

Subscribe to RSS
DOI: 10.1055/s-0043-1764466
Measurement Analysis of Ice Ball Size during CT-Guided Cryoablation Procedures for Better Prediction of Final Ice Ball Size and Avoidance of Complications
Authors
Funding None.


Abstract
Introduction Cryoablation is the destruction of living tissue by the application of extreme freezing temperature. There has been an increase in the use of cryoablation in the management of musculoskeletal lesions, in particular fibromatosis.
Aim This study aimed to measure the average and relative increase in size of the cryoablation ice ball after the first (10 minutes) and second freeze cycles (20 minutes) to accurately predict the size of the ice ball between first and second freezes to help prevent any unwanted damage of the nearby skin and neurovascular structures. This is especially important when ablating in relatively small body parts such as in the appendicular skeleton.
Material and Methods Eight patients treated with cryoablation over a 12-month period for fibromatosis were, included in the study. The size and volume of the ice ball were measured during the first and second cycle of cryoablation.
Results The average patient age of the cohort was 35.6 years old (min 28 and max 43). There was female predominance in the study (3:2, F:M). There was a significant increase (26%) in the linear dimensions and almost doubling in the volume of the ice ball between freeze cycles (p-value = 0.0037 for dimensions and p-value = 0.0002 for volumes).
Conclusion This pilot study is a preliminary attempt to predict the eventual size of the ice ball during cryoablation procedures when treating cases of fibromatosis. This should help in planning cryoablation to ensure decrease morbidity by preventing injury to adjacent critical structures (neurovascular bundle and skin).
Introduction
Cryoablation is the destruction of living tissue by the application of extreme freezing temperature.[1] This will cause cellular death by direct and indirect pathways.[1] This has been utilized in cancer treatment since the mid-19th century.[1] The applications of cryoablation are currently wide including several organ systems such as the liver, kidney, prostate, lung, breast, head and neck, brain, and esophagus.[2] [3] [4] [5] [6] It was in the late 1960s, that its use increased in the management of musculoskeletal malignancy and benign conditions such as bone tumors, soft tissue sarcoma, and fibromatosis.[7] The benefits of applying freezing temperature are a reduction in size of the tumor and pain relief.[8]
These extreme freezing temperatures can be delivered locally by surgical (open or laparoscopic) or percutaneous approaches.[9] The fast-expanding utilization of image-guided procedures have significantly expanded the use of cryoablation and it can now be used for far more musculoskeletal procedures. Image-guided procedures are preferred as they have a lower rate of complications and morbidity.[7]
The percutaneous approach requires cryoprobes which deliver the extreme low temperatures utilizing the Joule-Thomson effect, when rapid expansion of a liquid gas (argon) leads to rapid drop in temperature of the gas leading to fast cooling along the shaft of the cryoprobe.[10]
Computed tomography (CT) can show the developing ice ball developed around the cryoprobe in real time. Freezing the target tissue will result in the formation of an ice ball around the cryoprobe with its size determined by four factors: rate of gas infusion, time for gas expansion, cryoprobe size, and probe configuration.[11] Typically, this stage will last for 10 minutes. In the second stage of the procedure, the thawing, the ice ball is either let to thaw by itself for 10 minutes (passive thawing) or actively warmed by, a combination of a passive thaw (6–8 minutes) and an active thaw (2–4 minutes) in which the probe is electronically heated. In the third stage, a second cycle of freezing results in a larger ice ball, and again this is typically 10 minutes in duration. The last stage comprises a final thaw following which the cryoprobes can be removed.
Other tissues likely to be injured in cryoablation especially in the appendicular skeleton are skin and neurovascular structures. Ideally, the ice ball should extend beyond the margins of the lesion by 5 mm as the peripheral 5 mm of the ice ball does not cause cell death. However, care must be taken not to excessively grow the ice ball and potentially cause peripheral normal tissue damage peripheral normal tissue damage. Therefore, the prediction of the target ice ball size and the real-time monitoring play an important role in avoiding such complications. Despite the presence of manufacturers' isotherms as reference guide, there are no studies that show in vivo measurement of the cryoablation ice ball after the first and second freeze cycles with their relative increase in size to aid the decision and planning of the cryoablation treatment.
Aim
This study aims to measure the average and relative increase in size of the cryoablation ice ball after the first (10 minutes) and second freeze cycles (20 minutes) to accurately predict the size of the ice ball between first and second freezes to help prevent any unwanted damage of the nearby skin and neurovascular structures. This is especially important when ablating in relatively small body parts such as in the appendicular skeleton.
Materials and Methods
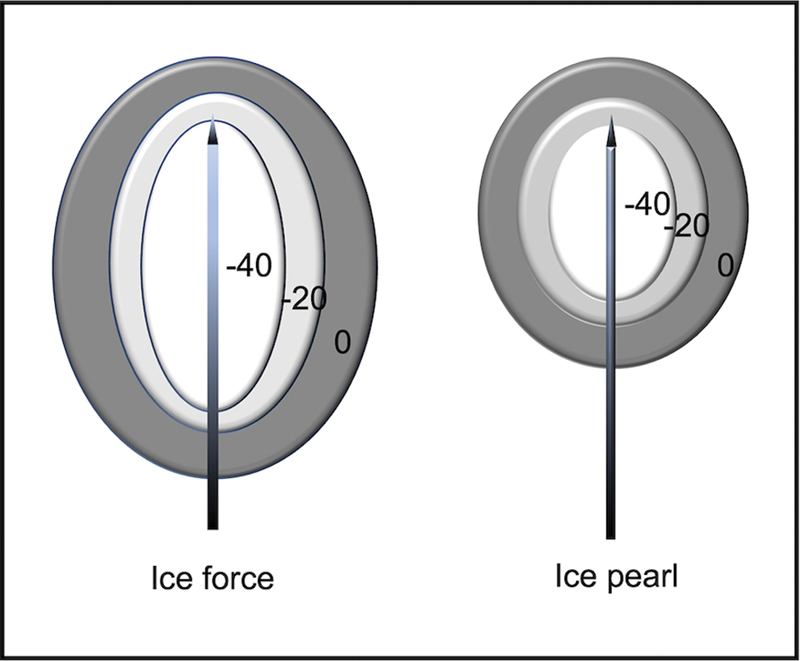
Eight patients treated with cryoablation over a 12-month period were included in the study. All patients had biopsy-proven fibromatosis. All cryoablation cases were performed under general anesthesia using the Visual Ice cryotherapy system (Boston Scientific). The following cryoprobes were used IceRod, IceSphere, and IceFORCE Boston Scientific ([Fig. 1], [Table 1]). Low-dose CT was acquired using the Siemens Somatom Sensation AS (Siemens Medical Systems) and was used in all cases for standardization of the results. No immediate complications were recorded on the day of any of the procedures. After application of single or multiple cryoprobes into the target lesion using CT-guided imaging, the first cycle of cryoablation was commenced for 10 minutes. Real-time monitoring was performed by CT scanning of the target site at intervals between 2 and 4 minutes with the last one at the end of the 10th minute. The dimensions and the volume of the resultant ice ball was recorded using the following equation [V=4/3 П (A*B*C)3 where A, B & C are the semi-axises of the ellipsoid shaped ice ball].
A thawing stage was achieved by a combination of a passive and active melting phase of the ice ball for a further 10 minutes. A second cycle of freezing was performed for further 10 minutes with intermittent targeted CT scanning at 2- to 4-minute intervals. After the end of the second cycle of freezing, a final CT scan was performed to measure the final size of the ice ball. An important note to make is that all probes were kept at 100% of power delivery. If the power to any of the probes was reduced from 100% for any reason (e.g., the ice ball was growing too large), these cases would not have been included in the study.
All ice ball measurements were performed by one experienced consultant radiologist with more than 10 years of experience to ensure consistency.
After data collection, the measurements were tabulated to statistically analyze the average size of the ice balls after each cycle and the relative increase of the size after the second cycle.
Results
The average patient age of the cohort was 35.6 years old (min 28 and max 43). There was female predominance in the study (3:2, F:M). All patients were treated for fibromatosis in different parts of the body. Two types of measurements are used in this study: the volume and the three perpendicular dimensions—length, width, and depth according to the planes of the scan. Each variable was measured twice after the 10-minute first cycle and after the 10-minute second cycle. The measurement performed after the thawing cycle was not recorded. We used two types of statistical comparisons between the two set of measurements: average comparison and regression analysis. There was a clear increase in volume and dimensions of the ice ball (p-value = 0.0037 for dimensions and p-value = 0.0002 for volumes) as we expected as the size and dimensions of the ice ball in the second cycle will be larger than in the first cycle.
In terms of ice ball volume, the average volume increased from 12.21 cm3 after the first cycle to 24.74 cm3 after the second cycle representing an increase by 102.6%. This means that ice ball size is more than doubled after the second cycle. However, the observer has to understand that the doubling size is a reflection of increase in the dimensions used to calculate the volume, which is not necessarily doubled themselves. Therefore, we have observed that the average dimensions have increased from 2.675 cm after the first cycle to 3.275 cm after the second cycle representing an increase by 26.1% in all directions when considering all the dimensions as one group. This was also evident as a positive regression when regression analysis was applied. The dimensions and volume average comparison and regression analysis is demonstrated in [Figs. 2] [3] [4] [5] [6] and [Tables 2] and [3].





Discussion
Cryoablation causes cellular death and tissue necrosis.[8] This is achieved by direct and indirect pathways.[8] The direct pathway results in cell damage by dehydration and shrinkage of cells as free water moves from the intracellular compartment to the highly crystalized extracellular compartment because of a change of osmolarity between the two compartments.[8] Additionally, there is cold-induced damage of cellular organelles and cold denaturation of the cellular proteins.[12] During the thawing stage, the extracellular water melts faster than the intracellular compartment resulting in a shift of water from outside the damaged cells to inside causing rapid cellular swelling, bursting, and cell death.[8] The indirect mechanism of tissue damage which could also be termed as delayed cellular death results from the body inflammatory response to cold injury. The vascular endothelium is damaged during the cooling and thawing processes leading to thrombosis and local tissue ischemia. This will be followed by an inflammatory phase which attempts to repair the tissue; however, chemotactic macrophages and neutrophils will start to remove the damaged cells and cellular debris leading to delayed tissue damage.[8]
Advantage of Image-Guided Percutaneous Cryoablation
The main advantage of image-guided percutaneous cryoablation is the ability to monitor the target tissue during the procedure. The ice ball can be clearly seen by both CT and ultrasound during the treatment.[8] The ice ball is also visible on magnetic resonance imaging (MRI) but requires MRI-specific hardware which is much less readily available. CT and ultrasound scan are preferred in our institution. On ultrasound, the superficial part of the ice ball is visualized clearly in real time as a hyperechoic curvilinear structure which casts a dense acoustic shadow which obscures the deeper aspect of the ice ball. CT shows the ice ball to be hypodense relative to the adjacent soft tissues and allows it to be visualized clearly including its deeper aspect. We use a combination of both during procedures in our institution.
Disadvantage of the Cryoablation
The primary drawback of the procedure although uncommon, is the postprocedural inflammatory reaction leading sometimes to a systemic response called cryoshock.[13] [14] This syndrome can induce a constellation of symptoms including hypotension, respiratory insufficiency, multiple organ failures, and disseminated intravascular coagulation.[15] This is thought to be mediated by the delayed phase and the production of inflammatory cytokine production.[15]
Cryoablation Complications
Application of liquid gas to living tissues and resultant cryoablation can cause certain complications to healthy tissues. In a study on 200 cryotherapy treatments when either carbon dioxide or liquid nitrogen was poured into bone tumors, complications such as fractures, infections, and paresthesia were documented in 2.34% of cases.[16] It was worth noting that all these were intraoperative open surgeries with active adjacent soft tissue protection/management including warm saline application.[16]
In their attempt to relate the size of the ice ball to the incidence of postcryoablation myositis, Bing et al[17] found that myositis has occurred in 87% of the cases with variable grades (0–3) and the grade of the muscle injury is positively correlated with the size of the ice ball (p < 0.001); however, only two patients (9.5%) with grade 3 myositis were symptomatic and required simple anti-inflammatory medications to achieve pain resolution.[17] They also measured the average size of the ice ball with each grade (Grade 0 = 2.8 cm3, Grade 1 = 9.2 cm3, Grade 2 = 17.1 cm3, and Grade 3 42.9 cm3). Conditions treated by cryoablation in their cohort of patients included metastasis, aneurysmal bone cysts, and desmoid tumors.
There are no previous studies to compare the size and dimension of the ice ball between the first and second cryoablation cycles in the medical literature. Therefore, we compared our results with the manufacturer guide measurement in laboratory studies. The maximum dimensions of the ice ball according to the manufacturer guidelines range between 3.7 to 5.3 cm for a single probe application and between 4.8 and 5.9 cm for double probe application. Our results have confirmed our practical observations, that the size of the ice ball at the end of the second cycle was always larger than the size of the ice ball at the end of the first cycle. This is unsurprising from the understanding of the process of cryoablation.
How large the ice ball will grow between the first and second freeze cycles is extremely important as it gives a guide as to whether the ice ball size is sufficient to cover the tumor and if it is going to get close to important structures such as skin and neurovascular spaces especially in tight soft tissue spaces such as the extremities. Predicting the volume is difficult to appreciate in 3-plane imaging such as CT. Therefore, dimension measurements are important to analyze. If we measure the dimension of the ice ball after the first cycle and measure how far it is from an important structure such as a neurovascular bundle, this study will help us to predict how much safe margin we still have if we apply the second cycle of cryoablation. If there is a concern that the margin is close to an important structure the power to the particular needle can be reduced or hydro-/pneumodissection can be performed. Taking 26.1% increase in dimension in any direction ± 10% will be our guidelines for such procedures. It is worth noting that the dimensions and the volume of the ice ball recorded were generally smaller than those provided by manufacturers from laboratory studies. The reasons could be due to different in vivo tissue characteristics than laboratory experiment or measurements provided by the manufacturers represent maximum rather than average.
As a small pilot, our study has some limitations. One of the most important limitations is the small sample size. Other limitations include that we only treated fibromatosis and therefore, the ice ball behavior, size, and dimension cannot be extrapolated to other types of tissues which may have a differing resistance to freezing or compliance with low temperatures. We also used one type of cryoablation, and this again cannot be generalized to other types of cryoprobes or cryogas or different manufacturers. The study ignored the cases when more than three probes were inserted as volume and dimension measurement become complicated and difficult to reproduce or measure without sophisticated tools and software. Nevertheless, the main objective of our study was to provide some guidance or measurement of the ice ball to avoid damage of important structures in tight and small spaces and we think this study has given an early indication of such benefit.
Despite these limitations, we believed that our study has given a preliminary prediction for the ice ball size and dimensions when performing such procedures. No immediate complications were observed in any of the study patients.
Conclusion
This pilot study is a preliminary attempt to predict the eventual size of the ice ball during cryoablation procedures when treating cases of fibromatosis. Being able to predict the ice ball size at the end of the procedure will help to identify if there are any normal structures that are potentially at risk of injury or if the ablation zone is going to be large enough to cover the entirety of the lesion. This hopefully gives the operator additional confidence when performing such procedures especially in tight spaces such as in the limbs.
Conflict of Interest
None declared.
-
References
- 1 Goldberg SN, Grassi CJ, Cardella JF. et al; Society of Interventional Radiology Technology Assessment Committee International Working Group on Image-Guided Tumor Ablation. Image-guided tumor ablation: standardization of terminology and reporting criteria. Radiology 2005; 235 (03) 728-739
- 2 Gage AA, Baust JG. Cryosurgery for tumors - a clinical overview. Technol Cancer Res Treat 2004; 3 (02) 187-199
- 3 Callstrom MR, Charboneau JW. Technologies for ablation of hepatocellular carcinoma. Gastroenterology 2008; 134 (07) 1831-1835
- 4 Mazaris EM, Varkarakis IM, Solomon SB. Percutaneous renal cryoablation: current status. Future Oncol 2008; 4 (02) 257-269
- 5 Ritch CR, Katz AE. Prostate cryotherapy: current status. Curr Opin Urol 2009; 19 (02) 177-181
- 6 Littrup PJ, Jallad B, Chandiwala-Mody P, D'Agostini M, Adam BA, Bouwman D. Cryotherapy for breast cancer: a feasibility study without excision. J Vasc Interv Radiol 2009; 20 (10) 1329-1341
- 7 Rose PS, Morris JM. Cryosurgery/cryoablation in musculoskeletal neoplasms: history and state of the art. Curr Rev Musculoskelet Med 2015; 8 (04) 353-360
- 8 Erinjeri JP, Clark TW. Cryoablation: mechanism of action and devices. J Vasc Interv Radiol 2010; 21 (08) , Suppl): S187-S191
- 9 Hui GC, Tuncali K, Tatli S, Morrison PR, Silverman SG. Comparison of percutaneous and surgical approaches to renal tumor ablation: metaanalysis of effectiveness and complication rates. J Vasc Interv Radiol 2008; 19 (09) 1311-1320
- 10 O'Rourke AP, Haemmerich D, Prakash P, Converse MC, Mahvi DM, Webster JG. Current status of liver tumor ablation devices. Expert Rev Med Devices 2007; 4 (04) 523-537
- 11 Shah TT, Arbel U, Foss S. et al. Modeling cryotherapy ice ball dimensions and isotherms in a novel gel-based model to determine optimal cryo-needle configurations and settings for potential use in clinical practice. Urology 2016; 91: 234-240
- 12 Hoffmann NE, Bischof JC. The cryobiology of cryosurgical injury. Urology 2002; 60 (02, Suppl Suppl 1): 40-49
- 13 Chapman WC, Debelak JP, Blackwell TS. et al. Hepatic cryoablation-induced acute lung injury: pulmonary hemodynamic and permeability effects in a sheep model. Arch Surg 2000; 135 (06) 667-672 , discussion 672–673
- 14 Washington K, Debelak JP, Gobbell C. et al. Hepatic cryoablation-induced acute lung injury: histopathologic findings. J Surg Res 2001; 95 (01) 1-7
- 15 Seifert JK, Stewart GJ, Hewitt PM, Bolton EJ, Junginger T, Morris DL. Interleukin-6 and tumor necrosis factor-α levels following hepatic cryotherapy: association with volume and duration of freezing. World J Surg 1999; 23 (10) 1019-1026
- 16 Chen C, Garlich J, Vincent K, Brien E. Postoperative complications with cryotherapy in bone tumors. J Bone Oncol 2017; 7: 13-17
- 17 Bing F, Garnon J, Tsoumakidou G, Enescu I, Ramamurthy N, Gangi A. Imaging-guided percutaneous cryotherapy of bone and soft-tissue tumors: what is the impact on the muscles around the ablation site?. Am J Roentgenol 2014; 202 (06) 1361-1365
Address for correspondence
Publication History
Article published online:
20 March 2023
© 2023. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Goldberg SN, Grassi CJ, Cardella JF. et al; Society of Interventional Radiology Technology Assessment Committee International Working Group on Image-Guided Tumor Ablation. Image-guided tumor ablation: standardization of terminology and reporting criteria. Radiology 2005; 235 (03) 728-739
- 2 Gage AA, Baust JG. Cryosurgery for tumors - a clinical overview. Technol Cancer Res Treat 2004; 3 (02) 187-199
- 3 Callstrom MR, Charboneau JW. Technologies for ablation of hepatocellular carcinoma. Gastroenterology 2008; 134 (07) 1831-1835
- 4 Mazaris EM, Varkarakis IM, Solomon SB. Percutaneous renal cryoablation: current status. Future Oncol 2008; 4 (02) 257-269
- 5 Ritch CR, Katz AE. Prostate cryotherapy: current status. Curr Opin Urol 2009; 19 (02) 177-181
- 6 Littrup PJ, Jallad B, Chandiwala-Mody P, D'Agostini M, Adam BA, Bouwman D. Cryotherapy for breast cancer: a feasibility study without excision. J Vasc Interv Radiol 2009; 20 (10) 1329-1341
- 7 Rose PS, Morris JM. Cryosurgery/cryoablation in musculoskeletal neoplasms: history and state of the art. Curr Rev Musculoskelet Med 2015; 8 (04) 353-360
- 8 Erinjeri JP, Clark TW. Cryoablation: mechanism of action and devices. J Vasc Interv Radiol 2010; 21 (08) , Suppl): S187-S191
- 9 Hui GC, Tuncali K, Tatli S, Morrison PR, Silverman SG. Comparison of percutaneous and surgical approaches to renal tumor ablation: metaanalysis of effectiveness and complication rates. J Vasc Interv Radiol 2008; 19 (09) 1311-1320
- 10 O'Rourke AP, Haemmerich D, Prakash P, Converse MC, Mahvi DM, Webster JG. Current status of liver tumor ablation devices. Expert Rev Med Devices 2007; 4 (04) 523-537
- 11 Shah TT, Arbel U, Foss S. et al. Modeling cryotherapy ice ball dimensions and isotherms in a novel gel-based model to determine optimal cryo-needle configurations and settings for potential use in clinical practice. Urology 2016; 91: 234-240
- 12 Hoffmann NE, Bischof JC. The cryobiology of cryosurgical injury. Urology 2002; 60 (02, Suppl Suppl 1): 40-49
- 13 Chapman WC, Debelak JP, Blackwell TS. et al. Hepatic cryoablation-induced acute lung injury: pulmonary hemodynamic and permeability effects in a sheep model. Arch Surg 2000; 135 (06) 667-672 , discussion 672–673
- 14 Washington K, Debelak JP, Gobbell C. et al. Hepatic cryoablation-induced acute lung injury: histopathologic findings. J Surg Res 2001; 95 (01) 1-7
- 15 Seifert JK, Stewart GJ, Hewitt PM, Bolton EJ, Junginger T, Morris DL. Interleukin-6 and tumor necrosis factor-α levels following hepatic cryotherapy: association with volume and duration of freezing. World J Surg 1999; 23 (10) 1019-1026
- 16 Chen C, Garlich J, Vincent K, Brien E. Postoperative complications with cryotherapy in bone tumors. J Bone Oncol 2017; 7: 13-17
- 17 Bing F, Garnon J, Tsoumakidou G, Enescu I, Ramamurthy N, Gangi A. Imaging-guided percutaneous cryotherapy of bone and soft-tissue tumors: what is the impact on the muscles around the ablation site?. Am J Roentgenol 2014; 202 (06) 1361-1365