

Subscribe to RSS
DOI: 10.1055/s-0043-1762445
Novel Repair of Extensive Skull Base Hyperpneumatization with Associated Pneumocele and Pneumatocele
Authors

Introduction: Skull base hyperpneumatization is the pathologic proliferation of temporal bone air cells that usually occurs secondary to trauma or infection. Spontaneous hyperpneumatization is extremely rare and has been associated with congenital temporal bone defects and repeated Valsalva maneuvers. Pneumatoceles are air-containing spaces that arise within the cranium and in typically non-aerated bone. Pneumatoceles occur when a pneumocele extends beyond the periosteum and into the surrounding soft tissue. We present a rare case of skull base hyperpneumatization associated with both pneumatoceles and pneumatoceles treated with a novel surgical approach.
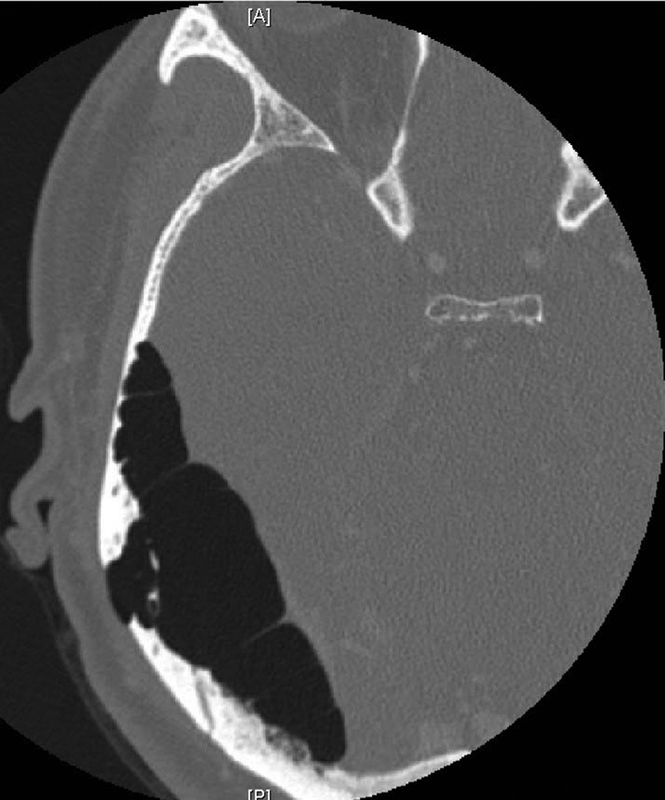
Case Description: A 50-year-old male was referred to our clinic after identification of skull base hyperpneumatization and midline shift on imaging performed following an episode of vertigo with persistent gait imbalance and associated headaches, cognitive decline, and cervicalgia. He denied hearing loss but reported bilateral tinnitus. The patient reported daily forceful nose blowing. CT imaging demonstrated marked hyperpneumatization of the right temporal bone and skull base with an associated pneumocele of the middle cranial fossa. There was pneumatocele formation in the right postauricular region, atlanto-occipital joint, and posterior paraspinal soft tissue.
A diagnosis of pneumocele and pneumatocele secondary to right skull base hyperpneumatization was made. Surgery was recommended given his symptoms of neck pain, headaches, and cognitive decline. A right temporary tympanostomy tube placement, mastoidectomy, and middle fossa craniotomy were performed. An abdominal fat graft was placed in the mastoid between the choke points with the middle fossa and mastoid tip. Hydroxyapatite bone cement was used to seal off the mastoid antrum from the mastoid proper. Postoperatively, his headaches and mentation improved. He will undergo repeat imaging at 6 months postoperatively.
Conclusions: Skull base hyperpneumatization with concurrent cranial pneumocele and cervical pneumatocele is an extremely rare phenomenon. Given this unique presentation, a novel combined surgical approach was implemented to address all hyperpneumatized areas and prevent recurrence. While individual surgical approaches have been reported to manage hyperpneumatization-related pneumocele or pneumatocele, this novel combined approach is not known to have been previously reported.



No conflict of interest has been declared by the author(s).
Publication History
Article published online:
01 February 2023
© 2023. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany