
Subscribe to RSS
DOI: 10.1055/s-0043-1771515
Lipofilling—A Regenerative Alternate for Remodeling Burn Scars: A Clinico-Immunohistopathological Study


- Abstract
- Introduction
- Materials and Methods
- Results
- Histopathological and Immunohistochemical Markers Analysis
- Discussion
- Conclusion
- Highlights
- References
Abstract
Introduction Any injury involving the dermis will lead to scarring. Scar tissue can cause functional limitations, cosmetic impairments, pain, and itch. Adipose-derived stem cells have also been shown to play a role in scar modulation. This study evaluates changes in lipofilled scar over the period of time and compares it with non-lipofilled scar tissue.
Materials and Methods A prospective case–control study with intraindividual follow-up was performed on 30 adult patients with post-burn scars from November 2016 to May 2019. Clinical, histopathological, and immunohistochemical parameters were assessed among the case and control regions of the scar.
Results Mean age of the study population was 30.6 years. The duration of the scar included in this study ranged from 1 to 28 years, with a mean duration of 5.91 years. There was a significant reduction in pain, itch, stiffness, and an increase in the pliability of the scar, and a substantial improvement in the modified Vancouver Scar Score in the lipofilled group. In histopathological analysis, the case group showed organized parallel collagen fibers, a significant reduction in melanocytes, improvement in vascularity, and a significantly increased amount of collagen fibers at the reticular dermis. Immunohistochemical analysis indicated new cell synthesis in the scar tissue and reduced melanocytes.
Conclusion The remodeling effect of adipocyte-derived stem cells is long-lasting, and there is a gradual improvement in most of the parameters. Lipofilling has regenerative capacity, which leads to the improved overall appearance of scar and improvement at the cellular level.
Introduction
Any injury involving the dermis will lead to scarring. Burn injury involving the dermis leads to scars involving large areas. Scar tissue can cause functional limitations, cosmetic impairments, pain, and itch. It may also cause psychosocial and behavioral problems, mainly when it is located in exposed areas.[1] In the contemporary era, there is a significant improvement in survival of patients suffering from burn injuries. With ever-increasing patient survival more substantial number of burns, patients are presenting for secondary reconstruction to enhance the cosmetic appearance and to improve the function of the scarred, contracted area with the aim of bettering the overall quality of life.[2] Levine et al concluded that patients with facial scars report higher levels of depression and anxiety, and they feel dissatisfied with their body image.[3] Scars can also induce chronic pain, which may develop after acute pain, a symptom of normal wound healing. There is no standard treatment for scar, and a multimodal approach is recommended, which includes corticosteroids, silicone gels/sheets, pressure garments, emollient agents, and massages. To date, no gold standard exists for the treatment of scar tissue. Treatments are primarily based on the individual experience of clinicians, with varying degrees of success. Neuber enlightened a new approach to managing these scars by using autologous fat for scar remodeling. This technique was further refined and standardized by Colemann.[4] Adipose derived stem cells have also been shown to play a role in skin regeneration by forming tissue consisting of hypodermis, dermis, and epidermis. It is this regenerative capacity that is of particular interest in burn scar therapy. This study evaluates changes in lipofilled scars over a period of time and compares them with non-lipofilled scar tissue.
Materials and Methods
Study Design and Patients
A prospective case–control study with intraindividual follow-up was performed in 30 adult patients with post-burn scars from November 2016 to May 2019. Scar more than 20 cm squares in patients between 18 and 55 years were included in this study. They were post-burn scars that had healed by about a month from the burn injury, as elicited from the patient's history. Scars were divided into two homogenous parts. In the first half of the scar area, lipofilling was performed through subscar and intrascar infiltration; the second half of the scar area was the control one. The regional medical ethics committee approved the study protocol. As per the Declaration of Helsinki, written informed consent was obtained from all patients.
Scar Evaluation
Clinical parameters were evaluated at 6-month intervals, 1 day before first sitting of lipofilling, 6 months later at second sitting of liopfilling, and at the end of 1 year.
Photographs were taken at the same focal length and exposure. The firmness of the scar evaluated with a Shore type A durometer. The measurements of each area were taken perpendicularly to the plane of the scar for 10 seconds after leaning the instrument to make the reading accurate. Baseline durometer reading was taken as the average of 10 readings at different areas of the scar and noted in the proforma by a single investigator who was not a part of the study group.
In addition, the entire scar area was subjected to the modified Vancouver scar scale (mVSS) and Patient and Observer Scar Assessment Scale (POSAS). Histopathological analysis, in the form of hematoxylin & eosin stain (H&E), Verhoeff elastin stain, and Masson trichrome (MT) stain, was done from biopsies taken before the first lipofilling and at the end of 1 year. Immunohistochemical analysis was done using p-53 and s-100 markers in the same manner. Points are given to different parameters in histology and immunohistochemistry with a maximum score of 18 in each category.
Lipofilling
All the patients were operated under general anesthesia. Two sessions of lipofilling were done at 6 months intervals. We followed the standard Coleman technique for fat grafting. Fat was harvested using 3 mm Luer Lock-mounted cannulas. Manual suction was performed with gradual negative pressure. Compression dressing was applied to the donor site. Harvested fat was transferred in 10 mL syringes and centrifuged at 3,000 rpm for 3 minutes. Once centrifuged, harvested fat will divide into three layers. The upper oily layer was decanted using surgical cotton for 5 minutes. Then the lowermost layer was discarded, and the middle layer was transferred. Lipofilling was done at a subscar level using an 18G sharp needle and by a retrograde method in small pockets of 0.5 mL. Many radiating passages are made to distribute fat in different directions to form a lattice pattern. Approximately 2.5 mL of fat grafted for an area of 6.45 cm2 of scar surface. Contour irregularities are minimized using digital pressure immediately after placement.
A small biopsy was taken at the preplanned site, and the biopsy site closed with nylon 5-0 suture and a noncompressive dressing applied. Both groups had scar massages and application of silicon sheets and pressure garments as per departmental protocol.
Statistical Analysis
All the data were entered in an Excel spreadsheet (Microsoft Corp. 2013). All the data evaluated using SPSS version 25 (IBM Corp., Armonk, New York, United States). The statistical significance of quantitative variables between the two groups was determined by the unpaired t-test/nonparametric Mann–Whitney U test. The statistical significance of qualitative variables between the two groups was determined by the chi-squared test/Fisher's exact test. In both cases, the level of statistical significance was taken as a p-value less than 0.05.
Results
The mean age of the study population was 30.6 years. The maximum number of patients was from the 18- to 25-year age group (60%). Out of 30 patients, 17 were female patients. The duration of scars included in this study ranged from 1 to 28 years, with a mean duration of 5.91 years. The thigh area was our donor area of choice, followed by the abdomen. Scars ranging from 28 cm2 to 143 cm2 in size was included in the study. The mean amount of fat injected was 14.85 mL ([Table 1]; [Figs. 1] and [2]).


Durometer Reading
The durometer reading in the lipofilled region showed significant changes as early as 6 months from first sitting, and the reading improves further as time passes over the first year. In control regions, the durometer reading changes were appreciable only at the end of the first year, and the 6 months readings showed no improvement ([Graph 1]).
Assessment of Scar-by-Scar Assessment Scales
Modified Vancouver Scar Scale
In lipofilled areas, the mean score was 10.33, 9.73, and 8.37 at baseline, 6-month, and 1-year intervals. There was a significant improvement in mVSS scores as early as the initial 6 months and improved further over the first year. In control areas, the mean score was 10.66, 10.33, and 9.33 at baseline, 6-month, and 1-year intervals. The improvement was noticeable only at the end of the first year in control areas ([Graph 2]).

POSAS Scale
In lipofilled areas, improvement in all the parameters of the patient scale remains significant except for the thickness and surface area. Maximum improvement was noted in pliability relief, vascularity, and pigmentation. Most of the patients were able to appreciate these changes in the lipofilled areas as early as 6 months post-treatment. Patients did not appreciate the reduction in the thickness of the scar. In the control area, there was no improvement in any parameters at the end of 6 months. But there was an improvement in vascularity and pigmentation, at the end of 1 year ([Table 2]).
Abbreviations: POSAS, Patient and Observer Scar Assessment Scale; SD, standard deviation.
Histopathological and Immunohistochemical Markers Analysis
([Table 3], [Figs. 3],[4],[5],[6],[7], [Graphs 1],[2] [3] [4] [5])
Abbreviation: SEM, standard error of mean.








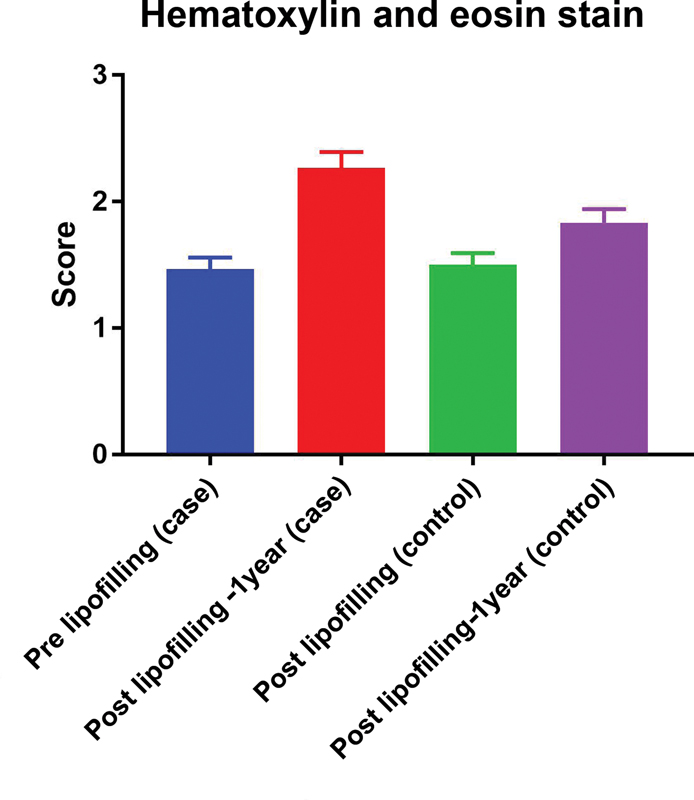
In H&E staining, after two sittings of lipofilling, there was a significant reduction in melanocytes. Collagen fibers that were irregular initially became parallel to the epidermis and finer. Improvement in collagen fibers was significant. In Verhoeff elastin stain, preoperative results show that 60% of cases have minimal elastin fibers in scar tissue, whereas 40% show a focal presence of elastin fibers. At the end of 1 year, in the lipofilled area, there is a significant improvement in elastin fibers. With respect to MT stain, preoperative results show 43.3% of scars had minimal and 56.6% of scars had focal collagen at the dermoepidermal junction. After 1 year of lipofilling, 20 out of 30 scars, the lipofilled regions showed significant improvement in collagen synthesis p-53 suggests the level of cellular activity in any tissue. In pre-lipofilling status, the mean p-53 score was 13.3, which improved significantly to 35.93 after 1 year of lipofilling s-100 satins the mealnocytes. Pre-treatment level of the mean s-100 score was 102, which reduced to 66.4 after 1 year of treatment in the lipofilled region. An intergroup analysis of the parameters was done among the lipofilled and non-lipofilled region parameters using Tukey's multiple variable comparison test (H&E stain, Verhoff stain, MT stain, p-53 and s-100). The comparison in the lipofilled regions pre- and post-intervention showed significant improvement in all the parameters analyzed. In the control regions, pre- and post-treatment analysis showed statistically significant improvement only in p-53 and s-100 scores. In the post-treatment analysis of case and control regions, the mean difference in all the parameters was statistically significant. Overall, the improvement in the parameters studied was much better in the lipofilled region when compared to the non-lipofilled areas.
Discussion
Management of burn scars remains a challenge to date for treating surgeons as they involve large areas and have a tendency for hypertrophy and hyperpigmentations. For the treatment of scars, clinicians and researchers have described a variety of protocols. Yet, limited data about the effectiveness are derived from well-designed, prospective, randomized, controlled clinical trials. To date, no gold standard exists for the treatment of scar tissue. Treatments are mainly based on the individual experience of clinicians, with varying degrees of success.
This study aimed to understand the remodeling effect of lipofilling in post-burn scars in patients of Indian origin. This study was conducted in a single center over a period of 30 months. A total of 30 scars in burned patients were included in this study and followed up for 12 months. The mVSS shows significant improvement in the score as early as 6 months postoperative follow-up; this trend of improvement is also present from 6 to 12 months of postoperative time (p < 0.05). When we compare preoperative parameters with 1-year postoperative parameters among the POSAS, we found that improvement in vascularity, pigmentation, relief, and pliability shows significant improvement ([Table 2]).
Reduction in the thickness of the scar was noted but remains statistically insignificant. No reduction in surface area was noted at any time interval. Klinger et al reported significant improvement in all the parameters of the observer scale over 3 months.[5] Pallua et al reported significant improvement in pigmentation and pliability. Improvement was also noted in the remaining parameters but remained statistically nonsignificant.[6] Caviggioli et al. reported significant improvement in all the parameters over 3 months.[7]
Over 1 year, there has been a significant improvement in collagen fiber arrangement and a reduction in melanocyte staining on H&E staining. Verhoeff stain shows a significant increase in elastin fibers in liopfilled areas after a 1-year interval. MT shows the laying of new collagen fibers at the dermoepidermal junction and reticular dermis. A significant improvement in the p-53 value suggests increased tissue regeneration in a quiescent scar. s-100 values reduce significantly over the period of 1 year, suggesting a reduction in the melanocytes in the scar. This finding also correlates with a reduction in melanocytes in H&E stains. A study by Bruno et al also shows improved vascularization of dermal papillae, better organization of collagen, a significant decrease in s-100-positive cells and Langerin-positive cells, and marked improvement in p-53 and Ki-67 expression.[8] Klinger et al show epithelial hyperplasia and neoangiogenesis in lipofilled scar tissue.[5] In their study, Brongo et al also reported histologic findings, which showed new collagen deposition, neoangiogenesis, and dermal hyperplasia in the context of new tissue, demonstrating tissue regeneration.[9] Lipofilling has efficacy in remodeling the scar, and the effect can be seen clinically as early as the initial 6 months. The remodeling effect of adipocyte-derived stem cells is long-lasting, and there is gradual improvement in most of the parameters. However, further study with a large sample size and long-term follow-up is required to confirm the remodeling capacity of lipofilling.
Conclusion
Lipofilling is an emerging therapy that provides a new armamentarium to deal with burn scars. There is a significant reduction in pain, itch, and stiffness, an increase in the pliability of scar, and a significant improvement in mVSS score seen over 1 year. H&E staining shows organized parallel collagen fibers, a significant reduction in melanocytes, and an improvement in vascularity. Elastin fibers show a generalized and more organized distribution on the Verhoeff stain. MT stain shows a significantly increased collagen fiber at the reticular dermis. Immunohistochemical marker p-53 increases significantly, which indicates new cell synthesis in the scar tissue. The s-100 score reduces significantly over the lipofilling period, indicating a melanocyte reduction. We conclude that lipofilling has a regenerative capacity that leads to improvement in the overall appearance of scar and improvement at the cellular level over the follow-up period.
Highlights
-
This study evaluates changes in lipofilled burn scar over a period of time and compares them with non-lipofilled burn scar tissue.
-
Significant reduction in pain, itch, stiffness, and increase in the pliability of burn scar and significant improvement in modified mVSS in lipofilled group.
-
Immunohistochemical analysis indicated new cell synthesis in the burn scar tissue and reduced melanocytes.
-
Lipofilling has regenerative capacity, leading to improved overall appearance of burn scar and improvement at the cellular level.
Conflict of Interest
None declared.
Authors' Contribution
B.J., D.K. and C.A. were involved in conceptualization, designing, and drafting of the manuscript. V.M. and B.J. helped in drafting of the manuscript, and collection and analysis of data. All authors read and approved the final manuscript.
-
References
- 1 Niessen FB, Spauwen PH, Schalkwijk J, Kon M. On the nature of hypertrophic scars and keloids: a review. Plast Reconstr Surg 1999; 104 (05) 1435-1458
- 2 Levine E, Degutis L, Pruzinsky T, Shin J, Persing JA. Quality of life and facial trauma: psychological and body image effects. Ann Plast Surg 2005; 54 (05) 502-510
- 3 Fearmonti RM, Bond JE, Erdmann D, Levin LS, Pizzo SV, Levinson H. The modified Patient and Observer Scar Assessment Scale: a novel approach to defining pathologic and nonpathologic scarring. Plast Reconstr Surg 2011; 127 (01) 242-247
- 4 Neuber G. Fat transplantation. Verh Dtsch Ges Chir 1893; 22: 66
- 5 Klinger M, Marazzi M, Vigo D, Torre M. Fat injection for cases of severe burn outcomes: a new perspective of scar remodeling and reduction. Aesthetic Plast Surg 2008; 32 (03) 465-469
- 6 Pallua N, Baroncini A, Alharbi Z, Stromps JP. Improvement of facial scar appearance and microcirculation by autologous lipofilling. J Plast Reconstr Aesthet Surg 2014; 67 (08) 1033-1037
- 7 Caviggioli F, Maione L, Forcellini D, Klinger F, Klinger M. Autologous fat graft in postmastectomy pain syndrome. Plast Reconstr Surg 2011; 128 (02) 349-352
- 8 Bruno A, Delli Santi G, Fasciani L, Cempanari M, Palombo M, Palombo P. Burn scar lipofilling: immunohistochemical and clinical outcomes. J Craniofac Surg 2013; 24 (05) 1806-1814
- 9 Brongo S, Nicoletti GF, La Padula S, Mele CM, D'Andrea F. Use of lipofilling for the treatment of severe burn outcomes. Plast Reconstr Surg 2012; 130 (02) 374e-376e
Address for correspondence
Publication History
Article published online:
16 August 2023
© 2023. Association of Plastic Surgeons of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Niessen FB, Spauwen PH, Schalkwijk J, Kon M. On the nature of hypertrophic scars and keloids: a review. Plast Reconstr Surg 1999; 104 (05) 1435-1458
- 2 Levine E, Degutis L, Pruzinsky T, Shin J, Persing JA. Quality of life and facial trauma: psychological and body image effects. Ann Plast Surg 2005; 54 (05) 502-510
- 3 Fearmonti RM, Bond JE, Erdmann D, Levin LS, Pizzo SV, Levinson H. The modified Patient and Observer Scar Assessment Scale: a novel approach to defining pathologic and nonpathologic scarring. Plast Reconstr Surg 2011; 127 (01) 242-247
- 4 Neuber G. Fat transplantation. Verh Dtsch Ges Chir 1893; 22: 66
- 5 Klinger M, Marazzi M, Vigo D, Torre M. Fat injection for cases of severe burn outcomes: a new perspective of scar remodeling and reduction. Aesthetic Plast Surg 2008; 32 (03) 465-469
- 6 Pallua N, Baroncini A, Alharbi Z, Stromps JP. Improvement of facial scar appearance and microcirculation by autologous lipofilling. J Plast Reconstr Aesthet Surg 2014; 67 (08) 1033-1037
- 7 Caviggioli F, Maione L, Forcellini D, Klinger F, Klinger M. Autologous fat graft in postmastectomy pain syndrome. Plast Reconstr Surg 2011; 128 (02) 349-352
- 8 Bruno A, Delli Santi G, Fasciani L, Cempanari M, Palombo M, Palombo P. Burn scar lipofilling: immunohistochemical and clinical outcomes. J Craniofac Surg 2013; 24 (05) 1806-1814
- 9 Brongo S, Nicoletti GF, La Padula S, Mele CM, D'Andrea F. Use of lipofilling for the treatment of severe burn outcomes. Plast Reconstr Surg 2012; 130 (02) 374e-376e