

Subscribe to RSS
DOI: 10.1055/s-0043-1774298
Utility of Contrast-Enhanced Computed Tomography for Differentiating Pancreatic Ductal Adenocarcinoma from Inflammatory Mass in Chronic Calcific Pancreatitis
Authors
Funding None.


Abstract
Objective The aim of this study was to identify the most useful contrast-enhanced computed tomography (CECT) features for differentiating pancreatic ductal adenocarcinoma (PDAC) from mass-forming chronic pancreatitis (MFCP) in chronic calcific pancreatitis (CCP).
Methods In total, 101 patients with CCP and focal pancreatic mass formed the study group. Sixteen qualitative and four quantitative parameters were analyzed. Qualitative parameters included size, site, margin, intralesional hypodensity, collateral duct sign, abrupt pancreatic duct (PD) cutoff, upstream PD dilatation, distal pancreatic atrophy, double duct sign, enhancement pattern, contrast attenuation, peripancreatic inflammation, vascular involvement, regional nodes, and metastasis. Quantitative parameters included duct-to-body ratio, common bile duct (CBD) diameter, main pancreatic duct (MPD) diameter, and carcinoembryonic antigen 19-9 (CA19-9). Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated for prediction of PDAC. A receiver operating characteristic (ROC) curve analysis was performed and the area under ROC curve (AUROC) was calculated to determine diagnostic accuracy to assess the optimal cutoff.
Results PDAC was confirmed in 48 patients and MFCP in 53 patients. A duct-to-body ratio greater than 0.48 had 95.5% sensitivity, 83.3% specificity, 80.8% PPV, 96.2% NPV, and 88.5% accuracy for predicting PDAC. A CBD diameter cutoff ≥9.5 mm had an accuracy of 75% (p < 0.019) and an MPD cutoff ≥6.25 mm had an accuracy of 67.8% (p = 0.008) for predicting PDAC. On binary logistic regression, the duct-to-body ratio was found to be the significant independent factor associated with malignancy.
Conclusion A duct-to-body ratio greater than 0.48, intralesional hypodensity, and abrupt duct cutoff are the most helpful computed tomography (CT) features for distinguishing PDAC from MFCP in CCP. On binary logistic regression, the duct-to-body ratio was found to be a significant independent factor. Interspersed normal parenchyma was observed as a very specific sign of MFCP. Intraparenchymal hypodensity has high specificity, but further validation is needed.
Keywords
pancreatic ductal carcinoma - inflammatory mass - chronic pancreatitis - pancreatic calcificationIntroduction
Chronic calcific pancreatitis (CCP) is characterized by pancreatic duct (PD) dilatation, pancreatic atrophy, and coarse pancreatic ductal calcification.[1] There in an increased risk of pancreatic ductal adenocarcinoma (PDAC) in CCP.[2] [3] In approximately 30% of patients with CCP, fibrosis and inflammation of the glandular elements manifest as focal pancreatic enlargement that may simulate a mass, an entity known as mass-forming chronic pancreatitis (MFCP) and is a benign entity.[4] Differentiating PDAC from MFCP is difficult due to their overlapping clinical and imaging features.[5] However, the differentiation between PDAC and MFCP is important, as surgical resection is the standard of care for PDAC and the only effective means of cure, whereas MFCP is managed conservatively.[4] Incorrect diagnosis of MFCP as PDAC can result in an unnecessary surgical resection and conversely PDAC diagnosed as MFCP may delay surgical.[2] Noninvasive imaging may play a crucial role in early diagnosis of cancer to differentiate between these two entities.
Multiphasic contrast-enhanced computed tomography (CECT) is the most common initial imaging modality used for evaluation of patients with focal mass lesions in chronic pancreatitis. A literature search shows a few studies differentiating between benign and malignant lesions in CCP.[6]
With CECT, PDAC in CCP shows variable enhancement characteristics. PDAC appearance can vary from a hypodense to isodense to hyperdense mass.[7] MFCP also has variable attenuation based on the extent of fibrosis and inflammatory component and shows increased enhancement compared to PDAC but could appear isodense or hypodense.[7] The imaging features of PDAC and MFCP overlap, making it difficult to differentiate the two entities based on enhancement characteristics alone. Several features of PDAC have been described as characteristic of PDAC including intralesional hypodensity, duct-to-body ratio (DBR), abrupt duct cutoff, distal pancreatic parenchymal atrophy,[8] [9] double duct sign, and vascular involvement,[10] whereas association of a pancreatic mass with pseudocysts, walled-off necrosis, peripancreatic inflammatory changes, collateral duct sign, and interspersed normal parenchyma should raise the possibility of MFCP.[11] [12] [13] Perfusion CT and dual-energy CT are useful advanced technologies that may be helpful in differentiating MFCP from PDAC using perfusion characteristics and iodine uptake within the lesions.[14] [15] However, perfusion CT and dual-energy CT techniques are not widely available.
The purpose of this study is to identify the most useful CT features on multiphasic CECT that would help distinguish PDAC and MFCP in the setting of CCP.
Methods
Study Population
This retrospective study included 101 consecutive patients with CCP who underwent a CECT and had a diagnosis of focal pancreatic mass that was histologically confirmed. The study period was from January 2015 to December 2020 at our institute. The inclusion criteria were (1) CT imaging features of CCP, (2) presence of a focal pancreatic mass, and (3) pathological confirmation of the mass. The pathological specimens were obtained with either endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) or surgical resection. Pathological interpretation was performed by the institutional pathologist with 20 years of experience. Patients without a dedicated multiphasic CECT from our institute were excluded from the study.
Imaging Technique
All the patients were imaged using either a 64-slice multidetector row CT (MDCT; General Electric [GE] Lightspeed, GE Healthcare, Milwaukee, WI, United States) or 128-slice Maxima (GE Healthcare). All the patients received 600 mL of Gastrografin (GE Healthcare) as oral contrast. The protocol consisted of a noncontrast CT performed initially followed by CECT in two phases: pancreatic parenchymal phase at 40 to 50 seconds and portal venous phase at 65 to 70 seconds after the start of injection. A total of 80 to 100 mL (1.5 mL/kg body weight) of 350 mg iodine/mL (Iohexol [Omnipaque], GE Healthcare, Shanghai, China) or Iopromide (Ultravist, Bayer Zydus Pharma Ltd, Whippany, NJ, United States) was administered intravenously at a flow rate of 4 mL/s using a dual head pressure injector (Medrad Stellant CT Injector System, Indianola, PA, United States). The images were obtained from the dome of the diaphragm to the iliac crest in all three phases (noncontrast, pancreatic phase, and portal venous phase).
The CT parameters were current modulation, 5-mm slice thickness with 0.625-mm reconstruction, 35 to 50 cm field of view and 512 × 512 matrix with sagittal and coronal reconstructions.
Image Analysis
Two abdominal radiologists with 21 and 11 years of experience reviewed the images in consensus. The images were reviewed on advantage GE workstation 4.2 and picture archiving and communication system (PACS). Qualitative parameters included size, site of involvement, margin, intralesional hypodensity, collateral duct sign, abrupt PD cutoff, upstream PD dilatation, distal pancreatic atrophy, double duct sign, enhancement pattern, contrast attenuation, peripancreatic inflammation, vascular involvement, regional nodes, and metastasis. Quantitative parameters included DBR, common bile duct (CBD) diameter, main pancreatic duct (MPD) diameter, and carcinoembryonic antigen 19-9 (CA19-9). The final diagnosis of PDAC or MFCP was based on histopathology.
All the qualitative and quantitative parameters were studied in detail to differentiate between benign and malignant masses ([Table 1]).
|
Variable |
Malignancy (N = 53) |
Inflammatory mass (N = 48) |
p-value |
|---|---|---|---|
|
Age (y) |
|||
|
Mean |
53.53 ± 10.37 |
46.40 ± 13.15 |
0.003[a] |
|
Age (y) |
|||
|
10–20 |
0 (0) |
1 (2.1) |
0.039[a] |
|
21–30 |
0 (0) |
5 (10.4) |
|
|
31–40 |
3 (5.7) |
9 (18.8) |
|
|
41–50 |
18 (34) |
15 (31.3) |
|
|
51–60 |
17 (32.1) |
10 (20.8) |
|
|
61–70 |
13 (24.5) |
6 (12.5) |
|
|
71–80 |
1 (1.9) |
2 (4.2) |
|
|
81–90 |
1 (1.9) |
0 (0) |
|
|
Gender |
|||
|
Male |
32 (60.4) |
38 (79.2) |
0.041[a] |
|
Female |
21 (39.6) |
10 (20.8) |
|
|
Size of mass (cm) |
|||
|
<2 |
4 (7.5) |
3 (6.8) |
0.948 |
|
2–5 |
29 (54.7) |
23 (52.3) |
|
|
>5 |
20 (37.7) |
18 (40.9) |
|
|
Site of involvement |
|||
|
Head |
32 (61.5) |
39 (81.3) |
0.063 |
|
Body |
18 (34.6) |
9 (18.8) |
|
|
Tail |
2 (3.8) |
0 (0) |
|
|
Margin |
|||
|
Smooth |
9 (17) |
29 (60.4) |
<0.001[a] |
|
Lobulated |
44 (83) |
19 (39.6) |
|
|
Cystic change |
|||
|
Intralesional hypodensity |
27 (96.4) |
5 (19.2) |
<0.001[a] |
|
Cystic changes like WON/pseudocyst |
1 (3.6) |
21 (80.8) |
|
|
Interspersed parenchyma |
|||
|
Yes |
0 (0) |
28 (59.6) |
<0.001[a] |
|
No |
53 (100) |
19 (40.4) |
|
|
Collateral duct sign |
|||
|
Present |
4 (7.5) |
17 (35.4) |
0.001[a] |
|
Absent |
49 (92.5) |
31 (64.6) |
|
|
Abrupt pancreatic duct cutoff |
|||
|
Smooth |
20 (37.7) |
40 (83.3) |
<0.001[a] |
|
Abrupt |
33 (62.3) |
8 (16.7) |
|
|
Upstream PD dilatation |
|||
|
Yes |
33 (62.3) |
13 (27.1) |
<0.001[a] |
|
No |
20 (37.7) |
35 (72.9) |
|
|
Distal pancreatic atrophy |
|||
|
Yes |
11 (20.8) |
2 (4.3) |
0.014[a] |
|
No |
42 (79.2) |
45 (95.7) |
|
|
Double duct sign |
|||
|
Yes |
24 (45.3) |
22 (45.8) |
0.956 |
|
No |
29 (54.7) |
26 (54.2) |
|
|
Enhancement pattern |
|||
|
Homogenous |
22 (41.5) |
18 (40.9) |
0.138 |
|
Heterogeneous |
31 (58.5) |
26 (59.1) |
|
|
Contrast attenuation |
|||
|
Isodense |
27 (50.9) |
23 (52.3) |
0.978 |
|
Hypodense |
26 (49.1) |
21 (47.7) |
|
|
Peripancreatic inflammation/cyst |
|||
|
Yes |
9 (17) |
44 (97.1) |
<0.001[a] |
|
No |
44 (83) |
4 (8.3) |
|
|
Vascular involvement |
|||
|
Yes |
34 (64.2) |
16 (33.3) |
0.002[a] |
|
No |
19 (35.8) |
32 (66.7) |
|
|
Regional nodes |
|||
|
Yes |
30 (56.6) |
27 (61.4) |
0.635 |
|
No |
23 (43.4) |
17 (38.6) |
|
|
Metastasis |
|||
|
Yes |
14 (26.4) |
0 (0) |
<0.001[a] |
|
No |
39 (73.6) |
44 (100) |
|
|
MPD diameter |
|||
|
Mean (mm) |
10.75 ± 4.91 |
7.51 ± 3.38 |
0.004[a] |
|
Duct-to-body ratio |
|||
|
Mean |
0.69 ± 0.13 |
0.38 ± 0.19 |
<0.001[a] |
|
CBD diameter |
|||
|
Mean (mm) |
11.45 ± 3.65 |
8.90 ± 2.67 |
0.016[a] |
|
CA19-9 |
|||
|
Mean |
7,599.49 ± 45,664.30 |
130.52 ± 365.18 |
<0.001[a] |
Abbreviations: CBD, common bile duct; CCP, chronic calcific pancreatitis; computed tomography; MFCP, mass-forming chronic pancreatitis; MPD, main pancreatic duct; PD, pancreatic duct; PDAC, pancreatic ductal adenocarcinoma; WON; walled-off necrosis.
a Statistically significant.
Intralesional hypodensity was defined as a lack of contrast enhancement surrounded by an irregular inner wall in the postcontrast phase. Walled-off necrosis/abscess was seen in inflammatory mass and was defined as a low-density area with appreciable, thickened, or smooth enhancing wall.[16] [17] [18] They appeared as unilocular or multilocular cystic areas with septa with or without enhancement.
Intralesional interspersed parenchyma refers to the presence of islands of normal pancreatic tissue within the mass.
DBR and MPD diameter were determined just distal to the mass to within 1 cm and pancreatic parenchymal thickness measured perpendicular to the longitudinal axis of the parenchyma at the same point. The CBD diameter was measured at the suprapancreatic level.
The enhancement characteristics analyzed were categorized as homogeneous or heterogeneous depending on the pattern of enhancement and isodense/hyperdense/hypodense compared to the adjacent pancreatic parenchyma in the portal venous phase.
Statistical Analysis
All the data collected were coded and entered in a Microsoft Excel sheet, which was rechecked and analyzed using SPSS statistical software version 22. Quantitative variables were summarized using mean and standard deviation (SD). Categorical variables were represented using frequency and percentage. Independent sample test and Mann–Whitney U test were used to test the statistical significance of difference between the means of variables among different independent groups. Pearson's chi-squared test and Fisher's exact test were used for comparing the categorical variables between groups. The receiver operating characteristic (ROC) curves were generated for comparing the area under the curve (AUC) depicted by different parameters for prediction of malignancy and for finding out the diagnostic characteristics. Binary logistic regression was performed to determine independent factors associated with malignancy. A p-value of less than 0.05 was considered statistically significant.
Results
The study population comprised 70 males and 31 females with age ranging from 15 to 84 years. PDAC was confirmed in 48 patients and MFCP in 53 patients. The mean age of patients with PDAC was significantly higher than that of the patients with MFCP (53.5 ± 10.4 vs. 46.4 ± 13.2 years, p < 0.003). Both PDAC and MFCP were common in males as compared to females. Among the PDAC, 60.4% of patients were males, while 39.6% were females.
Most of the benign and malignant masses measured between 2 and 5 cm with no statistically significant difference between size groups of PDCA compared to MFCP (p = 0.948). The most common location for both MFCP and PDAC was the head (61.5 and 81.3%, respectively) of pancreas followed by the body (34.6 and 18.8%, respectively) with no significant differences (p = 0.06).
A comparison of the qualitative CECT features in PDAC and MFCP was made. The following features were significantly more common in PDAC as compared to MFCP: lobulated margins (83 vs. 39%, p < 0.001), intralesional hypodensity (96.4 vs. 19.2%, p < 0.001), abrupt PD cutoff (62.3 vs. 16.7%, p < 0.001), upstream pancreatic ductal dilatation (62.3 vs. 27.1%, p = 0.014), distal pancreatic atrophy (21 vs. 4.3%, p < 0.014), vascular involvement (64.2 vs. 33.3%, p < 0.002), and the presence of metastasis (26.4 vs. 0, p < 0.001; [Table 2]).
Abbreviations: CBD, common bile duct; CCP, chronic calcific pancreatitis; CECT, contrast-enhanced computed tomography; MPD, main pancreatic duct; NPV, negative predictive value; PD, pancreatic duct; PPV, positive predictive value.
The qualitative CECT features that were significantly more common in MFCP as compared to PDAC were the following: smooth margins (60.4 vs. 17%, p < 0.001), interspersed parenchyma (60 vs. 0%, p < 0.001), collateral duct sign (35.4 vs. 7.5%, p < 0.001), smooth narrowing of the PD (83.3 vs. 38%, p < 0.001), peripancreatic inflammation (97.1 vs.17%, p < 0.001), and peripancreatic cysts (53.8 vs. 5%, p < 0.001; [Table 3]).
Abbreviations: CCP, chronic calcific pancreatitis; NPV, negative predictive value; PPV, positive predictive value; PDAC, pancreatic ductal adenocarcinoma; WON; walled-off necrosis.
CBD dilatation, double duct sign, attenuation characteristics, and regional lymphadenopathy did not contribute to the significant difference between PDAC and MFCP. CBD dilatation was seen in masses located in the head/body lesions extending to the head (45% in PDAC vs 43.8 % in MFCP; p = 0.8).
Among quantitative parameters, the mean pancreatic duct diameter (10.7 ± 5 vs. 7.5 ± 3.4 mm, p = 0.004), pancreatic DBR (0.7 vs. 0.4, p < 0.001) and CBD diameter (11.5 ± 3.7 vs. 8.9 ± 2.7 mm, p = 0.016) were significantly higher in PDAC than in MFCP. An ROC analysis showed that DBR with a cutoff ≥0.48 had 95.5% sensitivity, 83.3% specificity, 80.8% positive predictive value (PPV), 96.2% negative predictive value (NPV), and 88.5% accuracy in predicting PDAC. When the DBR of greater than 0.62 mm was taken as cutoff, it had a sensitivity of 96.2% but a low specificity of 45.5% (p < 0.00). On binary logistic regression, the DBR was found to be the significant independent factor associated with PDAC ([Table 4]).
|
Variable |
p-value |
OR |
95% CI for OR |
|---|---|---|---|
|
Duct-to-body ratio |
0.005[a] |
43,061.189 |
24.700–75,070,225.66 |
|
CA19.9 |
0.050 |
1.004 |
1.000–1.008 |
|
Constant |
0.004[a] |
0.001 |
Abbreviations: CCP, chronic calcific pancreatitis; CI, confidence interval; OR, odds ratio; PDAC, pancreatic ductal adenocarcinoma.
a Statistically significant.
p-value < 0.001*, Cox and Snell R 2 = 0.537; Nagelkerke R 2 = 0.720.
In other ROC analysis results, a CBD diameter cutoff ≥9.5 mm had an accuracy of 75% (p < 0.019) and an MPD cutoff ≥6.25 mm had an accuracy of 67.8% (p = 0.008) for predicting PDAC. CA19-9 levels with cutoff ≥106 IU/mL had 56.6% sensitivity, 91.7% specificity, and 73.3% accuracy (p < 0.001). The CA19.9 levels were significantly higher in patients with PDAC as compared to those with MFCP ([Table 5], [Graphs 1] [2] [3] [4]).
|
Variable |
Area under the curve |
95% confidence interval |
p-value |
|---|---|---|---|
|
Duct-to-body ratio |
0.897 |
0.807–0.987 |
<0.001[a] |
|
MPD diameter |
0.703 |
0.571–0.834 |
0.008[a] |
|
CBD diameter |
0.717 |
0.538–0.895 |
0.019[a] |
|
CA19-9 |
0.721 |
0.614–0.828 |
<0.001[a] |
Abbreviations: CBD, common bile duct; CCP, chronic calcific pancreatitis; MPD, main pancreatic duct; PDAC, pancreatic ductal adenocarcinoma; ROC; receiver operating characteristic.
a Statistically significant.




Discussion
There is an increased risk of PDAC in CCP as evidenced by various studies with cumulative risk increasing over time from less than 2% at 10 years to 4% at 20 years following diagnosis of chronic pancreatitis.[3] We therefore evaluated the CT findings to identify the most useful features for diagnosing malignancy. In this retrospective study, we found that DBR, intraparenchymal hypodensity, and abrupt PD cutoff were the most significant radiological features with higher accuracy for predicting PDAC in CCP.
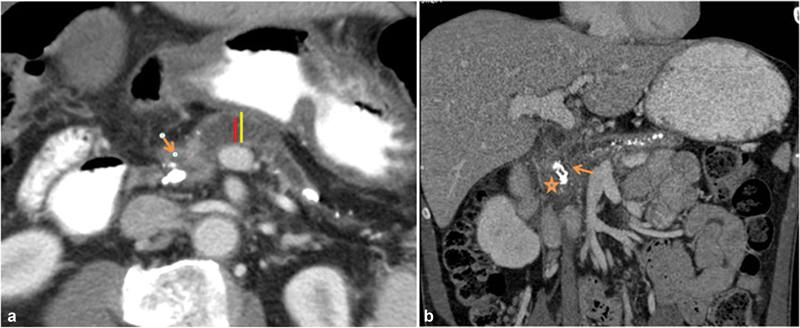
In a prior study, Eloubeidi et al showed that a DBR of greater than 0.34 strongly favors the diagnosis of PDAC.[13] In their study, the PPV, NPV, sensitivity, specificity, and accuracy of pancreatic DBR ≥ 0.34 for detecting malignancy were 87, 99, 94, 97, and 97%, respectively. When the presence of PD dilatation alone was considered, the PPV and accuracy was only 50 and 83%, respectively, for the detection of pancreatic cancer. Another study by Karasawa et al showed that a DBR of greater than 0.5 indicated malignancy.[19] Our study results with DBR of greater than 0.48 are comparable to these studies. On binary logistic regression, the DBR was found to be the significant independent factor associated with malignancy similar to those obtained by Karasawa et al[19] ([Fig. 1]).
Intralesional hypodensity had a high accuracy, sensitivity, and NPV in identifying malignant lesions, although there were overlaps. The diagnosis of intrapancreatic fluid-containing cysts indicated inflammatory mass. Distinguishing intralesional hypodensity from walled-off necrosis is important, although at times difficult. In our study, intralesional hypodensity was more frequent in PDAC compared to MFCP, which was consistent with the study by Ren et al[17] where this finding was seen in 59.6% of PDAC as compared to 28.6% of MFCP cases ([Fig. 2]).

In our study, MPD abrupt cutoff had moderate accuracy of 68% but a high sensitivity of 96.2% for predicting malignancy. Gangi et al[20] has reported that MPD abrupt cutoff and upstream MPD dilatation were the earliest finding of PDAC, and this was detected more than 18 months before the PDAC diagnosis. Abrupt duct cutoff can be identified in malignant lesions, whereas progressive narrowing with smooth tapering of ducts is seen in benign cases.[16] The combination of abrupt PD cutoff and DBR increased the diagnostic accuracy ([Figs. 3] and [4]).


CA19-9, a diagnostic and prognostic marker of malignancy, is also elevated in inflammatory lesions of the pancreas. In our study, a cutoff of 106 for CA19-9 had good specificity but with low sensitivity. There are several studies proposing different cutoffs.[21] [22] In a study by Bedi et al, CA19-9 using a cutoff value of 37 U/mL had 68% sensitivity and 70% specificity.[21] Higher positivity rates were obtained using other cutoff values such as 100, 200, and 300 U/mL and reaching 100% specificity for PDAC using 300U/mL.
Ruan et al[18] showed larger lesions with lobulated margins were predominantly observed in PDAC than in MFCP (83.33 vs. 12.5%) as in our study. It is difficult to assess the margins if the lesions are small and contour nondeforming (<2 cm).[23]
Visible remnants of normal pancreatic tissue (interspersed normal parenchyma) within lesions were a very helpful finding and could be used to distinguish MFCP from PDAC,[18] and our study showed that this finding had a PPV of 100% ([Fig. 5]).

The presence of dilated collateral or side branches of the PD coursing throughout the mass is a finding that can be seen in inflammatory masses.[24] A collateral duct sign is better appreciated in magnetic resonance imaging (MRI) than in CT. In our study, the collateral duct sign was shown to have poor specificity in predicting MFCP. This may be due to the fact that our study included only CECT studies.
We found that the enhancement pattern and contrast attenuation of mass were not statistically significant to differentiate between PDAC and MFCP, which may be due to a variable extent of necrosis or fibrosis in these lesions as suggested by Johnson et al.[25]
Peripancreatic inflammation and pseudocysts had low sensitivity, specificity, and accuracy in differentiating between benign and malignant lesions as pseudocysts could be seen in malignancy due to obstructive pancreatitis.[18] [26]
Vascular involvement may help in differentiation although the vessels can be involved in both MFCP and PDAC. Venous narrowing of the splenoportal confluence with collateral formation is seen in both PDAC and MFCP. Hence, venous encasement did not help in differentiating between benign and malignant lesions. Our study showed vascular involvement in the majority of malignant lesions (64.2%; p = 0.002). However, 33% of MFCP also showed vascular involvement on imaging decreasing the specificity ([Fig. 6]).

Our study has some limitations. This was a retrospective design as our inclusion criteria were histological confirmation of the pancreatic mass. Some of the parameters assessed could not be applied to all masses, for example, DBR could not be applied to masses present in the body and tail masses; CBD dilatation was studied only for head masses. Intralesional hypodensity which is one of the most helpful features in differentiating benign from malignant lesions was seen only in 58% of total cases studied. It is possible that MRI may be more useful in demonstrating several of these signs and the advantage of multiplanar imaging capability. This study focused only on the CECT features as it was the most commonly performed imaging modality in our study population. The utility of MRI should be evaluated in future studies.
Conclusion
Differentiating PDAC from MFCP in CCP continues to be a challenge. A DBR greater than 0.48, intralesional hypodensity, abrupt PD cutoff, and CA19-9 value of 106 IU/mL were the most useful quantitative CT features for distinguishing PDAC from MFCP. The DBR was found to be the significant independent factor associated with malignancy. Interspersed parenchyma is a very specific sign for MFCP. Further characterization of intralesional hypodensity may be possible with advanced imaging applications, large-scale data analysis, and radiomics.
Conflict of Interest
None declared.
Compliance with Ethical Principles
All procedures performed were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all patients for being included in the study.
Author Contributions
All the authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by T.P., D.J., and V.K. The first draft of the manuscript was written by D.J., and all the authors commented on the previous versions of the manuscript. All the authors read and approved the final version of the manuscript.
-
References
- 1 Devière J, Baron TH, Kozarek RA. Chronic pancreatitis: stones and strictures. In: Baron TH, Kozarek TA, Carr-Locke DL. eds. ERCP. 3rd ed.. Philadelphia, PA: Elsevier Inc.; 2019: 516-524.e2
- 2 Raimondi S, Lowenfels AB, Morselli-Labate AM, Maisonneuve P, Pezzilli R. Pancreatic cancer in chronic pancreatitis; aetiology, incidence, and early detection. Best Pract Res Clin Gastroenterol 2010; 24 (03) 349-358
- 3 Lowenfels AB, Maisonneuve P, Cavallini G. et al; International Pancreatitis Study Group. Pancreatitis and the risk of pancreatic cancer. N Engl J Med 1993; 328 (20) 1433-1437
- 4 Schima W, Böhm G, Rösch CS, Klaus A, Függer R, Kopf H. Mass-forming pancreatitis versus pancreatic ductal adenocarcinoma: CT and MR imaging for differentiation. Cancer Imaging 2020; 20 (01) 52
- 5 Zhang T-T, Wang L, Liu HH. et al. Differentiation of pancreatic carcinoma and mass-forming focal pancreatitis: qualitative and quantitative assessment by dynamic contrast-enhanced MRI combined with diffusion-weighted imaging. Oncotarget 2017; 8 (01) 1744-1759
- 6 Liao Q, Zhao YP, Wu WW, Li BL, Li JY. Diagnosis and treatment of chronic pancreatitis. Hepatobiliary Pancreat Dis Int 2003; 2 (03) 445-448
- 7 Yamada Y, Mori H, Matsumoto S, Kiyosue H, Hori Y, Hongo N. Pancreatic adenocarcinoma versus chronic pancreatitis: differentiation with triple-phase helical CT. Abdom Imaging 2010; 35 (02) 163-171
- 8 Frampas E, Morla O, Regenet N, Eugène T, Dupas B, Meurette G. A solid pancreatic mass: tumour or inflammation?. Diagn Interv Imaging 2013; 94 (7–8): 741-755
- 9 Freeny PC, Marks WM, Ryan JA, Traverso LW. Pancreatic ductal adenocarcinoma: diagnosis and staging with dynamic CT. Radiology 1988; Jan; 166 (01) 125-133
- 10 Tamada T, Ito K, Kanomata N. et al. Pancreatic adenocarcinomas without secondary signs on multiphasic multidetector CT: association with clinical and histopathologic features. Eur Radiol 2016; 26 (03) 646-655
- 11 Kim T, Murakami T, Takamura M. et al. Pancreatic mass due to chronic pancreatitis: correlation of CT and MR imaging features with pathologic findings. AJR Am J Roentgenol 2001; 177 (02) 367-371
- 12 Choueiri NE, Balci NC, Alkaade S, Burton FR. Advanced imaging of chronic pancreatitis. Curr Gastroenterol Rep 2010; 12 (02) 114-120
- 13 Eloubeidi MA, Luz LP, Tamhane A, Khan M, Buxbaum JL. Ratio of pancreatic duct caliber to width of pancreatic gland by endosonography is predictive of pancreatic cancer. Pancreas 2013; 42 (04) 670-679
- 14 Yadav AK, Sharma R, Kandasamy D. et al. Perfusion CT: can it resolve the pancreatic carcinoma versus mass forming chronic pancreatitis conundrum?. Pancreatology 2016; 16 (06) 979-987
- 15 Yin Q, Zou X, Zai X. et al. Pancreatic ductal adenocarcinoma and chronic mass-forming pancreatitis: differentiation with dual-energy MDCT in spectral imaging mode. Eur J Radiol 2015; 84 (12) 2470-2476
- 16 Kim SW, Kim SH, Lee DH. et al. Isolated main pancreatic duct dilatation: CT differentiation between benign and malignant causes. AJR Am J Roentgenol 2017; 209 (05) 1046-1055
- 17 Ren S, Chen X, Cui W. et al. Differentiation of chronic mass-forming pancreatitis from pancreatic ductal adenocarcinoma using contrast-enhanced computed tomography. Cancer Manag Res 2019; 11: 7857-7866
- 18 Ruan Z, Jiao J, Min D. et al. Multi-modality imaging features distinguish pancreatic carcinoma from mass-forming chronic pancreatitis of the pancreatic head. Oncol Lett 2018; 15 (06) 9735-9744
- 19 Karasawa E, Goldberg HI, Moss AA, Federle MP, London SS. CT pancreatogram in carcinoma of the pancreas and chronic pancreatitis. Radiology 1983; 148 (02) 489-493
- 20 Gangi S, Fletcher JG, Nathan MA. et al. Time interval between abnormalities seen on CT and the clinical diagnosis of pancreatic cancer: retrospective review of CT scans obtained before diagnosis. AJR Am J Roentgenol 2004; 182 (04) 897-903
- 21 Bedi MMS, Gandhi MD, Jacob G, Lekha V, Venugopal A, Ramesh H. CA 19-9 to differentiate benign and malignant masses in chronic pancreatitis: is there any benefit?. Indian J Gastroenterol 2009; 28 (01) 24-27
- 22 Nouts A, Lévy P, Voitot H, Bernades P. Diagnostic value of serum Ca 19-9 antigen in chronic pancreatitis and pancreatic adenocarcinoma. Gastroenterol Clin Biol 1998; 22 (02) 152-159
- 23 Lee ES, Lee JM. Imaging diagnosis of pancreatic cancer: a state-of-the-art review. World J Gastroenterol 2014; 20 (24) 7864-7877
- 24 Busireddy KK, AlObaidy M, Ramalho M. et al. Pancreatitis-imaging approach. World J Gastrointest Pathophysiol 2014; 5 (03) 252-270
- 25 Johnson PT, Outwater EK. Pancreatic carcinoma versus chronic pancreatitis: dynamic MR imaging. Radiology 1999; 212 (01) 213-218
- 26 Momtahen AJ, Balci NC, Alkaade S, Akduman EI, Burton FR. Focal pancreatitis mimicking pancreatic mass: magnetic resonance imaging (MRI)/magnetic resonance cholangiopancreatography (MRCP) findings including diffusion-weighted MRI. Acta Radiol 2008; 49 (05) 490-497
Address for correspondence
Publication History
Article published online:
18 September 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Devière J, Baron TH, Kozarek RA. Chronic pancreatitis: stones and strictures. In: Baron TH, Kozarek TA, Carr-Locke DL. eds. ERCP. 3rd ed.. Philadelphia, PA: Elsevier Inc.; 2019: 516-524.e2
- 2 Raimondi S, Lowenfels AB, Morselli-Labate AM, Maisonneuve P, Pezzilli R. Pancreatic cancer in chronic pancreatitis; aetiology, incidence, and early detection. Best Pract Res Clin Gastroenterol 2010; 24 (03) 349-358
- 3 Lowenfels AB, Maisonneuve P, Cavallini G. et al; International Pancreatitis Study Group. Pancreatitis and the risk of pancreatic cancer. N Engl J Med 1993; 328 (20) 1433-1437
- 4 Schima W, Böhm G, Rösch CS, Klaus A, Függer R, Kopf H. Mass-forming pancreatitis versus pancreatic ductal adenocarcinoma: CT and MR imaging for differentiation. Cancer Imaging 2020; 20 (01) 52
- 5 Zhang T-T, Wang L, Liu HH. et al. Differentiation of pancreatic carcinoma and mass-forming focal pancreatitis: qualitative and quantitative assessment by dynamic contrast-enhanced MRI combined with diffusion-weighted imaging. Oncotarget 2017; 8 (01) 1744-1759
- 6 Liao Q, Zhao YP, Wu WW, Li BL, Li JY. Diagnosis and treatment of chronic pancreatitis. Hepatobiliary Pancreat Dis Int 2003; 2 (03) 445-448
- 7 Yamada Y, Mori H, Matsumoto S, Kiyosue H, Hori Y, Hongo N. Pancreatic adenocarcinoma versus chronic pancreatitis: differentiation with triple-phase helical CT. Abdom Imaging 2010; 35 (02) 163-171
- 8 Frampas E, Morla O, Regenet N, Eugène T, Dupas B, Meurette G. A solid pancreatic mass: tumour or inflammation?. Diagn Interv Imaging 2013; 94 (7–8): 741-755
- 9 Freeny PC, Marks WM, Ryan JA, Traverso LW. Pancreatic ductal adenocarcinoma: diagnosis and staging with dynamic CT. Radiology 1988; Jan; 166 (01) 125-133
- 10 Tamada T, Ito K, Kanomata N. et al. Pancreatic adenocarcinomas without secondary signs on multiphasic multidetector CT: association with clinical and histopathologic features. Eur Radiol 2016; 26 (03) 646-655
- 11 Kim T, Murakami T, Takamura M. et al. Pancreatic mass due to chronic pancreatitis: correlation of CT and MR imaging features with pathologic findings. AJR Am J Roentgenol 2001; 177 (02) 367-371
- 12 Choueiri NE, Balci NC, Alkaade S, Burton FR. Advanced imaging of chronic pancreatitis. Curr Gastroenterol Rep 2010; 12 (02) 114-120
- 13 Eloubeidi MA, Luz LP, Tamhane A, Khan M, Buxbaum JL. Ratio of pancreatic duct caliber to width of pancreatic gland by endosonography is predictive of pancreatic cancer. Pancreas 2013; 42 (04) 670-679
- 14 Yadav AK, Sharma R, Kandasamy D. et al. Perfusion CT: can it resolve the pancreatic carcinoma versus mass forming chronic pancreatitis conundrum?. Pancreatology 2016; 16 (06) 979-987
- 15 Yin Q, Zou X, Zai X. et al. Pancreatic ductal adenocarcinoma and chronic mass-forming pancreatitis: differentiation with dual-energy MDCT in spectral imaging mode. Eur J Radiol 2015; 84 (12) 2470-2476
- 16 Kim SW, Kim SH, Lee DH. et al. Isolated main pancreatic duct dilatation: CT differentiation between benign and malignant causes. AJR Am J Roentgenol 2017; 209 (05) 1046-1055
- 17 Ren S, Chen X, Cui W. et al. Differentiation of chronic mass-forming pancreatitis from pancreatic ductal adenocarcinoma using contrast-enhanced computed tomography. Cancer Manag Res 2019; 11: 7857-7866
- 18 Ruan Z, Jiao J, Min D. et al. Multi-modality imaging features distinguish pancreatic carcinoma from mass-forming chronic pancreatitis of the pancreatic head. Oncol Lett 2018; 15 (06) 9735-9744
- 19 Karasawa E, Goldberg HI, Moss AA, Federle MP, London SS. CT pancreatogram in carcinoma of the pancreas and chronic pancreatitis. Radiology 1983; 148 (02) 489-493
- 20 Gangi S, Fletcher JG, Nathan MA. et al. Time interval between abnormalities seen on CT and the clinical diagnosis of pancreatic cancer: retrospective review of CT scans obtained before diagnosis. AJR Am J Roentgenol 2004; 182 (04) 897-903
- 21 Bedi MMS, Gandhi MD, Jacob G, Lekha V, Venugopal A, Ramesh H. CA 19-9 to differentiate benign and malignant masses in chronic pancreatitis: is there any benefit?. Indian J Gastroenterol 2009; 28 (01) 24-27
- 22 Nouts A, Lévy P, Voitot H, Bernades P. Diagnostic value of serum Ca 19-9 antigen in chronic pancreatitis and pancreatic adenocarcinoma. Gastroenterol Clin Biol 1998; 22 (02) 152-159
- 23 Lee ES, Lee JM. Imaging diagnosis of pancreatic cancer: a state-of-the-art review. World J Gastroenterol 2014; 20 (24) 7864-7877
- 24 Busireddy KK, AlObaidy M, Ramalho M. et al. Pancreatitis-imaging approach. World J Gastrointest Pathophysiol 2014; 5 (03) 252-270
- 25 Johnson PT, Outwater EK. Pancreatic carcinoma versus chronic pancreatitis: dynamic MR imaging. Radiology 1999; 212 (01) 213-218
- 26 Momtahen AJ, Balci NC, Alkaade S, Akduman EI, Burton FR. Focal pancreatitis mimicking pancreatic mass: magnetic resonance imaging (MRI)/magnetic resonance cholangiopancreatography (MRCP) findings including diffusion-weighted MRI. Acta Radiol 2008; 49 (05) 490-497