

Subscribe to RSS
DOI: 10.1055/s-0043-117601
Endoscopic ultrasound appearance of dead Ascaris lumbricoides in the biliary tract
Authors
Corresponding author
Publication History
Publication Date:
10 August 2017 (online)

A 2-year-old Indian girl was referred with symptoms of biliary colic and obstructive jaundice of 3 weeks’ duration. Abdominal ultrasonography revealed dilation of intrahepatic biliary radicles, a distended gallbladder, and a dilated common bile duct (CBD) of 15 mm (normal diameter up to 6 mm) containing multiple ill-defined, oval, hyperechoic shadows near the lower end ([Fig. 1]). Magnetic resonance cholangiopancreatography (MRCP) showed multiple intraluminal curvilinear, hypointense areas in the lower CBD consistent with stones or worm ([Fig. 2]). Linear endoscopic ultrasound (EUS) was performed for evaluation of the CBD filling defects visualized on abdominal ultrasound and MRCP. Linear EUS from the stomach and duodenal bulb revealed a dilated CBD with multiple hyperechoic structures without acoustic shadowing. EUS showed curvilinear, disc-shaped short-segment echogenic structures, 2 – 6 mm in size, with a central anechoic core and parallel and equidistant from each other; this was suggestive of recently broken down soft parallel fragments of roundworms ([Fig. 3], [Video 1]). The central anechoic core represented the digestive tract of Ascaris lumbricoides. Cholangiography revealed a dilated CBD with tapering at the lower end showing multiple filling defects ([Fig. 4]). After multiple balloon sweeps on endoscopic retrograde cholangiopancreatography (ERCP), creamy white structures and yellow-colored material were removed that were suggestive of recently fragmented roundworm ([Fig. 5], [Video 1]). The patient’s clinical condition improved significantly after ERCP, and repeat abdominal ultrasound after 1 week demonstrated decreased size of the CBD. The patient underwent deworming with albendazole, with the passage of multiple roundworms in stools further confirming the diagnosis of obstructive jaundice due to Ascaris.


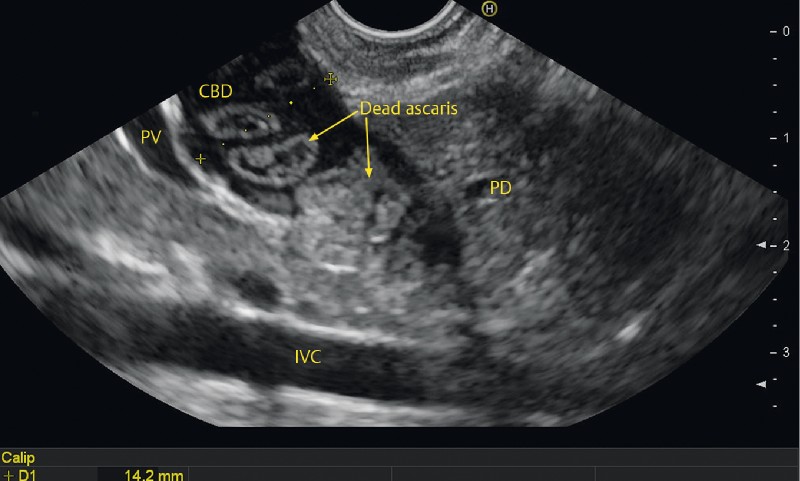
Video 1 Appearance at linear endoscopic ultrasonography (EUS) of dead Ascarislumbricoides causing obstructive jaundice in a 2-year-old girl, and removal of thefragmented roundworm at endoscopic retrograde cholangiopancreatography (ERCP). CD, cysticduct; CBD, common bile duct; IVC, inferior vena cava.


Pancreaticobiliary ascariasis is a common problem in tropical countries [1]. Dead Ascaris is a rare but an important cause of obstructive jaundice in the developing world [2]. In conclusion, we describe an unusual appearance of recently dead Ascaris lumbricoides on abdominal ultrasound, MRCP, and EUS. In endemic regions, biliary ascariasis should be considered in any child presenting with obstructive jaundice [3].
Endoscopy_UCTN_Code_CCL_1AF_2AF_3AD
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high quality video and all
contributions are freely accessible online.
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
Competing interests
All authors have no conflict of interest to disclose.
-
References
- 1 Somani P, Sharma M, Pathak A. et al. Endoscopic ultrasound imaging of pancreatic duct ascariasis. Endoscopy 2016; 48: E33-E34
- 2 Sharma M, Pathak A, Bansal S. Dead worm in common bile duct. Trop Gastroenterol 2011; 32: 343-345
- 3 Sharma M, Mookiah B, Hari RS. Double duct sign in a 3-year-old child. Gastroenterology 2014; 146: e6-e7
Corresponding author
-
References
- 1 Somani P, Sharma M, Pathak A. et al. Endoscopic ultrasound imaging of pancreatic duct ascariasis. Endoscopy 2016; 48: E33-E34
- 2 Sharma M, Pathak A, Bansal S. Dead worm in common bile duct. Trop Gastroenterol 2011; 32: 343-345
- 3 Sharma M, Mookiah B, Hari RS. Double duct sign in a 3-year-old child. Gastroenterology 2014; 146: e6-e7