

Subscribe to RSS
DOI: 10.1055/s-0043-117943
SpyGlass percutaneous transhepatic cholangioscopy-guided lithotripsy of a large intrahepatic stone
Authors
Corresponding author
Publication History
Publication Date:
19 September 2017 (online)

Occasionally, biliary stone management can be really challenging, depending on location, size, number, altered anatomy, and presence of strictures [1]. Although different approaches can be used in this setting, such as endoscopic retrograde cholangiopancreatography (ERCP), percutaneous transhepatic biliary drainage (PTBD), and extracorporeal shock wave lithotripsy or surgery [2], more complex cases may require management using a combination of techniques [3] [4] [5].
A 40-year-old woman presented with recurrent cholangitis due to right hepatolithiasis ([Fig. 1]). Past history included a failed ERCP, and subsequent cholecystectomy with biliary exploration at another hospital. First, left PTBD was performed to improve the patient’s clinical status. A multidisciplinary team then decided in favor of surgical bile duct exploration with hepaticojejunostomy; however, the right intrahepatic stone could not be identified, even with intraoperative ultrasound. Biliary exploration through the PTBD drain was scheduled for the postsurgical recovery period. Meanwhile, cholangitis recurred, and the patient underwent urgent right PTBD following discovery of a 1.7 cm biliary stone, which had impacted in the confluence of the right anterior and posterior sectoral biliary ducts ([Fig. 2]). Balloon fragmentation was attempted, but was not successful. In addition, a basket was not considered to be a safe method of retrieval because of the size of the stone.


After clinical recovery of the patient, the multidisciplinary team opted for a hybrid procedure involving access to the biliary tree through the right PTBD site and cholangioscopy-guided laser lithotripsy using the intraductal cholangioscopy system SpyGlass DS (Boston Scientific, Marlborough, Massachusetts, USA). Informed consent was obtained.
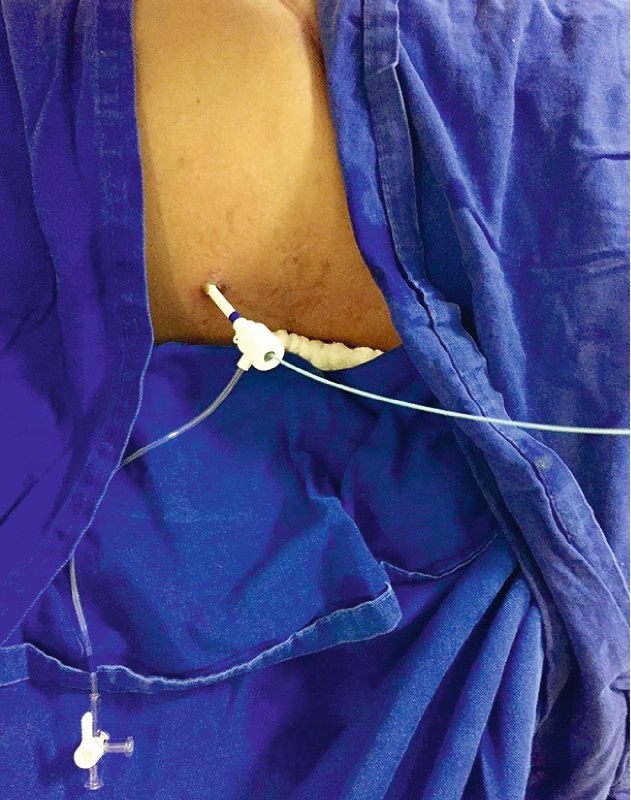
The procedure was performed under general anesthesia, and prophylactic ciprofloxacin 400 mg was given intravenously. The previously inserted biliary drain was exchanged for a 12 Fr sheath ([Fig. 3]), allowing the insertion of the Spyscope under fluoroscopic and direct visualization ([Fig. 4]). A large impacted stone causing biliary ulceration was visualized. Lithotripsy was performed using Holmium laser with power output at 10 W ([Fig. 5], [Video 1]). Stone fragments were mobilized through the hepaticojejunostomy ([Fig. 6]), and new biliary drains were inserted bilaterally. The total procedure time was 58 minutes. The patient developed postoperative cholangitis, which was treated successfully with antibiotics.


Video 1 SpyGlass (Boston Scientific, Marlborough, Massachusetts, USA) percutaneous transhepatic cholangioscopy-guided lithotripsy.

Endoscopy_UCTN_Code_TTT_1AR_2AH
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high quality video and all
contributions are freely accessible online.
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
Competing interests
None
-
References
- 1 Franzini TA, Moura RN, de Moura EG. Advances in therapeutic cholangioscopy. Gastroenterol Res Pract 2016; 2016: 5249152
- 2 Mori T, Sugiyama M, Atomi Y. Gallstone disease: management of intrahepatic stones. Best Pract Res Clin Gastroenterol 2006; 20: 1117-1137
- 3 Cannavale A, Bezzi M, Cereatti F. et al. Combined radiological-endoscopic management of difficult bile duct stones: 18-year single center experience. Ther Adv Gastroenterol 2015; 8: 340-351
- 4 Tellez-Avila FI, Duarte-Medrano G, Valdovinos-Andraca F. et al. Percutaneous laser application using the SpyGlass system in a patient with intrahepatic lithiasis, liver cirrhosis, and surgically altered anatomy. Endoscopy 2016; 48: E49-50
- 5 Bhandari S, Bathini R, Sharma A. et al. Percutaneous endoscopic management of intrahepatic stones in patients with altered biliary anatomy: a case series. Indian J Gastroenterol 2016; 35: 143-146
Corresponding author
-
References
- 1 Franzini TA, Moura RN, de Moura EG. Advances in therapeutic cholangioscopy. Gastroenterol Res Pract 2016; 2016: 5249152
- 2 Mori T, Sugiyama M, Atomi Y. Gallstone disease: management of intrahepatic stones. Best Pract Res Clin Gastroenterol 2006; 20: 1117-1137
- 3 Cannavale A, Bezzi M, Cereatti F. et al. Combined radiological-endoscopic management of difficult bile duct stones: 18-year single center experience. Ther Adv Gastroenterol 2015; 8: 340-351
- 4 Tellez-Avila FI, Duarte-Medrano G, Valdovinos-Andraca F. et al. Percutaneous laser application using the SpyGlass system in a patient with intrahepatic lithiasis, liver cirrhosis, and surgically altered anatomy. Endoscopy 2016; 48: E49-50
- 5 Bhandari S, Bathini R, Sharma A. et al. Percutaneous endoscopic management of intrahepatic stones in patients with altered biliary anatomy: a case series. Indian J Gastroenterol 2016; 35: 143-146