RSS-Feed abonnieren
DOI: 10.1055/s-0043-1761600
Zurich Mini Cementless Total Hip Arthroplasty in 42 Small Breed Dogs and 8 Cats: Surgical Technique and Outcomes
Autor*innen

Abstract
This report aims to describe implant characteristics and procedure for implantation, and comment on and report the clinical outcomes in small dogs and cats using the new Zurich mini cementless total hip system. This study involved 8 cats and 42 dogs, with 3 cats and 6 dogs having bilateral total hip arthroplasties (THA). The mean body weight for cats was 6.5 kg, and the mean body weight for dogs was 9.2 kg. In the group of THAs in cats, capital physeal fracture was the reason for performing a THA in six cases (60%), hip dysplasia was the underlying reason in four cases (30%) and hip luxation in one case (10%). Among the 48 THAs in dogs, hip dysplasia was the underlying cause for performing THA in 27 cases (56%), avascular necrosis of the femoral head in 12 cases (25%), traumatic luxation with underlying hip dysplasia in 4 cases (8.5%), capital physeal fracture in 4 cases (8.5%), and traumatic femoral head fracture in 1 adult dog (2%). Seven postoperative complications were encountered, and all were solved without the need for explanting the prosthesis, except in one case because of the owner's decision. In conclusion, the Zurich mini cementless total hip system performed well in this study, with most dogs and cats having an excellent outcome and no patient being too small for the available implant sizes.
Keywords
arthroplasty - hip disease - joint replacement - soft-tissue surgery - THA in small dogs and catsIntroduction
Several diseases affect the hip in small breed dogs and cats.[1] [2] [3] [4] These processes include but are not limited to hip dysplasia leading to osteoarthritis, traumatic luxation of the hip, capital physeal fractures, comminuted femoral neck or head fractures, osteoarthritis of the hip joint secondary to previous trauma or fractures, failure of a previously performed femoral head and neck excisional arthroplasty (FHO), Legg-Calvé-Perthes disease and, unique to cats, spontaneous physeal dysplasia with slipped capital femoral epiphysis.[4] [5]
Some of the above conditions can be medically managed with non-steroidal anti-inflammatory drugs, and other analgesics, weight optimization to decrease the load resisted by the joint, chondroprotectants and specific physical rehabilitation protocols.[5] Surgical procedures are considered when the patient becomes refractory to medical or conservative management or in the case of irreparable fractures; the most used procedure in small-breed dogs and cats is excisional arthroplasty of the femoral head and neck (FHO).[4] [5] [6] One long-term study found significant gait abnormalities in cats 1 year following FHO.[5] Another study that included both cats and dogs evaluated the clinical, radiographic and gait analysis findings following FHO, revealing functional deficits in small and large breed dogs and cats of varying magnitude and frequency.[6]
Total hip arthroplasty (THA) is now commonly used in medium and large breed dogs for the previously mentioned hip conditions affecting the hip with favourable and predictable outcomes.[7] [8] The total hip replacement procedure in dogs eliminates pain secondary to osteoarthritis, and force plate analysis demonstrated regular leg use following a THA procedure.[9] There is a limited number of case series involving THA surgeries in small-breed dogs and cats; all report favourable outcomes following the THA procedure.[1] [2] [3] [4] In these publications involving small-breed dogs and cats, the Micro and Nano BioMedtrix Cemented total hip systems were used, and most dogs and cats had excellent outcomes. The most common postoperative complication encountered was prosthetic dislocation, femoral fracture and aseptic loosening.[1] [2] [3] Several studies evaluating the Zurich Cementless Total Hip System (Kyon AG, Zurich CH) in medium to large breed dogs have demonstrated good to excellent outcomes.[10] [11] [12] [13] [14] There are no current reports in the veterinary literature assessing the use of the sixth-generation Zurich mini cementless total hip system, which became available in early 2020 by the same manufacturer. This report aims to describe implant characteristics and procedure for implantation and to comment on and report the clinical outcomes in 42 small dogs and eight cats using the sixth-generation Zurich mini cementless total hip system.
Materials and Methods
Zurich Cementless Mini-THR Implants
The Kyon mini-THR stem component implants are like the standard-size implant system. The modular construct consists of a stem secured to the medial cortex with locking screws, a neck in different offset lengths, a ceramic head and an acetabular cup. The stems are manufactured from Ti6Al7Nb titanium alloy and are available in sizes XS, SN, S, M, L, and XL ([Fig. 1]). [Fig. 1] shows the stem width and the number of holes for screws in the stem. The stems undergo specific surface processing to improve fatigue strength, followed by plasma coating of Ti and HA (hydroxyapatite) coatings on the cranial, medial and caudal surfaces to enhance early bone ongrowth. The stems have four or five tapered holes, depending on the length of the stem, which are directed medially, allowing screw heads to lock into the stem. The screws differ in diameter and length according to the stem size.

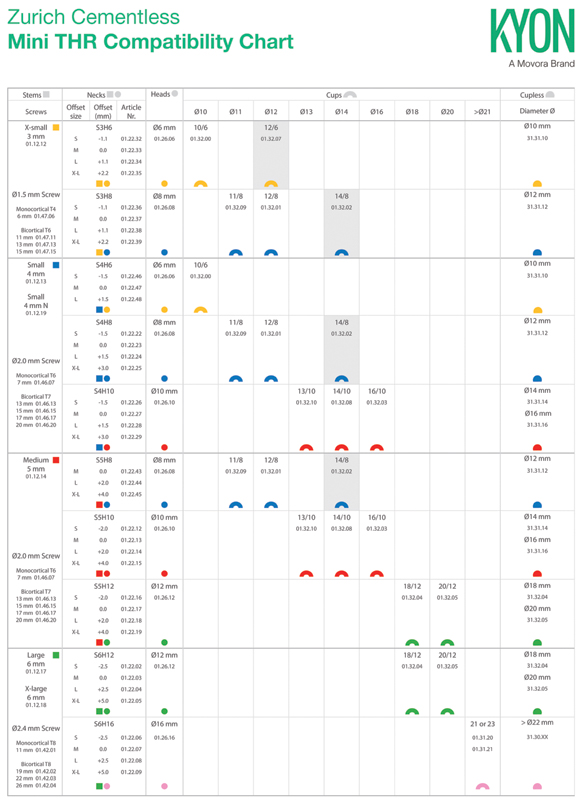
The neck of the femoral prosthesis is tapered for the locking attachment of the neck to the head. There is a default head size for each stem size, as can be seen in [Fig. 1]. The default head diameter is two times the stem width. However, the cup size needed may not always fit the stem size; the same stem size will accommodate different head sizes and consequently different cups. Since the taper at the base of the neck for coupling to the stem is independent of the taper at the top of the neck for coupling to the head, several combinations of stem sizes to head diameters can be achieved through different necks. To identify the necks ([Fig. 2]), a scheme with labels has been adopted to describe the possible combinations for each neck. The necks are marked with an ‘S’ for stem followed by the stem size (number), then an ‘H’ for the head size followed by the diameter of the head (number). For example, a neck to be used for a 4-size stem and an 8 mm head is marked as S4H8. The necks have varying lengths to adjust the offset required between the stem and the cup. Based on the stem's size, the necks' offset increment varies from 1.1 to 2.5 mm, as shown in [Fig. 2], depending on the stem size, 3 or 4 length necks are identified as S, M, L, or XL. The necks are produced from Ti6Al7Nb alloy, and the surface is processed to improve fatigue strength. The entire Kyon mini-THR chart covering all stem sizes and the many combinations of caps that can be used is shown in the Appendix. The size 6 stem can be used with a neck designated as S6H16 for a 16 mm diameter head, corresponding to a 21.5 mm or 23.5 mm cup from the standard implant sizes.

The ceramic heads are made of CeraVet (produced by CeramTec, Plochingen, Germany, for veterinary use). It is a blend of zirconia and alumina, equivalent to BioLox, used for the ceramic heads in human THR. The CeraVet heads come in 6, 8, 10, and 12 mm for the mini-THR system and 16 mm when combined with the standard size ([Fig. 1]).
The cups for the mini-system are available in outer diameters from 10 to 20 mm in 1 mm increments from the 10 mm cup to the 14 mm cup and then in 2 mm increments up to the 20 mm cup ([Fig. 2]). The two larger cups with outer diameters of 18 mm and 20 mm are constructed in the same fashion as the standard THR system cups. They consist of four components: an outer titanium shell with perforated holes, a solid inner titanium shell, a polyetheretherketone (PEEK) liner, and a carbon fibre reinforced PEEK (CFR-PEEK) ring in the area of head contact in the pole of the cup ([Fig. 3]).

The smaller cups with an outside diameter of 10 mm, 11 mm, 12 mm, 13 mm, 14 mm, and 16 mm, are engineered as a single piece of CFR-PEEK, with a designed macrostructure on the outside for mechanical integration. The inner diameter openings are 6 mm, 8 mm, and 10 mm ([Fig. 3]). The outer surface is lined with Ti and HA coatings for early bone integration. Additionally, since the CFR-PEEK cups are radiolucent, a titanium ring (Grade 5 titanium) is placed in a groove that runs around the cup's circumference just below the equator. The position of the cup opening can be evaluated by the shape of the ring in the various radiographic projections. The inner shape of these CFR-PEEK cups is aspherical to create the same contact with the head at 45 degrees, achieved with the larger cups and the CFR-PEEK ring, as declared by the manufacturer. The compatibility of each size of the implants with the animal's body weight, as suggested by the manufacturer, is shown in [Table 1].
Mini-THR Instrumentation
The instruments required for the mini-THR system are scaled-down versions, like those used for Kyon's standard THR system. The stem insertion instruments consist of a jig base, right and left arms for the jig, drill sleeves, drill bits, drill stops and screwdrivers ([Figs. 4],[5],[6],[7]). The main difference from the standard THR system is that in the mini-system the left and right arms are used to connect the stem to the base of the jig. A series of intramedullary reamers made from nitinol with flexible shafts violin shaped are available for the preparation of the intramedullary canal. These reamers scrape the cancellous bone from the medullary canal. The violin reamers start at 2.7 mm and are in 0.5 mm steps up to 6.7 mm. The tips of the reamers have a smaller diameter blunt nose to steer the reamer down the centre of the femoral canal, which prevents the reamer from penetrating the cortical wall. Those nitinol reamers are used with a low-speed motor.




For the preparation of the acetabular cup, there is a set of TiN-coated reamers. They are available in diameters from 8 to 14 mm in 1 mm increments. A cup impactor shaft with orientation pins is available to impact the cups, like the standard THR system ([Figs. 8] and [9]). Impactor heads for each cup size are available. The impactor head is assembled onto the impactor shaft, and the orientation pins are placed through the openings in the shaft.


Inclusion Criteria
Cats and dogs weighing from 2 to 18 kg with unilateral or bilateral THR performed during a 20-time month-long period were included in this study. A client consent form was signed by all the owners before the implantation of the new THR system. Implant size was selected according to pre-operative radiographic assessment study and intra-operative findings.
Surgical Technique
The technique of performing a primary THA using the mini-system is like that of a standard Zurich THA.[1] [12] [13] [14] Still, it requires dedicated instrumentation and careful preparation of the femoral canal and acetabulum. Impaction of the cup and reduction of the prosthesis are slightly different. The animals are positioned on the surgical table with a custom-made positioner and the superimposition of the pelvis is checked with an image intensifier (C-arm) before starting the surgical procedure. A wooden board is placed under the back of the animal in direct contact to maintain higher patient stability during the surgical procedure, especially during the prosthetic cup implantation.
Femoral canal preparation: The femur is externally rotated perpendicular to the pelvis (patella facing the ceiling). The femoral head is excised parallel and just distal to the equator. Either by hand or using power, a 1.5 to 2.0 mm drill bit is used to open the femoral canal, with the drill bit directed in a lateral and caudal direction to follow the direction of the neck. Once the drill bit is seated in the neck, the position of the drill bit is changed to be parallel to the long axis of the femur to enter the femoral canal. The trochanteric fossa is opened to the level of the intertrochanteric crest using small rongeurs and high-speed burr. The femoral neck ostectomy can be refined using an oscillating saw leaving 2 to 3 mm of the femoral neck proximal to the lesser trochanter, making sure to keep the initial inclination of the ostectomy. The dedicated nitinol flexible reamers (violin-shaped) are then used to complete the femoral reaming. The tendons of the Gemelli and internal obturator muscles are identified medial to the greater trochanter by removing fat and joint capsule overlying them. The tendons serve as a landmark to ensure proper lateral reaming. A high-speed burr is necessary to widen the entrance into the femoral canal to the tendons laterally. Fine maxillofacial rasps can be used to refine the femoral canal reaming to insert the trial stem, with some freedom in rotation to account for the proper stem anteversion.
Acetabulum preparation: The femur is returned to a neutral position, and a mini Hohmann retractor is inserted caudally to the acetabulum perforating the joint capsule. The femur positioning is maintained caudally and distally with the Hohmann retractor. Two small Gelpi retractors are positioned, one in a craniocaudal and one in a ventrodorsal direction, to properly retract the joint capsule and surrounding soft tissues away from the acetabulum. With sharp dissection, the redundant joint capsule is removed to visualize the acetabulum's entire perimeter. It is also essential to remove the remainder of the round ligament. Acetabular reaming, with a power handpiece set on low speed, is started initially with an acetabular reamer two sizes smaller than originally templated, aiming in the direction of the fossa. In cases of coxa plana, the reamer is aimed in a ventral direction, which will help excavate the filled acetabulum.
Reaming is continued with the power hand piece to the acetabulum's medial wall, ensuring to preserve it and the caudal pillar. The presence of osteophytes protruding over the reamer is checked and removed using rongeurs. This will ensure that solid bone exists over the cranial and caudal pillars of the acetabulum. Checking the radiographs is helpful in identifying the location of osteophytes, both cranial and caudal, in the acetabulum. The final reaming is performed with low-speed power, without wobbling with the reamer 1 mm smaller than the diameter of the cup. The final reamer of the same diameter is used gently by the hand. Osteostixis in cortical portions of the reamed acetabulum should be performed with a 1.5 mm drill bit and a protective drill sleeve set at a depth of 2 mm.
Implant preparation: The femoral stem is assembled onto the jig to align the screw holes on the femoral stem to the drill sleeve holes on the jig. The set screw is tightened securely. The drill stopper for the cis-cortex drill bits is set to avoid contacting the femoral stem when drilling the lateral cortex. The drill stopper for the transcortex drill bit is set to prevent too much of the drill tip from passing into soft tissues on the medial side of the femur.
Cup insertion: The anatomical retroversion of the acetabulum is identified by inserting the final reamer and centring it along the cranial and caudal pillars of the acetabulum, with the cranial and caudal borders of the reamer equally distant in respect to the pillars. The positioning bar orientation is marked with a haemostat on the surgical field and partial impaction of the cup is performed, aiming slightly ventral with the bar aligned with the previously set orientation marker (haemostat). Following the initial impaction with the mallet, the positioning bar is lowered in a ventral direction during the remaining impaction to have the positioning bar parallel to the floor at the conclusion, which means 45 degrees angle of lateral opening (ALO), providing that the pelvis is perfectly lateral. The ALO of the cup is checked with the C-arm. Suppose the pelvis has shifted and is not aligned due to the surgical manoeuvres. In that case, the animal's thorax is manipulated through the drapes to obtain a lateral view of the pelvis, or the table is tilted dorsally or ventrally. Complete impaction is performed if the ALO is acceptable with gentle firm blows, or the ALO is adjusted according to the C-arm's findings, holding the bar firmly to avoid tilting in a cranial or caudal direction and keeping the orientation bar parallel to the floor. Counterpressure is imperative in such small animals with light body mass and is provided by the assistant by maintaining a solid instrument, like a heavy hammer, against the patient's pelvis. Full seating of the cup is tested by inserting a no. 15 scalpel blade between the acetabular cup and the dorsal acetabular rim. Suppose the scalpel blade passes between the dorsal acetabular ridge and the acetabular component. In that case, the cup is impacted again. The ALO of the cup is again checked with the C-arm to verify that the proper orientation was maintained.
Stem insertion: The clearance between the femoral osteotomy and a short trial neck with a proper head inserted inside the cup is tested, pulling the femur distally with small-pointed forceps. When the distance is not enough to accommodate the neck touching the femoral osteotomy (too short a distance), the leg is externally rotated and 1 to 2 mm of the femoral neck is removed with a narrow saw blade. The clearance test is repeated after returning the femur to a neutral position. With the leg externally rotated, the femoral stem with the jig is inserted inside the femoral canal, using extreme care to avoid excessive rotational movement, which could lead to femoral fracture. While the stem is being inserted into the femoral canal, it is also essential to dorsally retract the soft tissues (gluteal musculature) to allow smooth insertion of the stem. To insert the stem, the jig is advanced distally while pushing the stifle proximally. In obese dogs, a longer dorsal skin incision should be performed to provide more freedom for stem insertion. The leg is internally rotated only when the stem is fully inserted with the dorsal soft tissues retracted. If not, the jig could lever against the soft tissues proximally, risking a fissure or fracture of the femur.
Complete insertion of the stem is verified by checking that the jig's base is level with the femoral osteotomy. With the leg in a neutral position, the stifle is flexed at 90 degrees, and the tibia is kept parallel to the table. The anteversion of the stem is checked by looking at the jig orientation using the gauge on the tibia, aiming for 20 degrees ( ± 5 degrees) of anteversion. The fascia lata is elevated, and caudally retracted with the biceps muscle by inserting a Gelpi retractor between the fascia lata retracted caudally and the vastus lateralis muscle cranially. Holding the jig firmly, the jig is pushed medially to get the stem in contact with the medial wall of the femur while the assistant counteracts the force by keeping the femur elevated with a Hohmann retractor positioned medially on the proximal femur.
The more oversized drill sleeve is used for the lateral (Cis) cortex, inserted in the 3rd hole of the jig and the lateral cortex is drilled with the proper drill bit. The small sleeve for the medial (trans) cortex is inserted to engage the conical hole in the corresponding drill hole in the stem. The medial cortex is drilled with the proper drill bit. All drilling should be done with the assistant simultaneously flushing with saline. A suitable size Torx screwdriver (prepared in advance by the assistant) is used to place the monocortical screw until it stops. The same procedure is repeated as above for the first screw (most proximal screw) hole in the jig, looking at the required length for the bicortical screw as indicated by the drill sleeve (the first screw is bicortical to withstand torsional forces). The sequence is repeated to insert the monocortical screws in the last hole of the jig, then in the remaining holes. All the screws are re-tightened in the same sequence with uniform force. The limb is externally rotated, retracting the soft tissues dorsally to allow access to the set screw of the jig, which is unscrewed to remove the jig. The leg is returned to a neutral position, and the tissues surrounding the acetabulum are retracted with Gelpi retractors to check for potential impingement from the exuberant joint capsule, which, if present, is removed.
Reduction in the hip joint: The suitable neck and ceramic head are assembled without touching the conical peg of the neck and impacted with a few strikes of a Teflon impactor. After insertion of the neck and head inside the cup, the femur is retracted laterally and distally with a pointed bone holding forceps fixed at the greater trochanter. The peg of the femoral stem is guided until it enters the recess of the neck. To complete the insertion of the femoral stem's peg inside the neck's cavity, the trochanter is pushed ventrally until the peg will lock inside the neck. It is essential to check if any soft tissue is entrapped between the head and the acetabular cup and, if trapped, must be removed. The stability of the reduction is tested using the baby Hohmann retractor doing the pull-down test to evaluate the tightness of the reduction (1 mm is the maximal subluxation tolerated) and the pull-up test to check for proper ALO of the acetabular component. Gentle external rotation of the femur to test the resistance to cranial-dorsal dislocation and full flexion with gentle internal rotation to test for caudo-ventral dislocation. Closure of the surgical site is performed similarly to standard-sized THA.
Postoperative radiographs: Four radiographic views are required to evaluate the proper positioning and orientation of the implants. Ventro-dorsal/frog leg view of the pelvis (avoid extending the pelvic limbs, this will strain the sutures of the deep gluteal tendon repair). The pelvis needs to be positioned correctly (not tilted right or left), to evaluate the proper positioning, orientation and proper impaction of the cup. A lateral view of the pelvis with perfect superimposition of the ilium bodies and wings is required to measure the ALO, using the formula sin-1 of the short diameter (dorsal-ventral) divided by the long diameter (cranio-caudal) of the oval projection of the cup.[10] [11] The retroversion of the cup is measured between the axis joining the centre of a circle inscribed in the wing of the ileum and the centre of a circle on the ischial tuberosity, with the long axis of the cup. A mediolateral view of the femur with the stifle positioned at 90 degrees with superimposition of the femoral condyle is required to measure the stem ante-version, which should be converted to the actual ante-version using the formula: real anteversion = sin-1 [(tan 55 degrees) × (tan of measured angle)], which consider the 135 degrees of the inclination angle of the neck.[10] [11] A caudo-cranial projection of the proximal femur, keeping the femur perpendicular to the pelvis and externally rotated away from the table by 60 to 70 degrees, makes the beam perpendicular to the stem and the pelvis is tilted, making the beam perpendicular to the cup. This view is used to evaluate the contact of the stem to the medial femoral cortex, proper locking of the screws in the femur, the centring of the cup about the cranial and caudal acetabular pillars, and to evaluate appropriate seating of the cup inside the acetabulum.
Postoperative care: All cases were discharged from the hospital 24 hours after the surgery. Antibiotics medications (amoxicillin-clavulanic acid, Konclav, ATI, Italy, 20 mg/kg three times daily per os) were given for 5 days and non-steroidal anti-inflammatory drugs were prescribed (meloxicam, Rheumocam Teknofarma, Italy, 0.7 mg/kg, once daily, for 5 days and then on alternated days for 2 weeks). Sedation was recommended, especially in young dogs, to keep them sedated for the first 3 to 5 weeks (trazodone, Trittico 150 mg retard tablets, ACRAF Italy, 7 to 10 mg/kg twice daily), or acepromazine (Killitam, ATI, Italy, 2–20 drops as needed) or gabapentin (Pfizer, Italy, 300 mg tablets, twice daily or thrice daily). Confinement in an intimate environment with non-slip flooring was required for 2 months, leash walking was allowed, and off-leash activity was not permitted (no running, jumping, or playing with other dogs). After the clinical and radiographic re-examination check 2 months following surgery, regular free activity was gradually permitted in the following month.
Re-examination checks were mandatory to be included in this study, to receive objective feedback on the outcomes and identify any possible complications present, even without clinical signs. The first re-examination check was required after 2 months; the second 8 to 10 months after.
Data Collection
Signalment (breed, sex, body weight and body condition score), underlying hip joint disease or trauma, side of arthroplasty, implant size and implant positioning were recorded. Pre-operative radiographic views with calibrated digital radiography were required with five radiographic views: ventrodorsally views in the hip-extended and hip flexed positions, aiming for the most symmetrical view of the ilium, oblique view of the pelvis with the radiographic beam tangential to acetabulum including the proximal part of the femur held perpendicular to the pelvis, and with 60 to 70 degrees external rotation to obtain a craniocaudal view and a mediolateral view of the femur with the stifle at 90 degrees and superimposition of the femoral condyles. All radiographic projections were obtained with fluoroscopic guidance for accurate positioning.
Postoperative radiographic evaluation: implant positioning ([Fig. 8]) was evaluated for the acetabular cup, the ALO, the retroversion angle and for the stem version angle. Cup positioning was calculated from a lateral–lateral radiographic image of the pelvis. Stem positioning was measured as previously described from a mediolateral radiographic image of the entire femur with the stifle at 90 degrees, with superimposition of the femoral condyles. All complications were recorded. A complication was defined as any event resulting in any outcome other than the normal function of the prosthesis. Any revision procedures were documented.
In-Hospital Follow-Up Assessment
For inclusion in the study, follow-up examinations were required at a minimum of 2 months and when available at 6 months postoperatively or/and later. At each follow-up, all patients underwent a physical and orthopaedic examination that included hind limb muscle mass evaluation, hip range of motion to assess for pain or discomfort, video recording of dogs when walking toward and away from the camera and side views. Video recordings of cats at home were provided by the owners. Any abnormal findings were documented. A minimum of four radiographic projections were taken during each follow-up examination: a lateral view of the pelvis with ileum and ischium bodies superimposed, a ventrodorsally view of the hip with the hind limbs in extension, an oblique view of the pelvis so that the radiographic beam was tangential to the cup equator, and the femur externally rotated so that the radiographic beam was perpendicular to the stem screws, and a mediolateral view of the femur with the stifle at 90 degrees and femoral condyles superimposed. Radiographs were assessed for any evidence of cup or stem failure or loosening, change in position, migration, bone remodelling or radiolucent zones. The follow-up radiographs were compared with the radiographs taken preoperatively ([Fig. 9]) and immediately postoperatively, and any changes noticed on the radiographs were recorded. Intraoperative and postoperative complications were recorded. Cup loosening was defined as a radiolucent zone around the acetabular component. Stem loosening was defined as two or more screws with radiolucent lines or an increase in the gap of the femoral prosthesis at the level of the medial cortex of the femur. A good clinical outcome was defined as a regular functioning prosthesis, at the last follow-up.
Statistical Analysis
Only descriptive statistics were performed using ‘R-4.0.5 for Windows’, available under the General Public License (R Core Team; 2013). Frequencies for nominal variables were described, and for continuous data, normality was assessed using Shapiro–Wilk normality test. Then, variables were reported as mean and standard deviation.
Results
59 THAs in 50 animals were performed using the Mini Zurich cementless total hip system between January 2020 and July 2021 at the Clinica Veterinaria Vezzoni, Cremona, Italy, by the same surgeon (A.V.: 56 cases) and at VA-MD College of Veterinary Medicine, USA, by the same surgeon (O.L.: 3 cases). There were eight cats and 42 dogs, with three cats and six dogs having bilateral THAs performed at an interval variable from 2 months to 1 year.
Among the eight cats, there were three females and five males. The mean body weight was 6.5 kg (standard deviation [SD] 2.4); the median age was 24 months, (range: 11–37 months). Breeds included were as follows: Maine Coon cat (n = 5), Domestic Shorthair cat (n = 2), and British Shorthair cat (n = 1).
In the group of 11 THAs in cats, capital physeal fracture was the reason for performing a THA in 6 cases (60%), hip dysplasia was the underlying reason in 4 patients (30%), and hip luxation in 1 cat (10%).
In the 11 THAs in cats, the 10 mm cup for 6 mm head was used in 2 cases (18.3%), the 12 mm cup for 8 mm head was used in 4 patients (36.3%), the 14 mm cup for 8 mm head was used in 1 case (9.1%), the 14 mm cup for 10 mm head was used in 4 cases (36.3%). The 3 mm femoral stem was used in 2 cases (18.2%), the 4 mm femoral stem was used in 5 cases (45.5%) and the 5 mm femoral stem was used in 4 cases (36.3%). Among all neck sizes, the short neck was used in 6 cases (54.6%), the medium neck in 3 cases (27.2%) and the long neck in 2 cases (18.2%).
Among the 43 dogs 25 were females and 18 were male. The mean body weight was 9.2 kg (SD: 4.9); the median age was 25 months (range: 4–114 months). Breeds included were as follows: Toy Poodle (n = 7), Jack Russell Terrier (n = 6), Cocker Spaniel (n = 4), Maltese (n = 4), mixed breed dog (n = 4), Border Collie (n = 3), Yorkshire Terrier (n = 2), American Cocker Spaniel (n = 1), Bolognese (n = 1), Breton (n = 1), English Setter (n = 1), French Bulldog (Bouledogue Français) (n = 1), Labrador (n = 1), Maltipoo (n = 1), Piccolo Levriere Italiano (n = 1), Pinscher Toy (n = 1), Scottish Terrier (n = 1), Shetland Sheepdog (n = 1), West Highland White Terrier (n = 1), and mongrel (n = 1).
Among the 48 THAs in dogs, hip dysplasia was the underlying cause for performing THA in 27 cases (56%), Legg-Perthes-Calvé disease in 12 patients (25%), traumatic luxation with underlying hip dysplasia in 4 dogs (8.5%), capital physeal fracture in 4 cases (8.5%), and lastly, traumatic femoral head fracture in one adult dog (2%).
In the 48 THAs in dogs, the 10 mm cup for 6 mm head was used in one case (2%), the 12 mm cup for 8 mm head was used in 16 cases (33%), the 14 mm cup for 10 mm head was used in 8 cases (16%), the 16 mm cup for 10 mm head was used in 5 cases (10%), the 18 mm cup for 12 mm head was used in 9 cases (18%), the 20 mm cup for 12 mm head was used in 3 cases (6%), and the 21 mm cup for 16 mm head was used in 7 cases (hybrid combination with standard system) (15%).
The 3 mm femoral stem was used in 9 cases (18%), the 4 mm femoral stem was used in 14 cases (29%), the 5 mm femoral stem was used in 9 cases (18%), and the 6 mm femoral stem was used in 17 cases (7 L and 10 XL) (35%). Among all neck sizes, the short neck was used in 27 cases (56%), the medium neck in 18 cases (38%), and the long neck in 3 cases (6%).
Intraoperative Complications
Three trochanteric fractures were repaired with a plate (1 ALPS 8 [Kyon AG, Zurich, CH] with ten holes and 3 + 3 screws, 1 ALPS 5 with 11 holes and 3 + 3 screws and 1 ALPS 3.5 with 11 holes and 3 + 3 screws). Two screws subsided and were stripped (4th screw distal hole in the femoral implant) in the 3 mm stem, which was replaced with a bicortical screw. Reinforcement of the femur with cerclage wires to reduce the risk of femoral fractures in aged dogs (8 years or more) was used in 6 and with an ALPS plate in 4 dogs, according to the increased risk of peri-prosthetic femoral fracture in older dogs with severe OA experienced with standard Zurich THR.[15] [16] [17]
Postoperative Radiographic Findings
The ALO, cup retroversion and stem ante version were measured in all cases. In the 48 THAs in dogs, ALO average was 43.5 degrees and median 43 degrees (min 35–max 56 degrees), SD 4.5; average cup retroversion was 20.3 degrees and median 20 degrees (min 0–max 40 degrees), SD 7.5; average stem ante version was 21.6, median 20.8 degrees (min 11–max 49 degrees), SD 5.7.
In the 11 THAs in cats, the ALO average was 43.5 degrees, median 43 degrees (min 40–max 54 degrees), average cup retroversion was 21.1 degrees, median 22 degrees (min 5–max 30 degrees) and average stem ante version was 19.3 degrees, median 17.7 (min 11.5–max 20.8 degrees), SD 3.2.
Postoperative Follow-Ups and Outcome
All dogs' radiographic and clinical follow-up examinations had a mean follow-up time of 7 months (SD: 4.51) and a median follow-up time of 8 months, with a range of 2 to 17 months and were available in all 48 cases (100%). All cats' radiographic and clinical follow-up examinations had a mean follow-up time of 9.4 months (SD: 4.23) and a median follow-up time of 10 months, with a range of 4 to 16 months and were available in all 11 cases (100%). Implant position and orientation were evaluated in the follow-up radiographs and no changes were noted compared with postoperative radiographs, except for the two below cases of cup dislodgement and loosening. Postoperative complications occurred in six dogs (12.5%) and one cat (9%). The remaining 52 cases showed normal gait at the last follow-up, without lameness or pain on manipulation of the operated leg.
A femoral fracture occurred way distal to the femoral implant 5 days following surgery in a very active cat, without involving the stem, which was repaired using a Synthes 2.4 LCP plate. The femoral fracture healed without further complications, with the latest follow-up at 9 months.
A cup dislocation occurred in the immediate postoperative period in a Border Collie, in which the 20 mm cup was not fully impacted. Surgical revision with a new 20 mm cup was successful after re-reaming the acetabulum deeper. At the 9-month follow-up, there was complete osteointegration of the acetabular cup, and the dog had a normal gait.
A ventro-caudal dislocation occurred 1 month after surgery in a Yorkshire Terrier, in which a 3 mm stem and a 10 mm cup with a 6 mm head were implanted. Two closed reductions and one surgical revision using a longer neck failed to resolve the dislocation. A second surgical revision was done, and the acetabular cup was replaced with a 12 mm and an 8 mm head, which successfully corrected the dislocation at the 8-month recheck. The increase in head diameter from 6 mm to 8 mm, increases the jump distance, which decreases the incidence of dislocation.
Another ventral dislocation occurred in a 2-year-old Cocker Spaniel 5 months following surgery while playing with another dog. The hip was reduced in a closed fashion and remained reduced at the 4-month recheck.
Asymptomatic loosening of a 21 mm cup occurred at the 2-month recheck in an English Setter. Surgical revision with a 23 mm cup was performed 5 months after the initial surgery because of a lack of osseointegration of the cup, presumably due to poor press fit. At the 3-month follow-up following the revision with a 23 mm cup, there was complete osseointegration of the acetabular cup, and the dog had a normal gait.
Stem-peg breakage of the 3 mm stem occurred in a Toy Poodle 8 months after surgery. The owner elected the explant of the implants.
The uncoupling of the neck on the peg of a 3 mm stem occurred in a Toy Poodle 15 months following surgery. During the revision surgery, the peg of the stem appeared worn and had wear marks on the inside of the neck. Therefore, removing the 3 mm stem through a lateral slot in the femur was necessary, and inserting a 4 mm stem. The femur was repaired using an ALPS 5 plate. At the 2-month follow-up, the stem showed osseointegration and the dog had a normal gait.
No other complications were noted in the follow-up period in the remaining dogs or cats. Also, there was no evidence of femoral or screw loosening in any of the cases. Complete osseointegration was confirmed at the last follow-up visit in all remaining cases.
In total, seven postoperative complications were encountered (12%), and all were solved without the need for the explanting of the prosthesis, except for one case because the owners were unwilling to have their dog undergo a revision.
Statistical Analysis
Continuous data normality was assessed using Shapiro–Wilk normality test. Then variables were reported in [Table 2] as the mean and standard deviation for dogs and cats.
Abbreviations: ALO, angle of lateral opening; BCS, body condition score; FU, follow-up; SD, standard deviation; THA, total hip arthroplasty.
Discussion
Feasibility and Surgical Issues
Our clinical experience demonstrated that the Cementless Z-Mini THR system is technically feasible and efficacious both in cats and small and toy breed dogs. While a long-term follow-up study would be required to establish the longevity of the implants, their osseointegration was apparent at the 2 to 3 months postoperative radiographs and remained stable in all the cases with long-term follow-up radiographs (12 months or longer in 26 cases). The surgical technique was like the standard Cementless Zurich total hip system, with dedicated instrumentation, which requires extreme precision in preparation and surgical execution. This is particularly true for the small stem sizes, the 3 to 5 mm stems, and the smaller cup sizes, 10 to 16 mm. Smaller-sized implants make less error margin in the femoral canal preparation and the acetabular reaming.[1] [2] The use of special flexible nitinol reamers for the femoral canal, which are available in 0.5 mm incremental sizes, was found to be extremely useful in entering the femoral canal, especially when combined with a high-speed burr. To achieve the proper press fit with the smaller diameter cups without an outer titanium shell, from 10 mm to 16 mm, careful and precise preparation of the acetabulum was required. In cats and dogs with low body weights, counter force during acetabular impaction was required and could be accomplished with the aid of a solid heavy instrument placed dorsal to the wings of the ilium.
Different Combinations of Implants in Dogs and Cats
Several combinations were possible with all sizes of implants used for small dogs and cats in this study. Combining the same stem size with different cup sizes and vice versa was beneficial given the differences in anatomy, especially in small animals. Small dogs routinely required smaller stems and larger cups compared with cats of similar body weight, where larger stems and smaller cups were needed. The significant difference in size between the 3 and 4 mm femoral stems necessitated the production of a narrow 4 mm stem (4N-SN) ([Fig. 1]), which became available after this study. It will be used in cases where a 3 mm stem will be too small, and a regular 4 mm stem will be too large. This new stem was used in the 3 mm stem revision discussed above.
Implant Orientation and Intraoperative Fluoroscopy Guidance
The use of intraoperative fluoroscopy is of great help in standard THA procedures. Still, it has proved essential in these smaller patients. The positioning of smaller patients undergoing a THA procedure should be verified with fluoroscopy before starting surgery to assure the anatomical landmarks are accurate. It was again used to check the orientation of the cup after partial and after complete impaction. The low body mass of these patients made them prone to pelvic displacement during routine surgical manoeuvres; therefore, it was essential to perform fluoroscopy to verify the orientation of the cup.
Cup, Appropriate Size with a Good Press Fit
In small dogs, especially cats, which have a shallow acetabulum, it is highly recommended to use a cup size that provides adequate coverage from the cranial and caudal pillars and to resist the temptation of using a larger cup. The wear of the cup in small patients is most likely minimal, due to the light body weight and the resistance to wear in vitro of ceramic head on CFR-PEEK liner[18]; therefore, most probably it is not necessary to resort to a larger cup size. One reason for increasing the cup diameter is to use a larger head. Still, apart from the Yorkshire, in which a 6 mm head was initially used, and that dislocated, the incidence of dislocation with the other small diameter heads (8, 10, and 12 mm) was not significant (two cases, 3%). Achieving the press-fit in most miniature cups, from 10 mm to 16 mm in diameter, requires extreme care when reaming the acetabulum. The final reaming is performed by hand or low-speed power with the acetabular reamer that is the same size in diameter as the intended cup. It is imperative not to wobble the acetabular reamer during the final reaming process, as this could cause the cup not to press fit in the acetabulum. The acetabulum and the cup must be thoroughly dry to achieve maximum contact of the cup to the bone. Indeed, the smaller the cup, the more difficult it is to prepare the acetabulum to obtain a proper press fit. If the press fit is not obtained, one should ream deeper with the previous small-sized reamer. This will keep the pole of the cup from prematurely contacting the medial wall before a press-fit is obtained. It is essential to remember that in smaller patients, the assistant must effectively counteract the mallet's impact during the cup's impaction.
Complications and Their Management
Seven postoperative complications occurred among 59 cases (12%), and all were successfully revised except one, in which the owner refused a revision surgery.
Two complications among 7 (29%) occurred in cases with the 3 mm stem, highlighting how the smaller femoral stem is at greater risk of complications. The use of a 4 mm narrow stem instead of a 3 mm stem when feasible seems to be a possibility to reduce this risk. Following these complications, the manufacturer changed the peg's design to increase its mechanical strength. Furthermore, the manufacturer added a size 4 narrow stem (4N-SN) ([Fig. 1]), which permits a stem with a more robust peg to be used in cases when a patient is close to the upper weight limit for a size 3 stem. Although it is advisable to use the widest stem possible depending on the size of the femoral canal, the ratio of stem size to patient weight, as indicated in [Table 1], must be respected to avoid breakage risk. The patient's weight must then be maintained throughout life to compatibility with the implant used. Postoperative ventral-caudal dislocation occurred in two cases, while no matter had a cranial-dorsal dislocation. While the incidence of postoperative dislocation is reported to be greater in the cranial-dorsal direction in the standard THAs,[16] [17] [19] [20] this difference in the mini-THAs could indicate that too closed an ALO should be avoided with the mini-THAs. In the cases mentioned above, the ALO was less than 40 degrees. An intermediate cup size of 11 mm holding an 8 mm head was deemed to be more suitable instead of the 10 mm cup holding a 6 mm head, for higher resistance to luxation. This further size was asked from the manufacturer and it's now available, over the 13 mm cup size ([Fig. 3]).
Finally, as for the standard THAs, and all orthopaedic surgeries, a certain percentage of complications is unpredictable, despite proper procedure execution, due to the postoperative management of these cases. as for any orthopaedic surgeries.
Conclusions
The Zurich mini cementless total hip system overall performed well in the small breed dogs and cats in this study and was associated with an excellent outcome in 98% of cases. Of the seven complications encountered, five were all resolved with surgical revision, one complication was resolved with closed reduction and one was explanted. None of the dogs or cats in this study were too small for the available prosthesis. And in one patient only (1.7%), the prosthesis was explanted due to the owner's unwillingness to have a surgical revision. The Zurich mini cementless total hip system is a practical and effective surgical procedure for small-breed dogs and cats with hip disease.
Conflict of Interest
Aldo Vezzoni, Otto Lanz, Simona Boano and Alyssa Sacristani received honoraria as Z-THR course instructors; Otto Lanz is a payed scientific consultant of Kyon. Stephen Bresina is employed by Kyon as Chief Technology officer. Implants for the first 25 cases were donated by Kyon.
Acknowledgments
The authors acknowledge Slobodan Tepic for continued support and contributions toward refining and perfecting THA in small animals, and Dario Drudi for the statistical analysis.
-
References
- 1 Liska WD. Micro total hip replacement for dogs and cats: surgical technique and outcomes. Vet Surg 2010; 39 (07) 797-810
- 2 Marino DJ, Ireifej SJ, Loughin CA. Micro total hip replacement in dogs and cats. Vet Surg 2012; 41 (01) 121-129
- 3 Ireifej S, Marino D, Loughin C. Nano total hip replacement in 12 dogs. Vet Surg 2012; 41 (01) 130-135
- 4 Liska WD, Doyle N, Marcellin-Little DJ, Osborne JA. Total hip replacement in three cats: surgical technique, short-term outcome and comparison to femoral head ostectomy. Vet Comp Orthop Traumatol 2009; 22 (06) 505-510
- 5 Schnabl-Feichter E, Schnabl S, Tichy A, Gumpenberger M, Bockstahler B. Measurement of ground reaction forces in cats 1 year after femoral head and neck ostectomy. J Feline Med Surg 2021; 23 (04) 302-309
- 6 Off W, Matis U. Excision arthroplasty of the hip joint in dogs and cats. Clinical, radiographic, and gait analysis findings from the Department of Surgery, Veterinary Faculty of the Ludwig-Maximilians-University of Munich, Germany. 1997. Vet Comp Orthop Traumatol 2010; 23 (05) 297-305
- 7 Marcellin-Little DJ, DeYoung BA, Doyens DH, DeYoung DJ. Canine uncemented porous-coated anatomic total hip arthroplasty: results of a long-term prospective evaluation of 50 consecutive cases. Vet Surg 1999; 28 (01) 10-20
- 8 Montgomery RD, Milton JL, Pernell R, Aberman HM. Total hip arthroplasty for treatment of canine hip dysplasia. Vet Clin North Am Small Anim Pract 1992; 22 (03) 703-719 Review.
- 9 Drüen S, Böddeker J, Meyer-Lindenberg A, Fehr M, Nolte I, Wefstaedt P. Computer-based gait analysis of dogs: evaluation of kinetic and kinematic parameters after cemented and cementless total hip replacement. Vet Comp Orthop Traumatol 2012; 25 (05) 375-384
- 10 Tepic S. . Concepts of cementless Zurich prosthesis. Proceedings of the ESVOT 2004 Pre-congress Total Hip Replacement Seminar. Munich; 2004:18–20
- 11 Montavon P, Tepic S. . Clinical application of Zurich Cementless canine total hip prosthesis. Proceedings of 1st World Orthopaedic Veterinary Congress. Munich, Germany; 2002:150
- 12 Guerrero TG, Montavon PM. Zurich cementless total hip replacement: retrospective evaluation of 2nd generation implants in 60 dogs. Vet Surg 2009; 38 (01) 70-80
- 13 Vezzoni L, Vezzoni A, Boudrieau RJ. Long-term outcome of Zürich cementless total hip arthroplasty in 439 cases. Vet Surg 2015; 44 (08) 921-929
- 14 Lanz OI, Forzisi I, Vezzoni A. Zurich cementless dual mobility cup for canine total hip prosthesis: implant characteristics and surgical outcome in 105 cases. Vet Comp Orthop Traumatol 2021; 34 (04) 294-302
- 15 Pozzi A, Peck JN, Chao P, Choate CJ, Barousse D, Conrad B. Mechanical evaluation of adjunctive fixation for prevention of periprosthetic femur fracture with the Zurich cementless total hip prosthesis. Vet Surg 2013; 42 (05) 529-534
- 16 Hummel DW, Lanz OI, Werre SR. Complications of cementless total hip replacement. A retrospective study of 163 cases. Vet Comp Orthop Traumatol 2010; 23 (06) 424-432
- 17 Vezzoni A. . Complications of total hip replacement with the Zurich cementless system. Chapter 114. In: Dominique Griffon, Annick Hamaide, eds. Complications in Small Animal Surgery. First ed. New York: John Wiley & Sons, Inc.; 2016
- 18 Brockett C, John G, Williams S, Isaac G, Fisher J. Wear of ceramic-on-carbon fibre reinforced PEEK hip replacements. Orthop Proc 2018; 94: 21
- 19 Nelson LL, Dyce J, Shott S. Risk factors for ventral luxation in canine total hip replacement. Vet Surg 2007; 36 (07) 644-653
- 20 Dyce J, Wisner ER, Wang Q, Olmstead ML. Evaluation of risk factors for luxation after total hip replacement in dogs. Vet Surg 2000; 29 (06) 524-532
Address for correspondence
Publikationsverlauf
Eingereicht: 04. Juli 2022
Angenommen: 21. Oktober 2022
Artikel online veröffentlicht:
24. Februar 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Liska WD. Micro total hip replacement for dogs and cats: surgical technique and outcomes. Vet Surg 2010; 39 (07) 797-810
- 2 Marino DJ, Ireifej SJ, Loughin CA. Micro total hip replacement in dogs and cats. Vet Surg 2012; 41 (01) 121-129
- 3 Ireifej S, Marino D, Loughin C. Nano total hip replacement in 12 dogs. Vet Surg 2012; 41 (01) 130-135
- 4 Liska WD, Doyle N, Marcellin-Little DJ, Osborne JA. Total hip replacement in three cats: surgical technique, short-term outcome and comparison to femoral head ostectomy. Vet Comp Orthop Traumatol 2009; 22 (06) 505-510
- 5 Schnabl-Feichter E, Schnabl S, Tichy A, Gumpenberger M, Bockstahler B. Measurement of ground reaction forces in cats 1 year after femoral head and neck ostectomy. J Feline Med Surg 2021; 23 (04) 302-309
- 6 Off W, Matis U. Excision arthroplasty of the hip joint in dogs and cats. Clinical, radiographic, and gait analysis findings from the Department of Surgery, Veterinary Faculty of the Ludwig-Maximilians-University of Munich, Germany. 1997. Vet Comp Orthop Traumatol 2010; 23 (05) 297-305
- 7 Marcellin-Little DJ, DeYoung BA, Doyens DH, DeYoung DJ. Canine uncemented porous-coated anatomic total hip arthroplasty: results of a long-term prospective evaluation of 50 consecutive cases. Vet Surg 1999; 28 (01) 10-20
- 8 Montgomery RD, Milton JL, Pernell R, Aberman HM. Total hip arthroplasty for treatment of canine hip dysplasia. Vet Clin North Am Small Anim Pract 1992; 22 (03) 703-719 Review.
- 9 Drüen S, Böddeker J, Meyer-Lindenberg A, Fehr M, Nolte I, Wefstaedt P. Computer-based gait analysis of dogs: evaluation of kinetic and kinematic parameters after cemented and cementless total hip replacement. Vet Comp Orthop Traumatol 2012; 25 (05) 375-384
- 10 Tepic S. . Concepts of cementless Zurich prosthesis. Proceedings of the ESVOT 2004 Pre-congress Total Hip Replacement Seminar. Munich; 2004:18–20
- 11 Montavon P, Tepic S. . Clinical application of Zurich Cementless canine total hip prosthesis. Proceedings of 1st World Orthopaedic Veterinary Congress. Munich, Germany; 2002:150
- 12 Guerrero TG, Montavon PM. Zurich cementless total hip replacement: retrospective evaluation of 2nd generation implants in 60 dogs. Vet Surg 2009; 38 (01) 70-80
- 13 Vezzoni L, Vezzoni A, Boudrieau RJ. Long-term outcome of Zürich cementless total hip arthroplasty in 439 cases. Vet Surg 2015; 44 (08) 921-929
- 14 Lanz OI, Forzisi I, Vezzoni A. Zurich cementless dual mobility cup for canine total hip prosthesis: implant characteristics and surgical outcome in 105 cases. Vet Comp Orthop Traumatol 2021; 34 (04) 294-302
- 15 Pozzi A, Peck JN, Chao P, Choate CJ, Barousse D, Conrad B. Mechanical evaluation of adjunctive fixation for prevention of periprosthetic femur fracture with the Zurich cementless total hip prosthesis. Vet Surg 2013; 42 (05) 529-534
- 16 Hummel DW, Lanz OI, Werre SR. Complications of cementless total hip replacement. A retrospective study of 163 cases. Vet Comp Orthop Traumatol 2010; 23 (06) 424-432
- 17 Vezzoni A. . Complications of total hip replacement with the Zurich cementless system. Chapter 114. In: Dominique Griffon, Annick Hamaide, eds. Complications in Small Animal Surgery. First ed. New York: John Wiley & Sons, Inc.; 2016
- 18 Brockett C, John G, Williams S, Isaac G, Fisher J. Wear of ceramic-on-carbon fibre reinforced PEEK hip replacements. Orthop Proc 2018; 94: 21
- 19 Nelson LL, Dyce J, Shott S. Risk factors for ventral luxation in canine total hip replacement. Vet Surg 2007; 36 (07) 644-653
- 20 Dyce J, Wisner ER, Wang Q, Olmstead ML. Evaluation of risk factors for luxation after total hip replacement in dogs. Vet Surg 2000; 29 (06) 524-532