

RSS-Feed abonnieren
DOI: 10.1055/s-0043-105262
Patterns of Gall Bladder Wall Thickening in Dengue Fever: A Mirror of the Severity of Disease
Autoren
Correspondence
Publikationsverlauf
received 12. Oktober 2016
revised 06. Februar 2017
accepted 27. Februar 2017
Publikationsdatum:
07. Juni 2017 (online)


Abstract
Background Dengue fever is a major public health problem with an increased incidence in recent years. Gall bladder wall thickening has been reported as one of the most common findings in dengue fever. There is a paucity of literature regarding the various patterns of gall bladder wall thickening in dengue fever and their significance in predicting the severity of disease.
Methodology and Significant Findings Out of 93 seropositive patients included in the study, 54 patients with dengue fever had gall bladder wall thickening. 4 patterns of gall bladder wall thickening are demonstrated in this study. A uniform echogenic pattern in 20 patients, striated or tram track pattern in 11 patients, an asymmetric pattern in 2 patients and a honeycombing pattern in 21 patients. The range of patterns of wall thickening included normal wall thickening or uniform echogenic wall thickening in DF without warning signs, a striated or tram track pattern, and a honeycomb pattern in severe DF. Serial ultrasound done on consecutive alternate days revealed a change in the pattern of gall bladder wall thickening according to the severity of disease.
Conclusion The present study revealed 4 distinct patterns of gall bladder wall thickening. The uniform echogenic pattern was found to be more prevalent in dengue fever without warning signs, while the honeycomb pattern was found to be more prevalent in severe dengue fever. A change in the pattern of gall bladder wall thickening on subsequent serial ultrasound can predict the severity of the disease.
Introduction
Dengue fever (DF) is a major public health problem with an increased incidence in recent years [1]. DF epidemics in recent years have shown varied clinical presentations thus delaying diagnosis and treatment [2]. Gall bladder wall thickening (GBWT) has been reported as one of the common findings in DF. A few recent studies have reported that ultrasound plays an important role as a prognostic indicator in assessing patients at risk for progressing to the critical phase by measuring GBWT [3] [4] [5]. Some authors have described a few patterns of GBWT. However, no study has been conducted regarding the clinical significance of these patterns of GBWT and the severity of DF [6] [7]. There is a paucity of literature regarding the various patterns of GBWT in DF and their significance in predicting the severity of disease.
Aims and objectives
The primary aim of this study was to examine patterns of GBWT in DF.
The secondary aim was to study the clinical significance of patterns of GBWT in predicting the severity and prognosis of DF.
Materials and Methods
A total of 160 patients suspected of having DF were referred from July 2015 to December of 2015 to the radiology department for ultrasound. 93 of these cases (58.12%) were serologically confirmed cases of DF and were included in the study.
The clinical manifestations included fever, frontal headache, retroocular pain, muscle and joint pains, nausea, vomiting, rash, leukopenia, and thrombocytopenia.
The diagnosis of DF was confirmed by NS1 antigen test or Dengue IgM or IgG antibody test.
Abdominal ultrasound was performed on a GE LOGIQ P6 unit, equipped with a 4C wide bandwidth (1.5 to 4.6 MHz) convex probe and 11L wide bandwidth (4 to 12 MHz) linear probe. The linear probe was used for pediatric patients. The abdominal ultrasound was done in all cases after 4 h of fasting for better visualization of the gall bladder (GB). A single radiologist performed the ultrasound examinations and the serial ultrasound examinations were performed every consecutive alternate day. Monitoring lasted until clinical improvement of the patients.
A thickened GB wall was defined as being ≥3 mm and was measured by placing calipers between the two layers of anterior wall. GBWT was measured and the pattern of GBWT was assessed. The pattern of GBWT was correlated with the severity of disease. The severity of disease (DF without warning sign, DF with warning sign and severe DF) was assessed with the help of the “suggested dengue case classifications and levels of severity” proposed by WHO in 2009 [9].
Ethics statement
The study was approved by institutional ethics committee and scientific research committee.
Informed consent
All adult subjects and the parent/guardian of the pediatric subjects provided informed written consent for the study.
Statistical analysis
Type of study: Prospective observational study
Statistical methods
Statistical testing was conducted with the Statistical Package for the Social Sciences (SPSS) version 17.0. Continuous variables are presented as mean±SD or median if the data is unevenly distributed. Categorical variables are expressed as frequencies and percentages. The comparison of normally distributed continuous variables between the groups was performed using Student’s t-test. Nominal categorical data between the groups was compared using Chi-square test or Fisher’s exact test, as appropriate. For all statistical tests, a “p” value less than 0.05 was taken to indicate a significant difference.
Observations and Results
A total of 160 suspected cases of DF were referred to the radiology department for ultrasound examination. 93 patients (60 (64.5%) males and 33 (35.5%) females) with positive serology were included in this study. The mean±standard deviation of age was 32.28±15.0 years. 19 (20.4%) patients were pediatric patients.
Out of 93 seropositive patients, 38 (40.8%) patients were classified as DF without warning signs, 26 (27.9%) patients as DF with warning signs and 29 (31.1%) as patients with severe DF. A thickness of less than 3 mm was considered a normal gall bladder wall. GBWT was present in 54 cases of dengue fever on the day of presentation. [Fig. 1] shows the percentage of cases with GBWT in DF according to the classification of DF.

The mean GB wall thickness was 3.32 mm in DF without warning signs, 4.95 mm in DF with warning signs and 8.80 mm in severe DF. There is a significant correlation between GBWT and the severity of the disease [based on observed means and the error term is mean square (error) 2094.911. The mean difference is significant at p<0.05].
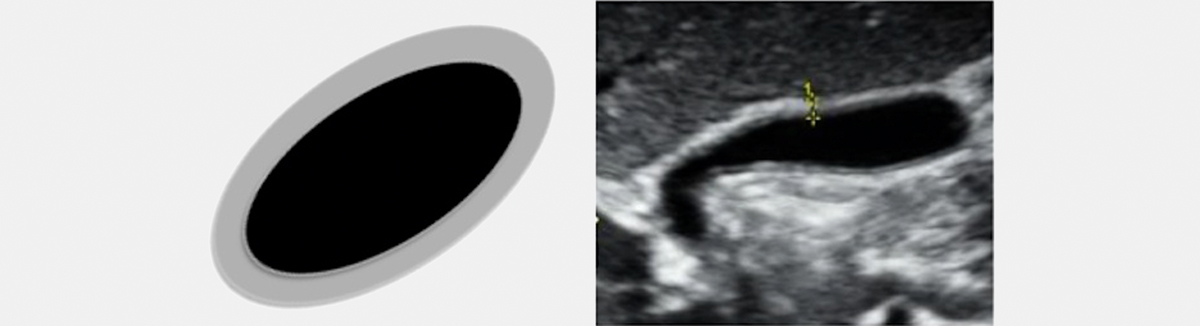
The present study showed four patterns of GBWT. A uniform echogenic pattern uniform echogenic layer ([Fig. 2]), striated or tram track pattern – multiple linear hypoechoic layers separated by parallel echogenic layers ([Fig. 3]) or a central hypoechoic zone separated by two echogenic layers ([Fig. 4]), an asymmetric pattern – an asymmetric echogenic tissue projecting into the gall bladder lumen ([Fig. 5]) and a honeycombing pattern – multiple hypoechoic layers separated by multiple echogenic layers ([Fig. 6]). A uniform echogenic pattern were present in 20 (21.5%) patients, striated or tram track pattern in 11 (11.8) patients, asymmetric pattern in 2 (2.1%) patients and honeycomb pattern in 21 (22.5%) patients.




The occurrence of a normal gall bladder wall and uniform echogenic pattern in DF without warning signs and honeycomb pattern in severe DF was statistically significant (p<0.05).
[Fig. 7] shows the pattern of GBWT in DF according to the severity. 95.24% of cases of honeycomb pattern were found in severe DF and 4.76% in DF with warning signs, while it was not found in DF without warning signs. 50% of cases of asymmetric pattern were found in severe DF and 50% in DF with warning signs while it was not found in DF without warning signs. 36.36% of cases of striated/tram track pattern were found in severe DF and 45.45% in DF with warning signs, while 18.18% of cases were found in DF without warning signs. 69.23% of cases of uniform echogenic pattern were found in DF without warning signs and 28.20% in DF with warning signs, while only 2.5% of cases were found in severe DF.

Discussion
Dengue fever (DF) is an acute mosquito-transmitted, flavivirus infection caused by 1 of 4 virus serotypes (DEN-1, DEN-2, DEN-3, and DEN-4) [1]. DF is endemic in Southeast Asia. In recent years, many outbreaks have erupted in this part of world with significant associated mortality [8].
DF is an acute febrile illness. Its manifestations are from mild febrile illness with associated symptoms of frontal headache, retroocular pain, muscle and joint pain, nausea, vomiting, and rash to severe dengue fever with hemorrhagic manifestation and shock syndrome [2] [9]. Common laboratory abnormalities include neutropenia, lymphocytosis, increased liver enzymes and thrombocytopenia.
Clinical manifestations and laboratory results suggest the possibility of DF in an endemic area. Serologic virus detection or antiviral antibody detection can confirm the diagnosis of DF but the results are often obtained late. This means there is a need for additional and readily available tools for the diagnosis of dengue fever. Ultrasound has been used in the evaluation of dengue fever [8] [9].
GBWT has been reported as one of the most common ultrasound findings in DF. In the present study we observed four distinct patterns of GBWT [10]. A uniform echogenic pattern in 20 patients, striated/tram track pattern in 11 patients, asymmetric pattern in 2 patients and honeycomb pattern in 21 patients. In 2010, Oliveira GA et al. reported transient reticular gall bladder wall thickening in severe DF due to plasma leakage in the wall and the author identified four distinct gall bladder wall thickening patterns: 1- A striated pattern of multiple hypoechoic layers separated by echogenic zones; 2- Asymmetric pattern with echogenic tissue projecting into the gall bladder lumen; 3- A central hypoechogenic zone separated by two echogenic layers; and 4- A uniform echogenic pattern [6]. Sachar et al. demonstrated that a “honeycomb” pattern in the thickened gall bladder wall on ultrasound specifically suggests the diagnosis of DHF [7].
In the present study, the occurrence of a honeycomb pattern is more prevalent in severe dengue fever than in dengue fever with warning signs, while this pattern was not found in the patients with dengue fever without warning signs.
The range of patterns of wall thickening included normal wall thickening or uniform echogenic wall thickening in DF without warning signs, a striated or tram track pattern, and a honeycomb pattern in severe DF. Clinically recovering patients showed a change from a honeycomb pattern in severe DF to a normal wall thickness or uniform echogenic wall thickening on subsequent ultrasound. The GBWT decreased from day four to day seven of fever. The pattern of GBWT was honeycomb on day 4 (a) & 5 (b) of fever and diffuse echogenic on day 7 of fever (c). The ultrasound and clinical findings were consistent with the recovery of the patient from severe DF on the 4th day of fever to DF without warning signs on the 7th day of fever ([Fig. 8]).

In contrast, clinically deteriorating patients showed a change from uniform echogenic wall thickening in DF without warning signs in the earlier days of fever to a honeycomb pattern in severe DF in the later days of fever. The GBWT increased from day two to day five of fever. The gall bladder wall was normal on the 2nd day of fever (A), a central hypoechoic zone separated by two echogenic layers was seen on the 3rd day fever (B) and finally honeycombing was seen on the 5th day of fever (C). The findings were consistent with the clinical deterioration of patients with DF without warning signs on the 2nd day of fever to DF with warning signs on the 3rd day of fever and finally severe DF on the 5th day of fever ([Fig. 9]).

Thus, the pattern of GBWT can also be used for the prediction of the severity of disease and the recovery or deterioration of the patient.
Conclusion
In the present study we observed four distinct patterns of GBWT. The normal gall bladder wall and the uniform echogenic pattern were found to be more prevalent in DF without warning signs and DF with warning signs than in severe dengue fever, while the honeycomb pattern was found to be more prevalent in severe dengue fever.
Moreover, these patterns were found to be a spectrum of gall bladder wall thickening from normal wall thickening or uniform echogenic pattern in DF without warning signs to a honeycomb pattern in severe dengue fever. Thus, recognizing the pattern of GBWT can help in the recognition of the severity of disease, and a change in the pattern of gall bladder wall thickening on subsequent ultrasound from a honeycomb pattern to a uniform echogenic pattern/normal wall thickening or from a normal/uniform echogenic pattern to a honeycomb pattern should suggest the clinical recovery or deterioration of the disease, respectively.
Summary
Dengue fever is one of the most common viral infections with variable clinical presentations and degrees of severity. Gall bladder wall thickening is one of the most common findings in dengue fever. The authors demonstrated four distinct patterns of gall bladder wall thickening in dengue fever patients. The uniform echogenic layer was found to be more common in dengue fever without warning sign, while the honeycomb pattern was more common in severe dengue fever.
The research concluded that the patterns of gall bladder wall thickening can be used to diagnose the severity of disease and, when combined with the pattern type in serial ultrasound, may predict the prognosis of the disease.
Limitations
Patterns of GBWT cannot be studied in patients with a history of cholecystectomy or gall bladder diseases.
Conflict of interest
The authors declare that they have no conflict of interest.
-
References
- 1 Hadinegoro S. The revised WHO dengue case classification: Does the system need to be modified?. Pediatrics and international child health 2012; 32: 33-38
- 2 World Health Organization . Working to overcome the global impact of neglected tropical diseases. First WHO report on neglected tropical diseases. Geneva, Switzerland: WHO; 2010
- 3 Pramuljo H, Harun S, Srivastava N, Sharma S, Berry M, Pandey R. Ultrasound findings in dengue haemorrhage fiver. Pediatr Radiol J 1991; 21: 100-102
- 4 Setiawan M, Samsi T, Pool T, Wulur H, Sugianto D, Pool T. Gallbladder wall thickening in dengue hemorrhagic fever: An ultrasonographic study. J Clin Ultrasound. 1995; 23: 357-362
- 5 Setiawan MW, Samsi TK, Wulur H, Sugianto D, Pool T. et al. Dengue haemorrhagic fever: Ultrasound as an aid to predict the severity of the disease. Pediatr Radiol. 1998; 28: 1-4
- 6 Oliveira G, Machado R, Horvat J, Gomes L, Guerra L, Vandesteen L. et al. Transient reticular gallbladder wall thickening in severe dengue fever: A reliable sign of plasma leakage. Pediatr Radiol 2010; 40: 720-724
- 7 Sachar S, Goyal S, Sachar S. Role of ultrasound (“Honeycomb sign”) in early detection of dengue hemorrhagic fever. Arch Clin Exp Surg 2013; 2: 38-42 Available at http://www.ejmanager.com/mnstemps/64/64-1340217637.pdf?t=1483123855.pdf
- 8 Gubler D. Dengue and dengue hemorrhagic fever. Clin Microbiol Rev 1998; 11: 480-496
- 9 WHO. 2009; Dengue: Guidelines for diagnosis, treatment, prevention and control. Available at: http://whqlibdoc.who.int/publications/2009/9789241547871_eng.pdf
- 10 Colbert J, Gordon A, Roxelin R, Silva S, Silva J, Rocha C. et al. Ultrasound measurement of gallbladder wall thickening as a diagnostic test and prognostic indicator for severe dengue in pediatric patients. Pediatr Infect Dis J 2007; 26: 850-852
Correspondence
-
References
- 1 Hadinegoro S. The revised WHO dengue case classification: Does the system need to be modified?. Pediatrics and international child health 2012; 32: 33-38
- 2 World Health Organization . Working to overcome the global impact of neglected tropical diseases. First WHO report on neglected tropical diseases. Geneva, Switzerland: WHO; 2010
- 3 Pramuljo H, Harun S, Srivastava N, Sharma S, Berry M, Pandey R. Ultrasound findings in dengue haemorrhage fiver. Pediatr Radiol J 1991; 21: 100-102
- 4 Setiawan M, Samsi T, Pool T, Wulur H, Sugianto D, Pool T. Gallbladder wall thickening in dengue hemorrhagic fever: An ultrasonographic study. J Clin Ultrasound. 1995; 23: 357-362
- 5 Setiawan MW, Samsi TK, Wulur H, Sugianto D, Pool T. et al. Dengue haemorrhagic fever: Ultrasound as an aid to predict the severity of the disease. Pediatr Radiol. 1998; 28: 1-4
- 6 Oliveira G, Machado R, Horvat J, Gomes L, Guerra L, Vandesteen L. et al. Transient reticular gallbladder wall thickening in severe dengue fever: A reliable sign of plasma leakage. Pediatr Radiol 2010; 40: 720-724
- 7 Sachar S, Goyal S, Sachar S. Role of ultrasound (“Honeycomb sign”) in early detection of dengue hemorrhagic fever. Arch Clin Exp Surg 2013; 2: 38-42 Available at http://www.ejmanager.com/mnstemps/64/64-1340217637.pdf?t=1483123855.pdf
- 8 Gubler D. Dengue and dengue hemorrhagic fever. Clin Microbiol Rev 1998; 11: 480-496
- 9 WHO. 2009; Dengue: Guidelines for diagnosis, treatment, prevention and control. Available at: http://whqlibdoc.who.int/publications/2009/9789241547871_eng.pdf
- 10 Colbert J, Gordon A, Roxelin R, Silva S, Silva J, Rocha C. et al. Ultrasound measurement of gallbladder wall thickening as a diagnostic test and prognostic indicator for severe dengue in pediatric patients. Pediatr Infect Dis J 2007; 26: 850-852