

Subscribe to RSS
DOI: 10.1055/s-0043-1761283
Facilitators and Challenges in Patient's Satisfaction with Quality of Cervical Cancer Care in a Tertiary Care Hospital, Puducherry, India: A Qualitative Study
Authors
Funding None.

Abstract

Background Chronic diseases require more attention in terms of patient satisfaction due to their physically and mentally exhausting nature. Cancer burden in India for 2021 was 26.7 million disability-adjusted life years (DALYs), and is projected to rise to 29.8 million by 2025. The second most common cause of cancer DALYs among females was cervix uteri (98.6 per 100,000). Evaluation of factors that influence satisfaction can assist in finding solutions to improve the quality of services provided.
Methods This study was conducted in the Regional Cancer Centre, Puducherry. One focused group discussion (FGD) was conducted among seven cervical cancer patients and eight key informant interviews (KII) with their healthcare providers (HCPs). The details collected included perceptions of patient satisfaction, difficulties they faced in achieving patient satisfaction, and possible recommendations for improvement. Thematic analysis was done after preparing transcripts.
Results The major facilitating factors reported were proper information exchange, the approachability of staff, and assisting patients with transportation concession certificates. Obstacles highlighted by patients included lack of family support, side effects of treatment, inability to do routine work, and long travel time. HCP reported misalignment between and within departments, overworked staff, lack of equipment for smooth telemedicine services, and inadequate space for OPD, counseling, and waiting as barriers to providing satisfactory services to patients.
Conclusions Most challenges were attributed to overworked staff, inequitable distribution of cancer center, and patients' knowledge and understanding of disease. Therefore, it is important to make patients aware of the disease, treatment, and value of the quality of life. It can enable them to make better use of resources, in addition to improvements in the health system.
Keywords
barriers - challenges - facilitators - oncology care - patient satisfaction - quality of care - uterine cervical neoplasmsIntroduction
Globally, noncommunicable diseases (NCDs) accounted for 71% of total deaths in 2019; out of these, 22% were from cancer alone.[1] In India, the cancer burden for 2021 was 26.7 million disability-adjusted life years (DALYs), with an expected rise to 29.8 million by 2025. The second most common cause of cancer DALYs among females was cervix uteri (98.6 per 100,000).[2] The International Classification of disease-10: C-53 indicated a belt of high incidence rates of cervical cancer in the North Eastern districts of Tamil Nadu state, including Pondicherry, which had the highest age-adjusted incidence rates of 39.2/100,000.[3]
In recent years, there has been a significant shift in the way patients are treated. An approach that views patients holistically and their illness as a complex event involving numerous yet interconnected levels, including biological, psychological, and social.[4] Patient-centered care has been found to improve outcome measures such as patient satisfaction, treatment adherence, and self-care, leading to long-term health benefits.[5] “Closing the care gap” is the need of the hour to focus on quality cancer care and address the inequalities and inequities in care with priority on breast and cervix cancer, as highlighted by the World Health Organization (WHO). This study attempts to contribute to this by exploring factors influencing patient satisfaction with cancer care quality.[6]
It is critical to include service users' and providers' perspectives when evaluating the quality of services.[7] [8] Respecting the patient's needs, preferences, and being sensitive to aspects of care other than medical aids helps in providing patients centered care.[9] Studies have shown that all patient needs are interconnected, therefore, identifying these issues early and providing the necessary support can help alleviate the problems of patients to a large extent.[10] Despite the widespread use and adaptation of patient satisfaction questionnaires, a survey may still have limitations in fully understanding needs, preferences, and attitudes; we addressed this in our study through qualitative research. The aim of this research is to look into the factors that influence cervical cancer patients' satisfaction.
Materials and Methods
Study Design and Settings
This qualitative research was undertaken as part of a larger study in the regional cancer center (RCC) of a tertiary care hospital, Puducherry, from January 2021 to July 2022. RCC offers services to around 3,000 new patients and 40,000 on follow-up every year. Out of these, around 18% are cervical cancer patients. Ethical clearance was obtained from the Institutional Ethics Committee (JIP/IEC/2021/148, date of approval of ethics is 05/05/2021).
Study Participants, Sample Size, and Sampling Procedure
Focused group discussion (FGD) was conducted among seven cervical cancer patients attending RCC and key informant interviews (KII) were conducted among eight HCP including consultants, junior residents, senior residents, staff nurses, radiation technologists, and medical-social worker from RCC selected through purposive sampling technique.
Study Procedure
After obtaining approval from institutional scientific and ethics committees, the study was conducted to explore patients' views, perceptions, and experiences on challenges and facilitating factors to satisfaction with the quality of care.
Data collection was done using a semistructured pretested interview guide. It was prepared through a review of literature, expert opinions, and discussions with a few cancer patients followed by review from two experts in qualitative research.
The aim of FGD was explained to study participants. A researcher fluent in Tamil conducted the FGD lasting typically 40 to 45 minutes, it was recorded after obtaining consent. The confidentiality of the information gathered was ensured.
Similarly, KII were conducted after explaining the aim of the study and taking consent. Interviews were carried out until the point of theoretical saturation with each session lasting for 15 to 20 minutes. To explore the health system perspective, the domains used were: (i) factors influencing satisfaction, (ii) quality of service delivery, (iii) manpower, (iv) infrastructure, and (v) suggestions for improvement. To explore the individual and societal perspective, the domains used were (i) importance of satisfaction, (ii) satisfactory factors if any, (iii) reasons for dissatisfaction.
Data Analysis
The recorded audio content from both were transcribed using the Microsoft Word. Codes, categories, and themes were generated based on the participant's statements. Statements were used as the unit of analysis; similar codes were grouped to form subthemes followed by themes.
Results
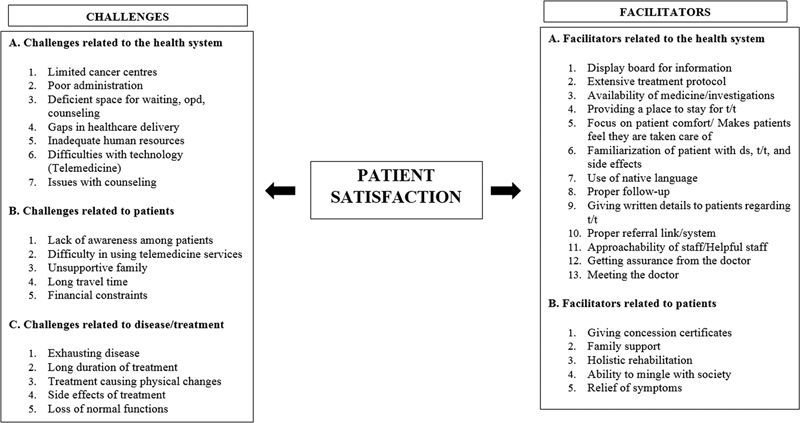
Qualitative exploration of HCP and patient's perception of factors influencing satisfaction with the quality of cervical cancer care. There were two main themes that were drawn from the interviews ([Fig. 1]):
-
Challenges in achieving patient satisfaction ([Supplementary Table S1], available in the online version)
-
Facilitators for patient satisfaction ([Supplementary Table S2], available in the online version)
Theme 1: Challenges in Achieving Satisfaction Among Cervical Cancer Patients Taking Treatment in RCC
Health System Factors
The qualitative findings revealed some challenges that could lead to decreased satisfaction, such as limited dedicated cancer centers and their unequal distribution that make services difficult to access. According to HCP and patients, centers available are also not properly equipped, which is one of the main causes of overcrowding. According to patients, gaps, such as unspecified appointment time, result in overcrowding and increased waiting time. Despite adequate treatment quality, both patient's and HCP's felt patient satisfaction was compromised due to lack of communication and less time for individual patients. The majority of HCPs believed there was a management gap between departments and within the RCC, lack of clear guidelines and synchronization between tests appointments and other services lead to an increased number of visits. The availability of space for conducting outpatient departments (OPDs) and counseling was limited, which compromised patient's privacy. Patients, in contrast, were not dissatisfied with the infrastructure, but they did mention having to wait in parking. Other challenges with counselling included the rotation of staff and limited sessions. HCPs believed that counseling is effective if continued for multiple sessions because patients get familiar with the staff over time, but staff rotation could send them back to their shells. They also expressed handling multiple responsibilities at once could interfere with continuity and privacy during counseling.
Due to an increasing number of cases, the workload was more on the existing workforce. Language barrier was an added disadvantage according to both stakeholders as it limited the involvement of the available staff with the patients from different states and vice versa. Despite the fact that patient sheets were kept and follow-up schedules were tracked by HCPs, there was a delay in treatment due to an unknown test schedule and an inability to get appointments as expressed by patients. Some patients were sceptical of telemedicine, while others did not own phones at all. This, in conjunction with a lack of technological literacy, made it difficult for patients to get appointments and for HCPs to serve the target population. Inadequate phones and staff in the hospital was also an obstacle.
“When I was diagnosed, initially I went to some other places but no treatment was available there for cancer.” Patient
“I have taken all scans on time but it will take the whole day. We're coming from a long distance, so we have to finish in and go.” Patient
“Sometimes they speak in English, which is difficult to understand” Patient
“In a government set up with a high volume of patients it is very difficult to like give so much time to a single patient. Maximum we can give around 10 to 15 minutes probably for a new patient or else for a follow up patient 5 to 10 minutes is maximum.” Senior Resident
“A counselling session should last at least two to three days. When we have a consistent relationship with a patient, she will gain confidence and establish a rapport. If I begin therapy with the patient, 2-3 people will intervene, and we will lose continuity.” Medical social worker
Patient Factors
HCPs believed the lack of knowledge/myths related to disease and treatment among patients, least bothered and different caregivers for each visit were some of the challenges. Patient's reported loss of wages, travel expenses, and family-related factors such as the lack of support from family members as major obstacles that had an impact on satisfaction with the quality of care.
Underutilization of resources such as counseling was assumed due to unwillingness on the patient's part or lack of knowledge about their existence. Some of the patients talked about the difficulty in accessing the services and loss of wages for patients as well as attenders because of long distance. Some patients considered their dependence on family members for daily activities to be a barrier and feared being left alone.
“People take it as current, shock therapy. Some patients even after explaining deny the treatment.”
“Some patients are willing to continue t/t but family members are not supportive, for them, it's waste of time”- hyphen before the name of participant for the verbatim (statements) can be removed, as it is not present uniformly for all statements Medical social worker
“I have a daughter. Another daughter has a job. She will take leave and come with me.”
“I have to get up early, make Tiffin, get a bus and come. We have to struggle a little for our needs.” Patient
Disease and Treatment-related Factors
HCPs informed that mental and physical burden due to cancer, years of treatment, and its side effects that make social mingling difficult are some of the reasons for nonadherence and dissatisfaction. Patients expressed how they were not able to do their daily activities and had side effects such as nausea and burning.
“My whole-body burns when I go out. I could not eat properly.”
“I was doing business in the village but after I got the disease, I'm always tired. I could not work.” Patient
“Convincing a patient for radiation and and convincing the patient to continue to come for six weeks is difficult.” Assistant Professor
Theme 2: Facilitators for Satisfaction Among Cervical Cancer Patients Taking Treatment in RCC
Health System Factors
The findings revealed HCPs make constant attempts to improve patient satisfaction by offering information about disease/treatment, being approachable, guiding patients regarding transportation concession certificates, focusing on relief of physical symptoms, presence of display board, and having a proper referral system, among other things.
Digital boards displaying side effects was a facilitator as they could disseminate necessary information to the masses at once. Patients perceived satisfaction as the availability of services in institution. HCPs stated they make conscious efforts to help patients throughout their treatment regarding their stays. They are referred to shelters if required by staff. Familiarizing the patient with the disease, treatment, and expected side effects was important part as it adjusts patient to the situation and decreases the chances of dropout. Other factors such as updating patients about their treatment progress increased patient's confidence. HCPs tried to develop trust and rapport with the patient by communicating at every point of care even if it is for a short duration. Patients also felt the helpful nature of the staff made their treatment process smooth. They also expressed that their symptoms were taken care of and doctor's provided assurance regarding their well-being. Telemedicine was a new concept for both the health system and patients. It helped HCP in streamlining the OPD by limiting the number of appointments. It also gave a sense of comfort to patients who had access to phones as they felt that the hospital is taking care of them.
“Even if I don't know, I can ask the security the correct way. Like. For doing the test you can go this way. Everybody will help Sir. Nobody will say they don't know.” Patient
“I contacted them through the phone, and they attended the call and gave an appointment. If we didn't do it on time, they will call us and give it.” Patient
“In our department, multiple people will be examining and cross-referring the findings. The patient will be satisfied.” Senior Resident
“We make the patient comfortable and explain what stage they are in and that cancer isn't the end of the world. We explain the therapy options and how long you must follow up, as well as what you will be going through.” Junior Resident
Patient Factors
HCPs felt providing bus and train concession forms to patients can decrease their financial burden. One of the staff is responsible for making people aware of the financial schemes available and also help them in the process of getting concession forms. In addition, patients felt having a supportive family was a facilitator in making the treatment process better. Another important facilitator was the quality of life. Patients expressed that after the treatment they expect to go back to their normal life, earn their livelihood, do daily activities, and have social relations. That is also the ultimate goal of HCPs, they focus on technicalities of treatment to give the best possible care to the patient and make them disease-free or at least relieve their physical symptoms.
“I was in the worst condition, but now I'm feeling well. I was not able to go to work, but now I am able to work normally.” Patient
“They will take leave and come with me. They will wait with me the whole time and take me back. They are very supportive.” Patient
“One medical social worker to explain the same and for travel and all that will be very expensive for travel, bus concession and all certificates are being given and so that that will enhance their compliance mode and they'll be more satisfied to come for visits follow up often.” Junior Resident
Discussion
This study has highlighted the facilitators and challenges that patients encounter starting from their way to the hospital until follow-up care. These were related to health system, patients as well as nature of disease and treatment.
Health System Factors
Based on the general themes that emerge, patients and HCP have similar ideas about quality cancer care and patient satisfaction. The equitable distribution of centers, better information interchange, more care coordination, psychosocial support, and timely care were mentioned by patients and HCPs in the current study. The intensive treatment schedule had conflicting reactions from participants; some thought it built trust in the institute, while others felt it fatigued them. In a study conducted by Hess et al, similar results including coordination of care, communication, and information exchange were reported as impediments to healthcare quality. Hess et al suggested that multidisciplinary care should be provided at the time of an initial diagnosis.[11] Findings of a study by Suija et al were in line with our study, all patients felt that having enough information about cancer was of utmost importance for them.[12] This study reported health system related shortcomings, such as long waiting times for doctors' appointment, and overcrowded places similar to findings by Suija et al.[12]
According to our research, two-way communication is the most significant factor in patient satisfaction. It is critical to put patients at ease during treatment, which includes understanding about their social history and issues they are facing during treatment. Learning this aspect of patient care can broaden the oncologist's supportive role, especially during critical times for the patient and family, such as diagnosis, disease recurrence, and transition to palliative care, which is consistent with the work of Thorne et al, and Baile et al on patient–healthcare provider communication.[13] [14]
Oncologists, nurses, radiation technologists, and medical social workers work together to provide counseling. It was discovered that lack of exclusive space and employees leads to a lack of privacy. One of the issues raised by patients in our study was the lack of waiting areas in comparison to the patient load. A study conducted in Ethiopia by Haileselassie et al yielded similar results, study reported that due to a lack of room, dozens of cancer patients and their relatives gathered in stairwells and surrouned the oncology unit.[15] Our center employs people from all across the country, which creates language and cultural barriers. The effect of language barriers on communication between patients and HCPs has been reported by a number of other studies also.[16] [17] [18] [19] [20]
Patient-related Factors
The majority of the challenges reported by HCPs and patients in this study were due to a lack of knowledge among patients that resulted in myths, and the fear of disease and treatment. Some patients even thought of radiation as current and refused treatment, similar patient experiences were also explored in a study by Prue et al.[21] These factors may contribute to defaulting the treatment and can lead to relapse or recurrence, with increasing severity of difficult-to-manage symptoms. Lack of family support, long travel times, wage loss, and a lack of information about the significance of treatment continuation were also cited as reasons for default.
In this study, patients were of the opinion that emotional support is just as important as healthcare support, which is primarily provided by family members. This viewpoint is supported by the work of Johanne et al and Orri et al It suggests that caregiver response and involvement in patient care boosts patient satisfaction.[22] [23] Waiting time was one of the concerns raised by patients, but in our survey, patients had no concerns regarding waiting because they were aware that this center serves patients from multiple states. They were also grateful for having access to services.[20]
Disease and Treatment-related Factors
Cancer is generally viewed as a fatal disease, resulting in a vicious cycle of helplessness, exhaustion, inability to perform normal functions, and depression.[16] [24] The type of treatment also plays a factor in their degree of satisfaction, according to the current study. HCPs perceived that although the chosen treatment may be the best option, but its effects on physical appearance may make patients uncomfortable in social situations. In our study, patients expressed inconvenience due to side effects of radiation, leading to increased drop outs, which was also found in two studies by Sibeoni et al and Corner et al, which reported that side effects, such as nausea and vomiting or asthenia, have a significant impact on day-to-day quality of life.[25] [26]
This study focuses on relatively unexplored area of patient satisfaction using qualitative design, which is the major strength of the study as it helped in exploring the challenges and suggestions to overcome it. The study was prone to recall and social desirability bias; to avoid it, questions were asked in a neutral and nonthreatening manner by a researcher from another department. Purposive sampling technique used to select participants might have resulted in bias during data collection. The study gives rise to programmatic and research implications. The recommendations proposed by the participants were making already existing centers better equipped with technology and staff, recruiting the right mix of staff, making designated space for counseling, proper waiting area, allocating more resources for telemedicine, and focusing on the Health Management Information System (HMIS) to improve care coordination.
Conclusion
This study concludes that in addition to improvements in the health system, patients should be made aware of the disease, treatment, and importance of quality of life to make better use of resources. It is critical that the healthcare system prioritizes patient satisfaction alongside diagnosis and treatment technicalities.
Conflict of Interest
None declared.
Acknowledgments
The authors are grateful to the participants who volunteered, shared their difficulties, and came up with possible recommendations. Without their enthusiastic participation, cooperation, and support, this study would not have been possible. I express my gratitude to Dr. Kalaiselvi, and Dr. Arivarasan, for their input. I would also like to thank my friend Dr. Mayank Sharma for his support and help.
Ethical Approval
Ethical clearance was obtained from the Institutional Ethics Committee (JIP/IEC/2021/148, date of approval of ethics is 05/05/2021).
-
References
- 1 World Health Organization. World Health Statistics 2018: Monitoring Health for the SDGs, Sustainable Development Goals. Geneva: World Health Organization; 2018
- 2 Kulothungan V, Sathishkumar K, Leburu S. et al. Burden of cancers in India - estimates of cancer crude incidence, YLLs, YLDs and DALYs for 2021 and 2025 based on National Cancer Registry Program. BMC Cancer 2022; 22 (01) 1-12
- 3 National Centre for Disease Informatics and Research, Indian Council of Medical Research. Welcome to National Cancer Registry Programme. Accessed April 22, 2022, at: https://www.ncdirindia.org/ncrp/ca/chapter6_Report.aspx?SiteName=Cerv&ReportType=Dist_Graph&Sex=F&MyBtn=View+Graph
- 4 Organización Mundial de la Salud. Estrategias y Prácticas Mundiales de Inmunización Sistemática (GRISP): Documento Complementario al Plan de Acción Mundial Sobre Vacunas (GVAP). Organización Mundial de la Salud; 2017. Accessed May 26, 2022, : https://apps.who.int/iris/handle/10665/258600
- 5 Chan CMH, Azman WA. Attitudes and role orientations on doctor-patient fit and patient satisfaction in cancer care. Singapore Med J 2012; 53 (01) 52-56
- 6 World Health Organisation. World Cancer Day: closing the care gap. Accessed April 22, 2022, at: https://www.who.int/news/item/03-02-2022-world-cancer-day-closing-the-care-gap
- 7 Avis M. Incorporating patients' voices in the audit process. Qual Health Care 1997; 6 (02) 86-91
- 8 Bangalore Sathyananda R, Krumeich A, Manjunath U, de Rijk A, van Schayck CP. Providers' perspectives on the performance of primary healthcare centres in India: the missing link. Int J Health Plann Manage 2021; 36 (05) 1533-1552
- 9 Phd CB. Patient-centered Care Measures for the National Health Care Quality Report (Defining Patient-centered Care). Published online 2000
- 10 Daya AP, Sarkar S, Kar SS. Estimation of palliative care need in the urban community of puducherry. Indian J Palliat Care 2017; 23 (01) 81-87
- 11 Hess LM, Pohl G. Perspectives of quality care in cancer treatment: a review of the literature. Am Health Drug Benefits 2013; 6 (06) 321-329
- 12 Suija K, Ilves K, Ööpik P, Maaroos HI, Kalda R. Patients' experience with cancer care: a qualitative study in family practice. Eur J Gen Pract 2013; 19 (02) 111-116
- 13 Thorne S, Hislop TG, Kim-Sing C, Oglov V, Oliffe JL, Stajduhar KI. Changing communication needs and preferences across the cancer care trajectory: insights from the patient perspective. Support Care Cancer 2014; 22 (04) 1009-1015
- 14 Baile WF, Aaron J. Patient-physician communication in oncology: past, present, and future. Curr Opin Oncol 2005; 17 (04) 331-335
- 15 Haileselassie W, Mulugeta T, Tigeneh W, Kaba M, Labisso WL. The situation of cancer treatment in Ethiopia: challenges and opportunities. J Cancer Prev 2019; 24 (01) 33-42
- 16 Banaser M, Stoddart K, Cunningham N. A qualitative study of patient satisfaction in oncology wards setting in Saudi Arabia. Research & Reviews: Journal of Nursing and Health Sciences 2017; 3 (03) 85-97
- 17 (PDF) Culturally Sensitive Caring for Saudi Patients. . Accessed September 22, 2022, at: https://www.researchgate.net/publication/11414729_Culturally_Sensitive_Caring_for_Saudi_Patients
- 18 Atallah MA, Hamdan-Mansour AM, Al-Sayed MM, Aboshaiqah AE. Patients' satisfaction with the quality of nursing care provided: the Saudi experience. Int J Nurs Pract 2013; 19 (06) 584-590
- 19 Steven B, Lange L, Schulz H, Bleich C. Views of psycho-oncologists, physicians, and nurses on cancer care-a qualitative study. PLoS One 2019; 14 (01) e0210325
- 20 Nkrumah J, Abekah-Nkrumah G. Facilitators and barriers of patient-centered care at the organizational-level: a study of three district hospitals in the central region of Ghana. BMC Health Serv Res 2019; 19 (01) 900
- 21 Prue G, O'Connor D, Brown M, Santin O. Exploring patient experiences of cancer care in Northern Ireland: a thematic analysis of free-text responses to the 2018 Northern Ireland Patient Experience Survey (NICPES). BMC Health Serv Res 2021; 21 (01) 564
- 22 Bergerød IJ, Braut GS, Wiig S. Resilience from a stakeholder perspective: the role of next of kin in cancer care. J Patient Saf 2020; 16 (03) e205-e210
- 23 Orri M, Sibeoni J, Bousquet G. et al. Crossing the perspectives of patients, families, and physicians on cancer treatment: a qualitative study. Oncotarget 2017; 8 (13) 22113-22122
- 24 Horneber M, Fischer I, Dimeo F, Rüffer JU, Weis J. Cancer-related fatigue: epidemiology, pathogenesis, diagnosis, and treatment. Dtsch Arztebl Int 2012; 109 (09) 161-171 , quiz 172
- 25 Sibeoni J, Picard C, Orri M. et al. Patients' quality of life during active cancer treatment: a qualitative study. BMC Cancer 2018; 18 (01) 951
- 26 Corner J, Wagland R, Glaser A, Richards SM. Qualitative analysis of patients' feedback from a PROMs survey of cancer patients in England. BMJ Open 2013; 3 (04) e002316
Address for correspondence
Publication History
Article published online:
12 April 2023
© 2023. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 World Health Organization. World Health Statistics 2018: Monitoring Health for the SDGs, Sustainable Development Goals. Geneva: World Health Organization; 2018
- 2 Kulothungan V, Sathishkumar K, Leburu S. et al. Burden of cancers in India - estimates of cancer crude incidence, YLLs, YLDs and DALYs for 2021 and 2025 based on National Cancer Registry Program. BMC Cancer 2022; 22 (01) 1-12
- 3 National Centre for Disease Informatics and Research, Indian Council of Medical Research. Welcome to National Cancer Registry Programme. Accessed April 22, 2022, at: https://www.ncdirindia.org/ncrp/ca/chapter6_Report.aspx?SiteName=Cerv&ReportType=Dist_Graph&Sex=F&MyBtn=View+Graph
- 4 Organización Mundial de la Salud. Estrategias y Prácticas Mundiales de Inmunización Sistemática (GRISP): Documento Complementario al Plan de Acción Mundial Sobre Vacunas (GVAP). Organización Mundial de la Salud; 2017. Accessed May 26, 2022, : https://apps.who.int/iris/handle/10665/258600
- 5 Chan CMH, Azman WA. Attitudes and role orientations on doctor-patient fit and patient satisfaction in cancer care. Singapore Med J 2012; 53 (01) 52-56
- 6 World Health Organisation. World Cancer Day: closing the care gap. Accessed April 22, 2022, at: https://www.who.int/news/item/03-02-2022-world-cancer-day-closing-the-care-gap
- 7 Avis M. Incorporating patients' voices in the audit process. Qual Health Care 1997; 6 (02) 86-91
- 8 Bangalore Sathyananda R, Krumeich A, Manjunath U, de Rijk A, van Schayck CP. Providers' perspectives on the performance of primary healthcare centres in India: the missing link. Int J Health Plann Manage 2021; 36 (05) 1533-1552
- 9 Phd CB. Patient-centered Care Measures for the National Health Care Quality Report (Defining Patient-centered Care). Published online 2000
- 10 Daya AP, Sarkar S, Kar SS. Estimation of palliative care need in the urban community of puducherry. Indian J Palliat Care 2017; 23 (01) 81-87
- 11 Hess LM, Pohl G. Perspectives of quality care in cancer treatment: a review of the literature. Am Health Drug Benefits 2013; 6 (06) 321-329
- 12 Suija K, Ilves K, Ööpik P, Maaroos HI, Kalda R. Patients' experience with cancer care: a qualitative study in family practice. Eur J Gen Pract 2013; 19 (02) 111-116
- 13 Thorne S, Hislop TG, Kim-Sing C, Oglov V, Oliffe JL, Stajduhar KI. Changing communication needs and preferences across the cancer care trajectory: insights from the patient perspective. Support Care Cancer 2014; 22 (04) 1009-1015
- 14 Baile WF, Aaron J. Patient-physician communication in oncology: past, present, and future. Curr Opin Oncol 2005; 17 (04) 331-335
- 15 Haileselassie W, Mulugeta T, Tigeneh W, Kaba M, Labisso WL. The situation of cancer treatment in Ethiopia: challenges and opportunities. J Cancer Prev 2019; 24 (01) 33-42
- 16 Banaser M, Stoddart K, Cunningham N. A qualitative study of patient satisfaction in oncology wards setting in Saudi Arabia. Research & Reviews: Journal of Nursing and Health Sciences 2017; 3 (03) 85-97
- 17 (PDF) Culturally Sensitive Caring for Saudi Patients. . Accessed September 22, 2022, at: https://www.researchgate.net/publication/11414729_Culturally_Sensitive_Caring_for_Saudi_Patients
- 18 Atallah MA, Hamdan-Mansour AM, Al-Sayed MM, Aboshaiqah AE. Patients' satisfaction with the quality of nursing care provided: the Saudi experience. Int J Nurs Pract 2013; 19 (06) 584-590
- 19 Steven B, Lange L, Schulz H, Bleich C. Views of psycho-oncologists, physicians, and nurses on cancer care-a qualitative study. PLoS One 2019; 14 (01) e0210325
- 20 Nkrumah J, Abekah-Nkrumah G. Facilitators and barriers of patient-centered care at the organizational-level: a study of three district hospitals in the central region of Ghana. BMC Health Serv Res 2019; 19 (01) 900
- 21 Prue G, O'Connor D, Brown M, Santin O. Exploring patient experiences of cancer care in Northern Ireland: a thematic analysis of free-text responses to the 2018 Northern Ireland Patient Experience Survey (NICPES). BMC Health Serv Res 2021; 21 (01) 564
- 22 Bergerød IJ, Braut GS, Wiig S. Resilience from a stakeholder perspective: the role of next of kin in cancer care. J Patient Saf 2020; 16 (03) e205-e210
- 23 Orri M, Sibeoni J, Bousquet G. et al. Crossing the perspectives of patients, families, and physicians on cancer treatment: a qualitative study. Oncotarget 2017; 8 (13) 22113-22122
- 24 Horneber M, Fischer I, Dimeo F, Rüffer JU, Weis J. Cancer-related fatigue: epidemiology, pathogenesis, diagnosis, and treatment. Dtsch Arztebl Int 2012; 109 (09) 161-171 , quiz 172
- 25 Sibeoni J, Picard C, Orri M. et al. Patients' quality of life during active cancer treatment: a qualitative study. BMC Cancer 2018; 18 (01) 951
- 26 Corner J, Wagland R, Glaser A, Richards SM. Qualitative analysis of patients' feedback from a PROMs survey of cancer patients in England. BMJ Open 2013; 3 (04) e002316