2 hyperintensity and
(or) diffusion restriction in addition to biliary dilatation.[26]
[27] Liver parenchyma may show inhomogeneous enhancement or (and) parenchymal cholangitic
abscesses ([Fig. 9]).
 Fig. 8 A 60-year-old male patient presenting with obstructive jaundice 2 days after endoscopic
retrograde cholangiopancreatography (ERCP). (A,B) Contrast-enhanced computed tomography (CECT) axial images show thickened and enhancing
bile duct walls (straight white arrows). Pericholecystic fluid (hollow white arrow) and surgical drain (curved white arrow) were also seen.
Fig. 8 A 60-year-old male patient presenting with obstructive jaundice 2 days after endoscopic
retrograde cholangiopancreatography (ERCP). (A,B) Contrast-enhanced computed tomography (CECT) axial images show thickened and enhancing
bile duct walls (straight white arrows). Pericholecystic fluid (hollow white arrow) and surgical drain (curved white arrow) were also seen.
 Fig. 9 A 46-year-old female patient presenting with history of persistent fever post endoscopic
retrograde cholangiopancreatography (ERCP) stenting. (A–C) Contrast-enhanced computed tomography (CECT) axial images show a few lesions scattered
in the liver with hyperdense contents in close vicinity of the biliary radicles. Few
lesions also appear hypodense and wedge shaped (straight white arrows). Stent noted in the bile duct (curved red arrow). (D) CECT image (axial) of the same patient showing eccentric filling defect in the anterior
branch of the right portal vein (straight white arrow) with pneumobilia (curved red arrow).
Fig. 9 A 46-year-old female patient presenting with history of persistent fever post endoscopic
retrograde cholangiopancreatography (ERCP) stenting. (A–C) Contrast-enhanced computed tomography (CECT) axial images show a few lesions scattered
in the liver with hyperdense contents in close vicinity of the biliary radicles. Few
lesions also appear hypodense and wedge shaped (straight white arrows). Stent noted in the bile duct (curved red arrow). (D) CECT image (axial) of the same patient showing eccentric filling defect in the anterior
branch of the right portal vein (straight white arrow) with pneumobilia (curved red arrow).
Cholecystitis
Acute cholecystitis is thought to occur due to the contamination of the GB by contaminated
iodinated contrast in the setting of obstruction of the cystic duct or GB dyskinesia.[11] A recent study by Cao et al[28] found a previous history of acute pancreatitis or chronic cholecystitis, metallic
stent placement into the biliary duct, and an elevated leucocyte counts before ERCP
as added risk factors.
Clinical presentation may be similar to cholangitis, and imaging is necessary to make
the correct diagnosis. Cross-sectional imaging may show a distended GB with thickened
wall showing abnormal wall enhancement and pericholecystic fluid.[29] Nontreated advanced cases may lead to GB perforation ([Fig. 10]).
 Fig. 10
(A,B) Axial contrast-enhanced computed tomography (CECT) scan of a 41-year-old female patient
presenting with pain in the right hypochondrium, 3 days after stenting, shows diffuse
wall thickening of the gallbladder (straight white arrow) with discontinuity of wall (thick white arrow), air in the gallbladder lumen (hollow white arow) with air–fluid level and pericholecystic and perihepatic fat stranding and fluid
collections (curved red arrows) suggesting emphysematous acute cholecystitis with perforation.
Fig. 10
(A,B) Axial contrast-enhanced computed tomography (CECT) scan of a 41-year-old female patient
presenting with pain in the right hypochondrium, 3 days after stenting, shows diffuse
wall thickening of the gallbladder (straight white arrow) with discontinuity of wall (thick white arrow), air in the gallbladder lumen (hollow white arow) with air–fluid level and pericholecystic and perihepatic fat stranding and fluid
collections (curved red arrows) suggesting emphysematous acute cholecystitis with perforation.
Duodenoscope Related
The most common infections seen post-ERCP procedure are those related to duodenoscope
due to inadequate sterilization especially of its unique elevator mechanism that helps
orient its accessories in the endoscopic field of view, damaged parts, and presence
of contaminated automated endoscope reprocessor (AER).
Other infections include hepatic abscesses and pseudocyst or Walled Off Necrosis (WON)
infection ([Fig. 11]) seen as hypoattenuating collections with peripheral wall enhancement.
 Fig. 11 A 51-year-old male patient presenting with fever and abdominal distention after endoscopic
retrograde cholangiopancreatography (ERCP). (A) Axial contrast-enhanced computed tomography (CECT) image shows two peripherally enhancing
collections in the right anterior pararenal space and right perinephric space with
air within suggesting infected walled of necrosis (straight white arrows). (B) Pigtail drain is noted in the collection post-intervention (thick white arrow).
Fig. 11 A 51-year-old male patient presenting with fever and abdominal distention after endoscopic
retrograde cholangiopancreatography (ERCP). (A) Axial contrast-enhanced computed tomography (CECT) image shows two peripherally enhancing
collections in the right anterior pararenal space and right perinephric space with
air within suggesting infected walled of necrosis (straight white arrows). (B) Pigtail drain is noted in the collection post-intervention (thick white arrow).
Stent-Related Complications
Acute complications due to stent placement are relatively infrequent and include pancreatitis,
hemorrhage, stent misplacement, and injury to the MPD or CBD.[30] Injury to MPD ([Fig. 12]) or CBD may result in irregularity or discontinuity of the duct and periductal collections
that may or may not show obvious communication with the duct. Small injuries without
evidence of peritonitis on imaging are managed conservatively followed by endoscopic
removal of stent. In the presence of peritonitis or large fluid collection, surgical
or interventional management is advised.[31]
 Fig. 12 A 46-year-old female patient presenting with suspicion of the main pancreatic duct
(MPD) injury and post endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis
1 day after ERCP). (A,B) Contrast-enhanced computed tomography (CECT) images showing ill-defined collection
in the head of the pancreas (thick white arrow) communicating with MPD (thin straight white arrow) that shows proximal dilatation and irregularity and abrupt cutoff with fat stranding
and fluid in the peripancreatic regions (hollow white arrows).
Fig. 12 A 46-year-old female patient presenting with suspicion of the main pancreatic duct
(MPD) injury and post endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis
1 day after ERCP). (A,B) Contrast-enhanced computed tomography (CECT) images showing ill-defined collection
in the head of the pancreas (thick white arrow) communicating with MPD (thin straight white arrow) that shows proximal dilatation and irregularity and abrupt cutoff with fat stranding
and fluid in the peripancreatic regions (hollow white arrows).
Stent obstruction, fracture, migration, and collapse are chronic complications. Stent
obstruction is most common. Obstructed stents are seen in about 6% of cases, which
are evident by the absence of pneumobilia in the biliary tree in addition to biliary
dilatation.[32] Migration is the most common especially with plastic stents. Migration may be proximal
or distal, commonly into the small intestine ([Fig. 13]).[33]
 Fig. 13 A 75-year-old male patient presenting with bleeding post endoscopic retrograde cholangiopancreatography
(ERCP). (A,B) Axial contrast-enhanced computed tomography (CECT) and (C) sagittal images (C) show displaced common bile duct (CBD) stent in the right upper quadrant within jejunal
loops (straight arrows). Fat stranding is seen in the peripancreatic region (thick arrow).
Fig. 13 A 75-year-old male patient presenting with bleeding post endoscopic retrograde cholangiopancreatography
(ERCP). (A,B) Axial contrast-enhanced computed tomography (CECT) and (C) sagittal images (C) show displaced common bile duct (CBD) stent in the right upper quadrant within jejunal
loops (straight arrows). Fat stranding is seen in the peripancreatic region (thick arrow).
Hemorrhage
Hemorrhage is an unusual complication taking place after ERCP, with an incidence of
0.3 to 2%.[34] It typically follows a sphincterotomy; other causes comprise dilatation of stricture,
biopsy, and ablative therapy.[35] On imaging, dilated intra-biliary channels with intraluminal hyperdense contents
or with a duodenal wall mural hematoma may be seen. A dense subcapsular collection
or hemoperitoneum may be seen due to rupture of the liver capsule vessels or biliary
tree during guidewire manipulation or balloon dilatation. Biliary stents may erode
adjacent blood vessels. Arterial phase CT scans in such cases may show active contrast
extravasation or pseudoaneurysms adjacent to the stent requiring vascular embolization
([Fig. 14]). The most common arterial or venous territories involved in these cases are anterior
and posterior pancreatoduodenal vessels.[36] Hepatic artery and its branches may also be involved adjacent to the stent as seen
in our case series.
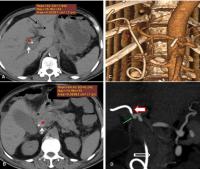 Fig. 14 A 72-year-old male patient presenting with history of melena, 2 months after biliary
stenting. (A,B) Noncontrast computed tomography (NCCT) of the abdomen shows hyperdense contents (red
#) in the common hepatic duct (CHD) and common bile duct (CBD; white arrows) with minimal intrahepatic biliary radicle dilatation (IHBRD; black arrow). (C) Coronal CT angiography scan VRT and (D) maximum intensity projection (MIP) images show a pseudoaneurysm ([red arrow in (C) and green arrow in (D)]) arising from the right hepatic artery (thick arrow) due to erosion by the upper part of the stent (hollow white arrow)
Fig. 14 A 72-year-old male patient presenting with history of melena, 2 months after biliary
stenting. (A,B) Noncontrast computed tomography (NCCT) of the abdomen shows hyperdense contents (red
#) in the common hepatic duct (CHD) and common bile duct (CBD; white arrows) with minimal intrahepatic biliary radicle dilatation (IHBRD; black arrow). (C) Coronal CT angiography scan VRT and (D) maximum intensity projection (MIP) images show a pseudoaneurysm ([red arrow in (C) and green arrow in (D)]) arising from the right hepatic artery (thick arrow) due to erosion by the upper part of the stent (hollow white arrow)
Other Complications
ERCP has also been associated with pneumothorax, ileus, air embolism, and pancreatic
or biliary fistulas after the procedure.[10] Accidental cannulation of the portal vein or stenting and subsequent thrombosis
is another reported complication.[37] Rarely, splenic injury has been reported due to traction applied while passing the
endoscope through the stomach's greater curvature.[38] Complications arising from accessories used during ERCP such as impacted retrieval
basket around a large calculus have also been reported.[39]






