

Subscribe to RSS
DOI: 10.1055/s-0043-1769014
Increased Levels of Inflammatory and Endothelial Biomarkers in Blood of Long COVID Patients Point to Thrombotic Endothelialitis
Authors
Abstract
The prevailing hypotheses for the persistent symptoms of Long COVID have been narrowed down to immune dysregulation and autoantibodies, widespread organ damage, viral persistence, and fibrinaloid microclots (entrapping numerous inflammatory molecules) together with platelet hyperactivation. Here we demonstrate significantly increased concentrations of von Willebrand factor (VWF), platelet factor 4 (PF4), serum amyloid A (SAA), α-2 antiplasmin (α-2AP), endothelial-leukocyte adhesion molecule 1 (E-selectin), and platelet endothelial cell adhesion molecule (PECAM-1) in the soluble part of the blood. It was noteworthy that the mean level of α-2 antiplasmin exceeded the upper limit of the laboratory reference range in Long COVID patients, and the other 5 were significantly elevated in Long COVID patients as compared to the controls. This is alarming if we take into consideration that a significant amount of the total burden of these inflammatory molecules has previously been shown to be entrapped inside fibrinolysis-resistant microclots (thus decreasing the apparent level of the soluble molecules). We conclude that presence of microclotting, together with relatively high levels of six biomarkers known to be key drivers of endothelial and clotting pathology, points to thrombotic endothelialitis as a key pathological process in Long COVID.
Keywords
long COVID - von Willebrand factor - platelet factor 4 - serum amyloid A - α2-antiplasmin - E-selectin - PECAM-1 - thrombotic endothelialitisLong COVID is a major global health burden, with a significant impact on physical and cognitive function, health-related quality of life, and participation in society.[1] [2] [3] [4] [5] [6] The potential mechanisms for the persistent symptoms in Long COVID include (1) viral persistence, (2) microclotting and platelet hyperactivation, (3) autoantibodies, (4) immune dysregulation, (5) widespread organ damage, (6) possible reactivation of dormant viruses,[7] [8] and (7) hypothetical integration of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) sequences in genomes of infected cells.[9] We have demonstrated that individuals with Long COVID have a significant fibrin amyloid microclot load in their circulation.[1] [7] These clots can also be induced in normal plasma by (recombinant) SARS-CoV-2 spike protein[10] and they are resistant to fibrinolysis.[1] [7] Trapped inside these fibrinolysis-resistant microclots are numerous inflammatory and endothelial molecules, including α-2 antiplasmin (α-2AP), various fibrinogen chains, von Willebrand factor (VWF), platelet factor 4 (PF4), serum amyloid A (SAA), as well as multiple antibodies.[1] [7] Although characterizing the inflammatory and endothelial molecule content of the fibrinolytic-resistant microclots is of considerable interest and academic value[1] [7] patients need more readily accessible diagnostic markers available in general pathology laboratories.
We undertook this study to identify six biomarker molecules in the soluble fraction of blood which could be used as part of a blood pathology testing suite to confirm the presence of inflammation, endothelial damage, and dysregulated coagulation. Such tests could assist clinicians to determine if there is clotting and/or vascular damage risk in an individual suffering from Long COVID. Four of the soluble molecules chosen had already been found trapped inside solubilized microclots[1] [7] and they are VWF, PF4, SAA, and α-2AP; another two specific endothelial-damage marker molecules—endothelial-leukocyte adhesion molecule 1 (E-selectin) and the platelet endothelial cell adhesion molecule 1 (PECAM-1)—were selected for the study. All six molecules have numerous receptors on platelets and endothelial cells and could potentially have direct protein–protein interactions with the plasma protein fibrinogen.
Unfortunately, a major pitfall in the diagnosis of Long COVID is that most—if not all—standard pathology tests do not yield abnormal results. We believe that this could be because most of the inflammatory molecules are entrapped in the microclots, and not necessarily in the soluble fraction of the blood. We have previously demonstrated this using proteomics analysis of the microclots.[1] [7] Although D-dimer is commonly used to evaluate clotting disorders, it is a product of fibrin degradation. Hence, it is elevated only when there is clot breakdown. In our previous publications, we have noted that the microclots in Long COVID are extremely resistant to clot breakdown (fibrinolysis).[1] [7] The D-dimer often comes back normal in Long COVID patients for this exact reason. Therefore, we opted to explore other markers.
If these markers were to be implemented in a clinical environment, additional research and validation would be required. Nevertheless, with this preliminary study, we hope to demonstrate that these markers have the potential to be useful indicators of Long COVID.
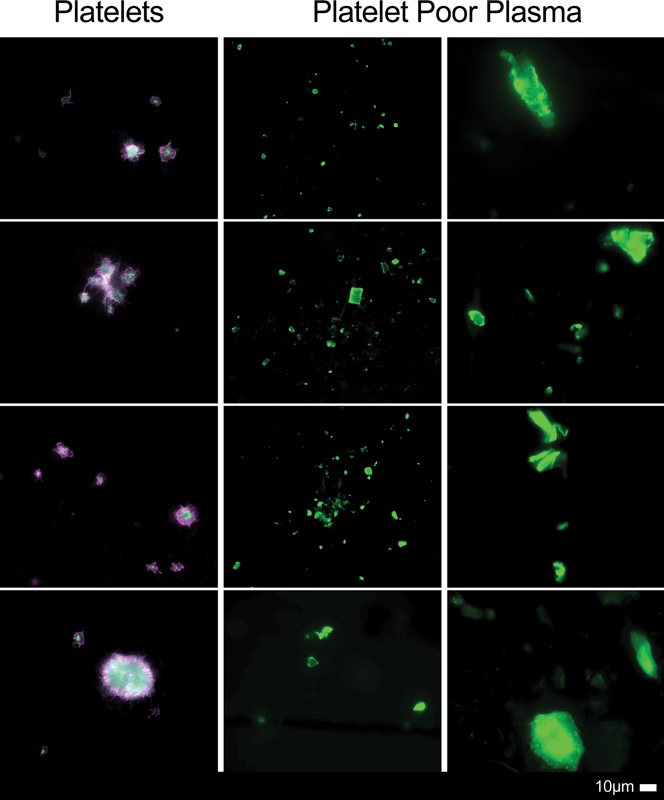
Ethical clearance for the study was obtained from the Health Research Ethics Committee (HREC) of Stellenbosch University (South Africa). Blood samples of 15 healthy individuals and 25 individuals with Long COVID were analyzed (for demographics, see [Table 1]). SAA was measured using Abcam's Human SAA ELISA Kit (ab100635) using a dilution factor of 500× (CV = 0.9%). α-2AP was measured using Abcam's Human α2-antiplasmin SimpleStep ELISA Kit (ab254502) using a dilution factor of 20,000× (CV = 0.94%). PF4 was measured using Elabscience's Human PF4 ELISA Kit (E-EL-H6107) with a dilution factor of 10× (CV = 0.9%). E-selectin was measured using Elabscience's E-selectin ELISA Kit (E-EL-H0876) with a dilution factor of 20× (CV = 1.68%). PECAM was measured using Elabscience's PECAM ELISA Kit (E-EL-H1640) with a dilution factor of 50× (CV = 1.7%). Only PECAM-1 and E-selectin were measured using serum; the rest of the molecules were measured using platelet-poor plasma (PPP). VWF was analyzed by PathCare, a pathology services laboratory (South Africa). We chose to test for VWF % antigen at PathCare, as VWF is the only molecule out of the six inflammatory molecules which is a standard test that can be performed in a pathology laboratory. This also makes the test more accessible to patients and doctors. For sample analysis, Siemens VWF Ag reagent was used for the immunoturbidimetric determination, using the Sysmex CS2500 instrument. Approximately 0.5 mL of PPP was utilized for the analysis. The Sysmex CS2500 instrument was calibrated according to standard protocol and the facility is accredited in accordance with the international ISO 15189:2012 standard. We also assessed the presence of microclots and platelet hyperactivation in Long COVID patients by adding thioflavin T to PPP and PAC-1 and CD62P to the hematocrit samples[1] (see [Supplementary Material] for protocol [available in the online version only]).
Abbreviations: α-2AP, α-2 antiplasmin; COPD, chronic obstructive pulmonary disease; PASC, post-acute sequelae of COVID-19; PECAM-1, platelet endothelial cell adhesion molecule 1; PF4, platelet factor 4; PPP, platelet-poor plasma; SAA, serum amyloid A; SD, standard deviation; VWF, von Willebrand factor.
All six molecules were significantly upregulated in the soluble part of the blood (serum and plasma) in individuals with Long COVID when compared to healthy participants (see [Table 1]). All individuals with Long COVID showed microclot formation and significant platelet hyperactivation, as shown in [Fig. 1]. Most of our healthy patient cohort had previously experienced acute COVID-19 but were fully recovered.
We argue that while there may be many mechanisms at play in the pathogenesis of Long COVID, the common pathological process is a thrombotic endothelialitis. This is characterized by formation of anomalous fibrinaloid microclots, hyperactivated platelets, endothelialitis, and elevated levels of prothrombotic inflammatory molecules. These molecules interact with each other as well as with platelets, circulating immune cells and the endothelium. It has already been demonstrated that Long COVID patients have endothelialitis, together with an increased risk of thrombosis.[11] [12] [13] As mentioned previously, there may be various mechanisms involved in the genesis of the thrombotic endothelialitis and the formation of microlots, including viral persistence and immune dysregulation.[14] [15] [16] [17]
Detailed proteomics analysis has previously revealed several-fold increased concentrations of inflammatory and endothelial molecules trapped within the microclots. The concentration of these inflammatory and endothelial molecules in the soluble fraction of the blood is alarming if we take into consideration that a significant proportion of the total burden of these molecules is trapped inside fibrinolysis-resistant microclots.[1] [7]
Over the years, we have shown that there are differences in clotting abnormalities in various diseases when compared to controls.[18] [19] [20] [21] An increase in inflammatory molecules in digested plasma from type 2 diabetes mellitus (T2DM) patients has been noted, but not to the same extent as found trapped inside the digested microclots in long COVID.[1] In that study,[1] as well as in a further follow-up one,[7] we utilized proteomics to examine plasma proteins in controls, T2DM, acute COVID-19, and Long COVID. We found that microclots in Long COVID exhibited a considerably higher number of trapped plasma proteins in comparison to the other groups. Furthermore, we observed that SAA, VWF, PF4, and α-2AP were notably elevated in Long COVID relative to the other groups. The number and size of microclots is also significantly greater in Long COVID as compared to acute COVID and T2DM.[1] Furthermore, Long COVID microclots are resistant to a single trypsinization, unlike those in T2DM.[1] We have also shown differences in the clotting pathology between different COVID-19 variants.[22]
Microclots have the potential to become a diagnostic marker for Long COVID. Unfortunately, both fluorescence microscopy and proteomics are complex techniques usually available only in research facilities and not in clinical laboratories. To establish the clinical use of microclots as a diagnostic marker, larger sample sizes and further validation studies will need to be conducted. The development of general pathology laboratory methods such as flow cytometry to detect these clots in blood samples will also need to be explored.
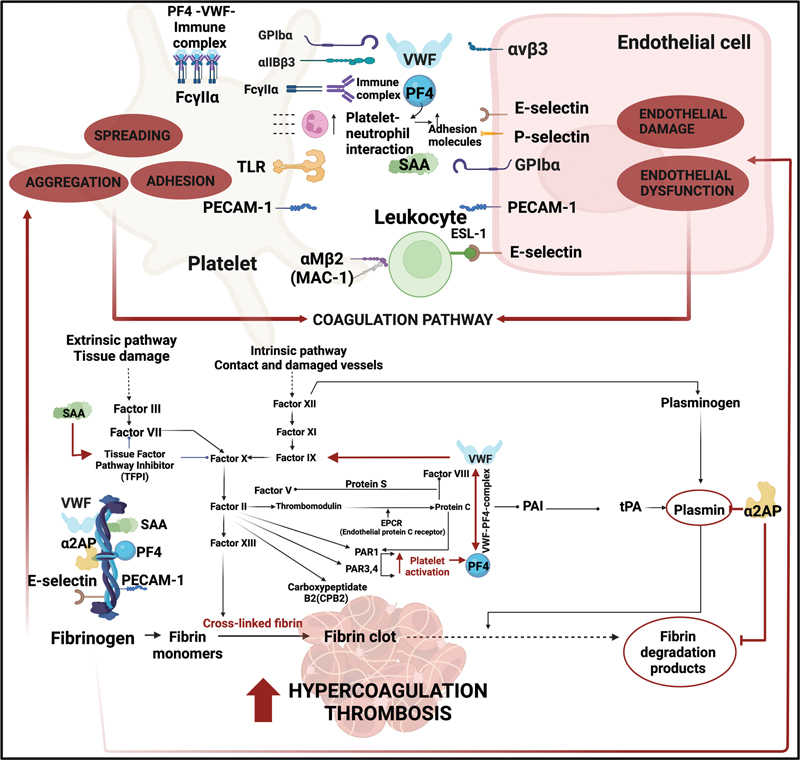
We argue that such a microclot detection method, together with the demonstration of relatively high levels of the six molecules described in this article, would be good evidence for the presence of an ongoing thrombotic endothelialitis in individuals with Long COVID. Each of the individual molecules can cause significant endothelial dysfunction and platelet activation, ultimately resulting in severe clotting imbalance and endothelial pathology. [Fig. 2] provides an overview diagram of the receptors and signaling pathways of our chosen molecules.
Given the significant increase in rates of thrombotic events following even mild[4] COVID-19 on a background of reports of endothelial cell infection and endothelialitis in acute[23] COVID-19, it is imperative that the thrombotic endothelialitis in Long COVID is investigated and treated urgently. The optimal therapeutic regimen is yet to be defined pending clinical trial data; however, given the complex pathophysiology, this is likely to incorporate antiplatelet drugs, as well as agents acting on the enzymatic pathway of coagulation.
In summary, the presence of fibrinaloid microclots and multiple inflammatory and endothelial molecules in the soluble part of blood points to thrombotic endothelialitis as a key pathological process in Long COVID.
This was a preliminary study with a limited sample size. Furthermore, it should be noted that the time from recovery varied among the individuals in the study; as a result, the detection time for these biomarkers was not uniform or consistent across all individuals. One other potential use of these biomarkers may be in tracking the response to treatment (anticoagulation). It may not be feasible to follow the response to treatment by repeated microscopic demonstration of microclots. However, the improvement in coagulopathy could potentially be measured by tracking these molecules. This could be the subject of a future therapeutic study.
Further research should aim to expand the sample size and consider comparing biomarker levels in both acute COVID patients and those recovering from Long COVID. It is also recommended that future research endeavors aim to explore the interrelatedness of these molecules.
Conflict of Interest
E.P. is themanaging director of Biocode Technologies. The other authors have no competing interests to declare. The funders had no role in the design of the study; in the collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Institutional Review Board Approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Stellenbosch University (B21/03/001_ COVID-19, project ID: 21911 [Long COVID Registry] and N19/03/043, project ID 9521 with yearly re-approval). Participants were either recruited via the Long COVID registry or identified from our clinical collaborator's practice. The experimental objectives, risks, and details were explained to volunteers and informed consent was obtained prior to blood collection. Strict compliance to ethical guidelines and principles of the Declaration of Helsinki, South African Guidelines for Good Clinical Practice, and Medical Research Council Ethical Guidelines for Research were kept for the duration of the study and for all research protocols.
Informed Consent Statement
Informed consent was obtained from all individuals involved in the study.
Authors' Contributions
Conceptualization: E.P. and D.B.K.
Methodologies: S.T., E.P., C.A.N., T.J.U.
Sample curation: C.V.
Clinician input: G.J.L., A.K., and M.A.K.
Writing of the manuscript: E.P. and S.T.
All authors reviewed and edited the manuscript.
-
References
- 1 Pretorius E, Vlok M, Venter C. et al. Persistent clotting protein pathology in long COVID/post-acute sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol 2021; 20 (01) 172
- 2 Proal AD, VanElzakker MB. Long COVID or post-acute sequelae of COVID-19 (PASC): an overview of 1 biological factors that may contribute to persistent symptoms. Front Microbiol 2021; 12: 698169
- 3 Davis HE, Assaf GS, McCorkell L. et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021; 38: 101019
- 4 Al-Aly Z, Bowe B, Xie Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med 2022; 28 (07) 1461-1467
- 5 Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med 2022; 28 (03) 583-590
- 6 Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 2023; 21: 133-146
- 7 Kruger A, Vlok M, Turner S. et al. Proteomics of fibrin amyloid microclots in long COVID/post-acute sequelae of COVID-19 (PASC) shows many entrapped pro-inflammatory molecules that may also contribute to a failed fibrinolytic system. Cardiovasc Diabetol 2022; 21 (01) 190
- 8 GAO. Science, Technology Assessment, and Analytics: Science & Tech Spotlight: Long COVID. Accessed September 2022 at https://www.gao.gov/assets/gao-22-105666.pdf
- 9 Zhang L, Richards A, Barrasa MI, Hughes SH, Young RA, Jaenisch R. Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues. Proc Natl Acad Sci USA 2021; 118 (21) e2105968118
- 10 Grobbelaar LM, Venter C, Vlok M. et al. SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19. Biosci Rep 2021; 41 (08) BSR20210611
- 11 Oikonomou E, Souvaliotis N, Lampsas S. et al. Endothelial dysfunction in acute and long standing COVID-19: a prospective cohort study. Vascul Pharmacol 2022; 144: 106975
- 12 Jing H, Wu X, Xiang M, Liu L, Novakovic VA, Shi J. Pathophysiological mechanisms of thrombosis in acute and long COVID-19. Front Immunol 2022; 13: 992384
- 13 Wang C, Yu C, Jing H. et al. Long COVID: the nature of thrombotic sequelae determines the necessity of early anticoagulation. Front Cell Infect Microbiol 2022; 12: 861703
- 14 Kell DB, Pretorius E. The potential role of ischaemia-reperfusion injury in chronic, relapsing diseases such as rheumatoid arthritis, Long COVID, and ME/CFS: evidence, mechanisms, and therapeutic implications. Biochem J 2022; 479 (16) 1653-1708
- 15 Buonsenso D, Piazza M, Boner AL, Bellanti JA. Long COVID: a proposed hypothesis-driven model of viral persistence for the pathophysiology of the syndrome. Allergy Asthma Proc 2022; 43 (03) 187-193
- 16 Bussani R, Zentilin L, Correa R. et al. Persistent SARS-CoV-2 infection in patients seemingly recovered from COVID-19. J Pathol 2023; 259 (03) 254-263
- 17 Turner S, Khan MA, Putrino D, Woodcock A, Kell DB, Pretorius E. Long COVID: pathophysiological factors and abnormalities of coagulation. Trends Endocrinol Metab 2023; 34 (06) 321-344
- 18 Pretorius E, Page MJ, Engelbrecht L, Ellis GC, Kell DB. Substantial fibrin amyloidogenesis in type 2 diabetes assessed using amyloid-selective fluorescent stains. Cardiovasc Diabetol 2017; 16 (01) 141
- 19 de Waal GM, de Villiers WJS, Forgan T, Roberts T, Pretorius E. Colorectal cancer is associated with increased circulating lipopolysaccharide, inflammation and hypercoagulability. Sci Rep 2020; 10 (01) 8777
- 20 de Waal GM, Engelbrecht L, Davis T, de Villiers WJS, Kell DB, Pretorius E. Correlative light-electron microscopy detects lipopolysaccharide and its association with fibrin fibres in Parkinson's disease, Alzheimer's disease and type 2 diabetes mellitus. Sci Rep 2018; 8 (01) 16798
- 21 Pretorius E, Page MJ, Mbotwe S, Kell DB. Lipopolysaccharide-binding protein (LBP) can reverse the amyloid state of fibrin seen or induced in Parkinson's disease. PLoS One 2018; 13 (03) e0192121
- 22 Grobbelaar LM, Kruger A, Venter C. et al. Relative hypercoagulopathy of the SARS-CoV-2 beta and delta variants when compared to the less severe omicron variants is related to TEG parameters, the extent of fibrin amyloid microclots, and the severity of clinical illness. Semin Thromb Hemost 2022; 48 (07) 858-868
- 23 Varga Z, Flammer AJ, Steiger P. et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020; 395 (10234): 1417-1418
Address for correspondence
Publication History
Article published online:
19 May 2023
© 2023. Thieme. All rights reserved.
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Pretorius E, Vlok M, Venter C. et al. Persistent clotting protein pathology in long COVID/post-acute sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol 2021; 20 (01) 172
- 2 Proal AD, VanElzakker MB. Long COVID or post-acute sequelae of COVID-19 (PASC): an overview of 1 biological factors that may contribute to persistent symptoms. Front Microbiol 2021; 12: 698169
- 3 Davis HE, Assaf GS, McCorkell L. et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021; 38: 101019
- 4 Al-Aly Z, Bowe B, Xie Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med 2022; 28 (07) 1461-1467
- 5 Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med 2022; 28 (03) 583-590
- 6 Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 2023; 21: 133-146
- 7 Kruger A, Vlok M, Turner S. et al. Proteomics of fibrin amyloid microclots in long COVID/post-acute sequelae of COVID-19 (PASC) shows many entrapped pro-inflammatory molecules that may also contribute to a failed fibrinolytic system. Cardiovasc Diabetol 2022; 21 (01) 190
- 8 GAO. Science, Technology Assessment, and Analytics: Science & Tech Spotlight: Long COVID. Accessed September 2022 at https://www.gao.gov/assets/gao-22-105666.pdf
- 9 Zhang L, Richards A, Barrasa MI, Hughes SH, Young RA, Jaenisch R. Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues. Proc Natl Acad Sci USA 2021; 118 (21) e2105968118
- 10 Grobbelaar LM, Venter C, Vlok M. et al. SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19. Biosci Rep 2021; 41 (08) BSR20210611
- 11 Oikonomou E, Souvaliotis N, Lampsas S. et al. Endothelial dysfunction in acute and long standing COVID-19: a prospective cohort study. Vascul Pharmacol 2022; 144: 106975
- 12 Jing H, Wu X, Xiang M, Liu L, Novakovic VA, Shi J. Pathophysiological mechanisms of thrombosis in acute and long COVID-19. Front Immunol 2022; 13: 992384
- 13 Wang C, Yu C, Jing H. et al. Long COVID: the nature of thrombotic sequelae determines the necessity of early anticoagulation. Front Cell Infect Microbiol 2022; 12: 861703
- 14 Kell DB, Pretorius E. The potential role of ischaemia-reperfusion injury in chronic, relapsing diseases such as rheumatoid arthritis, Long COVID, and ME/CFS: evidence, mechanisms, and therapeutic implications. Biochem J 2022; 479 (16) 1653-1708
- 15 Buonsenso D, Piazza M, Boner AL, Bellanti JA. Long COVID: a proposed hypothesis-driven model of viral persistence for the pathophysiology of the syndrome. Allergy Asthma Proc 2022; 43 (03) 187-193
- 16 Bussani R, Zentilin L, Correa R. et al. Persistent SARS-CoV-2 infection in patients seemingly recovered from COVID-19. J Pathol 2023; 259 (03) 254-263
- 17 Turner S, Khan MA, Putrino D, Woodcock A, Kell DB, Pretorius E. Long COVID: pathophysiological factors and abnormalities of coagulation. Trends Endocrinol Metab 2023; 34 (06) 321-344
- 18 Pretorius E, Page MJ, Engelbrecht L, Ellis GC, Kell DB. Substantial fibrin amyloidogenesis in type 2 diabetes assessed using amyloid-selective fluorescent stains. Cardiovasc Diabetol 2017; 16 (01) 141
- 19 de Waal GM, de Villiers WJS, Forgan T, Roberts T, Pretorius E. Colorectal cancer is associated with increased circulating lipopolysaccharide, inflammation and hypercoagulability. Sci Rep 2020; 10 (01) 8777
- 20 de Waal GM, Engelbrecht L, Davis T, de Villiers WJS, Kell DB, Pretorius E. Correlative light-electron microscopy detects lipopolysaccharide and its association with fibrin fibres in Parkinson's disease, Alzheimer's disease and type 2 diabetes mellitus. Sci Rep 2018; 8 (01) 16798
- 21 Pretorius E, Page MJ, Mbotwe S, Kell DB. Lipopolysaccharide-binding protein (LBP) can reverse the amyloid state of fibrin seen or induced in Parkinson's disease. PLoS One 2018; 13 (03) e0192121
- 22 Grobbelaar LM, Kruger A, Venter C. et al. Relative hypercoagulopathy of the SARS-CoV-2 beta and delta variants when compared to the less severe omicron variants is related to TEG parameters, the extent of fibrin amyloid microclots, and the severity of clinical illness. Semin Thromb Hemost 2022; 48 (07) 858-868
- 23 Varga Z, Flammer AJ, Steiger P. et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020; 395 (10234): 1417-1418