

Subscribe to RSS
DOI: 10.1055/s-0043-1768038
Definitive Surgery after Neoadjuvant Chemotherapy for Locally Advanced Oral Cavity Cancers: Experience from a Tertiary Care Center
Authors
Funding None.

Abstract


Background Oral cavity cancers require definitive surgical resection as the primary treatment, but with advanced T stage, complete resection with pathologically negative margins might be difficult to achieve. Induction chemotherapy helps achieve the balance between resection and morbidity in locally advanced technically unresectable tumors. The aim of this study was to analyze the impact of surgery in locally advanced, technically unresectable oral cavity cancers after neoadjuvant chemotherapy (NACT).
Materials and Methods A retrospective analysis of patients with borderline resectable, locally advanced oral cavity cancers who were given NACT between February 2017 and December 2021 was conducted. Data regarding clinical and pathological characteristics, NACT, surgery, adjuvant therapy, and recurrences was analyzed.
Results Of the 69 patients in the study, 69.6% had tongue cancer, rest were gingivobuccal complex cancers. All tumors were resected based on the post-NACT tumor volume and clear margins were achieved in 42% of cases. About 85.4% of the tongue cancers required a lesser resection than anticipated, thereby following the concept of organ and functional preservation post-NACT as proposed by Licitra et al. About 30.4% had ypT0 and 17.4% had ypN0. Recurrence and survival rates noted in our study were comparable to those reported in literature. Lymph node density of more than or equal to 0.07 was found in all recurrent cases.
Conclusions Induction chemotherapy offers a chance of achieving adequate surgical resection while reducing morbidity and improving functional outcomes for patients with technically unresectable oral cavity cancers. Nodal disease may not respond to chemotherapy as well as the primary tumor. There is a need for comprehensive evaluation of prognostic factors, which could help identify the patients who will most benefit with NACT.
Keywords
oral squamous cell carcinoma - neoadjuvant chemotherapy - induction chemotherapy - oral cavity cancer - NACT - borderline resectable oral cancer - technically unresectable cancerIntroduction
Oral squamous cell carcinoma is a major disease in India, constituting 30% of our cancers. A significant proportion of this population (85%) presents with locally advanced disease,[1] [2] [3] [4] [5] [6] [7] and requires multimodality treatment. Lesions involving the masticator space and infratemporal fossa (ITF), currently classified as T4b cancers, are considered unresectable and offered radical chemoirradiation alone. Survival rates are dismal, around 10 to 40% at 1 year across multiple studies.[8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] Advanced T stage impairs the ability to attain complete surgical resection with pathologically negative margins in technically unresectable tumors.[19] [20] [21] [22] [23] Neoadjuvant chemotherapy (NACT) may cause reduction in the tumor volume, help achieve the balance between radical clearance and surgical morbidity, and may also provide a survival benefit.[24] [25] [26] [27] [28] [29] [30] [31] We present our experience with NACT for technically unresectable tumors of the oral cavity and analyze the long-term outcomes at our tertiary care center.
Materials and Methods
We present a retrospective analysis of patients with locally advanced, technically unresectable oral cavity cancer who received NACT followed by surgery and adjuvant therapy at our center between February 2017 and December 2021. Data pertaining to each patient was retrieved from our institute's electronic medical records database. All the patients were diagnosed with biopsy proven, previously untreated oral cancer. Contrast-enhanced imaging (computed tomography or magnetic resonance imaging) was employed to determine the extent of disease. Tumors with skull base invasion, prevertebral fascia involvement, or carotid artery encasement were considered unresectable. Patients with distant metastasis at the time of presentation and those who had received incomplete NACT from another center were excluded from our study. All cases were discussed in the tumor board prior to initiation of treatment.
The criteria for borderline resectability followed by the multidisciplinary tumor board, as per the best available evidence available at the time, were as follows:
-
1) Primary tumor in the oral tongue, without involvement of posterior one-third of the tongue.
-
2) Primary tumor in the buccal mucosa with infranotch ITF involvement.
-
3) Peritumoral edema extending up to the hyoid bone or zygomatic arch.
Major vessel involvement of any degree was not chosen as a criterion for borderline resectability. A smaller percentage of cases with skin infiltration from nodal disease and tumors involving the intermediate or anterior ITF were considered for neoadjuvant therapy at the surgeon's discretion after discussion in the multidisciplinary tumor board. Patients with locally advanced disease that was likely to progress with delay in surgery were also offered NACT in select situations.
The primary end-points of the study were response rates to NACT, R0 resection rates and recurrence rates noted during a minimum of 6 months of follow-up for every patient in the study. The secondary end-points were lymph node density (LND) in relation to recurrence, organ preservation rates for oral tongue carcinoma, and overall survival rates. Follow-up was continued until the end of the study period to assess overall survival of the cohort.
Neoadjuvant Chemotherapy Regimens
The NACT regimen used for each patient was individualized, depending upon the performance status (ECOG, Eastern Cooperative Oncology Group score), creatinine clearance, patient preference, and financial status. The regimens had two or three drug combinations, comprising a platinum-based agent (cisplatin or carboplatin) and either paclitaxel or docetaxel, with or without 5-fluorouracil. The number of cycles ranged from one to four. After two cycles of NACT, every patient was assessed for clinical and radiological response and reviewed by the tumor board. Patients who had significant regression of disease after NACT and met the resectability criteria were planned for radical surgery. The extent of surgical resection was based on the post-chemotherapy residual tumor volume. All the patients who were operated received adjuvant therapy and were followed up for 6 months to 5 years (median follow-up of 29 months). Recurrence patterns and overall survival rates were analyzed.
Statistical Analysis
Categorical variables were summarized using numbers and percentages. All analyses were done using SPSS version 16.0. The Kaplan–Meier survival analysis method was applied to calculate the conditional probability of survival. The online resource “SankeyMATIC,” accessed at https://sankeymatic.com, has been used to generate the Sankey Diagrams for this study. The study was approved by the Institutional Review Board and Ethics Committee.
Results
A total of 79 patients with borderline resectable oral cavity cancers who received NACT were assessed in the time period studied. Ten of these patients had received NACT at another center and were therefore excluded from the study. The clinical parameters of the remaining 69 patients are summarized in [Table 1].
|
Demographic details ( n = 69) |
|
|
Age |
Range: 27–72 years |
|
Males |
53 (76.8%) |
|
Females |
16 (23.2%) |
|
Comorbidities |
|
|
Yes |
23 (33.3%) |
|
No |
46 (66.7%) |
|
Clinical parameters |
|
|
Oral cavity subsite |
|
|
Tongue |
48 (69.6%) |
|
Gingivobuccal complex |
21 (30.4%) |
|
Clinical T stage |
|
|
cT3 |
16 (23.2%) |
|
cT4a |
39 (56.5%) |
|
cT4b |
12 (17.4%) |
|
Clinical N stage |
|
|
cN0 |
19 (27.5%) |
|
cN1 |
20 (29%) |
|
cN2 |
18 (26.1%) |
|
cN3 |
12 (17.4%) |
|
Neoadjuvant chemotherapy |
|
|
2 drug regimen |
18 (26.1%) |
|
3 drug regimen |
51 (73.9%) |
|
Number of cycles |
1–4 (median = 2) |
|
Adverse reactions (CTCAE v5 grade)[34] |
11 (15.9%) |
|
Febrile neutropenia—grade 3 |
2 (2.9%) |
|
Acute kidney injury—grade 3 |
2 (2.9%) |
|
Electrolyte imbalance—grade 2 |
1 (1.4%) |
|
Anemia—grade 3 |
1 (1.4%) |
|
Thrombocytopenia—grade 3 |
1 (1.4%) |
|
Hypovolemic shock—grade 4 |
1 (1.4%) |
|
Hepatic dysfunction—grade 2 |
1 (1.4%) |
|
Skin reactions—grade 3 |
1 (1.4%) |
|
Details of surgery |
|
|
Tongue (n = 48) |
|
|
Wide local excision |
37 (77.1%) |
|
Compartment resection |
4 (8.3%) |
|
Subtotal glossectomy |
5 (10.4%) |
|
Total glossectomy |
2 (4.2%) |
|
Reconstruction for tongue defects |
|
|
Primary closure |
3 (6.3%) |
|
Local flaps |
32 (66.7%) |
|
Pedicled flaps |
10 (20.8%) |
|
Free flaps |
3 (6.3%) |
|
Postoperative wound complications |
0 |
|
Adjuvant therapy |
|
|
Radiation therapy alone |
28 (59.4%) |
|
Chemoirradiation |
41 (40.1%) |
|
Adverse effects (CTCAE v5 grade)[34] |
|
|
Grade 2 |
8 (11.5%) |
|
Grade 3 |
2 (2.9%) |
|
Grade 4 |
1 (1.4%) |
|
Recurrences |
|
|
Follow-up period |
6 months–5 years (median 29 months) |
|
Total number of recurrences |
20 (28.9%) |
|
Locoregional control rate |
21.7% |
|
Subsite |
|
|
Tongue |
12/48 (25%) |
|
GBC |
8/21 (38.1%) |
|
Site of recurrence |
|
|
Local alone |
15% |
|
Locoregional |
60% |
|
Distant metastasis |
25% |
|
Proportion of recurrences occurring within 1 year |
85% |
|
Recurrences noted during adjuvant therapy |
3 |
|
Recurrence after complete pathological response |
1 of 20 (5%) |
|
Median overall survival |
43 months (95% CI: 39–47 months) |
Abbreviations: CI, confidence interval; CTCAE, Common Terminology Criteria for Adverse Events; GBC, gingivobuccal complex.
Subsite and Stage
The predominant site of primary tumor in the study group was the oral tongue (n = 48, 69.6%). Cancer of the gingivobuccal complex (GBC), which includes the buccal mucosa, lower gingivobuccal sulcus, lower alveolus and the retromolar trigone, constituted the rest of the cases (n = 21, 30.4%).
All the patients had stage III or IV disease, as per the eighth American Joint Committee on Cancer (AJCC) Tumor (T), nodes (N), metastases (M) (TNM) cancer staging system. Selection criteria for NACT were as mentioned above. The primary tumor was at an advanced T stage in a majority of the cases (T4a—56.5% and T4b—17.4%). About 72.5% of the patients had clinical node positivity (N1—29%, N2—26.1%, and N3—17.4%).
Neoadjuvant Chemotherapy
The three-drug regimen was preferred in 73.9% of the patients. The two-drug regimen included a combination of docetaxel with cisplatin (n = 14), paclitaxel with cisplatin (n = 3), or paclitaxel with carboplatin (n = 1). The number of cycles varied between one and four, with a median number of two cycles. NACT was tolerated well by most of the patients. Of the eleven (15.9%) patients who developed toxicity, two (2.9%) had febrile neutropenia, two had acute kidney injury (2.9%), two developed electrolyte imbalance (2.9%), one patient developed anemia requiring blood transfusion (1.4%), one had thrombocytopenia (1.4%), one had hypovolemic shock (1.4%), one patient had hepatic dysfunction (1.4%), and one developed skin reactions (1.4%), all managed appropriately by the Department of Medical Oncology, with advice from specialist units where required. There was no mortality due to NACT.
Cumulative doses used for the chemotherapeutic agents in the neoadjuvant setting are as follows: paclitaxel 175 mg/m2, docetaxel 75 mg/m2, cisplatin 75 mg/m2, 5-fluorouracil 750 mg/m2, capecitabine 1,250mg/m2, per oral, twice a day. The median cumulative dose of platins was 225 mg/m2.
Reassessment after NACT
All the patients in this study group were reassessed clinically and radiologically after completion of at least two cycles of NACT. Response Evaluation Criteria in Solid Tumors (RECIST) criteria could not be utilized for response assessment because of asymmetric and often uneven shrinkage of the tumor after NACT, further complicated by the presence of necrotic areas, where tumor viability is under question. For these reasons, radiological response was assessed as decrease in the size of tumor, focused on examining the factors that rendered the disease borderline resectable at presentation. Partial or complete response to chemotherapy was observed in the primary tumor in a majority of cases (98.5%), only one patient with T3 disease showing progression. In contrast, nodal disease had either not progressed (37.7%) or progressed (21.7%), with fewer partial or complete responses. Of the three patients with nodal disease infiltrating the skin, two had complete response (66.7%) and one had no response (33.3%). All the patients in the group underwent definitive surgery. The one patient who progressed on NACT had remained borderline resectable at reassessment. Since there was no response to chemotherapy and the disease did not become unresectable, the patient underwent surgery followed by adjuvant chemoirradiation.
Surgery
Surgical margins were based on the post-chemotherapy residual tumor volume. Of the 48 tongue cancers, 37 (77.1%) required only wide local excision, 4 (8.3%) required a compartment resection, subtotal glossectomy for 5 (10.4%), and total glossectomy for 2 cases (4.2%). Cancers of the GBC required more extensive surgery, amounting to either segmental or hemimandibulectomy in all patients, with or without ITF clearance. Ipsilateral or bilateral neck dissection, selective or comprehensive, was performed for every patient, depending upon the extent of primary tumor and nodal status. The technique of reconstruction was left to the surgeon's discretion, and was chosen depending upon the size of the defect, nodal status, and patient factors. Though not quantified, excessive bleeding upon incising the neck skin was noted by the surgical team in a significant proportion of post-NACT patients. However, this did not translate into excessive perioperative transfusion of blood or blood products. None of the patients had postoperative wound complications or delayed wound healing.
Postoperative Histopathology
The overall complete pathological response rate was 20.3%. Complete tumor response was seen in 21 patients (30.4%) and complete nodal response was seen in 12 (17.4%), as depicted in [Figs. 1] and [2]. Clear surgical margins were achieved in 42% of cases. Two patients had a positive surgical margin (2.3%). Other pathological prognostic factors studied were lymphovascular invasion, perineural invasion, and depth of invasion, summarized in [Table 2]. Lymph node density (LND) was an important, additional factor studied in these patients, calculated as the number of positive lymph nodes divided by the total number of lymph nodes dissected. LND of greater than equal to 0.07 is considered to have prognostic significance and is a predictor of recurrence in oral cancers.[3] LND of more than 0.07 was noted in 27 patients in this series (39.1%).


Abbreviations: DOI, depth of invasion; GBC, gingivobuccal complex; LND, lymph node density; LVI, lymphovascular invasion; PNI, perineural invasion.
Adjuvant Therapy
Adjuvant radiation therapy (RT) with or without chemotherapy was received by all patients in the study. Adjuvant chemoradiation therapy (CTRT) was received by 41 (59.4%), RT alone by 28 (40.1%), since patient factors precluded the use of concurrent chemotherapy. The CTRT regimen comprised 66 Gy radiation in 2 Gy per fraction, along with weekly cisplatin (40 mg/m2), for a median of three cycles (range: 2–6 cycles). Three-dimensional conformal external beam radiation therapy with a Cobalt-60 machine was used in 50 patients, volumetric modulated arc therapy in 12, and intensity-modulated radiation therapy in 3 patients. Four patients received adjuvant therapy at their hometown, and the details of their adjuvant therapy were not available. Majority of the patients completed their treatment without any breaks. Six patients had a break in their RT due to grade 4 reactions (mucositis, dermatitis, herpes zoster reactivation, lower respiratory tract infection), which were managed appropriately, and all the patients recovered within 4 to 14 days to resume RT.
Follow-Up
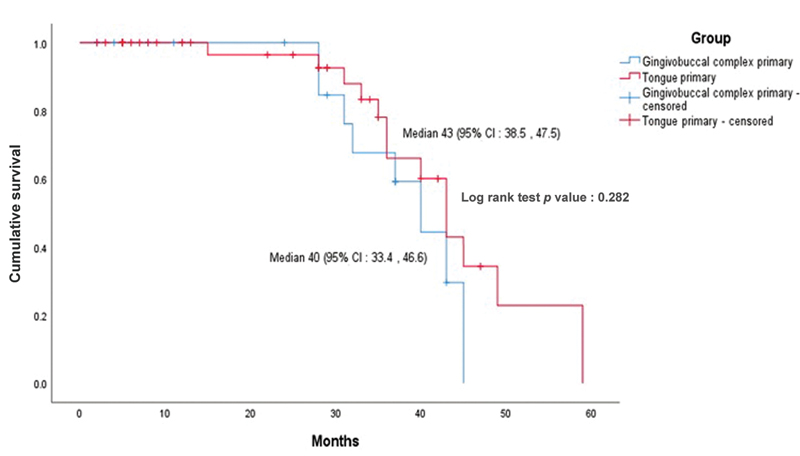
All patients were followed up for a maximum period of 5 years and minimum of 6 months (median of 29 months). During this time, a total of 20 patients were noted to have recurrent disease (28.9%). The index primary tumor was in the tongue in 12 and in the GBC in 8 patients. The locoregional control rate was 21.7%. Distant metastasis was detected in 5.6%. The median survival for the entire group was 43 months (95% confidence interval [CI]: 39–47 months), as depicted in [Fig. 3]. The median survival of patients with oral tongue cancer in our study was 43 months and that of GBC cancer was 40 months. Hence, the survival difference between the two groups was 3 months, with patients of oral tongue cancer surviving 3 months longer than those with GBC cancer, as seen in [Fig. 3]. The average time for recurrence in the entire cohort was 34 months (95% CI: 29–39 months). The pattern of disease recurrence is summarized in [Table 1].
Discussion
Oral cancer is the sixth most common cancer in the world.[1] [2] [4] [5] In India, oral cancer is becoming a major public health concern as it ranks among the three most common types of cancer in the country and accounts for over 30% of the cancer burden in the country.[6] [7] According to the present guidelines,[3] [23] management of oral cancer requires radical resection whenever feasible, followed by adjuvant therapy in the form of chemotherapy and/ or irradiation.[8] [9] [10] [11] [12] [13] [14] The treatment options become more limited in advanced oral cancer.
The ability to achieve complete surgical resection in advanced oral cancer, determined by fixed anatomical structures, is a significant prognostic factor.[20] [21] [22] [32] The involvement of prevertebral muscles, base of skull and encasement, or involvement of carotid artery is considered unresectable. Involvement of other complex anatomical structures in close proximity to the oral cavity remains a relative contraindication to resection, creating a subgroup of patients with borderline resectable or technically unresectable oral cancer. When treated with RT or chemoirradiation alone, the results are far from satisfactory and the prognosis quite grave. Survival rates for such advanced stage IV oral cancers vary widely across studies.[15] [16] [17] [18] In a recent study, Belcher et al reported a 29% 5-year survival rate for this group.[14] Although the results were not widely replicable, a study by Liao et al reported 45% survival at five years in T4b oral cancer treated by surgery.[19] [32] The lack of uniformity in predicting prognosis indicates the need for an intervention by which technically unresectable disease can be made resectable, offering patients the benefit of radical resection and adjuvant therapy. NACT is a promising method of achieving resectability in borderline resectable oral cancers.
The use of NACT in unresectable head and neck cancers was advocated by Vermorken et al (TAX 323 and 324) and Paccagnella et al.[15] [24] Since oral cancers comprised a minority of the patients included in these trials, and because the study population was predominantly European and North American where oral cancer burden is much lower, the results could not be extrapolated or achieved in unresectable oral cancers in South East Asia.
Other studies by Licitra et al and Zhong et al favored the use of chemotherapy in the neoadjuvant setting for advanced oral cavity cancers.[25] [26] Clinical complete response rate of up to 27% was achieved and these studies suggested the role of NACT in preservation of organ and function, and an improved post-treatment quality of life. However, the patients included in these studies had T2–4, N0–2 disease, which meant a majority of them would have had resectable disease even without administering NACT.
Patil et al conducted a widely cited retrospective study on the effect of NACT for borderline resectable oral cancers, mostly of the GBC, apt for the South East Asian population. Use of NACT in this large cohort of advanced oral cancers resulted in locoregional control rate of 20.6% at 24 months. The median estimated overall survival for patients in the surgical arm was 19.6 months, compared with 8.16 months in the nonsurgical arm.[27] [33]
At our center, a relatively homogenous group of patients with borderline resectable oral cancer was identified in the multidisciplinary tumor board meetings and offered NACT. The effect of NACT on the tumor and nodal response rates, surgical margins, and recurrence patterns was studied. When compared with other studies on NACT for advanced oral cancer, the majority (69.6%) of our patients had cancer of the oral tongue. There has been an increase in the incidence of tongue cancers in India,[1] [5] [6] and since most of the aforementioned studies have predominantly GBC cancers, our study fills a lacuna in the current knowledge regarding the behavior of tongue cancers after NACT. We propose the need for a subsite-wise evaluation of the impact of NACT on oral cancers.
The overall post-NACT complete pathological response rate of 20.3% is comparable to that reported in literature. However, upon subgroup analysis, our study shows a significantly better response of the primary tumor compared with nodal disease. This previously unreported influence of NACT on node positive disease needs to be further investigated, which could refine the present selection criteria for NACT.
Lymph node density is a previously unstudied pathological parameter in NACT, analyzed in our study. LND of more than 0.07 has been shown to be of prognostic significance in oral cancers.[32] In our study, all patients with recurrent disease had LND of more than 0.07. This could be a useful prognostic indicator for patients who undergo NACT.
Organ and function preservation following NACT, as proposed by Licitra et al,[25] was also observed in our study group. Lesser resection of the tongue could be performed in 85.4%, with no increase in the rate of compromised margins and an improved functional outcome and quality of life. In fact, the margin positivity rate was in our study was lesser than that observed in literature, despite limiting the extent of resection to the post-chemotherapy residual tumor volume.
Locoregional control rate of 21.7% in our study is comparable to that achieved in the study by Patil et al,[27] as is the median survival of 43 months. Majority of the recurrences occurred within 1 year of completion of treatment, which could reflect the biological aggressiveness of these tumors. It is of interest to note that 5% of the recurrences occurred despite a complete pathological response, which indicates the need to identify a reliable predictor of recurrence in such patients. A spectrum of recently detected molecular markers might hold the answer to this conundrum.
Limitations
The retrospective study design, a small study population, and absence of a comparison group limit our study. Although the data was retrospective, our findings have enabled us evaluate the impact of NACT on locally advanced, borderline resectable oral cancers and advocate the use of NACT to achieve resectability and an improved prognosis for patients with advanced disease.
Conclusions
NACT for patients with technically unresectable oral cavity cancers offers a chance of achieving adequate surgical resection, reducing surgical morbidity, and improving functional outcomes. Recurrence and survival rates noted in our study were comparable to those reported in literature. LND is a possible predictor of recurrent disease in the post-chemotherapy setting. Nodal disease may not respond to chemotherapy as well as the primary tumor. There is a need for comprehensive evaluation of prognostic factors, which could help identify the patients who will most benefit with NACT.
Conflicts of Interest
None declared.
Acknowledgments
We acknowledge the contributions of the numerous postdoctoral fellowship registrars, higher and general specialty residents pathologists and radiologists over the years, toward patient care and documentation, which were helpful for the conduct of this study.
Note
Interim analysis was presented at:
1. Oral presentation at Annual Research Day—2019, Christian Medical College, Vellore, India—awarded first place.
2. E-poster presented at Annual FHNO Conference, 2019 at Chennai, India.
Ethical Approval
This study has been approved by Institutional Review Board of Christian Medical College, Vellore; IRB No: 12662 [Retro].
Authors' Contributions
M.A., V.K., and A.J.T. conceptualized and designed the study. M.A., R.J. helped in data acquisition. V.K., R.K., A.S., and A.J. contributed to quality control of data and algorithms. M.A., V.K., R.J., R.K., A.S., and A.J. helped in data analysis and interpretation. M.A., V.K., and R.K. helped in statistical analysis. M.A. and V.K. prepared the manuscript. V.K. and A.J.T. edited the manuscript. A.J.T., A.S., and A.J. reviewed the manuscript.
-
References
- 1 Sankaranarayanan R. Oral cancer in India: an epidemiologic and clinical review. Oral Surg Oral Med Oral Pathol 1990; 69 (03) 325-330
- 2 Sankaranarayanan R, Ramadas K, Thomas G. et al; Trivandrum Oral Cancer Screening Study Group. Effect of screening on oral cancer mortality in Kerala, India: a cluster-randomised controlled trial. Lancet 2005; 365 (9475): 1927-1933
- 3 D'cruz A, Lin T, Anand AK. et al. Consensus recommendations for management of head and neck cancer in Asian countries: a review of international guidelines. Oral Oncol 2013; 49 (09) 872-877
- 4 Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol 2009; 45 (4-5): 301-308
- 5 Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55 (02) 74-108
- 6 Coelho KR. Challenges of the oral cancer burden in India. J Cancer Epidemiol 2012; 2012: 701932
- 7 Elango JK, Gangadharan P, Sumithra S, Kuriakose MA. Trends of head and neck cancers in urban and rural India. Asian Pac J Cancer Prev 2006; 7 (01) 108-112
- 8 Crombie AK, Farah C, Tripcony L, Dickie G, Batstone MD. Primary chemoradiotherapy for oral cavity squamous cell carcinoma. Oral Oncol 2012; 48 (10) 1014-1018
- 9 Chaudhary AJ, Pande SC, Sharma V. et al. Radiotherapy of carcinoma of the buccal mucosa. Semin Surg Oncol 1989; 5 (05) 322-326
- 10 Ghoshal S, Mallick I, Panda N, Sharma SC. Carcinoma of the buccal mucosa: analysis of clinical presentation, outcome and prognostic factors. Oral Oncol 2006; 42 (05) 533-539
- 11 Larizadeh MH, Shabani M. Survival following non surgical treatments for oral cancer: a single institutional result. Asian Pac J Cancer Prev 2012; 13 (08) 4133-4136
- 12 Bernier J, Cooper JS, Pajak TF. et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 2005; 27 (10) 843-850
- 13 Bernier J, Domenge C, Ozsahin M. et al; European Organization for Research and Treatment of Cancer Trial 22931. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004; 350 (19) 1945-1952
- 14 Belcher R, Hayes K, Fedewa S, Chen AY. Current treatment of head and neck squamous cell cancer. J Surg Oncol 2014; 110 (05) 551-574
- 15 Vermorken JB, Remenar E, van Herpen C. et al; EORTC 24971/TAX 323 Study Group. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med 2007; 357 (17) 1695-1704
- 16 Agarwal JP, Nemade B, Murthy V. et al. Hypofractionated, palliative radiotherapy for advanced head and neck cancer. Radiother Oncol 2008; 89 (01) 51-56
- 17 Mohanti BK, Umapathy H, Bahadur S, Thakar A, Pathy S. Short course palliative radiotherapy of 20 Gy in 5 fractions for advanced and incurable head and neck cancer: AIIMS study. Radiother Oncol 2004; 71 (03) 275-280
- 18 Huang SH, O'Sullivan B. Oral cancer: current role of radiotherapy and chemotherapy. Med Oral Patol Oral Cir Bucal 2013; 18 (02) e233-e240
- 19 Liao CT, Chang JT, Wang HM. et al. Surgical outcome of T4a and resected T4b oral cavity cancer. Cancer 2006; 107 (02) 337-344
- 20 Jerjes W, Upile T, Petrie A. et al. Clinicopathological parameters, recurrence, locoregional and distant metastasis in 115 T1-T2 oral squamous cell carcinoma patients. Head Neck Oncol 2010; 2: 9
- 21 Priya SR, D'Cruz AK, Pai PS. Cut margins and disease control in oral cancers. J Cancer Res Ther 2012; 8 (01) 74-79
- 22 Sutton DN, Brown JS, Rogers SN, Vaughan ED, Woolgar JA. The prognostic implications of the surgical margin in oral squamous cell carcinoma. Int J Oral Maxillofac Surg 2003; 32 (01) 30-34
- 23 National Comprehensive Cancer Network. Head and Neck Cancers (Version 1.2023). Accessed March 20, 2023 at: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf
- 24 Paccagnella A, Orlando A, Marchiori C. et al. Phase III trial of initial chemotherapy in stage III or IV head and neck cancers: a study by the Gruppo di Studio sui Tumori della Testa e del Collo. J Natl Cancer Inst 1994; 86 (04) 265-272
- 25 Licitra L, Grandi C, Guzzo M. et al. Primary chemotherapy in resectable oral cavity squamous cell cancer: a randomized controlled trial. J Clin Oncol 2003; 21 (02) 327-333
- 26 Zhong LP, Zhang CP, Ren GX. et al. Randomized phase III trial of induction chemotherapy with docetaxel, cisplatin, and fluorouracil followed by surgery versus up-front surgery in locally advanced resectable oral squamous cell carcinoma. J Clin Oncol 2013; 31 (06) 744-751
- 27 Patil VM, Prabhash K, Noronha V. et al. Neoadjuvant chemotherapy followed by surgery in very locally advanced technically unresectable oral cavity cancers. Oral Oncol 2014; 50 (10) 1000-1004
- 28 Pradhan SA. Surgery for cancer of the buccal mucosa. Semin Surg Oncol 1989; 5 (05) 318-321
- 29 Posner MR, Hershock DM, Blajman CR. et al; TAX 324 Study Group. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med 2007; 357 (17) 1705-1715
- 30 Salama JK, Stenson KM, Kistner EO. et al. Induction chemotherapy and concurrent chemoradiotherapy for locoregionally advanced head and neck cancer: a multi-institutional phase II trial investigating three radiotherapy dose levels. Ann Oncol 2008; 19 (10) 1787-1794
- 31 Haddad R, O'Neill A, Rabinowits G. et al. Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a randomised phase 3 trial. Lancet Oncol 2013; 14 (03) 257-264
- 32 Patel SG, Amit M, Yen TC. et al; International Consortium for Outcome Research (ICOR) in Head and Neck Cancer. Lymph node density in oral cavity cancer: results of the International Consortium for Outcomes Research. Br J Cancer 2013; 109 (08) 2087-2095
- 33 Patil V, Noronha V, Joshi A. et al. Is there a limitation of RECIST criteria in prediction of pathological response, in head and neck cancers, to postinduction chemotherapy?. ISRN Oncol 2013; 2013: 259154
- 34 Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. Using the Common Terminology Criteria for Adverse Events (CTCAE - Version 5.0) to evaluate the severity of adverse events of anticancer therapies. Actas Dermosifiliogr (Engl Ed) 2021; 112 (01) 90-92 (Engl Ed)
Address for correspondence
Publication History
Article published online:
10 April 2023
© 2023. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sankaranarayanan R. Oral cancer in India: an epidemiologic and clinical review. Oral Surg Oral Med Oral Pathol 1990; 69 (03) 325-330
- 2 Sankaranarayanan R, Ramadas K, Thomas G. et al; Trivandrum Oral Cancer Screening Study Group. Effect of screening on oral cancer mortality in Kerala, India: a cluster-randomised controlled trial. Lancet 2005; 365 (9475): 1927-1933
- 3 D'cruz A, Lin T, Anand AK. et al. Consensus recommendations for management of head and neck cancer in Asian countries: a review of international guidelines. Oral Oncol 2013; 49 (09) 872-877
- 4 Scully C, Bagan J. Oral squamous cell carcinoma overview. Oral Oncol 2009; 45 (4-5): 301-308
- 5 Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55 (02) 74-108
- 6 Coelho KR. Challenges of the oral cancer burden in India. J Cancer Epidemiol 2012; 2012: 701932
- 7 Elango JK, Gangadharan P, Sumithra S, Kuriakose MA. Trends of head and neck cancers in urban and rural India. Asian Pac J Cancer Prev 2006; 7 (01) 108-112
- 8 Crombie AK, Farah C, Tripcony L, Dickie G, Batstone MD. Primary chemoradiotherapy for oral cavity squamous cell carcinoma. Oral Oncol 2012; 48 (10) 1014-1018
- 9 Chaudhary AJ, Pande SC, Sharma V. et al. Radiotherapy of carcinoma of the buccal mucosa. Semin Surg Oncol 1989; 5 (05) 322-326
- 10 Ghoshal S, Mallick I, Panda N, Sharma SC. Carcinoma of the buccal mucosa: analysis of clinical presentation, outcome and prognostic factors. Oral Oncol 2006; 42 (05) 533-539
- 11 Larizadeh MH, Shabani M. Survival following non surgical treatments for oral cancer: a single institutional result. Asian Pac J Cancer Prev 2012; 13 (08) 4133-4136
- 12 Bernier J, Cooper JS, Pajak TF. et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 2005; 27 (10) 843-850
- 13 Bernier J, Domenge C, Ozsahin M. et al; European Organization for Research and Treatment of Cancer Trial 22931. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004; 350 (19) 1945-1952
- 14 Belcher R, Hayes K, Fedewa S, Chen AY. Current treatment of head and neck squamous cell cancer. J Surg Oncol 2014; 110 (05) 551-574
- 15 Vermorken JB, Remenar E, van Herpen C. et al; EORTC 24971/TAX 323 Study Group. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med 2007; 357 (17) 1695-1704
- 16 Agarwal JP, Nemade B, Murthy V. et al. Hypofractionated, palliative radiotherapy for advanced head and neck cancer. Radiother Oncol 2008; 89 (01) 51-56
- 17 Mohanti BK, Umapathy H, Bahadur S, Thakar A, Pathy S. Short course palliative radiotherapy of 20 Gy in 5 fractions for advanced and incurable head and neck cancer: AIIMS study. Radiother Oncol 2004; 71 (03) 275-280
- 18 Huang SH, O'Sullivan B. Oral cancer: current role of radiotherapy and chemotherapy. Med Oral Patol Oral Cir Bucal 2013; 18 (02) e233-e240
- 19 Liao CT, Chang JT, Wang HM. et al. Surgical outcome of T4a and resected T4b oral cavity cancer. Cancer 2006; 107 (02) 337-344
- 20 Jerjes W, Upile T, Petrie A. et al. Clinicopathological parameters, recurrence, locoregional and distant metastasis in 115 T1-T2 oral squamous cell carcinoma patients. Head Neck Oncol 2010; 2: 9
- 21 Priya SR, D'Cruz AK, Pai PS. Cut margins and disease control in oral cancers. J Cancer Res Ther 2012; 8 (01) 74-79
- 22 Sutton DN, Brown JS, Rogers SN, Vaughan ED, Woolgar JA. The prognostic implications of the surgical margin in oral squamous cell carcinoma. Int J Oral Maxillofac Surg 2003; 32 (01) 30-34
- 23 National Comprehensive Cancer Network. Head and Neck Cancers (Version 1.2023). Accessed March 20, 2023 at: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf
- 24 Paccagnella A, Orlando A, Marchiori C. et al. Phase III trial of initial chemotherapy in stage III or IV head and neck cancers: a study by the Gruppo di Studio sui Tumori della Testa e del Collo. J Natl Cancer Inst 1994; 86 (04) 265-272
- 25 Licitra L, Grandi C, Guzzo M. et al. Primary chemotherapy in resectable oral cavity squamous cell cancer: a randomized controlled trial. J Clin Oncol 2003; 21 (02) 327-333
- 26 Zhong LP, Zhang CP, Ren GX. et al. Randomized phase III trial of induction chemotherapy with docetaxel, cisplatin, and fluorouracil followed by surgery versus up-front surgery in locally advanced resectable oral squamous cell carcinoma. J Clin Oncol 2013; 31 (06) 744-751
- 27 Patil VM, Prabhash K, Noronha V. et al. Neoadjuvant chemotherapy followed by surgery in very locally advanced technically unresectable oral cavity cancers. Oral Oncol 2014; 50 (10) 1000-1004
- 28 Pradhan SA. Surgery for cancer of the buccal mucosa. Semin Surg Oncol 1989; 5 (05) 318-321
- 29 Posner MR, Hershock DM, Blajman CR. et al; TAX 324 Study Group. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med 2007; 357 (17) 1705-1715
- 30 Salama JK, Stenson KM, Kistner EO. et al. Induction chemotherapy and concurrent chemoradiotherapy for locoregionally advanced head and neck cancer: a multi-institutional phase II trial investigating three radiotherapy dose levels. Ann Oncol 2008; 19 (10) 1787-1794
- 31 Haddad R, O'Neill A, Rabinowits G. et al. Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a randomised phase 3 trial. Lancet Oncol 2013; 14 (03) 257-264
- 32 Patel SG, Amit M, Yen TC. et al; International Consortium for Outcome Research (ICOR) in Head and Neck Cancer. Lymph node density in oral cavity cancer: results of the International Consortium for Outcomes Research. Br J Cancer 2013; 109 (08) 2087-2095
- 33 Patil V, Noronha V, Joshi A. et al. Is there a limitation of RECIST criteria in prediction of pathological response, in head and neck cancers, to postinduction chemotherapy?. ISRN Oncol 2013; 2013: 259154
- 34 Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. Using the Common Terminology Criteria for Adverse Events (CTCAE - Version 5.0) to evaluate the severity of adverse events of anticancer therapies. Actas Dermosifiliogr (Engl Ed) 2021; 112 (01) 90-92 (Engl Ed)