

Subscribe to RSS
DOI: 10.1055/s-0043-1770153
A Pilot Study to Evaluate a Residual Inhibition Technique in Hearing Aids for Suppression of Tinnitus
Authors

Abstract
Tinnitus acoustic therapy is defined as any use of sound where the intent is to alter the tinnitus perception and/or the reactions to tinnitus in a clinically beneficial way. The parameters of sound that may cause beneficial effects, however, are currently only theorized with limited data supporting their effectiveness. Residual inhibition is the temporary suppression or elimination of tinnitus that is usually observed following appropriate auditory stimulation. Our pilot study investigated the effects of a therapeutic acoustic stimulus that was individually customized to maximize residual inhibition of tinnitus and extend its duration to determine if there could be a sustained suppression of the tinnitus signal (i.e., reduced tinnitus loudness) and a reduction in the psychological and emotional reactions to tinnitus. This pilot study had two objectives: (1) to evaluate the feasibility of residual inhibition technique therapy through daily use of hearing aids and (2) to determine its effects by measuring reactionary changes in tinnitus with the Tinnitus Functional Index (TFI) and perceptual changes in tinnitus loudness. A total of 20 adults (14 males, 6 females; mean age: 58 years, SD = 12.88) with chronic tinnitus were enrolled in a four-visit study that consisted of the following: (1) baseline visit and initiation of the intervention period, (2) a 1-month postintervention visit, (3) 2-month postintervention visit and initiation of a wash-out period, and (4) a 3-month visit to assess the wash-out period and any lasting effects of the intervention. The intervention consisted of fitting bilateral hearing aids and creating an individualized residual inhibition stimulus that was streamed via Bluetooth from a smartphone application to the hearing aids. The participants were instructed to wear the hearing aids and stream the residual inhibition stimulus all waking hours for the 2-month intervention period. During the wash-out period, the participants were instructed to use the hearing aids for amplification, but the residual inhibition stimulus was discontinued. At all visits, the participants completed the TFI, study-specific self-report measures to document perceptions of tinnitus, a psychoacoustic test battery consisting of tinnitus loudness and pitch matching, and a residual inhibition test battery consisting of minimum masking and minimum residual inhibition levels. At the end of the trial, participants were interviewed about the study experience and acceptability of the residual inhibition treatment technique. Repeated measures analyses of variance (ANOVA) were conducted on the two main outcomes (TFI total score and tinnitus loudness) across all four visits. The results showed a significant main effect of visit on the TFI total score (p < 0.0001). Specifically, the results indicated a significant reduction in TFI total scores from baseline to the 1-month post-intervention period, which remained stable across the 2-month post-intervention period and the wash-out period. The ANOVA results did not show a significant change in tinnitus loudness as a function of visit (p = 0.480). The majority of the participants reported a positive experience with the study intervention at their exit interview. This pilot study demonstrated that residual inhibition as a sound therapy for tinnitus, specifically through the daily use of hearing aids, was feasible and acceptable to individuals suffering from chronic tinnitus. In addition, participants showed improvement in reactions to tinnitus as demonstrated by sustained reduction in TFI scores on average over the course of the treatment period. Achieving residual inhibition may also provide patients a feeling of control over their tinnitus, and this may have a synergistic effect in reducing the psychological and emotional distress associated with tinnitus. There was no significant reduction in long-term tinnitus loudness resulting from the residual inhibition treatment; however, the current pilot study may not have had sufficient power to detect such a change. The combination of tinnitus suppression and improved psychosocial/emotional reactions to tinnitus may result in a better quality of life in both the short and long term. A larger-scale study is needed to determine the validity of using residual inhibition as a clinical therapy option and to ascertain any effects on both perception and reactions to tinnitus.
Tinnitus is the persistent perception of sound when there is no external source (Jastreboff 1990). In the United States, it has been estimated that 50 million adults experience chronic tinnitus, and of that population, 12 million seek some form of intervention (Tunkel et al. 2014). A variety of etiologies are associated with tinnitus, which can be categorized as primary or secondary.
Primary tinnitus is idiopathic in nature and may or may not be associated with sensorineural hearing loss (Tunkel et al. 2014). Primary tinnitus—by far the most common type of tinnitus—is typically evaluated and managed by audiologists. Tinnitus that is associated with an identifiable underlying cause or organic condition, other than sensorineural hearing loss, is categorized as secondary tinnitus. Secondary tinnitus is associated with auditory system disorders (e.g., Meniere's disease, otosclerosis, Eustachian tube dysfunction, or cerumen impaction) or non-auditory system disorders (e.g., intracranial hypertension, myoclonus, or vascular anomalies causing pulsatile tinnitus). In the current study, we targeted adults with primary tinnitus.
Although a cure for primary tinnitus does not exist, there are several therapies available. Examples include cognitive behavioral therapy (CBT) and sound therapy (Dobie 2004; Fuller et al. 2017; Henry & Quinn 2020; Tunkel et al. 2014). Sound therapy has been a primary management option for tinnitus sufferers, as it can mitigate the negative effects of tinnitus by providing background noise, masking, and relaxation (Hillecke et al. 2005). Sound therapy is used to manage tinnitus in two ways: (1) to reduce emotional and functional effects of tinnitus (during and beyond the stimulus exposure) and (2) to reduce or eliminate the actual perception of tinnitus (during the stimulus exposure). Henry and Quinn (2020) provide an in-depth review on the differences between tinnitus reactions and tinnitus perception.
Sound therapy for primary tinnitus often involves some type of ear-level device, including hearing aids (with a built-in sound generator and/or streaming capability), and dedicated sound generators. Sounds used to reduce reactions to tinnitus include background sound, masking, soothing sound, interesting sound, and/or music therapy (Henry & Quinn 2020). In contrast, sounds used to target the tinnitus percept (i.e., the tinnitus sound itself) focus on targeting the underlying neural mechanisms. Notched-sound therapy, matched-sound therapy, and neural desynchronization are all types of sound therapies that target underlying theoretical neural mechanisms (Henry & Quinn 2020). The present study applies one such perceptual sound therapy known as residual inhibition.
Residual inhibition is the temporary suppression or elimination of tinnitus that usually occurs following the appropriate auditory stimulation. Traditionally, residual inhibition is a form of clinical measurement performed during an audiological tinnitus evaluation to identify whether an individual could benefit from sound therapies (Vernon & Meikle 2000; Evered & Lawrenson 1981). The mechanism behind residual inhibition has been studied for decades, ultimately resulting in inconclusive evidence regarding its underlying mechanisms (Vernon & Meikle 2003; Roberts et al. 2006). In animal models, it is relatively agreed upon that tinnitus perception is associated with elevated neuronal spontaneous firing within the central auditory cortex (Eggermont 2017; Aurebach et al. 2014; Galazyuk et al. 2017). Galazyuk et al. (2017) found in an animal model that forward suppression of this spontaneous firing triggered by sound could be an underlying mechanism of the residual inhibition effect due to its similar psychoacoustic properties of residual inhibition in humans.
Residual inhibition has been shown to be an effective method of tinnitus suppression in humans in several studies (Feldmann 1971; Reavis et al. 2012; Roberts et al. 2008; Terry et al. 1983; Vernon & Meikle 2003). These types of studies have developed through approaches to both evaluate and characterize an individual's residual inhibition experience. For example, Roberts et al. (2008) created a detailed test battery to include (1) localization of tinnitus, (2) adjustments of sound intensity, (3) bandwidth selection of tinnitus, (4) temporal properties of tinnitus, (5) tinnitus loudness rating, (6) tinnitus loudness matching, (7) tinnitus likeness rating, (8) sound thresholds at 1,000 Hz, (9) brief residual inhibition test, and (10) a full residual inhibition test to measure depth, duration, and chronicity of tinnitus. Although these types of measures rely on the individual's ability to understand and perform the task to obtain meaningful data, they are important for research purposes when studying underlying mechanisms of residual inhibition. A limitation of obtaining these measures is that they are time consuming, and thus less feasible to implement in a clinical setting.
Nonetheless, others have defined a classic audiological method used to assess residual inhibition with patients (Henry & Meikle, 2000). After a series of psychoacoustic measures including minimum and maximum masking levels, residual inhibition duration is estimated after a prolonged acoustic stimulus is presented 30 to 60 seconds at an intensity of +10 dB of minimum masking level (MML), and then stopped (Henry & Meikle, 2000; Fournier et al. 2018). Though this method makes assessment of residual inhibition more clinically feasible, it is not routinely performed during a tinnitus evaluation. Thus, others have considered alternative approaches to efficiently measure residual inhibition within a clinical setting where time constraints are a common problem when performing full tinnitus evaluations.
Fournier et al. (2018) proposed a new method for assessing masking and residual inhibition, where instead of presenting a continuous acoustic stimulus for 30 to 60 seconds, they presented an acoustic sequence made of 2- to 3-second pulsed stimuli with 1-second silent intervals over 30 to 60 seconds. First, the MML was measured by raising the pulsed stimulus intensity until the tinnitus was inaudible during the stimulus presentation. Second, the level of the stimulus was further increased until the tinnitus was suppressed during the silent interval between the acoustic pulses. This level was called the minimum residual inhibition level (MRIL).
Their novel laboratory-based method using the acoustic sequence made of pulsed stimuli produced residual inhibition in 87% of the participants tested in their study.
The present pilot study builds on the work of Fournier et al. (2018) by evaluating the new method as a measurement technique and as a tinnitus sound therapy that can be administered as an immersive therapy via hearing aids. Specifically, the main purpose of this pilot study was to examine if the MRIL stimulus developed by Fournier and colleagues, when administered continuously through hearing aids, is able to reduce the reactionary effects of tinnitus and to suppress the perception of tinnitus. In addition, we sought to determine if this approach was feasible and acceptable to individuals suffering from chronic tinnitus.
Materials and Methods
Participants
All study procedures were approved by the Veterans Affairs (VA) Portland Health Care System (VAPORHCS) Institutional Review Board (protocol number: 1635437) and all participants provided written informed consent before participation.
Recruitment
Candidates were recruited through multiple sources, which included study fliers posted throughout VAPORHCS and on the VA Rehabilitation Research and Development, National Center for Rehabilitative Auditory Research's (NCRAR) Web site, and an NCRAR repository database that contains the contact information of former participants in various studies who agreed to be contacted about future research projects. Screening was conducted over the telephone using the Tinnitus Screener (TS), a six-item algorithmic instrument developed to categorize a person as having constant, intermittent, occasional, temporary, or no tinnitus, was administered during the telephone screening (Henry et al. 2016a; Henry et al. 2016b).
Inclusion Criteria
To be included in the study, candidates had to be categorized as having constant tinnitus on the TS. Other inclusion criteria included having bilateral tinnitus, age 18 years or older, and demonstrating an understanding of study requirements and protocol timeline. Technological limitations only allowed the study to create Apple Music audio files that could be streamed through an iPhone. As such, participants were required to have an iPhone 5 smartphone or newer with an operating system (iOS) of 10 or later.
Exclusion Criteria
Exclusion criteria included two or more hearing thresholds exceeding 70 dB HL and/or significant conductive hearing loss—defined as an air–bone gap of 15 dB at more than two frequencies in one ear, or an air–bone gap greater than 15 dB at any one frequency (audiometric testing procedures described later), inability to consistently achieve full or partial residual inhibition in the sound booth, suspicion of secondary (somatic) tinnitus, Meniere's disease, or tinnitus potentially related to temporo-mandibular joint disorder or whiplash, or any mental, emotional, or health conditions that would preclude full study participation.
Questionnaires
Questionnaires included (1) the TS, (2) the Tinnitus Functional Index (TFI), and (3) the Tinnitus Follow-up Questionnaire (TFQ)—a study-specific questionnaire to assess participants' posttreatment perceptions. Participants completed an exit interview to assess their acceptability of the residual inhibition therapy and approach.
Tinnitus Screener.
The TS, described earlier, was administered over the telephone to determine eligibility as a paper questionnaire during each study visit to verify the initial categorization, that is, to ensure participants were continuing to experience constant tinnitus. All participants endorsed constant tinnitus at each visit (Henry et al. 2016a; Henry et al. 2016b).
Tinnitus Functional Index.
The TFI is a 25-item questionnaire that captures the impact of tinnitus over the previous week. It contains eight subscales that measure the following domains: intrusiveness, sense of control, cognitive, sleep, auditory, relaxation, quality of life, and emotional. Of the 25 items, all but two use a 0 to 10 response scale, with 0 indicating no problem and 10 indicating the most severe problem. The other two items use a 0 to 100% scale, which quantify tinnitus awareness and tinnitus annoyance, respectively (higher percentages indicating greater difficulty). The TFI total score is calculated by summing all responses, dividing by the number of items, and multiplying by 10—resulting in a 0 to 100 scale of tinnitus functional effects. Higher scores indicate a higher tinnitus burden. Subscale scores are calculated in the same manner (Meikle et al. 2012).
Tinnitus Follow-up Questionnaire.
This questionnaire includes three questions regarding the participant's tinnitus characteristics and effects as well as four items that assess impressions of change in aspects of tinnitus over the course of the study. The TFQ was completed only at Visits 3 and 4. We will focus on the four items that assess impressions of change in tinnitus over the course of the study (see [Supplementary Appendix A] [available in the online version only]).
Exit Interview.
A total of 12 questions were asked of the participants in an exit interview when they completed the study. The questions included their ratings of overall satisfaction of the study, impressions about the therapy, future use of the therapy, and any perception of change in their tinnitus (see [Supplementary Appendix B] [available in the online version only]).
Tinnitus Psychoacoustic Testing
Four tinnitus psychoacoustic tests were administered at each visit, including (1) pitch match (PM), (2) loudness match (LM), (3) MML, and (4) MRIL. Before psychoacoustic testing, participants were asked to identify the ear with the predominant tinnitus. If the tinnitus in one ear was louder, the other ear was chosen as the stimulus ear. There were five total tests to assess consistency, and each trial entailed first recording the PM and then the LM. PM and LM stimuli were generated by and routed through the audiometer (Grason-Stadler AudioStar Pro) and presented through high-frequency headphones (Sennheiser HDA 200), while the participants were seated in a double-walled sound booth (Eckel Noise Control Technologies). General procedures for LM and PM testing were reported in Henry et al. (2004).
Pitch Match.
Participants were instructed that they would hear two pure tones in the stimulus ear. Using the two-alternative forced choice (2AFC) approach, the participant verbally reported whether the first or second tone was closer in pitch to the tinnitus in the non-stimulus ear. Starting at 1,000 Hz, the presented frequencies were differentiated by 1/6th octaves and the tester presented frequency ascension and descension based on the participant's response. PM was established when the participant selected a tone of a given frequency on two consecutive occasions. To confirm the PM frequency, octave-confusion testing was completed whereby a higher frequency and lower frequency octave were presented (when possible) with the PM frequency in the same format as the normal trial. Any change based on octave confusion was noted.
Loudness Match.
The LM was found at the PM frequency. Participants were informed that they were going to hear a tone in the stimulus ear and asked whether the intensity of the tone needed to increase or decrease to match the tinnitus volume in the non-stimulus ear. A bracketing technique was used, similar to the modified Hughson-Westlake method (Carhart & Jerger 1959), but with 2-dB step sizes. The LM response was found to the nearest 1 dB HL.
Residual Inhibition Testing
For both MML and MRIL testing, responses were measured at two narrow band noise frequencies: band of noise one octave wide that is centered around the PM frequency and a band of noise one octave wide that is centered around the midpoint of the slope of the hearing loss on the audiogram. The frequency of the slope of the hearing loss is chosen by visual inspection for each individual patient audiogram. The chosen frequency is most often between the cutoff frequency and the first frequency that reaches a difference threshold of ≥15 dB and equaled the threshold of the cutoff frequency. On some occasions, the tester selected one to two additional frequencies to find the largest MRIL response. All residual inhibition measurements were completed using stimuli presented through a custom MATLAB software (version R2014a8.3), routed through a laboratory desktop computer and sound attenuator (Grace Design M920), and presented through insert earphones (Etymōtic, Model ER-3A).
Minimum Masking Level
Starting at a comfortable loudness level, a pulsed noise stimulus (rise/fall time: 0.5 seconds, duration: 3.0 seconds, silence duration: 0.5 seconds, in dB SPL) was presented binaurally. Using increasing 3-dB steps, the participant was asked to let the tester know when the narrow band noise (one octave wide) was loud enough such that the perception of tinnitus was still present but somewhat masked by the stimulus (partial MML) and when the tinnitus was fully covered by the stimulus (complete MML). Both the partial MML and complete MML were recorded. As described earlier, multiple narrowband noise frequencies were measured to ensure the largest MRIL response was found.
Minimum Residual Inhibition Level
Pulsed narrow band noise, as described earlier, was presented binaurally and participants were asked to focus on the silent intervals in between the pulsed stimuli. They were asked to report any noticeable differences in the tinnitus, in particular any partial or complete inhibition. As with MML testing, intensity of the pulsed narrow bands of noise was increased in 3-dB steps and both partial and complete residual inhibition levels were recorded.
Residual Inhibition Stimulus Selection to Be Incorporated in the Hearing Aid Intervention
The stimulus that produced MRIL at the lowest intensity level was selected for streaming through the hearing aids. If no stimulus produced complete MRIL, the tester selected the lowest intensity signal that still induced partial MRIL. The MRIL stimulus was created as a .wav file through the MATLab software that recorded the MML and MRIL measurements. Intensity level of the stimulus (pulsed narrow bands of noise) was selected based on comfort level of the participant. The .wav file was transferred into the participants' iPhone through CopyTrans Management software, which required the cell phone to be connected to the computer through an Apple charging cable. The stimulus could then be accessed through the Apple Music application like a song track. The hearing aids were paired with the iPhone through Bluetooth to allow for the MRIL stimulus to stream from the Apple Music application.
Procedures
Participants attended four visits over a period of 12 weeks and were compensated $25 per visit. [Fig. 1] displays the study visits and the measurements performed at each visit.

Baseline Visit. Baseline Visit 1 included completion of the TS and TFI questionnaires. A standard audiologic evaluation was completed to ensure that the patient met the study criteria and included an otoscopic examination, tympanometry (Grason-Stadler, Model TympStar), pure-tone air conduction audiometry for octave frequencies of 250 to 16,000 Hz and interoctave frequencies of 3,000 and 6,000 Hz (Grason-Stadler AudioStar Pro), and bone-conduction audiometry for octave frequencies of 500 to 4,000 Hz and the interoctave frequency of 3,000 Hz (RadioEar Bone Transducer), using high-frequency headphones (Sennheiser HDA 200 Headphones).
After the audiologic evaluation, the psychoacoustic and residual inhibition test batteries were performed. Participants then were fitted with the study hearing aids that were donated by GN Resound. Specifically, participants were fitted with Resound Linx Quattro 9 receiver-in-the-ear (RITE) hearing aids, bilaterally, with open-dome coupling.
The following were the general settings for the hearing aids: directional mic mix was set to very low; time constant was syllabic; digital feedback suppression was mild; noise tracker was set as per environment; and wind guard was moderate. All hearing aids were programmed using the “All Around” (listening in quiet) program via first fit and minor fine-tuning adjustments were made for patient comfort. These settings were used for the duration of the trial and the volume control was disabled. The MRIL therapy was initiated at this session, with the custom MRIL stimulus streamed from the participant's iPhone to Resound Linx Quattro 9 hearing aids. Participants were oriented on the use of the device and streaming the MRIL stimulus. They were instructed to wear their hearing aids during waking hours with the MRIL stimulus playing for the entire period of time. This visit took an estimated 3 hours.
Visit 2. Participants returned to the laboratory for Visit 2 one to three weeks after the Baseline Visit. At this visit, the TS and TFI questionnaires were administered and the psychoacoustic test battery was completed. A listening check was performed on the hearing aids and adjustments were made in the hearing aid software for comfort and preference, if applicable, as the goal was for participants to wear the hearing aids all day during waking hours. Although data logging was not recorded, hearing aid data logging was checked to ensure that patients were wearing their devices consistently each day. The MRIL stimulus was also checked by the study audiologist to ensure that the stimulus was streaming appropriately and set to continuous replay. Participants were informed that they needed to continue to listen to their MRIL stimulus continuously until the next visit. This visit took an estimated 2 hours.
Visit 3. This visit occurred 8 weeks after the baseline visit, or 4 weeks after Visit 2. The TS, TFI, and TFQ questionnaires were administered and the psychoacoustic test battery was completed. A listening check was performed on the hearing aids by the audiologist to ensure that the hearing aids were functioning appropriately. No adjustments were made to the hearing aid settings at this visit. At this point, participants had been wearing the study hearing aids and listening to their custom MRIL therapy for 2 months. To determine if there was a residual inhibition effect and if that effect could be maintained without constant stimulation, the MRIL therapy was turned off at this visit and the wash-out period was initiated. Participants were instructed to wear the hearing aids without the MRIL stimulus playing for another month. This visit took an estimated 2 hours.
Visit 4. The final study visit, Visit 4, occurred 12 weeks after baseline, or 4 weeks after Visit 3. The TS, TFI, and TFQ questionnaires were administered and the psychoacoustic test battery was performed. Participants were allowed to keep the study hearing aids. Because the hearing aids had been set for comfort while listening to the MRIL therapy, the hearing aids were re-fit to the participants' individual hearing loss based on National Acoustic Laboratories Non-Linear 2 (NAL-NL2; Keidser et al. 2011) prescriptive targets and adjustments were made for comfort and patient preference if applicable (Audioscan Verifit 1). The exit interview ([Supplementary Appendix B] [available in the online version only]) was performed to determine the participants' perspectives on the usability and feasibility of the MRIL therapy. The interview included questions about their experiences in the study, including their assessment of the MRIL stimulus and hearing aids, and any changes in the perception of their tinnitus. Participants were also given the opportunity to provide feedback on the study. At this time, participants could choose to continue to use their custom MRIL therapy saved on their iPhone or they could discontinue use of the therapy. They were instructed that they could use the therapy at their discretion. This visit took an estimated 2 hours.
Statistical Methods
Descriptive statistics were used to summarize the demographics and clinical characteristics of the sample ([Table 1]). Repeated measures analyses of variance (ANOVA) were conducted on the two main outcome measures: (1) TFI total score and (2) tinnitus loudness across the four visits. Changes in TFI total scores represent change in reactions to tinnitus over time, while changes in measurement of tinnitus loudness represent change in the perception of tinnitus over time. The eight TFI subscales were also analyzed with repeated measures ANOVA as a secondary analysis.
Results
Descriptive Statistics
[Table 1] displays the age, sex, race, and Veteran status of the study participants. A total of 20 participants were enrolled in the study (six females, 14 males; median age: 62.5 years, SD = 12.9, range: 36–78 years). All participants had hearing loss, and the average audiogram for enrolled participants is shown in [Fig. 2]. Of the 20 participants, 15 completed all four study visits. All enrolled participants (n = 20) contributed data to the analyses. Two participants withdrew from the study before completing all visits, one because of time constraints and one because they found the MRIL stimuli annoying.

Three participants were lost to follow-up. The TS was used to determine eligibility but was administered throughout the study at each visit to confirm that the patient had constant tinnitus perception throughout the visits. All available data were included in the analyses. [Fig. 3] shows the study CONSORT (Consolidated Standards of Reporting Trials) flow diagram.

Tinnitus Functional Index (Primary Outcome Measure)
TFI total scores for each of the four study visits are shown in [Fig. 4]. As seen in the figure, the total scale scores appear to decrease between baseline and Visit 2, and then remain fairly stable through Visit 4. The repeated measures ANOVA on TFI total score confirmed the observations in [Fig. 4] and showed a significant main effect of visit (p < 0.0001). There was a significant 10.7 point improvement (reduction) in TFI score between baseline and Visit 2. Change in TFI score after visit 2 was small, though all visits were significantly better than the baseline visit.

[Fig. 5] illustrates the mean scores on each of the eight TFI subscales across the four visits. As seen in the figure, improvement (decrease) in scores is seen on six subscales: Intrusive, Sense of Control, Auditory, Relaxation, Quality of Life, and Emotional. A repeated measures ANOVA ([Table 2]) showed a significant main effect of visit on the above six subscales. These results suggest that the treatment has a significant impact on reactions to tinnitus, improving a participant's feelings toward how they are impacted by their tinnitus perception before treatment compared with after treatment, and this improvement maintained after the wash-out period (between Visits 3 and 4).

|
Repeated measures ANOVA |
||
|---|---|---|
|
TFI subscale |
F-statistic |
p-Value |
|
Intrusive |
3.52 |
0.0218[a] |
|
Sense of control |
4.19 |
0.0103[a] |
|
Cognitive |
2.35 |
0.0837 |
|
Sleep |
2.43 |
0.0766 |
|
Auditory |
3.32 |
0.0273[a] |
|
Relaxation |
15.60 |
<0.0001[a] |
|
Quality of life |
6.82 |
0.0006[a] |
|
Emotional |
3.28 |
0.0287[a] |
Abbreviations: ANOVA, analyses of variance; TFI, Tinnitus Functional Index.
Note: Numerator DF = 3; denominator DF = 48.
a Significant at the α = 0.05 level.
Loudness Match (Secondary Outcome Measure)
LMs were obtained at all visits, and the mean LMs and standard error are presented for the 20 participants in [Fig. 6]. As seen in the figure, the mean LMs are similar across the four visits. A repeated measures ANOVA using LM levels as the within-subjects variable across the four study visits did not show significant differences in LMs among the four visits (p = 0.480). This finding does not support our hypothesis that LM would reduce with MRIL therapy.

Self-Reported Tinnitus Perceptions (Follow-up Questionnaire)
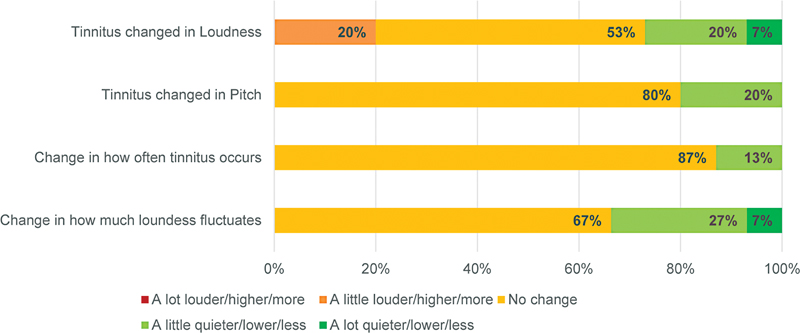
The TFQ was administered at Visits 3 and 4. This questionnaire, though not validated, helped identify participant tinnitus perceptions and reactions pre- and post-intervention. Participant responses for Visit 3 (2-month postintervention with MRIL) can be seen in [Fig. 7] and participant responses for Visit 4 (wash-out period) can be seen in [Fig. 8]. Overall, the majority of participants did not perceive a change in the fluctuation of loudness, frequency of occurrence, pitch, or loudness of their tinnitus. When comparing the questionnaire answers from Visit 3 to Visit 4, the percentage of participants who rated an increase (“a little” or “a lot louder/higher/more”) in loudness, pitch, frequency of occurrence, and fluctuation of loudness of their tinnitus decreased over all four items. Of interest, 27% of participants reported the loudness of their tinnitus fluctuated “a little less” and an additional 7% “a lot less” at Visit 4. Additionally, 20% of participants noted that their tinnitus was “a little quieter” and an additional 7% “a lot quieter” at Visit 4.

Exit Interview: Participant Perspectives
Participants were asked 12 questions about their overall experiences during the study, their tinnitus perception, and feasibility of using the hearing aids with the MRIL therapy. The questions and response scale can be seen in [Supplementary Appendix B] (available in the online version only). Participants expressed positive perceptions about the study, regardless of how much they reported that the therapy helped alleviate their tinnitus. Of the 15 participants who completed an exit interview, 13 rated their overall satisfaction with the therapy at 7 or higher on a 1 to 10 Likert scale where 1 = “extremely dissatisfied” to 10 = “extremely satisfied.” One participant rated satisfaction at 5, and one skipped this question. All 15 participants stated that they intend to keep using the device after the study ended (although one described plans to keep using the hearing aids without the therapy stimulus; others may have also had that intention without stating as such). A total of 93% (14/15) participants indicated that they would recommend the therapy to a friend.
Only six participants (out of 15) reported that their tinnitus had improved during the study. Of the remaining nine participants, six reported that their tinnitus did not change and two reported that it changed for the worse (one participant reported that their tinnitus changed but did not specify how). Although this was not one of the interview questions, five participants reported that they felt better about their tinnitus as a result of the study because they felt they had greater knowledge and/or control over their tinnitus than they did previously. Of those five, three reported that, overall, their tinnitus improved over the course of the study and two reported that it did not.
Participants generally found the hearing aids and streaming application comfortable and easy to use. Of the 15 participants, 13 reported finding them comfortable, and all 15 said they were easy to use, although several participants had minor complaints. The most common complaints were Bluetooth-related issues, such as the stimulus sound disconnecting or not being compatible with their personal devices (eight participants), hearing aid–related issues such as the earpieces falling out (three participants), and general difficulty getting used to the device and stimulus (three participants).
Discussion
The objectives of this study were to determine if listening to a customized MRIL therapy stimulus continuously through hearing aids during waking hours could be a viable tinnitus treatment option. If so, then we sought to determine if this technique could positively impact an individual's reaction to their tinnitus or suppress the perception of their tinnitus, or both. Utilizing the testing technique designed by Fournier et al. (2018) and the underlying mechanisms of residual inhibition, we created a customized, immersive sound therapy approach to suppress tinnitus perception and reactions. Below, we will interpret (1) the participant's reactions and perceptions through the primary (TFI) and secondary outcome measure (LM levels) findings, (2) discuss the feasibility of this type of tinnitus treatment through the lens of participant perspectives, and (3) propose the next phase of testing this MRIL therapy with hearing aid use for the purpose of advancing tinnitus sound therapy approaches.
Improvement of TFI Overall Scores
The TFI is a validated tinnitus outcome measure that reliably quantifies change in tinnitus reactions over time, particularly changes resulting from an intervention effect.
Our pilot study found a statistically significant change in overall TFI scores when comparing the baseline Visit 1 scores to all other visits. Participant scores decreased, meaning there was an improvement in how they reacted to their tinnitus from the baseline, pretreatment. Once treatment was initiated, TFI scores improved and continued to improve or maintain, even after the MRIL treatment was stopped at Visit 3.
The reduced TFI overall score was maintained through Visit 4 after the MRIL therapy had been discontinued. This is a somewhat expected result, as several sound therapy studies have shown maintained benefit after intervention has ceased (Neff et al. 2021; Okamoto et al. 2010; Stracke et al. 2010; Teismann et al. 2011). Though it has been reported, there is no evidence for permanent prolonged residual inhibition from any sound therapy source. Additionally, there are many factors that are often not controlled for in sound therapy trials, including hearing loss, hearing aid devices, tinnitus measurement techniques, and tinnitus perceptual characteristics. These are limitations of sound therapy trials in general, including this pilot study.
It is well known that both hearing aids and sound therapy have positive effects on tinnitus, but it is not well understood if these management strategies affect the perception of or reactions to tinnitus. Moreover, it is difficult to differentiate if hearing aids affect improvement in tinnitus, in hearing, or both. It is assumed that hearing aids affect both aspects, but evidence for this differentiation is lacking. For this study, the MRIL therapy had a positive impact on the reactions to tinnitus based on TFI scores at Visits 2 and 3 (re: the pretreatment Baseline Visit). However, though the mean TFI scores improved at Visits 2 and 3, there is a significant amount of individual variability, seen in [Fig. 4]. The variability could be due to how participants were impacted by the constant streaming of treatment, causing a negative effect on treatment acceptability.
The impact of hearing aids may also be a factor in these scores and will be discussed below when assessing the TFI Auditory subscale.
There has been a history of debate regarding what score is needed to be a “clinically significant” change in TFI scores. Meikle et al. (2012) caution that when interpreting a change in TFI scores, the magnitude of differences on the TFI may vary due to different interventions and how participants define their own “meaningful change.” Those authors continue to state that a reduction in TFI scores of ∼13 points can be regarded as a meaningful change for participants. In this study, 50% (10/20) participants showed a 13-point reduction (or more) in their TFI score from Visit 1 to Visit 2, indicating a meaningful improvement was seen in half of our participants after only a few weeks of MRIL treatment.
Improvement of TFI Subscale Scores
Our results show that six out of the eight subscales are statistically significant when comparing Baseline Visit 1 subscale scores to the other visits. Participant subscale scores indicated that their tinnitus was less intrusive, that they had more control over their tinnitus, that they had improved emotional responses and quality of life. Anecdotally, these are common types of improvements when any intervention is introduced to patients. A hearing aid, sound therapy, or cognitive behavioral therapy (CBT) will often provide relief and comfort to a patient just knowing that something is being done to reduce their tinnitus perception. The Relaxation subscale scores greatly improved over the course of the intervention, as seen in [Fig. 5] and [Table 2]. This could be a study-specific effect, with the possibility that the MRIL stimulus provided a calming effect.
The Auditory subscale scores also improved throughout the course of the visits. It is not surprising to see the Auditory subscale scores improve as hearing aids will improve audibility, even with the MRIL therapy streaming during all of a participant's waking hours. The TFI Auditory subscale questions do focus on how tinnitus affects auditory characteristics like hearing clearly, understanding others, and following conversations. However, in tinnitus research, it is a common instance to have a participant respond in terms of their hearing loss impact rather than their tinnitus impact (Henry et al. 2015). For this study, this may be the case, particularly by providing the MRIL therapy through hearing aids that have been fit for a participant's hearing loss.
Regardless, the TFI subscale improvements highlight the multifaceted reactionary benefit of the MRIL therapy via hearing aids.
Change in Loudness Match
The secondary outcome measure, the LM responses, did not show any evidence of a perceptual change in tinnitus. A reduction in LM levels across visits was neither indicated nor were any observed improvements considered statistically significant.
When compared with the TFQ and exit interview, a small percentage of participants felt that there was a reduction in loudness of their tinnitus or fluctuation of their loudness perception. When we examine the TFQ and the exit interview responses at Visits 3 and 4, we see some positive impact in loudness. TFQ responses at Visit 4 did note some improvement in negative treatment impact after the washout period.
This study performed manual psychoacoustic testing with only five sequential loudness and pitch matches at each visit. Though pitch and loudness training and orientation were provided for each participant before every psychoacoustic test battery, it is difficult to determine if participants truly understood the concepts behind pitch and loudness. Furthermore, tester bias is a factor when performing manual psychoacoustic testing. Though we are ultimately concluding that tinnitus LM levels and perception of tinnitus were not significantly impacted by MRIL therapy, an automated psychoacoustic test battery with more data acquisition could potentially provide a more detailed look at how perception might change during an intervention.
Self-Reported Tinnitus Perceptions (Follow-up Questionnaire and Exit Interview)
The collection of the Visit 3 and Visit 4 TFQ and the Visit 4 Exit Interview was an important factor in assessing if this type of immersive therapy could be feasible for clinical use. Overall, participants expressed positivity for MRIL therapy and its impact on their reactions to their tinnitus. When observing Exit Interview responses, as summarized earlier, many participants stated that they would continue using the therapy after the study had concluded because it provided them relief, comfort, and a sense of control. There was little to no concern with the use of the hearing aids, streaming the MRIL stimulus from their iPhone to their hearing aids, and the impact of the constant pulsation of sound during conversations with others. Hearing aid data logging and participant responses to the TFQ and Exit Interview questions provided evidence of feasibility, as most participants complied with daily hearing aid use for at least 8 hours. This information was an important goal of this study and is vital in considering further study of the MRIL therapy.
Additionally, it is important to compare both TFI scores and the qualitative information that participants provided in their TFQ and Exit Interview responses. As we illustrate in the Results, participants' thoughts regarding the therapy provided them with more knowledge about tinnitus and sound therapy, and also a sense of control around their tinnitus. The majority of participants also stated that they enjoyed the therapy and would recommend it to others. It can be concluded that even though participants did not feel that there was a perceptual change in tinnitus, their reactions were positively impacted, conveyed in both the TFI overall scores and their qualitative data.
Study Limitations
As a pilot study, the small sample size is a limitation. Though we successfully evaluated the two study objectives, a larger sample size is needed to determine the full potential of MRIL therapy through hearing aids. Furthermore, a randomized controlled trial (RCT) is needed to (1) differentiate the impact of hearing aid amplification and hearing loss and (2) include a control group to establish cause and effect. Our repeated measures study design, while effective for the purpose of this pilot study, does not provide rigorous review of determining the cause–effect relationship when administering MRIL therapy.
Tester bias may have been introduced during the psychoacoustic test battery despite our trained staff following standardized procedures. In future studies, an automated tinnitus testing system would help eliminate tester subjectivity when evaluating a participant's tinnitus perception during behavioral measurement assessment. Automated testing could also provide larger data samples of psychoacoustic testing to fully assess the reliability of a participant's tinnitus perception. This is particularly important for studies focusing on sound therapies intending to reduce tinnitus loudness. Additionally, there is no objective measure of tinnitus yet; therefore, it is beneficial for our field to consider additional types of testing to gain a larger perspective into the underlying mechanisms of tinnitus. The addition of electrophysiology, imaging, and electroencephalography (EEG) could be added to future test protocols to create a more robust picture of change in tinnitus perception.
Conclusions about change in tinnitus perception after any intervention type can only be made when there is a high level of confidence in the robustness of measures of tinnitus perception.
Participant-reported data tracked through their personal daily logs as an outcome measure are a potential limitation of this study. Participants actively initiated their own treatment daily and were instructed to track their own progress by using a daily log. However, the hearing aid data logging does contribute a potential bias to the data and the impact of the treatment effect. Future studies will formally measure the hearing aid data logging to track hearing aid and streaming use.
Conclusions and Future Directions
We demonstrated through this pilot study that our paradigm was feasible and acceptable to participants. The MRIL therapy provided resulted in an overall reduction in participants' reactions to tinnitus, but not in a change in perception of loudness. We propose that a larger scale RCT is needed to fully evaluate the efficacy of this sound therapy. It is unknown if one sound therapy is superior to another; therefore, further study is needed to ascertain to what degree the MRIL sound therapy effects tinnitus perception. CBT is currently the only evidence-based approach for tinnitus management and treatment. Sound therapy as an evidence-based tinnitus management and treatment could be established if research studies were aligned in testing approaches and validated outcome measures.
A future MRIL RCT would provide a thorough psychoacoustic test battery utilizing an automated system and would track both perceptual tinnitus differences pre- and posttreatment as well as provide a less biased testing approach. Without objective measures of tinnitus, it is important that our field utilize comparable testing approaches and validated outcome measures. Future use of electrophysiological outcome measures, specifically late auditory evoked potentials, could be utilized as biomarkers for pre- and post-treatment effects as well as the effect of concentration and attention on the effectiveness of sound therapy. A future RCT of MRIL therapy could provide a foundation for a standardized method of evaluating and implementing sound therapy approaches by using a battery of validated questionnaires and psychoacoustic measures, as well as objective electrophysiological measures. A standardized test battery for tinnitus sound therapies could not only provide a baseline for tracking meaningful change but a comprehensive guide for testing tinnitus interventions as well. Furthermore, the use and evaluation of hearing aids in conjunction with sound therapy could provide evidence for new, innovative ways to help tinnitus sufferers manage their tinnitus.
Conflict of Interest
Hearing aids and hearing aid supplies (i.e., domes, batteries, cleaning materials) were donated by GN ReSound. The authors declare no conflicts of interest.
Funding/Acknowledgments
The authors would like to acknowledge and thank the VA RR&D National Center for Rehabilitative Auditory Research (NCRAR) for providing funding and resources to conduct this study. Samuel Gordon is acknowledged for providing engineering and software support. Drs. Arnaud Norena and Philippe Fournier are acknowledged for their topic area expertise and collaboration. Dr. Michael Piskosz and GN Resound are acknowledged for providing hearing aids and supplies for this study.
Author Contributions: C.M.Q. and J.A.H. made substantial contributions to the conception and design of the work. C.M.Q., J.J.V., and D.K. acquired the data from the participants.
E.J.T. performed the data analysis with consultation from Dr. Garnett McMillan. All the authors contributed to the interpretation of data. C.M.Q. drafted the article and the other authors contributed substantially to revising the article critically for important intellectual content. All authors provided final approval of the version to be published.
The contents of this manuscript do not represent the views of the Department of Veterans Affairs or the U.S. government.
-
References
- Auerbach BD, Rodrigues PV, Salvi RJ. Central gain control in tinnitus and hyperacusis. Front Neurol 2014; 5: 206
- Carhart R, Jerger JF. Preferred method for clinical determination of pure tone thresholds. J Speech Hear Disord 1959; 24: 96-108
- Dobie RA. Overview: suffering from tinnitus. Tinnitus: Theory and Management. J.B. Snow. Lewiston, NY: BC Decker Inc.; 2004: 1-7
- Eggermont JJ. Acquired hearing loss and brain plasticity. Hear Res 2017; 343: 176-190
- Evered D, Lawrenson G. eds. Tinnitus. Ciba Foundation Symposium 85. London: Pitman Books, Ltd; 1981
- Feldmann H. Homolateral and contralateral masking of tinnitus by noise-bands and by pure tones. Audiology 1971; 10 (03) 138-144
- Fournier P, Cuvillier AF, Gallego S. et al. A new method for assessing masking and residual inhibition of tinnitus. Trends Hear 2018; 22: 2331216518769996
- Fuller TE, Haider HF, Kikidis D. et al. Different teams, same conclusions? A systematic review of existing clinical guidelines for the assessment and treatment of tinnitus in adults. Front Psychol 2017; 8 (206) 206
- Galazyuk AV, Voytenko SV, Longenecker RJ. Long-lasting forward suppression of spontaneous firing in auditory neurons: implication to the residual inhibition of tinnitus. J Assoc Res Otolaryngol 2017; 18 (02) 343-353
- Henry JA, Flick CL, Gilbert A, Ellingson RM, Fausti SA. Comparison of manual and computer-automated procedures for tinnitus pitch-matching. J Rehabil Res Dev 2004; 41 (02) 121-138
- Henry JA, Griest S, Austin D. et al. Tinnitus Screener: results from the first 100 participants in an epidemiology study. Am J Audiol 2016; a 25 (02) 153-160
- Henry JA, Griest S, Thielman E, McMillan G, Kaelin C, Carlson KF. Tinnitus Functional Index: development, validation, outcomes research, and clinical application. Hear Res 2016; b 334: 58-64
- Henry JA, Griest S, Zaugg TL. et al. Tinnitus and hearing survey: a screening tool to differentiate bothersome tinnitus from hearing difficulties. Am J Audiol 2015; 24 (01) 66-77
- Henry JA, Meikle MB. Psychoacoustic measures of tinnitus. J Am Acad Audiol 2020; 11 (03) 138-155
- Henry JA, Quinn CM. Sound therapy for tinnitus: options for audiologists. Perspectives Sig 8 Audiology. Public Health 2020; 5 (03) 669-683
- Hillecke T, Nickel A, Bolay HV. Scientific perspectives on music therapy. Ann N Y Acad Sci 2005; 1060 (01) 271-282
- Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res 1990; 8 (04) 221-254
- Keidser G, Dillon H, Flax M, Ching T, Brewer S. The NAL-NL2 prescription procedure. Audiology Res 2011; 1 (01) e24
- Meikle MB, Henry JA, Griest SE. et al. The tinnitus functional index: development of a new clinical measure for chronic, intrusive tinnitus. Ear Hear 2012; 33 (02) 153-176
- Neff PKA, Schoisswohl S, Simoes J. et al. Prolonged tinnitus suppression after short-term acoustic stimulation. Prog Brain Res 2021; 262: 159-174
- Okamoto H, Stracke H, Stoll W, Pantev C. Listening to tailor-made notched music reduces tinnitus loudness and tinnitus-related auditory cortex activity. Proc Natl Acad Sci U S A 2010; 107 (03) 1207-1210
- Reavis KM, Rothholtz VS, Tang Q, Carroll JA, Djalilian H, Zeng FG. Temporary suppression of tinnitus by modulated sounds. J Assoc Res Otolaryngol 2012; 13 (04) 561-571
- Roberts LE, Moffat G, Bosnyak DJ. Residual inhibition functions in relation to tinnitus spectra and auditory threshold shift. Acta Otolaryngol Suppl 2006; S556 (556) 27-33
- Roberts LE, Moffat G, Baumann M, Ward LM, Bosnyak DJ. Residual inhibition functions overlap tinnitus spectra and the region of auditory threshold shift. J Assoc Res Otolaryngol 2008; 9 (04) 417-435
- Stracke H, Okamoto H, Pantev C. Customized notched music training reduces tinnitus loudness. Commun Integr Biol 2010; 3 (03) 274-277
- Teismann H, Okamoto H, Pantev C. Short and intense tailor-made notched music training against tinnitus: the tinnitus frequency matters. PLoS One 2011; 6 (09) e24685
- Terry AM, Jones DM, Davis BR, Slater R. Parametric studies of tinnitus masking and residual inhibition. Br J Audiol 1983; 17 (04) 245-256
- Tunkel DE, Bauer CA, Sun GH. et al. Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg 2014; 151 (2, Suppl): S1-S40
- Vernon JA, Meikle MB. Tinnitus masking. In: Tyler R. ed. Tinnitus Handbook. San Diego: Singular Publishing Group; 2000: 313-356
- Vernon JA, Meikle MB. Tinnitus: clinical measurement. Otolaryngol Clin North Am 2003; 36 (02) 293-305 , vi
Address for correspondence
Publication History
Article published online:
28 June 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- Auerbach BD, Rodrigues PV, Salvi RJ. Central gain control in tinnitus and hyperacusis. Front Neurol 2014; 5: 206
- Carhart R, Jerger JF. Preferred method for clinical determination of pure tone thresholds. J Speech Hear Disord 1959; 24: 96-108
- Dobie RA. Overview: suffering from tinnitus. Tinnitus: Theory and Management. J.B. Snow. Lewiston, NY: BC Decker Inc.; 2004: 1-7
- Eggermont JJ. Acquired hearing loss and brain plasticity. Hear Res 2017; 343: 176-190
- Evered D, Lawrenson G. eds. Tinnitus. Ciba Foundation Symposium 85. London: Pitman Books, Ltd; 1981
- Feldmann H. Homolateral and contralateral masking of tinnitus by noise-bands and by pure tones. Audiology 1971; 10 (03) 138-144
- Fournier P, Cuvillier AF, Gallego S. et al. A new method for assessing masking and residual inhibition of tinnitus. Trends Hear 2018; 22: 2331216518769996
- Fuller TE, Haider HF, Kikidis D. et al. Different teams, same conclusions? A systematic review of existing clinical guidelines for the assessment and treatment of tinnitus in adults. Front Psychol 2017; 8 (206) 206
- Galazyuk AV, Voytenko SV, Longenecker RJ. Long-lasting forward suppression of spontaneous firing in auditory neurons: implication to the residual inhibition of tinnitus. J Assoc Res Otolaryngol 2017; 18 (02) 343-353
- Henry JA, Flick CL, Gilbert A, Ellingson RM, Fausti SA. Comparison of manual and computer-automated procedures for tinnitus pitch-matching. J Rehabil Res Dev 2004; 41 (02) 121-138
- Henry JA, Griest S, Austin D. et al. Tinnitus Screener: results from the first 100 participants in an epidemiology study. Am J Audiol 2016; a 25 (02) 153-160
- Henry JA, Griest S, Thielman E, McMillan G, Kaelin C, Carlson KF. Tinnitus Functional Index: development, validation, outcomes research, and clinical application. Hear Res 2016; b 334: 58-64
- Henry JA, Griest S, Zaugg TL. et al. Tinnitus and hearing survey: a screening tool to differentiate bothersome tinnitus from hearing difficulties. Am J Audiol 2015; 24 (01) 66-77
- Henry JA, Meikle MB. Psychoacoustic measures of tinnitus. J Am Acad Audiol 2020; 11 (03) 138-155
- Henry JA, Quinn CM. Sound therapy for tinnitus: options for audiologists. Perspectives Sig 8 Audiology. Public Health 2020; 5 (03) 669-683
- Hillecke T, Nickel A, Bolay HV. Scientific perspectives on music therapy. Ann N Y Acad Sci 2005; 1060 (01) 271-282
- Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res 1990; 8 (04) 221-254
- Keidser G, Dillon H, Flax M, Ching T, Brewer S. The NAL-NL2 prescription procedure. Audiology Res 2011; 1 (01) e24
- Meikle MB, Henry JA, Griest SE. et al. The tinnitus functional index: development of a new clinical measure for chronic, intrusive tinnitus. Ear Hear 2012; 33 (02) 153-176
- Neff PKA, Schoisswohl S, Simoes J. et al. Prolonged tinnitus suppression after short-term acoustic stimulation. Prog Brain Res 2021; 262: 159-174
- Okamoto H, Stracke H, Stoll W, Pantev C. Listening to tailor-made notched music reduces tinnitus loudness and tinnitus-related auditory cortex activity. Proc Natl Acad Sci U S A 2010; 107 (03) 1207-1210
- Reavis KM, Rothholtz VS, Tang Q, Carroll JA, Djalilian H, Zeng FG. Temporary suppression of tinnitus by modulated sounds. J Assoc Res Otolaryngol 2012; 13 (04) 561-571
- Roberts LE, Moffat G, Bosnyak DJ. Residual inhibition functions in relation to tinnitus spectra and auditory threshold shift. Acta Otolaryngol Suppl 2006; S556 (556) 27-33
- Roberts LE, Moffat G, Baumann M, Ward LM, Bosnyak DJ. Residual inhibition functions overlap tinnitus spectra and the region of auditory threshold shift. J Assoc Res Otolaryngol 2008; 9 (04) 417-435
- Stracke H, Okamoto H, Pantev C. Customized notched music training reduces tinnitus loudness. Commun Integr Biol 2010; 3 (03) 274-277
- Teismann H, Okamoto H, Pantev C. Short and intense tailor-made notched music training against tinnitus: the tinnitus frequency matters. PLoS One 2011; 6 (09) e24685
- Terry AM, Jones DM, Davis BR, Slater R. Parametric studies of tinnitus masking and residual inhibition. Br J Audiol 1983; 17 (04) 245-256
- Tunkel DE, Bauer CA, Sun GH. et al. Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg 2014; 151 (2, Suppl): S1-S40
- Vernon JA, Meikle MB. Tinnitus masking. In: Tyler R. ed. Tinnitus Handbook. San Diego: Singular Publishing Group; 2000: 313-356
- Vernon JA, Meikle MB. Tinnitus: clinical measurement. Otolaryngol Clin North Am 2003; 36 (02) 293-305 , vi