

Subscribe to RSS
DOI: 10.1055/s-0043-1776054
Readout-Segmented Echoplanar (RESOLVE) Diffusion-Weighted Imaging on 3T MRI in Detection of Cholesteatoma—Our Experience
Authors
Funding None.


Abstract
Background Several research studies have demonstrated the utility of diffusion-weighted imaging (DWI) in detecting middle ear cholesteatomas, especially with the non-echoplanar imaging (non-EPI) DWI technique. REadout Segmentation Of Long Variable Echo trains (RESOLVE), a multishot-EPI DWI, has better spatial resolution at a thinner section acquisition with reduced image distortion compared to the single-shot-EPI DWI technique.
Purpose In this study, we evaluated the diagnostic ability of RESOLVE -DWI in middle ear cholesteatomas with surgical and histopathological support.
Patients and Methods Fifty patients with clinical suspicion of primary cholesteatoma or postoperative recurrence were subjected to routine sequences and RESOLVE-DWI on magnetic resonance imaging (MRI). Thirty-eight patients had unilateral disease, while 12 patients had bilateral disease. The bilateral temporal bones of 50 patients were evaluated on MRI. The results attained by RESOLVE-DWI were correlated with intraoperative and histopathological findings.
Results RESOLVE-DWI truly detected 55 of the 58 surgically proven cholesteatomas. RESOLVE-DWI could not detect three cholesteatoma lesions due to their small size and falsely diagnosed one case each of impacted wax and non-cholesteatomatous otitis media as cholesteatoma. With a 95% confidence interval, RESOLVE-DWI showed 94.8% sensitivity, 95.2% specificity, 96% positive predictive value, 93% negative predictive value, and 95% diagnostic accuracy in cholesteatoma detection.
Conclusion RESOLVE-DWI is a sensitive and specific DWI technique for detecting middle ear cholesteatoma. However, RESOLVE-DWI has limitations in the diagnosis of small (<3 mm) cholesteatomas.
Introduction
Cholesteatoma, the most common complication of chronic suppurative otitis media (CSOM), is defined as keratin debris deposition in the middle ear and other pneumatized areas of the temporal bone.[1] Cholesteatoma insidiously spreads locally, causing bony destruction and severe complications, involving the semicircular canal or labyrinth with fistula formation and intracranial complications in advanced cases.[1] [2] [3] High-resolution computed tomography (HRCT) is the most commonly used radiological modality to assess cholesteatoma.[3] [4] [5] HRCT delineates the detailed anatomy of the temporal bone, including small bony structures and soft tissue lesions. However, HRCT cannot reliably distinguish inflammatory or granulation tissue, fluid, and scar tissue, and has a limited role in the postoperative suspected recurrent or residual cholesteatoma.[4] Magnetic resonance imaging (MRI) with improved soft tissue resolution and diffusion-weighted imaging (DWI) capabilities has become a significant part of evaluating cholesteatomas. DWI uses water molecule Brownian motion to create images with impedance to the free movement of water molecules resulting in high signal intensity that helps in the diagnosis. Cholesteatomas appear hyperintense on DWI due to less mobile water molecules and keratin debris restricting water diffusion and due to the T2-shine through effect.[1] DWI can help differentiate between cholesteatoma and inflammatory or granulation tissue, fluid, or scar tissue.[6] [7] [8] [9] DWI is classified into echoplanar imaging-based (EPI) and non-EPI-based techniques. Depending on the number of radiofrequency pulses applied, EPI and non-EPI DWI can be acquired by either single-shot (SS) or multishot (MS) techniques.[1]
The non-EPI DWI technique has been proven to be useful in cholesteatoma detection due to thinner achievable sections with excellent resolution, lack of susceptibility artifacts, and image distortions.[1] [2] [8] [10] [11] The conventional SS EPI-DWI technique is susceptible to severe artifacts at the interfaces of bone and air with a suboptimal image resolution of the temporal bones.[1] [12] [13] Readout Segmented EPI (RS-EPI) DWI or RESOLVE (REadout Segmentation Of Long Variable Echo trains) is a MS-EPI DWI technique. RESOLVE-DWI employs a similar diffusion preparation as the traditional SS-EPI, while dividing the k-space trajectories into different segments in the readout direction, with subsequent reduced echo spacing (TE) compared to SS-EPI DWI.[14] Two-dimensional phase navigator incorporated in the RESOLVE sequence allows for correction of motion errors and requires the phase navigator and reacquisition of unusable data in real-time image[14] [15] This improves spatial resolution at a thinner slice thickness with reduced image distortion and susceptibility artifacts compared to SS-EPI.[11] [12] RESOLVE-DWI can be achieved with a shorter TE (echo time) than some non-EPI DWI, allowing for higher resolution with thinner sections and shorter imaging time.[13]
We evaluated the accuracy of the RESOLVE-DWI sequence on a 3-tesla (3T) MRI scanner in identifying cholesteatoma in CSOM patients or those suspected of postoperative recurrence compared to surgical and histological results.
Patients and Methods
Study Design and Subjects
This observational, descriptive prospective study was conducted between September 2019 and August 2021 at a tertiary care hospital in western India. Prior Institutional Ethical Committee (IEC) clearance was obtained (IESC/PGS/2019/173). Fifty patients with clinical suspicion of CSOM or suspected postoperative recurrence were selected based on clinical signs and symptoms, otoscopic and HRCT (128 slice CT scanner, Philips Ingenuity Core, the Netherlands) temporal bone findings. MRI of the bilateral temporal bones was performed in all patients. All patients or the parent/guardian of minor patients provided written and informed consent.
Imaging Technique
MRI was obtained on a 3-tesla scanner (Magnetom Vida, Siemens Healthineers, Erlangen, Germany) using a 64-channel head coil after ruling out any MRI incompatibility factors. RESOLVE-DWI in transverse plane was obtained with 0, 800, and 1,000 s/mm2 b-values using 4-trace diffusion mode and following parameters: time of repetition (TR): 4700 ms; echo time (TE): 64 and 106 ms; flip angle (FA): 180 degrees; acceleration factor: iPAT =2; field of view (FOV): 200 mm; number of excitations (NEX) = 1; voxel size = 1.04 × 1.04 × 2.5 mm3 (reconstruction: 0.52 × 0.52 × 2.5 mm3); resolution 192 × 192; slice thickness 2.5 mm with no interslice gap; 25 slices with each sequence; acquisition time: 5 minutes, 07 seconds. Axial T1-weighted (TR 400 ms/TE 7.8 ms; 2.5 mm slice thickness ; FA: 150 degrees; FOV:160 mm; NEX: 2; matrix 320 × 320; time 2 min 34 sec), axial T2-weighted (TR 5000 ms/TE 90 ms; slice thickness: 2.5 mm; FA:150 degrees; FOV:190 mm; NEX:2; matrix 384 × 384; time: 2 min 47 sec), coronal T2-weighted and T2 fat saturated (TR 3400 ms /TE 89 ms; 2.5 mm slice thickness; FA:150 degrees; FOV:160 mm; NEX:2; matrix: 448 × 314; time:2 minutes, 24 seconds) sequences were obtained for anatomical structural evaluation and localization of the lesions.
Imaging Evaluation
MRI studies were independently assessed by two radiologists with 16 and 14 years of experience, respectively. MRI studies of the bilateral temporal bones of 50 patients were evaluated for the presence of soft tissue lesions, location, size, and characteristics of the lesion on routine sequences. The width of the lesions was measured on routine T2-weighted images (T2WI) and DWI sequences. The interpreters were blinded to the HRCT and intraoperative and histopathological examination (HPE) findings. In case of a difference of opinion, the final diagnosis was made after mutual discussion and consensus. Cholesteatoma appears isointense to hypointense on T1-weighted images (T1WI) compared to gray matter, hyperintense on T2WI, and exhibits a hyperintense signal on DWI with higher b-values (800, 1000 s/mm2) due to the presence of keratin in cholesteatoma and T2 shine through.[1] [2] The granulation tissue, scar/fibrous tissue, serous fluid, and cholesterol granuloma appear dark on DWI, particularly on higher b-values.[1] Hence, the lesions with the hyperintense signal on high b-value (800, 1000 s/mm2) RESOLVE-DWI were labeled as cholesteatoma.
The surgeries were carried out by two head and neck surgeons with 16 and 15 years of experience, respectively. The surgeons were blinded to the RESOLVE-DWI findings; however, they had access to the HRCT findings. Sixty-three temporal bones, based on clinical and imaging findings, underwent surgery within 16 weeks from the time of the MRI. The second look surgery was delayed and performed after 6 months of MRI in one postoperative temporal bone with no soft tissue on imaging. The patients with bilateral disease underwent the second operation 8 to 10 weeks after the first surgery. The average time gap between MRI and surgery was 4.4 weeks (shortest 3 days and longest 180 days). The final diagnosis was obtained using surgical and HPE corroboration.
Statistical Analysis
Quantitative and qualitative data were tabulated in Microsoft Excel and Word. The numerical data was presented as mean ± standard deviation, range, and percentages. The RESOLVE-DWI findings were categorized as true positives or negatives and false positives or negatives in correlation with intraoperative findings and HPE results. Cohen's kappa (κ) test was used to calculate the interobserver agreement. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of RESOLVE-DWI in diagnosing cholesteatoma with a 95% percent confidence interval were calculated. Microsoft Excel 2007 and SPSS version 26 (IBM Corp, USA) were used for statistical analysis.
Results
Fifty patients in the study had an average age of 25.4 ± 10.8 years (range: 8–65 years), with equal distribution of males and females. The common clinical symptoms included purulent ear discharge (84%), hearing loss (64%) and otalgia (46%), tinnitus (22%), bleeding (18%), and mucoid discharge (16%). The bilateral temporal bones of 50 patients, a total of 100 temporal bones, were assessed with MRI. The geometrical distortion and air–bone interface distortion artifacts on DWI could be identified and allocated in correlation with the routine MRI sequences. DWI were of diagnostic quality in all patients, and artifacts did not interfere with the image interpretation in any of the patients.
Out of 100 temporal bones, 57 temporal bones were positive, and 43 were negative on RESOLVE-DWI ([Fig. 1]). RESOLVE-DWI hyperintense lesions, better seen on b-value of 1000 s/mm2, were present in unilateral temporal bones in 33 patients, and bilateral temporal bones in 12 patients. Interobserver agreement between the two radiologists was excellent (94%, k = 0.877). Out of 57 temporal bones with DWI-positive lesions, 55 were proven as cholesteatomas that included 53 primary and 2 recurrent lesions ([Fig. 2]). Two postoperative temporal bones with DWI-positive lesions were found to be non-cholesteatomatous otitis media and impacted wax, labeled as false positive cases ([Fig 3] and [Fig 4A]-[C]). Three symptomatic temporal bones showed no lesion on routine MRI or RESOLVE-DWI. One temporal bone with cholesterol granuloma, postoperative one temporal bone with no cholesteatoma, and two with granulation tissue were correctly diagnosed and considered as true negatives. The remaining 36 asymptomatic temporal bones had no soft tissue on MRI and were also considered true negatives after clinical, otoscopic, and HRCT correlation for statistical purposes. No surgical procedures were done in these 36 asymptomatic normal temporal bones. This method was similarly applied by Yamashita et al in a comparative study of MS-EPI and SS-EPI DWI techniques in detecting cholesteatoma in 29 patients, which included assessment of 30 and 28 temporal bones with and without cholesteatomas, respectively.[16]

Thirty-seven out of 57 DWI positive lesions (64.9%) were of size more than 9 mm in size, 16 (28%) lesions were 6 to 9 mm, and 4 (7%) were in the 3 to 6 mm size range ([Fig. 2], [Fig. 4D]-[F]). The mean diameter of lesions was 11.3 mm (standard deviation ± 5.8), and the median size was 10.5 mm (range: 3–30 mm). The lesions were smaller on DWI compared to T2WI, with size discrepancy in the range of 0.2 to 1.3 mm. Three lesions of size less than 3 mm were not detected on RESOLVE-DWI and routine MRI, which included two postoperative temporal bones ([Fig. 5]). These surgically proved cholesteatomas measuring 2 mm (2 lesions) and 2.5 mm were categorized as false negative results. The mean apparent diffusion coefficient (ADC) value for cholesteatoma was 1000.2 × 10−6 mm2/s (range: 537.6–1646.3 × 10−6 mm2/s). The granulation tissue showed ADC value of 1722 × 10−6 mm2/s (range: 1,450–1,980 10−6 mm2/s), while cholesterol granuloma had ADC value of 2155 × 10−6 mm2/s. ADC values of 1050.3 × 10−6 mm2/s and 862 × 10−6 mm2/s were recorded in impacted wax and non-cholesteatomatous otitis media, respectively.

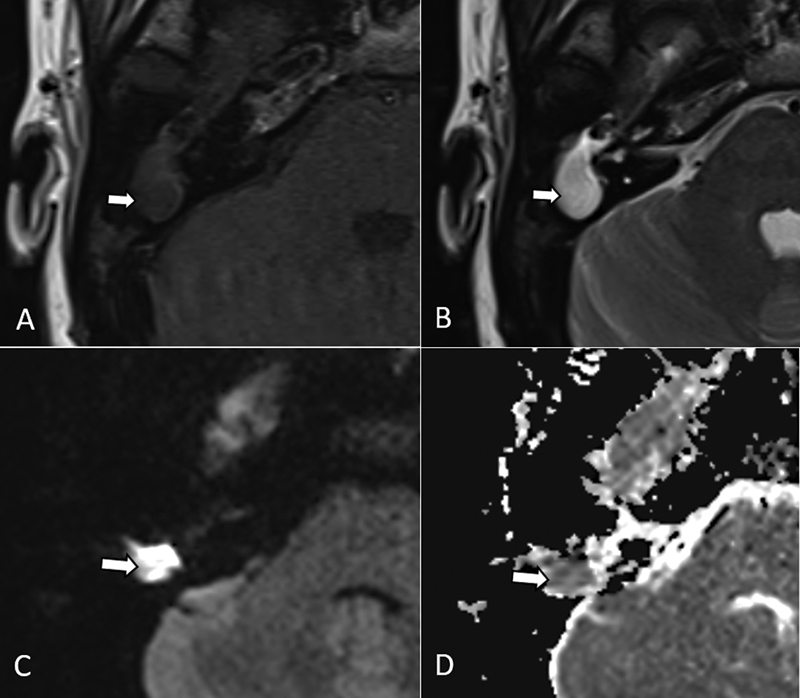
In nine postoperative temporal bones, the average period between surgery and postoperative MRI was 4.6 years. RESOLVE-DWI with surgical correlation detected cholesteatoma in two temporal bones and granulation tissue in two temporal bones. Routine MRI with DWI could not detect cholesteatoma in two postoperative temporal bones due to the small size (< 3 mm). Out of two false positives, one was due to impacted wax, which appeared hyperintense on T1WI but showed peripheral hypointense foci, which were hyperintense on DWI and were labeled as cholesteatoma ([Fig. 3]). The other lesion was a non-cholesteatomatous otitis media that showed mixed signals on T2WI and hypointense signals on T1WI with foci of hyperintense signal on DWI ([Fig. 4]). No cholesteatoma was seen in one postoperative temporal bone on MRI as well as during second-look surgery.


Fifty-eight (54 primary and 4 recurrent) temporal bones were proven to have cholesteatoma on surgery, out of which 55 lesions had concordance on RESOLVE-DWI. The overall sensitivity, specificity, PPV, NPV, and diagnostic accuracy of RESOLVE-DWI in detecting cholesteatoma were 94.8, 95.2, 96.5, 93, and 95%, respectively ([Table 1]). RESOLVE-DWI in the cases of recurrent cholesteatoma had a sensitivity of 50%, specificity of 60%, and diagnostic accuracy of 55.56% in our study ([Table 2]).
|
Hyperintense soft tissue on RESOLVE-DWI (n = 100)[a] |
Surgical /histopathological validation |
|
|---|---|---|
|
Present |
Absent |
|
|
Present |
55 (TP) |
2 (FP) |
|
Absent |
3 (FN) |
40 (TN) |
|
Statistical data of the diagnostic performance of RESOLVE-DWI |
||
|
Parameter |
Point estimate |
95% Confidence interval |
|
Sensitivity |
94.8% |
85.6–98.9 |
|
Specificity |
95.2% |
83.8–99.4 |
|
PPV |
96.5% |
87.9–99.6 |
|
NPV |
93.0% |
80.9–98.5 |
|
Accuracy |
95.0% |
88.7–98.4 |
Abbreviations: FN, false negatives; FP, false positives; NPV, negative predictive value; PPV, positive predictive value; RESOLVE-DWI, Readout-Segmented Echoplanar diffusion-weighted imaging; TN, true negatives; TP, true positives.
a Bilateral temporal bones in 50 patients; total of 100 temporal bones were evaluated.
Abbreviations: FN, false negatives; FP, false positives; RESOLVE-DWI, Readout-Segmented Echoplanar diffusion-weighted imaging; TN, true negatives; TP, true positives.
Discussion
Conventional SS-EPI DWI has limited value in the evaluation of the middle ear cholesteatoma due to susceptibility and T2 blurring artifacts, lack of thinner sections, and often missing smaller (< 5 mm) cholesteatoma.[9] [17] These artifacts in SS-EPI become more prominent on the higher strength 3-tesla magnet leading to suboptimal image resolution of middle ear.[8] [12] [18] RESOLVE-DWI, a new MS-EPI DWI technique with same diffusion preparation as SS-EPI, offers better spatial resolution and reduced image distortion and artifacts at thinner slices compared to SS-EPI and is proven superior to SS-EPI in detecting cholesteatoma.[12] [14] [16] [18] Only a few studies to date have evaluated RESOLVE-DWI in detecting cholesteatoma on a 3-tesla MR scanner.[17] [18] [19] The present validation study assessed the utility of RESOLVE-DWI in the identification of primary or recurrent cholesteatoma.
RESOLVE-DWI demonstrated an overall sensitivity of 94.8% and specificity of 95.2% for cholesteatoma detection in the current study. Fischer et al[12] and Yamashita et al[16] reported a similar trend of higher specificity (96 and 100%, respectively) than sensitivity (88 and 76.7%, respectively) using RESOLVE-DW-MRI, though Algin et al[18] reported higher sensitivity (100%) than specificity (78%). Significant variation in the results has been reported in other studies, with a sensitivity range of 68 to 100% and a specificity range of 60 to 96%.[12] [16] [18] [19] Wiesmueller et al explained the possible reason for low sensitivity (68%) and specificity (60%) in their study as the smaller sizes of the cholesteatomas (median 0.5 cm) and use of shortened TEs for RS-DWI that could reduce the hyperintense signals of cholesteatomas.[19] We found PPV of 96.5%, NPV of 93%, and accuracy of 95% for detecting cholesteatoma with RESOLVE-DWI, which was comparable to results achieved by Fischer et al, who reported PPV of 96%, NPV of 89%, and accuracy of 92%.[12]
The cholesteatomas were of iso to hypointense signals on T1WI and hyperintense signals on T2WI, consistent with the signal characteristics of cholesteatoma reported in the literature.[8] [13] [20] Dudau et al used the T1 hyperintense signal of the soft tissue as the criteria to downgrade the indeterminate middle ear and mastoid lesions in their study, which were mostly not cholesteatomas, emphasizing the importance of correlating conventional T1W sequences with DWI for the assessment of cholesteatoma.[13] Yamashita et al stated that T1 and DWI hyperintense lesion was strongly suggestive of cholesterol granuloma, as was seen in one of the lesions in our study.[16] We found the mean ADC values for cholesteatoma to be 1000.2 × 10−6 mm2/s (range: 537.6–1646.3 × 10−6 mm2/s), while granulation tissue and cholesterol granuloma showed ADC values of 1722 × 10−6 mm2/s and 2155 × 10−6 mm2/s, respectively. Russo et al reported 859.4 × 10−6 mm2/s average ADC value for cholesteatomas (range: 276.3 to 1,545 × 10−6 mm2/s) and 2,216.3 × 10−6 mm2/s for non-cholesteatomatous inflammatory lesions.[21] There is wide variation in the reported ADC values for cholesteatoma in the literature, and we could not find one absolute cutoff value.[6] [18] [21] [22] [23] The hyperintense signal on DWI seen in cholesteatoma is caused by either diffusion restriction or T2 shine-through effect.[1] [10] ADC values for a DWI hyperintense cholesteatoma lesion due to the T2 shine-through effect would come higher than expected, leading to nonuniformity in ADC values, which may not be in a diagnostical range.[1] [2] [23] Therefore, it may be diagnostically sufficient to analyze DWI at higher b-values alone to identify cholesteatoma.[1] [12] [13] [16] [24]
Three surgically confirmed cholesteatomas of less than 3 mm were not seen on RESOLVE-DWI or routine MRI using 2.5 mm slice thickness and no interslice gap. Fisher et al reported false negative results in the small size cholesteatomas on RESOLVE-DWI with a 3 mm slice thickness, one of which was of size 4 mm.[12] The detection can be improved with 2 mm slice thickness; however, this will increase the scan time.[12] [17] Lingam et al in their systematic review found that cholesteatomas of size less than 3 mm are likely to be missed on DWI performed on 1.5-tesla as well as 3-tesla MRI machines.[10] The lack of adequate keratin to produce a signal on DWI, autoatticotomy, suppurative cholesteatoma, movement artifacts, and lower imaging matrix are some of the possible causes for these false negative results.[10] [12] [25] Sheng et al[17] and Algin et al[18] mentioned magnetic susceptibility artifact and air–bone interface distortion with the suboptimal evaluation of the middle ear as the likely causes for the failure to detect small cholesteatoma on RESOLVE-DW-MRI. Lips et al reported higher sensitivity and specificity of non-EPI DWI on 1.5T (91 and 76%) than 3T (72 and 46%) for the detection of residual/recurrent cholesteatoma and stated that better resolution on 3T did not compensate for the more artifacts due to magnetic field inhomogeneities.[26] Lincot et al found no effect of magnetic field strength in the correct diagnosis of cholesteatomas in their comparative study of non-EPI-DWI on 1.5T and 3T scanners.[8] We mostly encountered geometrical distortion and air–bone interface artifacts in RESOLVE-DWI performed on 3T scanner ([Fig. 6]); however, they did not impede the imaging diagnoses in any of the cases. The DWI hyperintense signal due to air–bone artifacts could be very well differentiated from actual lesions using the synchronized T2WI with anatomical section localizer ([Fig. 6 C, D]).

The two false-positive cases in our study were due to impacted wax and non-cholesteatomatous otitis media in the postoperative patients. Lingam et al reported three false-positive cases in their study of 56 postoperative patients due to cerumen and non-cholesteatomatous tissue that can produce hyperintense signals on DWI.[22] Dental amalgam artifacts, myringosclerosis, granulation tissue, fluid with high protein or purulent contents, cholesterol granuloma, and neoplasm in adjacent structures like the external auditory canal can also produce false positive results.[10]
RESOLVE-DWI had a lower sensitivity (50%) and specificity (60%) in cases of recurrent cholesteatoma in our study, which may be due to the small sample size (9 cases) and the fact that two out of four lesions were less than 3 mm in size, which are likely to be missed on DWI.[10] [25] [26] [27] [28] [29] van Egmond et al found a wide range of reported sensitivity (43–92%) and specificity (58–100%) for the detection of cholesteatoma on DWI in postoperative patients in their systematic review and meta-analysis study.[27] Plouin-Gaudon et al reported 62% sensitivity and 88% specificity for DWI in their study of 21 pediatric patients suspected of recurrent cholesteatoma and could not detect cholesteatoma of size less than 3 mm or presenting as diffuse thin lining in the middle ear.[28] Lecler et al found even lower sensitivity for DWI in postoperative residual cholesteatoma (40 and 30% for two observers), which was mainly attributed to the small (<3 mm) size of the cholesteatomas.[29] Non-EPI DWI has been shown to perform better than EPI DWI in the detection of recurrent and residual cholesteatoma by many authors.[25] [30] However, Horn et al with a reported sensitivity of 59% for non-EPI DWI in the detection of recurrent cholesteatoma at 9 months follow-up concluded that it cannot replace the second look surgery due to false negatives.[31] RESOLVE-DWI, a relatively newer technique, needs to be evaluated further for its utility for recurrent or residual disease.
Non-EPI DWI is a well-established sensitive sequence in the detection of primary as well as recurrent cholesteatoma.[10] [11] [20] [27] Lingam and Bassett reported 91% sensitivity and 92% specificity for non-EPI DWI in the detection of middle ear cholesteatoma in a pooled analysis in their meta-analysis.[10] The non-EPI technique has various advantages over the EPI technique, including a superior signal-to-noise ratio, absence of significant image distortion and susceptibility flaws, and drastically higher spatial resolution.[1] [11] [13] [17] [27] However, false positive results due to wax/debris, abscess, encephaloceles, and bone/cartilage grafts[32] and false negative results due to small (<3 mm) lesions have also been reported with non-EPI DWI.[10] Dudau et al found RS-EPI (readout-segmented EPI) comparable to non-EPI DWI techniques for the detection of cholesteatoma with good correlation between the two techniques.[13] However, non-EPI DWI had less skull base susceptibility artifacts and better predicted the cholesteatoma in cases of disparity. Benson et al found non-EPI DWI (HASTE) superior to RESOLVE-DWI in the detection of primary and residual/recurrent cholesteatomas, mainly due to equivocal, often false negative results because of smaller and less hyperintense appearance of cholesteatomas on RESOLVE images.[24] According to Wiesmueller et al, the turbo spin-echo (TSE)-DWI technique is preferable with better sensitivity (92%) and specificity (80%) than RS-DWI (sensitivity 76%, specificity 60%) for diagnosing cholesteatomas.[19] Sheng et al found that turbo gradient- and spin-echo-DWI (TGSE) with BLADE trajectory, a non-EPI DWI technique, offered improved image quality compared to RESOLVE due to reduced susceptibility artifacts, image blurring, and distortion and was more useful in the detection of small (2 mm) sized cholesteatomas.[17]
One of the limitations of our study was that RESOLVE-DWI was not compared to the more commonly used non-EPI DWI techniques due to the resources and time constraints. We performed RESOLVE-DWI on a 3-tesla machine which gives exceptional image resolution; but also increases susceptibility artifacts because of its high field strength and inhomogeneities.[12] [26] The maximum number of lesions in our study were of size 9 mm and above and were relatively easy to identify and less affected by the image resolution. RESOLVE-DWI could not detect the cholesteatoma of size less than 3 mm in our study. The sample size for postoperative patients was also small in our study. Therefore, further work is required to determine the utility of RESOLVE-DWI in the detection of smaller cholesteatomas and postoperative recurrent/residual cholesteatoma.
Conclusion
In our study, RESOLVE-DWI revealed high overall sensitivity, specificity, and accuracy to detect middle ear cholesteatomas and can provide a viable alternate option to non-EPI DWI. However, RESOLVE-DWI could not detect small cholesteatoma of size less than 3 mm, which would necessitate close clinical follow-up and further imaging evaluation in such cases.
Conflict of Interest
None declared.
Note
The study was conducted at the Dr. D. Y. Patil Medical College, Hospital and Research Center, Pimpri, Pune, Maharashtra, India.
Ethical Approval and Consent to Participate
This study was approved prior by the IEC with research protocol number IESC/PGS/2019/173. All patients or the parent/guardian of minor patients provided written and informed consent.
-
References
- 1 Henninger B, Kremser C. Diffusion weighted imaging for the detection and evaluation of cholesteatoma. World J Radiol 2017; 9 (05) 217-222
- 2 Vaid S, Kamble Y, Vaid N. et al. Role of magnetic resonance imaging in cholesteatoma: the Indian experience. Indian J Otolaryngol Head Neck Surg 2013; 65 (Suppl. 03) 485-492
- 3 Castle JT. Cholesteatoma pearls: practical points and update. Head Neck Pathol 2018; 12 (03) 419-429
- 4 Tierney PA, Pracy P, Blaney SP, Bowdler DA. An assessment of the value of the preoperative computed tomography scans prior to otoendoscopic 'second look' in intact canal wall mastoid surgery. Clin Otolaryngol Allied Sci 1999; 24 (04) 274-276
- 5 Handi PS, Patil MN, Nisha P. High resolution computed tomography of temporal bone in the evaluation of otologic diseases. IntJ Otorhinolaryngol Head Neck Surg. 2018; 4: 87-92
- 6 Osman NM, Rahman AA, Ali MT. The accuracy and sensitivity of diffusion-weighted magnetic resonance imaging with apparent diffusion coefficients in diagnosis of recurrent cholesteatoma. Eur J Radiol Open 2017; 4: 27-39
- 7 Cimsit NC, Cimsit C, Baysal B, Ruhi IC, Ozbilgen S, Aksoy EA. Diffusion-weighted MR imaging in postoperative follow-up: reliability for detection of recurrent cholesteatoma. Eur J Radiol 2010; 74 (01) 121-123
- 8 Lincot J, Veillon F, Riehm S. et al. Middle ear cholesteatoma: compared diagnostic performances of two incremental MRI protocols including non-echo planar diffusion-weighted imaging acquired on 3T and 1.5T scanners. J Neuroradiol 2015; 42 (04) 193-201
- 9 De Foer B, Vercruysse JP, Bernaerts A. et al. The value of single-shot turbo spin-echo diffusion-weighted MR imaging in the detection of middle ear cholesteatoma. Neuroradiology 2007; 49 (10) 841-848
- 10 Lingam RK, Bassett P. A meta-analysis on the diagnostic performance of non-echoplanar diffusion-weighted imaging in detecting middle ear cholesteatoma: 10 years on. Otol Neurotol 2017; 38 (04) 521-528
- 11 Sharifian H, Taheri E, Borghei P. et al. Diagnostic accuracy of non-echo-planar diffusion-weighted MRI versus other MRI sequences in cholesteatoma. J Med Imaging Radiat Oncol 2012; 56 (04) 398-408
- 12 Fischer N, Schartinger VH, Dejaco D. et al. Readout-segmented echo-planar DWI for the detection of cholesteatomas: correlation with surgical validation. Am J Neuroradiol 2019; 40 (06) 1055-1059
- 13 Dudau C, Draper A, Gkagkanasiou M, Charles-Edwards G, Pai I, Connor S. Cholesteatoma: multishot echo-planar vs non echo-planar diffusion-weighted MRI for the prediction of middle ear and mastoid cholesteatoma. BJR Open 2019; 1 (01) 20180015
- 14 Porter DA, Heidemann RM. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two-dimensional navigator-based reacquisition. Magn Reson Med 2009; 62 (02) 468-475
- 15 Naganawa S, Yamazaki M, Kawai H, Sone M, Nakashima T, Isoda H. Anatomical details of the brainstem and cranial nerves visualized by high resolution readout-segmented multi-shot echo-planar diffusion-weighted images using unidirectional MPG at 3T. Magn Reson Med Sci 2011; 10 (04) 269-275
- 16 Yamashita K, Yoshiura T, Hiwatashi A. et al. Detection of middle ear cholesteatoma by diffusion-weighted MR imaging: multishot echo-planar imaging compared with single-shot echo-planar imaging. Am J Neuroradiol 2011; 32 (10) 1915-1918
- 17 Sheng Y, Hong R, Sha Y, Zhang Z, Zhou K, Fu C. Performance of TGSE BLADE DWI compared with RESOLVE DWI in the diagnosis of cholesteatoma. BMC Med Imaging 2020; 20 (01) 40
- 18 Algin O, Aydın H, Ozmen E. et al. Detection of cholesteatoma: high-resolution DWI using RS-EPI and parallel imaging at 3 tesla. J Neuroradiol 2017; 44 (06) 388-394
- 19 Wiesmueller M, Wuest W, May MS. et al. Comparison of readout-segmented echo-planar imaging and single-shot TSE DWI for cholesteatoma diagnostics. Am J Neuroradiol 2021; 42 (07) 1305-1312
- 20 Ishii K, Takahashi S, Kobayashi T, Matsumoto K, Ishibashi T. MR imaging of middle ear cholesteatomas. J Comput Assist Tomogr 1991; 15 (06) 934-937
- 21 Russo C, Elefante A, Di Lullo AM. et al. ADC benchmark range for correct diagnosis of primary and recurrent middle ear cholesteatoma. BioMed Res Int 2018; 2018: 7945482
- 22 Lingam RK, Khatri P, Hughes J, Singh A. Apparent diffusion coefficients for detection of postoperative middle ear cholesteatoma on non-echo-planar diffusion-weighted images. Radiology 2013; 269 (02) 504-510
- 23 Thiriat S, Riehm S, Kremer S, Martin E, Veillon F. Apparent diffusion coefficient values of middle ear cholesteatoma differ from abscess and cholesteatoma admixed infection. Am J Neuroradiol 2009; 30 (06) 1123-1126
- 24 Benson JC, Carlson ML, Lane JI. Non-EPI versus multishot EPI DWI in cholesteatoma detection: correlation with operative findings. Am J Neuroradiol 2021; 42 (03) 573-577
- 25 Lingam RK, Nash R, Majithia A, Kalan A, Singh A. Non-echoplanar diffusion weighted imaging in the detection of post-operative middle ear cholesteatoma: navigating beyond the pitfalls to find the pearl. Insights Imaging 2016; 7 (05) 669-678
- 26 Lips LMJ, Nelemans PJ, Theunissen FMD. et al. The diagnostic accuracy of 1.5 T versus 3 T non-echo-planar diffusion-weighted imaging in the detection of residual or recurrent cholesteatoma in the middle ear and mastoid. J Neuroradiol 2020; 47 (06) 433-440
- 27 van Egmond SL, Stegeman I, Grolman W, Aarts MC. A systematic review of non-echo planar diffusion-weighted magnetic resonance imaging for detection of primary and postoperative cholesteatoma. Otolaryngol Head Neck Surg 2016; 154 (02) 233-240
- 28 Plouin-Gaudon I, Bossard D, Fuchsmann C, Ayari-Khalfallah S, Froehlich P. Diffusion-weighted MR imaging for evaluation of pediatric recurrent cholesteatomas. Int J Pediatr Otorhinolaryngol 2010; 74 (01) 22-26
- 29 Lecler A, Lenoir M, Peron J. et al. Magnetic resonance imaging at one year for detection of postoperative residual cholesteatoma in children: is it too early?. Int J Pediatr Otorhinolaryngol 2015; 79 (08) 1268-1274
- 30 Muzaffar J, Metcalfe C, Colley S, Coulson C. Diffusion-weighted magnetic resonance imaging for residual and recurrent cholesteatoma: a systematic review and meta-analysis. Clin Otolaryngol 2017; 42 (03) 536-543
- 31 Horn RJ, Gratama JWC, van der Zaag-Loonen HJ, Droogh-de Greve KE, van Benthem PG. Negative predictive value of non-echo-planar diffusion weighted MR imaging for the detection of residual cholesteatoma done at 9 months after primary surgery is not high enough to omit second look surgery. Otol Neurotol 2019; 40 (07) 911-919
- 32 Muhonen EG, Mahboubi H, Moshtaghi O. et al. False-positive cholesteatomas on non-echoplanar diffusion-weighted magnetic resonance imaging. Otol Neurotol 2020; 41 (05) e588-e592
Address for correspondence
Publication History
Article published online:
23 November 2023
© 2023. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Henninger B, Kremser C. Diffusion weighted imaging for the detection and evaluation of cholesteatoma. World J Radiol 2017; 9 (05) 217-222
- 2 Vaid S, Kamble Y, Vaid N. et al. Role of magnetic resonance imaging in cholesteatoma: the Indian experience. Indian J Otolaryngol Head Neck Surg 2013; 65 (Suppl. 03) 485-492
- 3 Castle JT. Cholesteatoma pearls: practical points and update. Head Neck Pathol 2018; 12 (03) 419-429
- 4 Tierney PA, Pracy P, Blaney SP, Bowdler DA. An assessment of the value of the preoperative computed tomography scans prior to otoendoscopic 'second look' in intact canal wall mastoid surgery. Clin Otolaryngol Allied Sci 1999; 24 (04) 274-276
- 5 Handi PS, Patil MN, Nisha P. High resolution computed tomography of temporal bone in the evaluation of otologic diseases. IntJ Otorhinolaryngol Head Neck Surg. 2018; 4: 87-92
- 6 Osman NM, Rahman AA, Ali MT. The accuracy and sensitivity of diffusion-weighted magnetic resonance imaging with apparent diffusion coefficients in diagnosis of recurrent cholesteatoma. Eur J Radiol Open 2017; 4: 27-39
- 7 Cimsit NC, Cimsit C, Baysal B, Ruhi IC, Ozbilgen S, Aksoy EA. Diffusion-weighted MR imaging in postoperative follow-up: reliability for detection of recurrent cholesteatoma. Eur J Radiol 2010; 74 (01) 121-123
- 8 Lincot J, Veillon F, Riehm S. et al. Middle ear cholesteatoma: compared diagnostic performances of two incremental MRI protocols including non-echo planar diffusion-weighted imaging acquired on 3T and 1.5T scanners. J Neuroradiol 2015; 42 (04) 193-201
- 9 De Foer B, Vercruysse JP, Bernaerts A. et al. The value of single-shot turbo spin-echo diffusion-weighted MR imaging in the detection of middle ear cholesteatoma. Neuroradiology 2007; 49 (10) 841-848
- 10 Lingam RK, Bassett P. A meta-analysis on the diagnostic performance of non-echoplanar diffusion-weighted imaging in detecting middle ear cholesteatoma: 10 years on. Otol Neurotol 2017; 38 (04) 521-528
- 11 Sharifian H, Taheri E, Borghei P. et al. Diagnostic accuracy of non-echo-planar diffusion-weighted MRI versus other MRI sequences in cholesteatoma. J Med Imaging Radiat Oncol 2012; 56 (04) 398-408
- 12 Fischer N, Schartinger VH, Dejaco D. et al. Readout-segmented echo-planar DWI for the detection of cholesteatomas: correlation with surgical validation. Am J Neuroradiol 2019; 40 (06) 1055-1059
- 13 Dudau C, Draper A, Gkagkanasiou M, Charles-Edwards G, Pai I, Connor S. Cholesteatoma: multishot echo-planar vs non echo-planar diffusion-weighted MRI for the prediction of middle ear and mastoid cholesteatoma. BJR Open 2019; 1 (01) 20180015
- 14 Porter DA, Heidemann RM. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two-dimensional navigator-based reacquisition. Magn Reson Med 2009; 62 (02) 468-475
- 15 Naganawa S, Yamazaki M, Kawai H, Sone M, Nakashima T, Isoda H. Anatomical details of the brainstem and cranial nerves visualized by high resolution readout-segmented multi-shot echo-planar diffusion-weighted images using unidirectional MPG at 3T. Magn Reson Med Sci 2011; 10 (04) 269-275
- 16 Yamashita K, Yoshiura T, Hiwatashi A. et al. Detection of middle ear cholesteatoma by diffusion-weighted MR imaging: multishot echo-planar imaging compared with single-shot echo-planar imaging. Am J Neuroradiol 2011; 32 (10) 1915-1918
- 17 Sheng Y, Hong R, Sha Y, Zhang Z, Zhou K, Fu C. Performance of TGSE BLADE DWI compared with RESOLVE DWI in the diagnosis of cholesteatoma. BMC Med Imaging 2020; 20 (01) 40
- 18 Algin O, Aydın H, Ozmen E. et al. Detection of cholesteatoma: high-resolution DWI using RS-EPI and parallel imaging at 3 tesla. J Neuroradiol 2017; 44 (06) 388-394
- 19 Wiesmueller M, Wuest W, May MS. et al. Comparison of readout-segmented echo-planar imaging and single-shot TSE DWI for cholesteatoma diagnostics. Am J Neuroradiol 2021; 42 (07) 1305-1312
- 20 Ishii K, Takahashi S, Kobayashi T, Matsumoto K, Ishibashi T. MR imaging of middle ear cholesteatomas. J Comput Assist Tomogr 1991; 15 (06) 934-937
- 21 Russo C, Elefante A, Di Lullo AM. et al. ADC benchmark range for correct diagnosis of primary and recurrent middle ear cholesteatoma. BioMed Res Int 2018; 2018: 7945482
- 22 Lingam RK, Khatri P, Hughes J, Singh A. Apparent diffusion coefficients for detection of postoperative middle ear cholesteatoma on non-echo-planar diffusion-weighted images. Radiology 2013; 269 (02) 504-510
- 23 Thiriat S, Riehm S, Kremer S, Martin E, Veillon F. Apparent diffusion coefficient values of middle ear cholesteatoma differ from abscess and cholesteatoma admixed infection. Am J Neuroradiol 2009; 30 (06) 1123-1126
- 24 Benson JC, Carlson ML, Lane JI. Non-EPI versus multishot EPI DWI in cholesteatoma detection: correlation with operative findings. Am J Neuroradiol 2021; 42 (03) 573-577
- 25 Lingam RK, Nash R, Majithia A, Kalan A, Singh A. Non-echoplanar diffusion weighted imaging in the detection of post-operative middle ear cholesteatoma: navigating beyond the pitfalls to find the pearl. Insights Imaging 2016; 7 (05) 669-678
- 26 Lips LMJ, Nelemans PJ, Theunissen FMD. et al. The diagnostic accuracy of 1.5 T versus 3 T non-echo-planar diffusion-weighted imaging in the detection of residual or recurrent cholesteatoma in the middle ear and mastoid. J Neuroradiol 2020; 47 (06) 433-440
- 27 van Egmond SL, Stegeman I, Grolman W, Aarts MC. A systematic review of non-echo planar diffusion-weighted magnetic resonance imaging for detection of primary and postoperative cholesteatoma. Otolaryngol Head Neck Surg 2016; 154 (02) 233-240
- 28 Plouin-Gaudon I, Bossard D, Fuchsmann C, Ayari-Khalfallah S, Froehlich P. Diffusion-weighted MR imaging for evaluation of pediatric recurrent cholesteatomas. Int J Pediatr Otorhinolaryngol 2010; 74 (01) 22-26
- 29 Lecler A, Lenoir M, Peron J. et al. Magnetic resonance imaging at one year for detection of postoperative residual cholesteatoma in children: is it too early?. Int J Pediatr Otorhinolaryngol 2015; 79 (08) 1268-1274
- 30 Muzaffar J, Metcalfe C, Colley S, Coulson C. Diffusion-weighted magnetic resonance imaging for residual and recurrent cholesteatoma: a systematic review and meta-analysis. Clin Otolaryngol 2017; 42 (03) 536-543
- 31 Horn RJ, Gratama JWC, van der Zaag-Loonen HJ, Droogh-de Greve KE, van Benthem PG. Negative predictive value of non-echo-planar diffusion weighted MR imaging for the detection of residual cholesteatoma done at 9 months after primary surgery is not high enough to omit second look surgery. Otol Neurotol 2019; 40 (07) 911-919
- 32 Muhonen EG, Mahboubi H, Moshtaghi O. et al. False-positive cholesteatomas on non-echoplanar diffusion-weighted magnetic resonance imaging. Otol Neurotol 2020; 41 (05) e588-e592