

Subscribe to RSS
DOI: 10.1055/s-0043-1769777
Endoscopic Transsphenoidal Surgery of Pituitary Adenomas: Preliminary Results of the Neurosurgery Service of Hospital Cristo Redentor
Cirurgia endoscópica transesfenoidal de adenomas pituitários: resultados preliminares do Serviço de Neurocirurgia do Hospital Cristo RedentorAuthors


Abstract
Objective The transsphenoidal surgery is a safe and effective technique to manage different skull base pathologies, such as pituitary adenomas. The purpose of the present study is to describe the initial experience with endoscopic transsphenoidal surgery in the treatment of pituitary adenoma patients at a tertiary hospital that is a reference in neurosurgery in Southern Brazil.
Materials and Methods We retrospectively analyzed data from 60 patients with pituitary adenoma who underwent endoscopic transsphenoidal surgery between 2012 and 2019. Demographic characteristics, type of tumor, baseline hormonal changes, and clinical presentation were reported, as well as postoperative outcomes, tumor resection rate, and complications.
Results The male/female ratio was of 0.53:1, and the mean age of the sample was of 54 (range: 26 to 79) years. In total, 34 patients (57%) presented the non-functioning adenoma subtype, and 26 (43%), the functioning adenoma subtype. In the non-functioning and functioning subtype groups, the average tumor diameter was of 32 mm and 18 mm, and the mean follow-up was of 27 months and 32 months respectively. Regarding visual symptoms, 79% of the patients showed improvement after surgery. Hormonal remission was achieved in 71% of the patients with prolactinoma, 85% of those with cushing, and 57% of patients with acromegaly. Overall, gross total resection (GTR) was achieved in 50% of patients but with a significantly lower rate among patients with tumors with parasellar growth (high grade on the Knosp classification). The most prevalent surgical complications observed were postoperative cerebrospinal fluid (CSF) leak and meningitis in 11% and 6% of the cases respectively.
Conclusion We have shown that transsphenoidal endoscopic surgery can produce good results in the management of pituitary adenomas, with acceptable peri- and postoperative morbidity and mortality. Regardless of the technique used, the presence of large and giant pituitary adenomas with a high Knosp grade represents an enormous challenge for contemporary neurosurgery.
Resumo
Objetivo A cirurgia transesfenoidal é uma técnica segura e eficaz para o tratamento de patologias da base do crânio, como os adenomas hipofisários. O objetivo deste estudo é demonstrar a experiência inicial com a cirurgia endoscópica transesfenoidal no tratamento de pacientes com adenoma hipofisário em hospital terciário, referência em neurocirurgia no Sul do Brasil.
Materiais e Métodos Analisamos retrospectivamente os dados de 60 pacientes com adenoma hipofisário submetidos à cirurgia endoscópica transesfenoidal entre 2012 e 2019. Características demográficas, tipo de tumor, alterações hormonais basais e apresentação clínica foram relatadas, bem como evolução pós-operatória, grau de ressecção tumoral e complicações.
Resultados A proporção homem/mulher foi de 0.53:1, e a idade média da amostra foi de 54 (variação: 26 a 79) anos. Ao todo, 34 pacientes (57%) tinham o subtipo funcional de adenoma, e 26 (43%), o subtipo não funcional de adenoma. Nos grupos não funcional e funcional, o diâmetro médio do tumor foi de 32 mm e 18 mm, e o tempo médio de acompanhamento foi de 27 meses e 32 meses, respectivamente. Em relação aos sintomas visuais, 79% dos pacientes apresentaram melhora após a cirurgia. A remissão hormonal foi alcançada em 71% dos pacientes com adenomas secretores de prolactina, em 85% daqueles com adenomas secretores de hormônio adrenocorticotrófico e em 57% dos pacientes com adenomas secretores de hormônio do crescimento. A ressecção total foi obtida em 50% dos pacientes, mas com taxa significativamente menor em pacientes com tumores com crescimento parasselar (grau elevado na classificação de Knosp). As complicações cirúrgicas mais prevalentes observadas foram fístula liquórica pós-operatória e meningite, em 11% e 6% dos casos, respectivamente.
Conclusão Demostramos que a cirurgia endoscópica transesfenoidal pode produzir bons resultados no manejo de adenomas hipofisários, com aceitável morbimortalidade peri e pós-operatória. Independentemente da técnica utilizada, a presença de adenomas hipofisários grandes e gigantes com grau de Knosp elevado representa um enorme desafio para a neurocirurgia contemporânea.
Introduction
Transsphenoidal surgery dates back to the beginning of the twentieth century, when pioneering surgeons described the first access to the sella turcica region.[1] [2] [3] [4] [5] In 1910, Oskar Hirsch, a Viennese otolaryngologist, described his classic endonasal transseptal transsphenoidal approach;[6] [7] in the same year, Albert Halstead described the sublabial access,[5] popularized by Harvey Cushing, who performed more than 2 thousand operations between 1910 and 1925.[7] [8]
In Brazil, in 1935, Dr. Correa Meyer and Dr. Eliseu Paglioli described the successful performance of the transsphenoidal access using Hirsch's technique to remove a pituitary tumor.[9] Since the historical technical contributions of Jules Hardy, published in the late 1960s and early 1970s, transsphenoidal surgery has been modernized and became popular as the best option in the surgical management of intrasellar lesions.[5] [10] [11]
The advantages over the transcranial access are that it provides excellent visualization of the pituitary gland and neighboring structures, with lower rates of morbidity and mortality.[12] Gerard Guiot is recognized as the first neurosurgeon to use the endoscope in transsphenoidal surgery in 1963.[13]
The experience acquired by ear, nose and throat (ENT) physicians in sinus surgery, associated with that of neurosurgeons using the endoscope in an assisted manner, stimulated an interest in endoscopy that began in the end of the 1980s.[14]
As a result of this collaboration, the use of pure or isolated endoscopy started in the 1990s. In the last 25 years, there has been an exponential growth in its use, and it is currently considered a safe and effective technique to manage different skull base pathologies.[15] [16] [17] [18] [19] [20] [21] [22] [23] [24] [25] [26] [27] [28] [29] [30]
Hospital Cristo Redentor (HCR), a public hospital part of Grupo Hospitalar Conceição (GHC), located in the City of Porto Alegre, Southern Brazil, is considered a national reference in neurosurgery. In its facilities, through the effort and integration of the neurosurgery and otorhinolaryngology specialties, endoscopy in transsphenoidal surgery began in 2012.
The objective of the present study is to describe the initial experience with endoscopic transsphenoidal surgery in the treatment of pituitary adenomas at HCR.
Materials and Methods
We conducted a retrospective study to evaluate the first 60 patients with pituitary adenomas submitted to endoscopic transsphenoidal surgery from 2012 to 2019 and treated by the same main team (GP and AM). The study was submitted and approved by the GHC Ethics in Research Committee.
All patients underwent a preoperative evaluation to confirm the diagnosis, which was based on history, clinical examination, laboratory tests, ophthalmological evaluation, and imaging tests.
All patients underwent an evaluation of the pituitary function by the endocrinologist (FA). Imaging studies, such as computed tomography (CT) of the sinuses and magnetic resonance imaging (MRI) of the sella with all sequences, were performed in all cases. The Hammer and Radberg classification[31] was used to assess the extent of pneumatization of the sphenoid sinus in all cases.
The patients were divided into two groups according to the adenoma subtype (non-functioning and functioning), and their respective data were analyzed individually. The sizes of the adenomas were described, and their extensions were classified using Hardy and Vezina[32] and Knosp classifications.[33]
Surgical Technique
The patients were in supine position under general anesthesia and orotracheal intubation, with the back elevated (10°) and the head slightly rotated to the right. Intravenously, a single dose of cefazolin 1 g was administered as a prophylactic antibiotic during the initial phase of anesthesia.
The ENT physician and the neurosurgeon were positioned on the patient's right and left sides respectively. The video tower and rigid endoscopes of 4 mm at 0° and 30° were used, with the recording and storage of images performed routinely.
In the initial phase of the procedure, the nasoseptal flap was harvested. The flap was relocated to the original position at the end of the surgery using suture or biological.
The access to the sellar region was performed following the nasal, sphenoidal, and skull base phases. The use of the two nostrils enabled the surgical teams to work together with the optics and surgical instruments present in the operative field in an integrated manner.
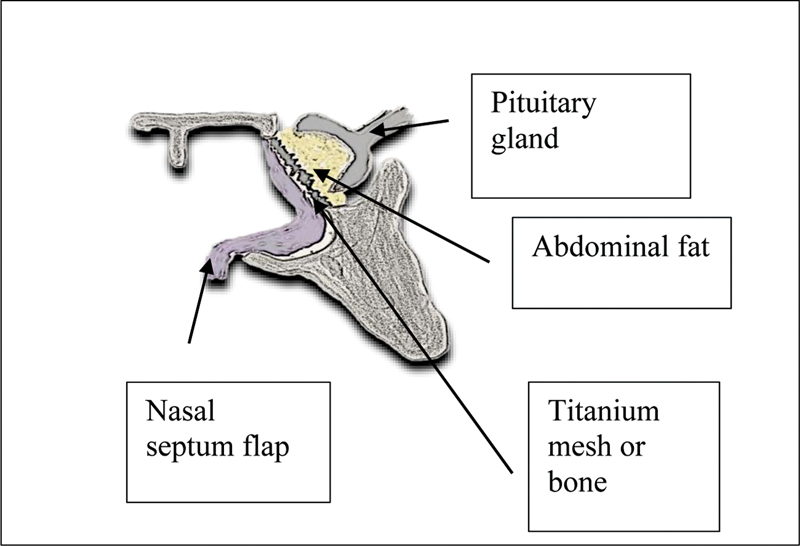
After opening the sella floor and dura mater, tumor removal and subsequent exploration of the sella were performed. The repair was performed sequentially using an abdominal fat graft, the nasoseptal flap, and fibrin glue in patients with the observed opening of the sellar diaphragm and cerebrospinal fluid (CSF) drainage. In these cases, at the end of the surgical procedure, a lumbar drain was maintained for 72 hours.
Considering the high number of cases of postoperative leak observed in the early years, the reconstruction technique was modified by adding bone graft or titanium mesh to reconstruct the sella turcica. ([Figure 1]). We observed an important decrease in the incidence of postoperative fistula after the routine adoption of this technical modification. The tumor samples collected during the procedures were sent for anatomopathological study and subsequent immunohistochemical analysis.
Postoperative Evaluation
The patients were evaluated postoperatively concerning the neuro-ophthalmological status and endocrinological evaluation. The immunohistochemistry findings were reported, and complications were reviewed and analyzed.
During the follow-up, the patients underwent MRI between 3 months and 1 year after the surgery. According to the last control performed, tumor removal was classified as gross total resection or subtotal/partial resection. Patients with functioning tumors were followed up by the endocrinology team using laboratory criteria and clinical symptoms to define the criteria for disease remission.
Results
Overall, we operated 60 patients with pituitary adenomas, 21 male (35%) and 39 female subjects (65%), with a mean age of 54 years: 34 cases were classified as non-functioning adenoma and 26, as functioning.
Hormone changes, with hyperfunction or hypofunction, were often found as the clinical presentation, as well as visual symptoms. Regarding the group with functioning tumors, 11 patients presented acromegaly, 7 subjects had macroprolactinomas, 7 presented Cushing syndrome, and 1 patient had hyperthyroidism/acromegaly syndrome.
Hypogonadism, hypothyroidism, and hypocortisolism were found in 26%, 23%, and 5% of the cases respectively. Panhypopituitarism was found in 5% of the patients, and 78% had preoperative vision disorder manifested by changes in the visual field or loss of visual acuity.
Symptoms such as headache were observed in 18% of the cases, while mental confusion, seizure, and hemiparesthesia were seen in 3%. A total of 3 patients (5%) had undergone previous surgical treatment; all of them underwent transsphenoidal microsurgery in other institutions.
Demographic characteristics, type of tumor, baseline hormonal changes, clinical presentation, and previous surgery history are summarized in [Table 1].
Suprasellar extension greater than 20 mm was observed in 20 patients (59%) in the non-functioning group and only in 3 patients (12%) in the functioning group. In the functioning group, 18 patients (69%) presented suprasellar extension measuring between 0 mm and 10 mm.
Regarding the Knosp classification, in the non-functioning group, 21 patients (65%) were categorized as grades 0 to 2, and 13 patients (35%), as grades 3 to 4. In the functioning tumor group, 21 patients (81%) were classified as grades 0 to 2, and 5 (19%), as grades 3 to 4. The suprasellar extension and degree of cavernous sinus invasion (Knosp scale) of both groups are detailed in [Table 2] and [2], [3], [4] and [5].




According to the Hammer and Radberg classification, 6 patients (10%) had a sinus of the presellar type, equally distributed between the two groups of patients. Most patients had the sellar type, and no cases of sphenoidal sinus of the conchal type were observed.
([Table 3])
Surgical Results
Regarding the immunohistochemistry results, in the group of non-functioning adenomas, 16 patients (47%) presented “null cell”. In the functioning group, the results showed gonadotropin, adrenocorticotropic hormone (ACTH), and prolactin in 41%, 6%, and 3% of the cases respectively.
Still according to the immunohistochemistry results, in the functioning group, there were 7 patients (27%) with tumors that secreted growth hormone (GH), 7 (27%) patients with prolactin-secreting tumors, 4 patients (15%) with ACTH-secreting tumors, and only 1 patient (4%) with a tumor that secreted thyroid-stimulating hormone (TSH) ([Table 4]).
Regarding the visual symptoms 79% of the patients experienced improvement after surgery, while 15% remained stable, and 6% presented worsening of the deficit in the postoperative period.
Hormonal disfunction was found in 55% of the patients, a rate similar to the preoperative rate. None of the patients progressed to panhypopituitarism, and there were no cases of improvement in the pituitary function during the postoperative follow-up period. A total of 54 patients underwent postoperative MRI between 3 months and 1 year, there were 5 cases of loss to outpatient follow-up, and 1 patient died in the first month after surgery.
Overall, GTR was possible in 27 cases (50%). In the non-functioning group, it was achieved in 12 patients (37%), and, in the remaining cases, the resection was subtotal or partial. The rate of GTR showed a difference when comparing the Knosp 0-2 and Knosp 3-4 patients: it was significantly lower in tumors with a high grade on the Knosp classification (p < 0.05).
Complete resection was achieved in 69% of the Knosp 0-2 patients and all Knosp 3-4 subjects underwent subtotal or partial resection. In total, 7 patients (13%) in whom only partial resection was achieved were referred for a new surgery; 3 of them underwent a new endoscopic endonasal procedure, and 4 were referred for craniotomy. After the second procedure, GTR was achieved in 3 (43%) patients, and the 4 (67%) remaining subjects with residual tumors were referred for radiotherapy. The 13 (40%) patients who remained with subtotal resection showed no progression of the symptoms during the follow-up period and were kept under outpatient observation.
Details of the results found for each functioning tumor subtype are described as follows.
Growth Hormone-Secreting Adenomas
Growth hormone-secreting adenoma was the most common hormone-secreting adenoma found in our series: 4 out of 11 patients were excluded due to loss to follow-up; all the remaining 7 patients had macroadenomas, and 1 of them had a cystic characteristic.
In 4 patients (57%), hormonal control was achieved in the postoperative period. The 3 patients without hormonal control after the surgery showed a good clinical response to pharmacological treatment during the follow-up.
Prolactinomas
Of the 7 patients with prolactinomas selected for surgery, 6 had macroadenomas with cystic and/or hemorrhagic characteristics. One patient had a macroadenoma with a high Knosp grade presented with no hormonal control using dopaminergic agonists. We achieved overall hormonal control after surgery in 5 patients (71%).
ACTH-Secreting Adenoma
A total of 6 patients had macroadenomas with sizes ranging from 10 mm to 20 mm, and only 1 patient had a microadenoma with a size of 6 mm. No tumor had cystic characteristics, and there was hormonal control after surgery in 6 cases (85%) during the follow-up.
TSH/GH-secreting Adenoma
In the present series, we found one patient with a macroadenoma with lateral extension (Knosp 4) and a plurihormonal profile (GH- and TSH-secreting). After the surgery, the TSH and GH values remained high, although lower than in the preoperative period. A control MRI showed subtotal resection (presence of residual tumor within the cavernous sinus). After introducing the drug treatment, reduction and control of the hormonal levels maintained during the follow-up period were achieved. The mean follow-up time was of 27 months and 32 months in the non-functioning and functioning adenoma groups respectively.
Details of the surgical results for each subgroup are shown in the following organizational chart:

Complications
Intraoperative CSF leak is the most frequent complication, and it was found in 13 patients (24%), followed by postoperative CSF leak in 6 patients (11%).
There were 4 patients (7.4%) with meningitis; 3 of them showed good evolution, but 1 developed severe meningitis and ventriculitis complications and died after a long period of hospitalization. One patient had epistaxis on the first day after surgery and needed to be reoperated.
According to the postoperative tomography, 2 patients (3.6%) with large tumors developed intrasellar hematoma. The management was conservative, given the stability of the visual symptoms. One case of a male patient with late visual deterioration (one year after surgery) was associated with chiasma prolapse in the empty sella. He underwent a transcranial approach for chiasmapexy, and evolved with the improvement in the visual deficit.
Transient diabetes insipidus (DI) was observed in 9 patients (16.6%), but there were no cases of postoperative permanent DI. All of them were managed in the intensive care unit and showed good response to the clinical interventions.
There was a death related to CSF fistula and central nervous system (CSN) infection that occurred within 30 days of the surgery. The complications have been summarized in [Table 5].
Discussion
Transsphenoidal surgery is considered an excellent alternative to craniotomy in the management of most pituitary adenomas.[34]
Throughout the twentieth century, the technique underwent improvements and modifications,[35] and the use of endoscopy in transsphenoidal surgery is considered a recent breakthrough.[36]
According to Yu et al.,[37] endoscopic endonasal transsphenoidal surgery in the treatment of pituitary adenomas presents results that are similar or better than those of traditional microscopy in terms of mass removal, improvement in visual symptoms, and preservation of endocrine function.
Regarding nasal morbidity and quality of life, it can be said that the endoscopic technique is less morbid because it does not use a sublabial incision or nasal plug, besides producing lower levels of mucosal detachment.[38] [39]
The technical advantages of endoscopic endonasal transsphenoidal surgery are related to an increase in the working angle, enabling a close and panoramic view of the anatomical structures.[27] [40] [41]
In the present study, we performed the isolated or pure endoscopic technique, in which only the endoscope is used in all stages of the procedure, as described by several authors in the 1990s.[15] [16] [17] [18]
In the present series, most of the tumors were macroadenomas. Analyzing the groups of patients with non-functioning and functioning adenomas, we observed that the mean sizes of the tumors was of 32 mm and 18 mm respectively, which are larger than the sizes reported in some of the previously described series.[42] [43]
Delay in diagnosis due to the difficulty on the part of the patients to access our health system could explain this finding.
Non-Functioning Tumors
The main objectives of the surgical treatment of non-functioning adenomas are to preserve the neighboring neural structures, to prevent functional worsening of the pituitary and visual function, and to revert any functional impact on the surrounding neural structures.[44] Although the improvement in pituitary function in the postoperative period has been reported to range from 16% to 48% of the cases,[45] no improvements were reported in previous series.[46] [47] In the present study, pituitary function remained unchanged, with no improvement or worsening observed in any patient.
According to Wichers-Rother et al.,[47] the objective of transsphenoidal surgery is to improve visual field defects rather than to improve the pituitary function. Regarding vision, 79% of our patients showed visual improvement in the postoperative period, a rate similar to that of previous reports.[44] [45] [48] In the present series, the rate of 37% of GTR in the non-functioning group is lower than the one reported in previous endoscopic series.[49] [50] [51] [52] [53] [54] [55] This result is related to the learning curve of the endoscopic technique[56] associated with the findings of large tumors with frequent lateral extension. Patients with high Knosp grades are more likely to present tumor invasion of the parasellar region, which decreases the chance of GTR.[57] Accordingly, we found a statistically significant difference in GTR when comparing patients with Knosp grades 0 to 2 and 3 to 4.
Tumors with Knosp grade 3 or 4 have a greater degree of cavernous sinus invasion and were predictors of greater difficulty in achieving a GTR.
In the present study, the approaches were restricted to the sellar region, which certainly limited the possibility of achieving GTR in tumors of larger size and volume.
Biological factors inherent to the tumor are important in relapse, so not all residual lesions will present a regrowth over time.[46] [58] In agreement with this, 13 patients (40%) in whom residual lesions were observed on the postoperative MRI in the present study did not present any changes during the follow-up.
As the postoperative recurrence rate for non-functioning tumors peaks between 1 and 5 years and only reduces after 10 years, it is essential to maintain the follow-up of these patients for longer periods.[59]
Functioning Tumors
Tumors that secrete GH and prolactin are the most common type of functioning pituitary adenomas.[49] In the present series, we found more GH-secreting adenomas (37%) and an equal number of ACTH- and prolactin-secreting adenomas (29%).
Regarding the subjects with GH-secreting tumors, we obtained control of hormonal levels in 4 patients (57%), a rate similar to the 56.4% mean historical control rate for first-time surgery.[60]
According to Nomikos et al.,[61] the remission rate in patients undergoing transsphenoidal surgery tended to decrease in macroadenomas, being of 33.3% for suprasellar tumors with visual impairment and of 44.5% for suprasellar tumors without impairment. In our case series, patients with acromegaly had large lesions, more than 1 cm in diameter, and we achieved a remission rate in 57% of cases.
Managing patients with acromegaly without control of hormonal levels after the first operation is a matter of discussion.[61] Three patients in whom control was not achieved after surgery were referred for drug treatment and showed good clinical response during the follow-up.
Regarding prolactinomas, although we found large tumors (the largest measuring 45 mm), most of them had cystic or hemorrhagic characteristics, increasing the chance of achieving GTR. Our resection rate of 71% for prolactin-secreting macroadenomas is similar to rates in previously described series.[53] [62] [63]
The surgical treatment of prolactinomas is indicated in patients who have tolerance or resistance to the use of dopaminergic agonists or who have tumors larger than 20 mm with an associated visual deficit.[53] In some countries, the cost of the drug treatment is also considered in this decision.[49] Therefore, there is some controversy about the best management. According to Donoho and Laws (ref [64]), patients with prolactinomas in the subacute evolution and mild early visual changes can be controlled with medication.
There is some controversy about the best management. According to Donoho and Laws,[64] patients with prolactinomas in subacute evolution and mild early visual changes could be managed with medications.
On the other hand, Akinduro et al.[65] report that, given the significant reduction in the largest tumor volume and prolactin levels occurring within six months after starting the treatment, surgery would play an important role in patients with a large tumor and acute visual deterioration.
We agree that patients with prolactin-secreting macroadenomas with cystic/hemorrhagic characteristics, suprasellar growth, and visual loss may actually benefit from the endoscopic endonasal transsphenoidal surgery.
Our disease control rate of 85% for Cushing disease is superior to that of a previous endoscopic series,[66] considering that 6 of the 7 operated patients had macroadenomas.
As previously described, the recurrence rate for Cushing disease can vary from 10% to 30% up to 10 years after surgery,[67] [68] with 50% of recurrences occurring during the first 50 months after surgery.[69] Considering that our follow-up was of 32 months, there is a need for longer follow-up periods to confirm the remission rate.
Tumors that secrete TSH (thyrotropinomas) are very rare pituitary tumors, corresponding to 1% to 5% of the cases.[70] [71] [72] They often concomitantly secrete other pituitary hormones, such as prolactin, gonadotropins, and GH, which is the most frequently co-secreted hormone.[71]
These tumors show an aggressive growth pattern and are harder to control only with surgery compared with other types of adenomas. Therefore, radiotherapy and drug treatment should be considered in the case of surgical failure.[72]
In the present series, one patient had a macroadenoma that simultaneously secreted TSH and GH. This patient underwent subtotal resection and achieved hormonal control during the follow-up after using long-acting somatostatin analogs.
Complications
The occurrence of intraoperative and postoperative CSF leaks in endoscopic surgery of pituitary adenomas varies from 16%b to 26% and from 1.3% to 10.3% respectively.[73] [74]
According to Lobatto et al.,[75] the following preoperative risk factors are associated with a potential higher risk of CSF leak: adenomas with intraventricular extension, age under 65 years, being female, peptic ulcer disease, and high body mass index (BMI). Boling et al.[76] describe intraventricular extension as the main risk factor associated with the occurrence of postoperative fistula, and they suggest aggressive treatment of the intraoperative fistula in these cases.[76]
The learning curve is also considered an important factor associated with the risk of CSF leak and most of the complications described.[73] In the present study, our CSF leak rate of 11% is strongly associated with the learning curve.
In endoscopic pituitary surgery, the incidence of intracranial infection ranges from 0 to 9.8%.[75] Longer operative time, diabetes mellitus, and intraoperative CSF leak are the main factors associated with its occurrence.[77] In the present study, the rate of CNS infection was of 7.4%, which falls within this range. All cases were associated with the occurrence of intraoperative CSF leak.
The occurrence of intratumoral bleeding of large and giant adenomas in the postoperative period has been reported to range from 2.1% to 3.7%.[78] [79] [80] Considering the high risk of visual deterioration, emergency craniotomy should always be considered in the management of this complication.[81] In the present study, the rate of intratumoral bleeding of 3.6% is similar to the rates reported in previous series. The patients in the present study who suffered from this complication did not show any visual deterioration, and they were not referred to emergency craniotomy.
The association of an empty sella with visual impairment was described almost 50 years ago.[82] Such a condition is associated with delayed visual deterioration after pituitary surgery.[83] The pathophysiology would be the presence of scar tissue related to the secondary empty sella, causing retraction and lower displacement of the sellar diaphragm and the optic apparatus. The repair of such a condition, known as chiasmapexy, can be performed by the transcranial or transsphenoidal routes.[84]
In the present series the only patient with chiasmapexy needed a transcranial repair in which retraction of the optic apparatus and its lower displacement along with the sellar diaphragm were observed. Release of fibrosis and scar tissue adhered to the optic nerves was achieved, improving visual acuity in the postoperative period.
Although it is a rare condition, the pituitary surgeon must watch out for patients with visual deterioration in the late postoperative period associated with the presence of an empty sella.
The prevalence of temporary and permanent DI is of 9.1 and 2.3% respectively, which is significantly lower when compared to microsurgery.[85] According to Kim et al.,[52] invasive tumors, previous surgery, and radiotherapy can increase its prevalence. In the present series, 9 patients (16.6%) developed transient DI, and none developed permanent DI.
The overall mortality rate in the present series was 1.8% (1 patient), which is higher than the mean rate of 0.5% reported in the literature.[76] The case was directly related to the surgical procedure (CSF leak/meningitis).
There certainly is a learning curve regarding the use of the endoscopic technique. As the experience increases, the incidence of complications as a whole will obviously decrease. This current study describes a small sample submitted to the initial experience with endoscopy in transsphenoidal surgery.
Conclusion
The current study describes a small sample submitted to the initial experience with endoscopy in transsphenoidal surgery in a public tertiary hospital, a reference in neurosurgery in Southern Brazil. We were able to show that the technique can yield good results in the management of pituitary tumors, with acceptable peri- and postoperative morbidity and mortality. Regardless of the technique currently used, the presence of large and giant pituitary adenomas with high Knosp grades represents a great challenge for contemporary neurosurgery.
Conflict of Interests
The authors have no conflict of interests to declare.
-
References
- 1 Liu JK, Das K, Weiss MH, Laws Jr ER, Couldwell WT. The history and evolution of transsphenoidal surgery. J Neurosurg 2001; 95 (06) 1083-1096
- 2 Prevedello DM, Doglietto F, Jane Jr JAJ, Jagannathan J, Han J, Laws Jr ERJ. History of endoscopic skull base surgery: its evolution and current reality. J Neurosurg 2007; 107 (01) 206-213
- 3 Grosvenor AE, Laws ER. The evolution of extracranial approaches to the pituitary and anterior skull base. Pituitary 2008; 11 (04) 337-345
- 4 Artico M, Pastore FS, Fraioli B, Giuffrè R. The contribution of Davide Giordano (1864-1954) to pituitary surgery: the transglabellar-nasal approach. Neurosurgery 1998; 42 (04) 909-911 , discussion 911–912
- 5 Kanter AS, Dumont AS, Asthagiri AR, Oskouian RJ, Jane Jr JA, Laws Jr ER. The transsphenoidal approach. A historical perspective. Neurosurg Focus 2005; 18 (04) e6
- 6 Liu JK, Cohen-Gadol AA, Laws Jr ERJ, Cole CD, Kan P, Couldwell WT. Harvey Cushing and Oskar Hirsch: early forefathers of modern transsphenoidal surgery. J Neurosurg 2005; 103 (06) 1096-1104
- 7 Lanzino G, Laws Jr ERJ. Pioneers in the development of transsphenoidal surgery: Theodor Kocher, Oskar Hirsch, and Norman Dott. J Neurosurg 2001; 95 (06) 1097-1103
- 8 Rosegay H. Cushing's legacy to transsphenoidal surgery. J Neurosurg 1981; 54 (04) 448-454
- 9 Meyer C, Ritter F. Tumor de Hipófise: Operação de Hirsch-Segura. - Estudo neuro-clínico e oftalmologico. Rev dos Cursos. Fac Med. 1935; 21 (21) 1-23
- 10 Hardy J. Transphenoidal microsurgery of the normal and pathological pituitary. Clin Neurosurg 1969; 16: 185-217
- 11 Hardy J. Transsphenoidal hypophysectomy. J Neurosurg 1971; 34 (04) 582-594
- 12 Cavallo LM, Messina A, Cappabianca P. et al. Endoscopic endonasal surgery of the midline skull base: anatomical study and clinical considerations. Neurosurg Focus 2005; 19 (01) E2
- 13 Castelnuovo P, Dallan I, Battaglia P, Bignami M. Endoscopic endonasal skull base surgery: past, present and future. Eur Arch Otorhinolaryngol 2010; 267 (05) 649-663
- 14 Doglietto F, Prevedello DM, Jane Jr JAJ, Han J, Laws Jr ERJ. Brief history of endoscopic transsphenoidal surgery–from Philipp Bozzini to the First World Congress of Endoscopic Skull Base Surgery. Neurosurg Focus 2005; 19 (06) E3
- 15 Jankowski R, Auque J, Simon C, Marchal JC, Hepner H, Wayoff M. Endoscopic pituitary tumor surgery. Laryngoscope 1992; 102 (02) 198-202
- 16 Sethi DS, Pillay PK. Endoscopic management of lesions of the sella turcica. J Laryngol Otol 1995; 109 (10) 956-962
- 17 Jho H-D, Carrau RL. Endoscopic endonasal transsphenoidal surgery: experience with 50 patients. J Neurosurg 1997; 87 (01) 44-51 https://thejns.org/view/journals/j-neurosurg/87/1/article-p44.xml
- 18 Cappabianca P, Alfieri A, de Divitiis E. Endoscopic endonasal transsphenoidal approach to the sella: towards functional endoscopic pituitary surgery (FEPS). Minim Invasive Neurosurg 1998; 41 (02) 66-73 10.1055/s-2008-1052019
- 19 Alfieri A, Jho H-D, Tschabitscher M. Endoscopic endonasal approach to the ventral cranio-cervical junction: anatomical study. Acta Neurochir (Wien) 2002; 144 (03) 219-225 , discussion 225 http://www.ncbi.nlm.nih.gov/pubmed/11956934
- 20 Cappabianca P, Frank G, Pasquini E, de Divitiis O, Calbucci F. Extended endoscopic endonasal transsphenoidal approaches to the suprasellar region, planum sphenoidale and clivus. In: de Divitiis E, Cappabianca P. eds. Endoscopic Endonasal Transsphenoidal Surgery [Internet]. Vienna: Springer Vienna; 2003: 176-187 . Available from: https://doi.org/10.1007/978-3-7091-6084-8_11
- 21 Solari D, Morace R, Cavallo LM. et al. The endoscopic endonasal approach for the management of craniopharyngiomas. J Neurosurg Sci 2016; 60 (04) 454-462
- 22 Linsler S, Oertel J. Endoscopic Endonasal Transclival Resection of a Brainstem Cavernoma: A Detailed Account of Our Technique and Comparison with the Literature. World Neurosurg 2015; 84 (06) 2064-2071
- 23 Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R. Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 2005; 19 (01) E6
- 24 Frank G, Pasquini E, Doglietto F. et al. The endoscopic extended transsphenoidal approach for craniopharyngiomas. Neurosurgery 2006; 59 (1, Suppl 1) ONS75-ONS83 , discussion ONS75–ONS83
- 25 Snyderman C, Kassam A, Carrau R, Mintz A. Endoscopic approaches to the petrous apex. Oper Tech Otolaryngol Neck Surg. 2006; 17: 168-173
- 26 Fernandez-Miranda JC, Gardner PA, Prevedello DM, Kassam AB. Expanded endonasal approach for olfactory groove meningioma. Acta Neurochir (Wien) 2009; 151 (03) 287-288 , author reply 289–290
- 27 Dehdashti AR, Ganna A, Witterick I, Gentili F. Expanded endoscopic endonasal approach for anterior cranial base and suprasellar lesions: indications and limitations. Neurosurgery 2009; 64 (04) 677-687 , discussion 687–689
- 28 Shin M, Kondo K, Saito N. Current Status of Endoscopic Endonasal Surgery for Skull Base Meningiomas: Review of the Literature. Neurol Med Chir (Tokyo) 2015; 55 (09) 735-743 https://pubmed.ncbi.nlm.nih.gov/26345667
- 29 Mangussi-Gomes J, Beer-Furlan A, Balsalobre L, Vellutini EAS, Stamm AC. Endoscopic Endonasal Management of Skull Base Chordomas: Surgical Technique, Nuances, and Pitfalls. Otolaryngol Clin North Am 2016; 49 (01) 167-182
- 30 Zoli M, Milanese L, Bonfatti R. et al. Clival chordomas: considerations after 16 years of endoscopic endonasal surgery. J Neurosurg 2018; 128 (02) 329-338
- 31 Hammer G, Rådberg C. The sphenoidal sinus. An anatomical and roentgenologic study with reference to transsphenoid hypophysectomy. Acta Radiol 1961; 56 (06) 401-422 https://journals.sagepub.com/doi/abs/10.1177/028418516105600601
- 32 Hardy J, Vezina JL. Transsphenoidal neurosurgery of intracranial neoplasm. Adv Neurol 1976; 15: 261-273
- 33 Knosp E, Steiner E, Kitz K, Matula C. Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery 1993; 33 (04) 610-617 , discussion 617–618
- 34 Li H-Y, Feng C-Y, Zhang C. et al. Microscopic surgery for pituitary adenomas to preserve the pituitary gland and stalk. Exp Ther Med 2017; 13 (03) 1011-1016
- 35 Gandhi CD, Christiano LD, Eloy JA, Prestigiacomo CJ, Post KD. The historical evolution of transsphenoidal surgery: facilitation by technological advances. Neurosurg Focus 2009; 27 (03) E8
- 36 Theodros D, Patel M, Ruzevick J, Lim M, Bettegowda C. Pituitary adenomas: historical perspective, surgical management and future directions. CNS Oncol 2015; 4 (06) 411-429
- 37 Yu S-Y, Du Q, Yao S-Y. et al. Outcomes of endoscopic and microscopic transsphenoidal surgery on non-functioning pituitary adenomas: a systematic review and meta-analysis. J Cell Mol Med 2018; 22 (03) 2023-2027 https://pubmed.ncbi.nlm.nih.gov/29314715
- 38 White DR, Sonnenburg RE, Ewend MG, Senior BA. Safety of minimally invasive pituitary surgery (MIPS) compared with a traditional approach. Laryngoscope 2004; 114 (11) 1945-1948
- 39 Nishioka H. Recent Evolution of Endoscopic Endonasal Surgery for Treatment of Pituitary Adenomas. Neurol Med Chir (Tokyo) 2017; 57 (04) 151-158 https://pubmed.ncbi.nlm.nih.gov/28239067
- 40 O'Malley Jr BWJ, Grady MS, Gabel BC. et al. Comparison of endoscopic and microscopic removal of pituitary adenomas: single-surgeon experience and the learning curve. Neurosurg Focus 2008; 25 (06) E10
- 41 Cappabianca P, Cavallo LM, Solari D, Stagno V, Esposito F, de Angelis M. Endoscopic endonasal surgery for pituitary adenomas. World Neurosurg 2014; 82 (06) S3-S11
- 42 Tabaee A, Anand VK, Barrón Y. et al. Predictors of short-term outcomes following endoscopic pituitary surgery. Clin Neurol Neurosurg 2009; 111 (02) 119-122
- 43 Jain AK, Gupta AK, Pathak A, Bhansali A, Bapuraj JR. Endonasal transsphenoidal pituitary surgery: is tumor volume a key factor in determining outcome?. Am J Otolaryngol 2008; 29 (01) 48-50
- 44 Esposito D, Olsson DS, Ragnarsson O, Buchfelder M, Skoglund T, Johannsson G. Non-functioning pituitary adenomas: indications for pituitary surgery and post-surgical management. Pituitary 2019; 22 (04) 422-434
- 45 Penn DL, Burke WT, Laws ER. Management of non-functioning pituitary adenomas: surgery. Pituitary 2018; 21 (02) 145-153
- 46 Dekkers OM, Pereira AM, Roelfsema F. et al. Observation alone after transsphenoidal surgery for nonfunctioning pituitary macroadenoma. J Clin Endocrinol Metab 2006; 91 (05) 1796-1801
- 47 Wichers-Rother M, Hoven S, Kristof RA, Bliesener N, Stoffel-Wagner B. Non-functioning pituitary adenomas: endocrinological and clinical outcome after transsphenoidal and transcranial surgery. Exp Clin Endocrinol Diabetes 2004; 112 (06) 323-327
- 48 Murad MH, Fernández-Balsells MM, Barwise A. et al. Outcomes of surgical treatment for nonfunctioning pituitary adenomas: a systematic review and meta-analysis. Clin Endocrinol (Oxf) 2010; 73 (06) 777-791
- 49 Wang F, Zhou T, Wei S. et al. Endoscopic endonasal transsphenoidal surgery of 1,166 pituitary adenomas. Surg Endosc 2015; 29 (06) 1270-1280
- 50 Gondim JA, Schops M, de Almeida JPC. et al. Endoscopic endonasal transsphenoidal surgery: surgical results of 228 pituitary adenomas treated in a pituitary center. Pituitary 2010; 13 (01) 68-77
- 51 Cappabianca P, Cavallo LM, de Divitiis E. Endoscopic endonasal transsphenoidal surgery. Neurosurgery 2004; 55 (04) 933-940 , discussion 940–941
- 52 Kim JH, Lee JH, Lee JH, Hong AR, Kim YJ, Kim YH. Endoscopic Transsphenoidal Surgery Outcomes in 331 Nonfunctioning Pituitary Adenoma Cases After a Single Surgeon Learning Curve. World Neurosurg 2018; 109: e409-e416
- 53 Torales J, Halperin I, Hanzu F. et al. Endoscopic endonasal surgery for pituitary tumors. Results in a series of 121 patients operated at the same center and by the same neurosurgeon. Endocrinol Nutr 2014; 61 (08) 410-416
- 54 Dehdashti AR, Ganna A, Karabatsou K, Gentili F. Pure endoscopic endonasal approach for pituitary adenomas: early surgical results in 200 patients and comparison with previous microsurgical series. Neurosurgery 2008; 62 (05) 1006-1015 , discussion 1015–1017
- 55 Bokhari AR, Davies MA, Diamond T. Endoscopic transsphenoidal pituitary surgery: a single surgeon experience and the learning curve. Br J Neurosurg 2013; 27 (01) 44-49
- 56 Ciric I, Ragin A, Baumgartner C, Pierce D. Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery 1997; 40 (02) 225-236 , discussion 236–237
- 57 Micko ASG, Wöhrer A, Wolfsberger S, Knosp E. Invasion of the cavernous sinus space in pituitary adenomas: endoscopic verification and its correlation with an MRI-based classification. J Neurosurg 2015; 122 (04) 803-811
- 58 Maletkovic J, Dabbagh A, Zhang D. et al. Residual Tumor Confers a 10-Fold Increased Risk of Regrowth in Clinically Nonfunctioning Pituitary Tumors. J Endocr Soc 2019; 3 (10) 1931-1941
- 59 Roelfsema F, Biermasz NR, Pereira AM. Clinical factors involved in the recurrence of pituitary adenomas after surgical remission: a structured review and meta-analysis. Pituitary 2012; 15 (01) 71-83 https://pubmed.ncbi.nlm.nih.gov/21918830
- 60 Almeida JP, Ruiz-Treviño AS, Liang B. et al. Reoperation for growth hormone-secreting pituitary adenomas: report on an endonasal endoscopic series with a systematic review and meta-analysis of the literature. J Neurosurg 2018; 129 (02) 404-416
- 61 Nomikos P, Buchfelder M, Fahlbusch R. The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical ‘cure’. Eur J Endocrinol 2005; 152 (03) 379-387
- 62 Han Y-L, Chen D-M, Zhang C, Pan M, Yang X-P, Wu Y-G. Retrospective analysis of 52 patients with prolactinomas following endoscopic endonasal transsphenoidal surgery. Medicine (Baltimore) 2018; 97 (45) e13198-e13198 https://pubmed.ncbi.nlm.nih.gov/30407358
- 63 Zielinski G, Ozdarski M, Maksymowicz M, Szamotulska K, Witek P. Prolactinomas: Prognostic Factors of Early Remission After Transsphenoidal Surgery. Front Endocrinol (Lausanne) 2020; 11: 439
- 64 Donoho DA, Laws Jr ER. The Role of Surgery in the Management of Prolactinomas. Neurosurg Clin N Am 2019; 30 (04) 509-514
- 65 Akinduro OO, Lu VM, Izzo A. et al. Radiographic and Hormonal Regression in Prolactinomas: An Analysis of Treatment Failure. World Neurosurg 2019; 129: e686-e694
- 66 Ferriere A, Tabarin A. Cushing's syndrome: Treatment and new therapeutic approaches. Best Pract Res Clin Endocrinol Metab 2020; 34 (02) 101381
- 67 Patil CG, Prevedello DM, Lad SP. et al. Late recurrences of Cushing's disease after initial successful transsphenoidal surgery. J Clin Endocrinol Metab 2008; 93 (02) 358-362
- 68 Pivonello R, De Leo M, Cozzolino A, Colao A. The Treatment of Cushing's Disease. Endocr Rev 2015; 36 (04) 385-486 https://pubmed.ncbi.nlm.nih.gov/26067718
- 69 Braun LT, Rubinstein G, Zopp S. et al. Recurrence after pituitary surgery in adult Cushing's disease: a systematic review on diagnosis and treatment. Endocrine 2020; 70 (02) 218-231
- 70 Johnston PC, Hamrahian AH, Prayson RA, Kennedy L, Weil RJ. Thyrotoxicosis with absence of clinical features of acromegaly in a TSH- and GH-secreting, invasive pituitary macroadenoma. Endocrinol Diabetes Metab Case Rep 2015; 2015: 140070
- 71 Lee EY, Ku CR, Kim HM. et al. A Case of Pituitary Adenoma with Simultaneous Secretion of TSH and GH. Endocrinol Metab (Seoul) 2011; 26 (02) 160-165
- 72 Berker D, Isik S, Aydin Y. et al. Thyrotropin secreting pituitary adenoma accompanying a silent somatotropinoma. Turk Neurosurg 2011; 21 (03) 403-407
- 73 Qureshi T, Chaus F, Fogg L, Dasgupta M, Straus D, Byrne RW. Learning curve for the transsphenoidal endoscopic endonasal approach to pituitary tumors. Br J Neurosurg 2016; 30 (06) 637-642
- 74 Thawani JP, Ramayya AG, Pisapia JM, Abdullah KG, Lee JY-K, Grady MS. Operative Strategies to Minimize Complications Following Resection of Pituitary Macroadenomas. J Neurol Surg B Skull Base 2017; 78 (02) 184-190 https://pubmed.ncbi.nlm.nih.gov/28321384
- 75 Lobatto DJ, de Vries F, Zamanipoor Najafabadi AH. et al. Preoperative risk factors for postoperative complications in endoscopic pituitary surgery: a systematic review. Pituitary 2018; 21 (01) 84-97
- 76 Boling CC, Karnezis TT, Baker AB. et al. Multi-institutional study of risk factors for perioperative morbidity following transnasal endoscopic pituitary adenoma surgery. Int Forum Allergy Rhinol 2016; 6 (01) 101-107
- 77 Zhang L, Chen M. Analysis of factors causing intracranial infection after endoscopic resection of pituitary tumors by transnasal-sphenoidal approach. Biomed Res 2014; 25 (04) 437-440
- 78 Komotar RJ, Starke RM, Raper DMS, Anand VK, Schwartz TH. Endoscopic endonasal compared with microscopic transsphenoidal and open transcranial resection of giant pituitary adenomas. Pituitary 2012; 15 (02) 150-159
- 79 de Paiva Neto MA, Vandergrift A, Fatemi N. et al. Endonasal transsphenoidal surgery and multimodality treatment for giant pituitary adenomas. Clin Endocrinol (Oxf) 2010; 72 (04) 512-519
- 80 Yano S, Hide T, Shinojima N. Efficacy and Complications of Endoscopic Skull Base Surgery for Giant Pituitary Adenomas. World Neurosurg 2017; 99: 533-542
- 81 Chowdhury T, Prabhakar H, Bithal PK, Schaller B, Dash HH. Immediate postoperative complications in transsphenoidal pituitary surgery: A prospective study. Saudi J Anaesth 2014; 8 (03) 335-341 https://pubmed.ncbi.nlm.nih.gov/25191182
- 82 Olson DR, Guiot G, Derome P. The symptomatic empty sella. Prevention and correction via the transsphenoidal approach. J Neurosurg 1972; 37 (05) 533-537
- 83 Thomé C, Zevgaridis D. Delayed visual deterioration after pituitary surgery–a review introducing the concept of vascular compression of the optic pathways. Acta Neurochir (Wien) 2004; 146 (10) 1131-1135 , discussion 1135–1136
- 84 Barzaghi LR, Donofrio CA, Panni P, Losa M, Mortini P. Treatment of empty sella associated with visual impairment: a systematic review of chiasmapexy techniques. Pituitary 2018; 21 (01) 98-106
- 85 Chen X, Huang W, Li H. et al. Comparison of outcomes between endoscopic and microscopic transsphenoidal surgery for the treatment of pituitary adenoma: a meta-analysis. Gland Surg 2020; 9 (06) 2162-2174 https://pubmed.ncbi.nlm.nih.gov/33447567
Address for correspondence
Publication History
Received: 10 November 2021
Accepted: 24 January 2023
Article published online:
28 June 2023
© 2023. Sociedade Brasileira de Neurocirurgia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Liu JK, Das K, Weiss MH, Laws Jr ER, Couldwell WT. The history and evolution of transsphenoidal surgery. J Neurosurg 2001; 95 (06) 1083-1096
- 2 Prevedello DM, Doglietto F, Jane Jr JAJ, Jagannathan J, Han J, Laws Jr ERJ. History of endoscopic skull base surgery: its evolution and current reality. J Neurosurg 2007; 107 (01) 206-213
- 3 Grosvenor AE, Laws ER. The evolution of extracranial approaches to the pituitary and anterior skull base. Pituitary 2008; 11 (04) 337-345
- 4 Artico M, Pastore FS, Fraioli B, Giuffrè R. The contribution of Davide Giordano (1864-1954) to pituitary surgery: the transglabellar-nasal approach. Neurosurgery 1998; 42 (04) 909-911 , discussion 911–912
- 5 Kanter AS, Dumont AS, Asthagiri AR, Oskouian RJ, Jane Jr JA, Laws Jr ER. The transsphenoidal approach. A historical perspective. Neurosurg Focus 2005; 18 (04) e6
- 6 Liu JK, Cohen-Gadol AA, Laws Jr ERJ, Cole CD, Kan P, Couldwell WT. Harvey Cushing and Oskar Hirsch: early forefathers of modern transsphenoidal surgery. J Neurosurg 2005; 103 (06) 1096-1104
- 7 Lanzino G, Laws Jr ERJ. Pioneers in the development of transsphenoidal surgery: Theodor Kocher, Oskar Hirsch, and Norman Dott. J Neurosurg 2001; 95 (06) 1097-1103
- 8 Rosegay H. Cushing's legacy to transsphenoidal surgery. J Neurosurg 1981; 54 (04) 448-454
- 9 Meyer C, Ritter F. Tumor de Hipófise: Operação de Hirsch-Segura. - Estudo neuro-clínico e oftalmologico. Rev dos Cursos. Fac Med. 1935; 21 (21) 1-23
- 10 Hardy J. Transphenoidal microsurgery of the normal and pathological pituitary. Clin Neurosurg 1969; 16: 185-217
- 11 Hardy J. Transsphenoidal hypophysectomy. J Neurosurg 1971; 34 (04) 582-594
- 12 Cavallo LM, Messina A, Cappabianca P. et al. Endoscopic endonasal surgery of the midline skull base: anatomical study and clinical considerations. Neurosurg Focus 2005; 19 (01) E2
- 13 Castelnuovo P, Dallan I, Battaglia P, Bignami M. Endoscopic endonasal skull base surgery: past, present and future. Eur Arch Otorhinolaryngol 2010; 267 (05) 649-663
- 14 Doglietto F, Prevedello DM, Jane Jr JAJ, Han J, Laws Jr ERJ. Brief history of endoscopic transsphenoidal surgery–from Philipp Bozzini to the First World Congress of Endoscopic Skull Base Surgery. Neurosurg Focus 2005; 19 (06) E3
- 15 Jankowski R, Auque J, Simon C, Marchal JC, Hepner H, Wayoff M. Endoscopic pituitary tumor surgery. Laryngoscope 1992; 102 (02) 198-202
- 16 Sethi DS, Pillay PK. Endoscopic management of lesions of the sella turcica. J Laryngol Otol 1995; 109 (10) 956-962
- 17 Jho H-D, Carrau RL. Endoscopic endonasal transsphenoidal surgery: experience with 50 patients. J Neurosurg 1997; 87 (01) 44-51 https://thejns.org/view/journals/j-neurosurg/87/1/article-p44.xml
- 18 Cappabianca P, Alfieri A, de Divitiis E. Endoscopic endonasal transsphenoidal approach to the sella: towards functional endoscopic pituitary surgery (FEPS). Minim Invasive Neurosurg 1998; 41 (02) 66-73 10.1055/s-2008-1052019
- 19 Alfieri A, Jho H-D, Tschabitscher M. Endoscopic endonasal approach to the ventral cranio-cervical junction: anatomical study. Acta Neurochir (Wien) 2002; 144 (03) 219-225 , discussion 225 http://www.ncbi.nlm.nih.gov/pubmed/11956934
- 20 Cappabianca P, Frank G, Pasquini E, de Divitiis O, Calbucci F. Extended endoscopic endonasal transsphenoidal approaches to the suprasellar region, planum sphenoidale and clivus. In: de Divitiis E, Cappabianca P. eds. Endoscopic Endonasal Transsphenoidal Surgery [Internet]. Vienna: Springer Vienna; 2003: 176-187 . Available from: https://doi.org/10.1007/978-3-7091-6084-8_11
- 21 Solari D, Morace R, Cavallo LM. et al. The endoscopic endonasal approach for the management of craniopharyngiomas. J Neurosurg Sci 2016; 60 (04) 454-462
- 22 Linsler S, Oertel J. Endoscopic Endonasal Transclival Resection of a Brainstem Cavernoma: A Detailed Account of Our Technique and Comparison with the Literature. World Neurosurg 2015; 84 (06) 2064-2071
- 23 Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R. Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 2005; 19 (01) E6
- 24 Frank G, Pasquini E, Doglietto F. et al. The endoscopic extended transsphenoidal approach for craniopharyngiomas. Neurosurgery 2006; 59 (1, Suppl 1) ONS75-ONS83 , discussion ONS75–ONS83
- 25 Snyderman C, Kassam A, Carrau R, Mintz A. Endoscopic approaches to the petrous apex. Oper Tech Otolaryngol Neck Surg. 2006; 17: 168-173
- 26 Fernandez-Miranda JC, Gardner PA, Prevedello DM, Kassam AB. Expanded endonasal approach for olfactory groove meningioma. Acta Neurochir (Wien) 2009; 151 (03) 287-288 , author reply 289–290
- 27 Dehdashti AR, Ganna A, Witterick I, Gentili F. Expanded endoscopic endonasal approach for anterior cranial base and suprasellar lesions: indications and limitations. Neurosurgery 2009; 64 (04) 677-687 , discussion 687–689
- 28 Shin M, Kondo K, Saito N. Current Status of Endoscopic Endonasal Surgery for Skull Base Meningiomas: Review of the Literature. Neurol Med Chir (Tokyo) 2015; 55 (09) 735-743 https://pubmed.ncbi.nlm.nih.gov/26345667
- 29 Mangussi-Gomes J, Beer-Furlan A, Balsalobre L, Vellutini EAS, Stamm AC. Endoscopic Endonasal Management of Skull Base Chordomas: Surgical Technique, Nuances, and Pitfalls. Otolaryngol Clin North Am 2016; 49 (01) 167-182
- 30 Zoli M, Milanese L, Bonfatti R. et al. Clival chordomas: considerations after 16 years of endoscopic endonasal surgery. J Neurosurg 2018; 128 (02) 329-338
- 31 Hammer G, Rådberg C. The sphenoidal sinus. An anatomical and roentgenologic study with reference to transsphenoid hypophysectomy. Acta Radiol 1961; 56 (06) 401-422 https://journals.sagepub.com/doi/abs/10.1177/028418516105600601
- 32 Hardy J, Vezina JL. Transsphenoidal neurosurgery of intracranial neoplasm. Adv Neurol 1976; 15: 261-273
- 33 Knosp E, Steiner E, Kitz K, Matula C. Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery 1993; 33 (04) 610-617 , discussion 617–618
- 34 Li H-Y, Feng C-Y, Zhang C. et al. Microscopic surgery for pituitary adenomas to preserve the pituitary gland and stalk. Exp Ther Med 2017; 13 (03) 1011-1016
- 35 Gandhi CD, Christiano LD, Eloy JA, Prestigiacomo CJ, Post KD. The historical evolution of transsphenoidal surgery: facilitation by technological advances. Neurosurg Focus 2009; 27 (03) E8
- 36 Theodros D, Patel M, Ruzevick J, Lim M, Bettegowda C. Pituitary adenomas: historical perspective, surgical management and future directions. CNS Oncol 2015; 4 (06) 411-429
- 37 Yu S-Y, Du Q, Yao S-Y. et al. Outcomes of endoscopic and microscopic transsphenoidal surgery on non-functioning pituitary adenomas: a systematic review and meta-analysis. J Cell Mol Med 2018; 22 (03) 2023-2027 https://pubmed.ncbi.nlm.nih.gov/29314715
- 38 White DR, Sonnenburg RE, Ewend MG, Senior BA. Safety of minimally invasive pituitary surgery (MIPS) compared with a traditional approach. Laryngoscope 2004; 114 (11) 1945-1948
- 39 Nishioka H. Recent Evolution of Endoscopic Endonasal Surgery for Treatment of Pituitary Adenomas. Neurol Med Chir (Tokyo) 2017; 57 (04) 151-158 https://pubmed.ncbi.nlm.nih.gov/28239067
- 40 O'Malley Jr BWJ, Grady MS, Gabel BC. et al. Comparison of endoscopic and microscopic removal of pituitary adenomas: single-surgeon experience and the learning curve. Neurosurg Focus 2008; 25 (06) E10
- 41 Cappabianca P, Cavallo LM, Solari D, Stagno V, Esposito F, de Angelis M. Endoscopic endonasal surgery for pituitary adenomas. World Neurosurg 2014; 82 (06) S3-S11
- 42 Tabaee A, Anand VK, Barrón Y. et al. Predictors of short-term outcomes following endoscopic pituitary surgery. Clin Neurol Neurosurg 2009; 111 (02) 119-122
- 43 Jain AK, Gupta AK, Pathak A, Bhansali A, Bapuraj JR. Endonasal transsphenoidal pituitary surgery: is tumor volume a key factor in determining outcome?. Am J Otolaryngol 2008; 29 (01) 48-50
- 44 Esposito D, Olsson DS, Ragnarsson O, Buchfelder M, Skoglund T, Johannsson G. Non-functioning pituitary adenomas: indications for pituitary surgery and post-surgical management. Pituitary 2019; 22 (04) 422-434
- 45 Penn DL, Burke WT, Laws ER. Management of non-functioning pituitary adenomas: surgery. Pituitary 2018; 21 (02) 145-153
- 46 Dekkers OM, Pereira AM, Roelfsema F. et al. Observation alone after transsphenoidal surgery for nonfunctioning pituitary macroadenoma. J Clin Endocrinol Metab 2006; 91 (05) 1796-1801
- 47 Wichers-Rother M, Hoven S, Kristof RA, Bliesener N, Stoffel-Wagner B. Non-functioning pituitary adenomas: endocrinological and clinical outcome after transsphenoidal and transcranial surgery. Exp Clin Endocrinol Diabetes 2004; 112 (06) 323-327
- 48 Murad MH, Fernández-Balsells MM, Barwise A. et al. Outcomes of surgical treatment for nonfunctioning pituitary adenomas: a systematic review and meta-analysis. Clin Endocrinol (Oxf) 2010; 73 (06) 777-791
- 49 Wang F, Zhou T, Wei S. et al. Endoscopic endonasal transsphenoidal surgery of 1,166 pituitary adenomas. Surg Endosc 2015; 29 (06) 1270-1280
- 50 Gondim JA, Schops M, de Almeida JPC. et al. Endoscopic endonasal transsphenoidal surgery: surgical results of 228 pituitary adenomas treated in a pituitary center. Pituitary 2010; 13 (01) 68-77
- 51 Cappabianca P, Cavallo LM, de Divitiis E. Endoscopic endonasal transsphenoidal surgery. Neurosurgery 2004; 55 (04) 933-940 , discussion 940–941
- 52 Kim JH, Lee JH, Lee JH, Hong AR, Kim YJ, Kim YH. Endoscopic Transsphenoidal Surgery Outcomes in 331 Nonfunctioning Pituitary Adenoma Cases After a Single Surgeon Learning Curve. World Neurosurg 2018; 109: e409-e416
- 53 Torales J, Halperin I, Hanzu F. et al. Endoscopic endonasal surgery for pituitary tumors. Results in a series of 121 patients operated at the same center and by the same neurosurgeon. Endocrinol Nutr 2014; 61 (08) 410-416
- 54 Dehdashti AR, Ganna A, Karabatsou K, Gentili F. Pure endoscopic endonasal approach for pituitary adenomas: early surgical results in 200 patients and comparison with previous microsurgical series. Neurosurgery 2008; 62 (05) 1006-1015 , discussion 1015–1017
- 55 Bokhari AR, Davies MA, Diamond T. Endoscopic transsphenoidal pituitary surgery: a single surgeon experience and the learning curve. Br J Neurosurg 2013; 27 (01) 44-49
- 56 Ciric I, Ragin A, Baumgartner C, Pierce D. Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery 1997; 40 (02) 225-236 , discussion 236–237
- 57 Micko ASG, Wöhrer A, Wolfsberger S, Knosp E. Invasion of the cavernous sinus space in pituitary adenomas: endoscopic verification and its correlation with an MRI-based classification. J Neurosurg 2015; 122 (04) 803-811
- 58 Maletkovic J, Dabbagh A, Zhang D. et al. Residual Tumor Confers a 10-Fold Increased Risk of Regrowth in Clinically Nonfunctioning Pituitary Tumors. J Endocr Soc 2019; 3 (10) 1931-1941
- 59 Roelfsema F, Biermasz NR, Pereira AM. Clinical factors involved in the recurrence of pituitary adenomas after surgical remission: a structured review and meta-analysis. Pituitary 2012; 15 (01) 71-83 https://pubmed.ncbi.nlm.nih.gov/21918830
- 60 Almeida JP, Ruiz-Treviño AS, Liang B. et al. Reoperation for growth hormone-secreting pituitary adenomas: report on an endonasal endoscopic series with a systematic review and meta-analysis of the literature. J Neurosurg 2018; 129 (02) 404-416
- 61 Nomikos P, Buchfelder M, Fahlbusch R. The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical ‘cure’. Eur J Endocrinol 2005; 152 (03) 379-387
- 62 Han Y-L, Chen D-M, Zhang C, Pan M, Yang X-P, Wu Y-G. Retrospective analysis of 52 patients with prolactinomas following endoscopic endonasal transsphenoidal surgery. Medicine (Baltimore) 2018; 97 (45) e13198-e13198 https://pubmed.ncbi.nlm.nih.gov/30407358
- 63 Zielinski G, Ozdarski M, Maksymowicz M, Szamotulska K, Witek P. Prolactinomas: Prognostic Factors of Early Remission After Transsphenoidal Surgery. Front Endocrinol (Lausanne) 2020; 11: 439
- 64 Donoho DA, Laws Jr ER. The Role of Surgery in the Management of Prolactinomas. Neurosurg Clin N Am 2019; 30 (04) 509-514
- 65 Akinduro OO, Lu VM, Izzo A. et al. Radiographic and Hormonal Regression in Prolactinomas: An Analysis of Treatment Failure. World Neurosurg 2019; 129: e686-e694
- 66 Ferriere A, Tabarin A. Cushing's syndrome: Treatment and new therapeutic approaches. Best Pract Res Clin Endocrinol Metab 2020; 34 (02) 101381
- 67 Patil CG, Prevedello DM, Lad SP. et al. Late recurrences of Cushing's disease after initial successful transsphenoidal surgery. J Clin Endocrinol Metab 2008; 93 (02) 358-362
- 68 Pivonello R, De Leo M, Cozzolino A, Colao A. The Treatment of Cushing's Disease. Endocr Rev 2015; 36 (04) 385-486 https://pubmed.ncbi.nlm.nih.gov/26067718
- 69 Braun LT, Rubinstein G, Zopp S. et al. Recurrence after pituitary surgery in adult Cushing's disease: a systematic review on diagnosis and treatment. Endocrine 2020; 70 (02) 218-231
- 70 Johnston PC, Hamrahian AH, Prayson RA, Kennedy L, Weil RJ. Thyrotoxicosis with absence of clinical features of acromegaly in a TSH- and GH-secreting, invasive pituitary macroadenoma. Endocrinol Diabetes Metab Case Rep 2015; 2015: 140070
- 71 Lee EY, Ku CR, Kim HM. et al. A Case of Pituitary Adenoma with Simultaneous Secretion of TSH and GH. Endocrinol Metab (Seoul) 2011; 26 (02) 160-165
- 72 Berker D, Isik S, Aydin Y. et al. Thyrotropin secreting pituitary adenoma accompanying a silent somatotropinoma. Turk Neurosurg 2011; 21 (03) 403-407
- 73 Qureshi T, Chaus F, Fogg L, Dasgupta M, Straus D, Byrne RW. Learning curve for the transsphenoidal endoscopic endonasal approach to pituitary tumors. Br J Neurosurg 2016; 30 (06) 637-642
- 74 Thawani JP, Ramayya AG, Pisapia JM, Abdullah KG, Lee JY-K, Grady MS. Operative Strategies to Minimize Complications Following Resection of Pituitary Macroadenomas. J Neurol Surg B Skull Base 2017; 78 (02) 184-190 https://pubmed.ncbi.nlm.nih.gov/28321384
- 75 Lobatto DJ, de Vries F, Zamanipoor Najafabadi AH. et al. Preoperative risk factors for postoperative complications in endoscopic pituitary surgery: a systematic review. Pituitary 2018; 21 (01) 84-97
- 76 Boling CC, Karnezis TT, Baker AB. et al. Multi-institutional study of risk factors for perioperative morbidity following transnasal endoscopic pituitary adenoma surgery. Int Forum Allergy Rhinol 2016; 6 (01) 101-107
- 77 Zhang L, Chen M. Analysis of factors causing intracranial infection after endoscopic resection of pituitary tumors by transnasal-sphenoidal approach. Biomed Res 2014; 25 (04) 437-440
- 78 Komotar RJ, Starke RM, Raper DMS, Anand VK, Schwartz TH. Endoscopic endonasal compared with microscopic transsphenoidal and open transcranial resection of giant pituitary adenomas. Pituitary 2012; 15 (02) 150-159
- 79 de Paiva Neto MA, Vandergrift A, Fatemi N. et al. Endonasal transsphenoidal surgery and multimodality treatment for giant pituitary adenomas. Clin Endocrinol (Oxf) 2010; 72 (04) 512-519
- 80 Yano S, Hide T, Shinojima N. Efficacy and Complications of Endoscopic Skull Base Surgery for Giant Pituitary Adenomas. World Neurosurg 2017; 99: 533-542
- 81 Chowdhury T, Prabhakar H, Bithal PK, Schaller B, Dash HH. Immediate postoperative complications in transsphenoidal pituitary surgery: A prospective study. Saudi J Anaesth 2014; 8 (03) 335-341 https://pubmed.ncbi.nlm.nih.gov/25191182
- 82 Olson DR, Guiot G, Derome P. The symptomatic empty sella. Prevention and correction via the transsphenoidal approach. J Neurosurg 1972; 37 (05) 533-537
- 83 Thomé C, Zevgaridis D. Delayed visual deterioration after pituitary surgery–a review introducing the concept of vascular compression of the optic pathways. Acta Neurochir (Wien) 2004; 146 (10) 1131-1135 , discussion 1135–1136
- 84 Barzaghi LR, Donofrio CA, Panni P, Losa M, Mortini P. Treatment of empty sella associated with visual impairment: a systematic review of chiasmapexy techniques. Pituitary 2018; 21 (01) 98-106
- 85 Chen X, Huang W, Li H. et al. Comparison of outcomes between endoscopic and microscopic transsphenoidal surgery for the treatment of pituitary adenoma: a meta-analysis. Gland Surg 2020; 9 (06) 2162-2174 https://pubmed.ncbi.nlm.nih.gov/33447567