
RSS-Feed abonnieren
DOI: 10.1055/s-0042-1759580
Dementia Prevention in Clinical Practice
- Abstract
- Alzheimer's Disease Overview
- Approach to Risk Stratification
- Risk Reduction and Prevention Overview
- Risk Factors and Interventions
- Future Directions and Conclusion
- References
Abstract
Over 55 million people globally are living with dementia and, by 2050, this number is projected to increase to 131 million. This poses immeasurable challenges for patients and their families and a significant threat to domestic and global economies. Given this public health crisis and disappointing results from disease-modifying trials, there has been a recent shift in focus toward primary and secondary prevention strategies. Approximately 40% of Alzheimer's disease (AD) cases, which is the most common form of dementia, may be prevented or at least delayed. Success of risk reduction studies through addressing modifiable risk factors, in addition to the failure of most drug trials, lends support for personalized multidomain interventions rather than a “one-size-fits-all” approach. Evolving evidence supports early intervention in at-risk patients using individualized interventions directed at modifiable risk factors. Comprehensive risk stratification can be informed by emerging principals of precision medicine, and include expanded clinical and family history, anthropometric measurements, blood biomarkers, neurocognitive evaluation, and genetic information. Risk stratification is key in differentiating subtypes of dementia and identifies targetable areas for intervention. This article reviews a clinical approach toward dementia risk stratification and evidence-based prevention strategies, with a primary focus on AD.
#
Dementia is a neurodegenerative disease with a significant impact on the lives of patients affected, their caregivers, and society. Dementia is an umbrella term for a range of conditions characterized by progressive cognitive impairment and behavioral changes that interfere with daily functioning. Neurodegenerative dementias such as Alzheimer's disease (AD) are most common, followed by microangiopathies such as vascular dementia (VaD) and Lewy body dementia (LBD), with mixed pathology often seen.
As of 2021, more than 55 million people were living with dementia, but with an aging population, dementia is an increasingly prevalent threat to population health with a projected 131 million people affected by the disease by 2050.[1] [2] [3] This will continue to pose a significant threat to domestic and global economies, with disease-related costs estimated at $200 billion per year in the United States (expected to rise to two trillion by 2030) and $600 billion worldwide.[4] [5] [6] Given this emerging public health crisis, the search for effective treatments has increased with urgency, as current treatment approaches are “symptomatic” without altering the underlying pathological course of the disease, and approved therapies have shown limited efficacy with considerable side effects.[7] [8] [9] [10]
The pivot toward primary and secondary prevention strategies—before irreversible neuronal loss and clinical dementia—has been motivated by discouraging results from pharmaceutical trials in AD in addition to growing evidence that modifiable risk factors provide an opportunity for early intervention. According to the Lancet Commission 2020 Report, these modifiable risk factors account for approximately 40% of dementia cases worldwide.[11] Findings from projection models estimate that delaying AD by just 1 year would reduce the total worldwide number of cases in people older than 60 years in 2050 by 11%, and others have shown that medical advances aimed at delaying disease onset for 5 years or longer would result in a 41% lower prevalence and 40% lower cost of AD in 2050.[12] [13] Therefore, investing resources and efforts in prevention may be a more fruitful and actionable path in clinical practice today toward decreasing dementia incidence and socioeconomic impact.[14]
In this article, we review the current clinical approach to dementia risk stratification and early detection as well as evidence-based prevention strategies, with a primary focus on AD, the most common neurodegenerative dementia.
Alzheimer's Disease Overview
In 2021, an estimated 6.2 million Americans were living with AD, and that number is projected to increase to 13.8 million by 2050.[15] While the cause of AD is not fully understood, a combination of genetic (nonmodifiable) and environmental/lifestyle (modifiable) factors likely contribute (as well as a host of other comorbid diseases that have their own unique modifiable and nonmodifiable risk factors). AD is associated with abnormal deposition of amyloid-beta (Aβ) proteins accumulating in amyloid plaques, and hyperphosphorylated tau (p-tau) proteins resulting in neurofibrillary tangles and, hence, is referred to as a tauopathy. AD preferentially affects the hippocampus which is responsible for the first symptoms of amnestic cognitive decline.
AD is a heterogeneous disease and may present and progress differently depending on the person and individual factors leading to the disease pathology. To this end, various models of subtyping AD based on a criterion such as disease phenotypes, pathological findings, and other biomarkers have been proposed.[16] [17] [18] [19] While these are important steps toward characterizing early individual disease variation, using a single biomarker to determine disease risk and clinical trajectory may not provide a complete picture of the potential factors contributing to AD pathology. Furthermore, the coexistence of multiple pathologies (i.e., microangiopathic changes, alpha-synuclein deposits, and tau aggregates) on an individual level suggests a strong overlap between these neurodegenerative processes. As such, we advocate for a practical approach to AD and dementia risk stratification using individual clinical attributes and biomarkers. This also more optimally allows for personalized care based on modifiable risk factors and specific underlying disease pathology.
#
Approach to Risk Stratification
When applying dementia prevention methods in cognitively normal patients, proper risk stratification is imperative to allow for pathology-specific interventions. [Table 1] summarizes the clinical domains considered in dementia risk stratification. Often, family history of AD or dementia is the primary motivator for patients to seek risk reduction management.[20] [21] As AD is responsible for 60 to 80% of all dementia cases, and significant overlap between clinical presentation exists, other less common forms of dementia are often misdiagnosed as AD.[22] [23] [24] It is necessary to diligently investigate any family history of diagnosed AD, other dementias, or undiagnosed symptoms of cognitive impairment—especially in first-degree relatives—along with the age of onset and clinical presentation for any affected relatives. For example, dementia onset at age <65 years (yet more likely with onset in 40s–50s) in multiple relatives may suggest involvement of highly penetrant autosomal dominant genes. These include amyloid precursor protein (APP), presenilin 1 (PSEN1), and presenilin 2 (PSEN2) in the appropriate clinical context and may warrant genetic testing for these variants after genetic counseling is performed. A family history prominent for psychiatric disease, anterolateral sclerosis (ALS), or autism spectrum disorder (ASD) may suggest frontotemporal dementia (FTD) is more likely.[25]
|
Domain |
Supports underlying, typical LOAD pathology |
Supports underlying, typical vascular dementia pathology |
Supports underlying, typical EOAD pathology |
Supports underlying synucleinopathy (PD, DLB) |
Supports underlying FTD pathology |
Supports underlying atypical neurodegenerative disease (atypical AD, CBS, PSP) |
|---|---|---|---|---|---|---|
|
Age |
≥65[44] |
≥65[310] |
<65[311] |
Variable but typically ≥60[312] |
>40[313] |
≥60[314] |
|
Sex |
Male > female[315] |
Female > male[311] |
Male > female[313] |
|||
|
Cognition |
Amnestic Impairments in episodic memory and semantic function[320] [321] |
Impairments on attentional/executive function, semantic memory, and visuospatial skills[320] |
Amnestic, frontal/executive function and visual memory impairment |
Non-amnestic (bradyphrenia, poor learning, logopenia) Impairments in visuospatial function and letter fluency[312] |
Non-amnestic (language, behavioral, visual, or dysexecutive)[324] |
Non-amnestic (language, behavioral, visual, or dysexecutive)[325] |
|
Medical history |
Vascular and metabolic conditions (e.g., heart disease, stroke, high blood pressure, diabetes, obesity)[209] [225] [226] [227] Developmental and learning disabilities, head injury[319] |
Vascular and metabolic conditions (e.g., heart disease, stroke, high blood pressure, diabetes, obesity)[310] |
Cancers, especially melanoma; seborrheic dermatitis; constipation; apathy; visual changes and vertigo; changes to handwriting; exposures to pesticides/solvents; well water[312] |
|||
|
Family history |
Amnestic-type dementia Developmental and learning disabilities[319] |
Early-onset dementia in multiple family members in autosomal dominant pattern[115] |
Parkinsonian disorders Psychiatric disorders especially suicide |
ALS, ASD, substance use disorders, and other psychiatric disorders[324] |
Learning disability or atypical dementia[327] non-amnestic dementia |
|
|
Sleep |
Sleep apnea |
Sleep disturbances[330] |
REM behavior restless leg syndrome Periodic limb movements of sleep[312] |
Somnolence, narcolepsy-like attacks, insomnia[331] |
Irregular sleep/wake behavior[332] |
|
|
Mood |
Late-life depression/anxiety Irritability Apathy[245] |
Early-life depression/anxiety obsessive compulsive disorder Visual hallucinations[312] |
Emotional blunting, mood changes, disinhibition[335] |
Apathy Disinhibition Loss of empathy |
||
|
Motor |
Slowed walking (without parkinsonism)[336] |
Parkinsonian-like gait disorder, dysarthria, and autonomic dysfunction[310] |
Aberrant motor behavior[334] |
Parkinsonism (bradykinesia, rigidity, tremor, stooped posture, gait changes, imbalance/falls) or autonomic dysfunction (constipation, urinary frequency, orthostatic hypotension, impotence)[312] |
Parkinsonism, dysphagia[324] |
Muscle twitching Muscle atrophy Myoclonus Dystonia Gaze paralysis Difficulty walking Eye movement difficulty[325] |
|
Genetic |
APOE4, TOMM40, APOC1, mitochondrial haplotype |
APOE, SNCA, LRRK2, VPS35, PRKN, PINK1, DJ-1, GBA[331] |
C9orf72, GRN, MAPT [339] |
MAPT, C9orf72 [340] |
Abbreviations: AD, Alzheimer's disease; ALS, amyotrophic lateral sclerosis; APOC1, apolipoprotein C1; APOE, apolipoprotein E-4; APP, amyloid precursor protein, PSEN1, presenilin 1; ASD, autism spectrum disorder; C9orf72, chromosome 9 open reading frame 72; CBS, corticobasal syndrome; EOAD, early-onset Alzheimer's disease; FTD, frontotemporal dementia; GRN, progranulin; LOAD, late-onset Alzheimer's disease; LRRK2, leucine-rich repeat kinase 2; MAPT, microtubule-associated protein tau; PD, Parkinson's disease, DLB, dementia with Lewy bodies; PSEN2, presenilin 2; PSP, progressive supranuclear palsy; REM, rapid eye movement; SNCA, alpha synuclein; TOMM40, translocase of outer mitochondrial membrane 40; VPS35, vacuolar protein sorting-35, PINK1, PTEN-induced kinase-1.
A dementia-prevention–focused clinical history including age, biological sex, medical history, and factors related to early life brain development (academic performance, class ranking, standardized test scores, and career achievement) should be performed. This expanded history should also include assessment of past and current lifestyle habits (exercise, diet, sleep, stress management) that would be targetable risk factors. A detailed review of systems for symptoms that may indicate alternate pathology should be included.[21] For example, the presence of REM sleep behavior disorder is strongly associated with the development of Parkinson's disease (PD) or other synucleinopathy (e.g., LBD).[26] The identification of conditions such as hypertension, hearing impairment, periodontal disease, obesity, depression, diabetes, alcoholism, and traumatic brain injury is of the utmost importance, as these conditions are some of the strongest risk factors for developing AD.[11] Physical and neurological exam should follow. Physical exam findings such as bradykinesia, myoclonus, orthostatic hypotension, and loss of the optokinetic reflex may suggest atypical AD or alpha-synuclein pathology. Although it is nonspecific, olfactory impairment is a common and early sign of neurodegenerative diseases corresponding to emerging pathologic processes in the olfactory system. While patients may report hyposmia or anosmia, objective testing is necessary to accurately determine olfactory function.[27]
Vital signs and anthropometric measurements are also essential. Collecting objective measurements of body composition including lean dry mass, skeletal muscle mass, and body fat percentage using tools such as bioimpedance devices or other more rigorous means (e.g., a dual-energy X-ray absorptiometry [DEXA] scan) should be performed in a standardized manner (e.g., fasting, same device, same time of the day) for more accurate longitudinal comparisons. Measurements such as body mass index (BMI) are imprecise and not as informative, whereas waist-to-hip circumference—which is associated with hippocampal volume—may be a better proxy.[28]
Additionally, blood biomarkers are an essential component of the risk stratification process and can aid in identifying modifiable risk factors. Since hypercholesterolemia and hypertriglyceridemia are associated with cognitive decline, advanced lipid and inflammatory panels more routinely performed by the preventive cardiology field should be considered.[29] Although clinical guidelines in the United States advise on the use of low-density lipoprotein cholesterol (LDL-C) and non–high-density lipoprotein cholesterol (HDL-C) to guide cholesterol management decisions, the 2019 European Society of Cardiology/European Atherosclerosis Society Guidelines concluded that apolipoprotein B (apoB) is a more accurate measure of risk, especially in younger patients. Obtaining advanced lipid panels to better guide risk stratification and to monitor adequacy of lipid lowering therapy has been successfully deployed in AD prevention clinical practice over the last decade.[20] [21] [30] [31] In apolipoprotein E (ApoE4) carriers, Apo-A1 (a component of HDL cholesterol) is a marker for increased AD risk, whereas N-terminal probrain natriuretic peptide (NT-proBNP) is a plasma protein associated with VaD.[32] [33] Insulin resistance is associated with poor cognitive function and can promote neuroinflammation and amyloid deposition.[34] [35] As such, metabolic metrics (e.g., glycosylated hemoglobin [HgbA1C%], fasting insulin, fasting glucose, and HOMA-IR) should be evaluated. Nutritional measures such as omega-3/6 fatty acids, vitamin levels (B12 and D), and homocysteine should be considered as they may guide the need for dietary modification or supplementation directly related to brain health outcomes.[21]
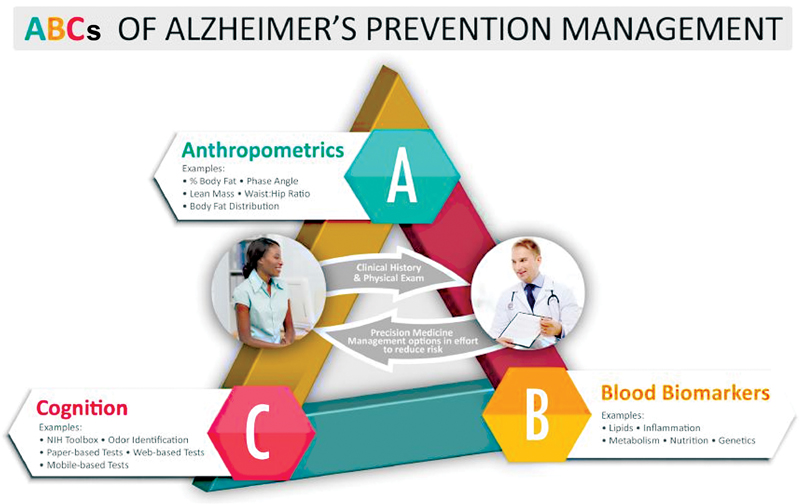
Neurocognitive evaluation using both computerized and more traditional individual tests (as well as preclinical focused batteries) to quantify global cognitive status, executive function, processing speed, language, verbal knowledge, and learning and memory may demonstrate early presymptomatic changes.[36] [37] [38] Although AD typically presents with episodic and associative memory dysfunction, language and executive dysfunction are seen in early FTD and visuospatial deficits are common in early LBD.[24] [39] [40] See [Fig. 1] for a comprehensive model of AD prevention management.
Though genetic information must be interpreted in the context of family and complete clinical history, it may be valuable for risk assessment in the appropriate clinical context and with adequate patient counseling. The ApoE gene—whose E4 allele is the most significant and well-studied genetic risk factor for AD—affects lipid homeostasis, especially in the central nervous system (CNS), and impedes Aβ clearance at the blood–brain barrier (BBB).[41] ApoE4 carriers account for an estimated 40 to 65% of AD cases despite making up only around 20% of the general population.[42] While estimates vary among different studies, the ApoE4 genotype incurs a 2- to 3-fold increased risk of AD in heterozygotes and an 8- to 12-fold increased risk in homozygotes as compared to ApoE3 homozygotes.[15] The ApoE2 genotype—present in only 5% of the population—is protective with carriers being two times less likely to develop AD.[43] [44]
ApoE is not only an important mediator of AD risk, but it also may account for specific disease heterogeneity.[45] For example, ApoE4 carriers may have greater memory impairment due to more tau deposition and brain atrophy in the medial temporal lobe, whereas AD patients without an ApoE4 variant demonstrate greater executive, visuospatial, and language dysfunction due to more tau accumulation and atrophy in the frontal and parietal lobes.[45]
However, being a carrier of ApoE4 does not ensure that an individual will develop the disease—its influence is variable across age, race, ethnicity, and biological sex, and can change once modifiable risk factors are targeted.[21] It is further complicated by specific gene–gene interactions including other somatic and mitochondrial genetic variances/haplogroups that may alter the impact of ApoE by neutralizing, enabling, or synergizing its expression.[46] [47] [48] For example, KL-VS heterozygosity (KL-VShet)—having one copy of the Klotho gene—incurs a protective effect on ApoE4 carriers and has been linked higher cognitive performance in adulthood.[49] [50] [51] [52] Recent findings showed that a substantial portion of the approximately 15% of Americans carrying the ApoE4 allele are protected by their KL-VShet status.[49] [50] Given the complex genetic architecture of AD, a risk stratification methodology needs to be developed accounting for polygenic risk scores as well as additional clinical and genetic components that may directly modify ApoE expression or independently modify overall AD risk.
Until recently, invasive cerebrospinal fluid (CSF) biomarkers (Aβ1-42, T-tau, and P-tau181) and costly imaging studies (amyloid-PET, tau-PET, fMRI, etc.) were the only clinically available methods to diagnose preclinical AD. Advancements in blood-based biomarkers have opened the door to a new era of early detection and intervention.[53] PrecivityAD, a mass spectrometry-based plasma Aβ42/Aβ40 assay, is not only highly concordant with CSF biomarkers and amyloid PET scan in cognitively normal individuals, but it may be more sensitive in detecting preclinical AD. “False positives” were highly likely to convert to positive by CSF biomarkers (13-fold higher risk over an average follow-up period of 7.3 years) or amyloid PET (9-fold higher risk over an average follow-up period of 6.2 years), suggesting their superiority in detecting preclinical AD.
#
Risk Reduction and Prevention Overview
The pathophysiological changes of AD and other neurodegenerative disorders begin decades before clinical apparent symptoms, providing the opportunity for early intervention. Observational studies have identified several modifiable risk factors for AD that, if addressed, may prevent—or at minimum delay—a significant portion of AD cases.[11] A 2020 report by the Lancet commission added three modifiable risk factors—excessive alcohol consumption, traumatic brain injury, and air pollution—to the nine previously identified in 2017—less education, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, and low social interaction—which together account for approximately 40% of global dementia cases.[11] Other prospective studies have evaluated the effectiveness of AD risk reduction via addressing modifiable risk factors. The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) trial, a large 2-year randomized clinical trial, demonstrated a decrease in AD risk at 24 months using multidomain lifestyle interventions including dietary and exercise recommendations, social activity, cognitive training, and metabolic/vascular monitoring when compared to general medical advice. The Exercise and Nutritional Interventions for Cognitive and Cardiovascular Health Enhancement (ENLIGHTEN) trial, which focused on aerobic exercise and dietary approaches to stop hypertension (DASH) diet, saw the greatest improvement in executive function in participants who received the combined intervention of aerobic exercise and the DASH diet rather than aerobic exercise alone, DASH alone, or general health education.[54] The Comparative Effectiveness Dementia and Alzheimer's Registry (CEDAR) study demonstrated that an individualized multidomain risk reduction approach improves cognitive function related to both AD pathology and changes more so characterized by cognitive aging, as well as reduced both AD and cardiovascular risk scores in both high- and low-compliance primary prevention and preclinical AD patients and high-compliance patients with MCI due to AD at 18 months.[55]
However, multidomain risk reduction interventions may be less effective in older patients and those with more advanced pathology. The nurse-led Prevention of Vascular Dementia by Intensive Care (PreDIVA) trial did not demonstrate a reduction in incident dementia with a multidomain cardiovascular risk factor reduction intervention in individuals aged 70 to 78 years.[56] The authors concluded that the intensity of care delivered might have been insufficient to induce the necessary effects on lifestyle change. The Multidomain Alzheimer Preventive Trial (MAPT) failed to demonstrate benefit on cognitive decline at 3 years with nutritional counseling, physical exercise, and cognitive training, omega-3 fatty acid supplementation, or both, though a post hoc analysis performed on participants with positive amyloid scans showed a significant benefit in favor of the interventions.[57] Defining appropriate recommendations based on the totality of evidence is imperative and may be in part responsible for these conflicting results. The French National Nutrition and Health Program (PNNS) guidelines were used to guide dietary recommendations instead of individualizing interventions based on more recent evidence (e.g., Mediterranean–DASH Intervention for Neurocognitive Delay [MIND] diet). The necessity of individually tailored recommendations may also be supported by the Lifestyle Interventions and Independence for Elders (LIFE) study, which failed to demonstrate positive cognitive benefit from moderate-intensity physical activity interventions (walking, resistance training, flexibility).[58] It is thought that the lack of benefit in this 2-year study stems from a higher mean age of participants and interventions that were not individually tailored.
Past studies suggest that personalized multidomain interventions may offer the greatest opportunity to decrease the incidence of, delay, or prevent AD and other dementias.[59] Individualizing risk reduction interventions requires accurate risk stratification based on both nonmodifiable and modifiable risk factors. Examples of risk factor and intervention considerations are described in [Table 3].
|
Domains |
Considerations |
Benefits for ApoE4+ carriers |
|---|---|---|
|
Dietary patterns[133] |
||
|
Low-glycemic index/Low-carbohydrate diets |
Regular dietary pattern |
• Protects against insulin resistance • Lessens risk of Aβ degradation impairment by insulin • Reduces GSK3β-mediated hyperphosphorylation of tau • Ameliorates reduced cerebral blood flow • Protects against AGE formation and ApoE4 glycation, with consequences on cerebral lipid metabolism • Overall associated with reduced AD risk |
|
Organic food |
Regular substitution of non-organic foods |
• Reduces body burden of toxins • Reduced exposure to certain pesticides that tend to effect ApoE4 carriers[341] |
|
Extra virgin olive oil |
1-2 Tbsp/day |
• Anti-amyloid and anti-tau properties induced through phenolic compounds, oleocanthal and hydroxytyrosol • Increases levels of LRP1 • Inhibits CypA-NFκB-MMP9 • Increases ABCA1 |
|
Fatty fish |
2–4 servings/week |
• Inhibits NLRP3 formation • Inhibits CypA-NFκB-MMP9 • Improves amyloid and tau pathologies in animal models • Overall consumption associated with reduced AD risk |
|
Alcohol |
Limit alcohol consumption |
• Reduced consumption overall associated with reduced AD risk |
|
Biomarkers [133] |
||
|
Low RBC omega-3 (EPA/DHA)/omega-3 index |
Nutritional counseling + consider supplementation |
• Possible improvements in memory reaction time in males • Improved attentional measures of cognition • Improved composite cognition scores |
|
Low serum vitamin D (<30 nmol/L) |
Consider supplementation and increase exposure to natural sunlight |
• Possible improvement in cognitive function |
|
Insulin resistance |
Nutritional counseling, low-glycemic index or low carbohydrate diet; consider early referral to endocrinology; consider Zone 2 training, supplementation with cocoa flavanols |
• Possible reduction in age-related cognitive dysfunction[173] |
|
Hyperlipidemia (elevated ApoB, LDL-C, and/or LDL-P) |
Early referral to preventive cardiology |
• Management of dementia-related cardiovascular risk factors |
|
Exercise |
||
|
Aerobic/Resistance training |
Increased overall amount and intensity of exercise |
• Helps counteract the increased clinical decline and brain atrophy in ApoE4 carriers |
|
HIIT |
Implementation of HIIT in regular exercise routine[195] |
• Higher intensity exercise may protect against cognitive decline for ApoE4 carriers[342] |
Abbreviations: ABCA1, ATP binding cassette subfamily A member 1; AD, Alzheimer's disease; AGE, advanced glycation end; ApoB, apolipoprotein B; Aβ, amyloid-beta; CypA-NFκB-MMP9, cyclophilin A-nuclear factor kappa B-matrix metallopeptidase 9; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; GSK3β, glycogen synthase kinase-3β; HIIT, high-intensity interval training; LDL-C, low-density lipoprotein cholesterol; LDL-P, low-density lipoprotein particles; LRP1, LDL receptor-related protein 1; NLRP3, NOD-, LRR-, and pyrin domain-containing protein 3; RBC, red blood cell.
|
Risk factor |
Individual factor |
Intervention considerations |
Servings |
|---|---|---|---|
|
Diet[129] |
|||
|
Green leafy vegetables |
6 or more servings/week |
||
|
Other vegetables |
6 or more servings/week |
||
|
Berries |
2 or more servings/week |
||
|
Other whole fruit (low glycemic) |
7–14 servings/week |
||
|
Plant-based fats (i.e., avocado, seeds) |
5 or more servings/week |
||
|
Legumes |
5 or fewer servings/week |
||
|
Whole grains |
1–2 servings/day |
||
|
Fish (not fried or shelled) |
2–4 servings/week |
||
|
Poultry (not fried) |
4 or fewer servings/week |
||
|
Eggs |
4–8 or fewer/week |
||
|
Unprocessed red meat and pork (grass-fed when possible) |
2 or fewer servings/week |
||
|
Coffee, tea |
2 or more servings/day |
||
|
Dark cocoa powder |
5–7 servings/week |
||
|
Wine, other alcohol |
Women: 1 serving/day |
||
|
Men: 1–2 serving/day |
|||
|
Extra virgin olive oil |
Preferred over other monounsaturated fats |
||
|
Evidence of insulin resistance, elevated visceral body fat, or elevated waist:hip ratio |
Time-restricted eating pattern |
12–16 h ∼5 d/wk |
|
|
Total carbohydrates |
≤120 g/d daily depending on amount of regular exercise |
||
|
Fast fried foods |
Limit intake |
||
|
Desserts, pastries, sweets |
Limit intake |
||
|
Nutritional biomarkers |
|||
|
Low RBC omega-3 (EPA/DHA)/omega-3 index |
|||
|
Vitamin D deficiency |
Cholecalciferol +/− daily, brief exposure to sunlight[345] [346] |
||
|
Vitamin B12 deficiency |
With absorption deficit[347] |
Oral vs. IM B12 supplementation; nutritional counseling[163] |
|
|
With absorption and/or potential genetic methylation deficit (e.g., MTHFR) |
Methylated B12 or B complex |
||
|
With elevated homocysteine |
Consider methylated B-complex vitamins (folate, pyridoxine, cobalamin); TMG; NAC[347] [348] |
||
|
Exercise |
|||
|
Female |
Greater ratio of cardiovascular to resistance training[87] [88] [89] [90] [91] [92] [93] [94] |
||
|
Male |
Equal-to-greater ratio of resistance to cardiovascular training |
||
|
Elevated visceral body fat |
Cardiovascular exercises, such as fast walking (Zone 2, 65–70% of maximum heart rate), running, swimming, and cycling; HIIT |
||
|
Low muscle mass |
Resistance training to improve strength and endurance, often with use of weights |
||
|
Insulin resistance |
Zone 2 or steady-state cardiovascular training; HIIT |
||
|
Sleep |
|||
|
Insufficient sleep/sleep disturbances |
Maintain a consistent sleep schedule and optimize sleep environment |
||
|
Careful review to identify sources of impaired sleep |
|||
|
Limit use of electronics and restrict food and alcohol use before bed |
|||
|
Avoid caffeine after ∼1 pm |
|||
|
Avoid sleep aids such as Benadryl |
|||
|
Consider low-dose melatonin |
|||
|
Sleep apnea |
Type of apnea |
CPAP or other treatment as indicated Refer to sleep specialist |
|
|
Education |
|||
|
Suboptimal cognitive activity or reserve |
Adult education and/or cognitive training Second language training or musical training |
||
|
Social interaction |
|||
|
Social isolation |
Referral to social worker or geriatric care manager Encourage activity programs and social engagement[243] [352] |
||
|
Mental health/stress |
|||
|
Chronic stress, depression, and/or anxiety |
Depression may pose higher risk in males[252] |
Mindfulness training, meditation, periodic vacations, cognitive behavioral therapy, exercise counseling +/− medication[105] [106] [107] [108] [110] [111] [112] |
|
|
Stress and anxiety may pose higher risk in females; Females may be more vulnerable to depression risk in the perimenopausal period[100] [101] [102] [103] [104] |
As above May also benefit more from vacation and meditation[110] [113] |
||
|
Management of other medical conditions |
|||
|
Hearing loss |
Management of hearing loss Introduction of hearing devices as per recommendation of primary care physician |
||
|
Periodontal disease |
Consistent oral hygiene through teeth brushing and flossing |
||
|
Regular dental check-ups and teeth cleanings |
|||
|
Perimenopause (<5–7 y after start of menopause transition) |
Careful consideration of risks/benefits of type, route, and dose of HRT for an individualized period of time[82] [84] |
||
|
Induced menopause[355] |
|||
|
Hypertension |
Midlife[173] |
Systolic BP target of 120 mm Hg or lower and diastolic BP target of 70 or lower mm Hg.[212] [213] Consider ARBs (especially candesartan and telmisartan) or ACE inhibitors[212] [213] [214] [215] Avoid CNS-active beta-blockers[216] |
|
|
Insulin resistance/type 2 diabetes mellitus |
With unhealthy lifestyle[173] |
Lifestyle counseling |
|
|
Already healthy lifestyle |
Consider referral to endocrinology; exercise as above, supplementation with cocoa flavanols; TRE[173] |
||
|
May pose higher risk for females[86] |
As above Tighter targets for control |
||
|
Hyperlipidemia |
Due to elevated sterol absorption |
Ezetimibe Refer to preventive cardiologist[356] |
|
|
Due to elevated sterol production |
Hydrophilic statin therapy Refer to preventive cardiologist[357] |
||
|
Refractory to monotherapy |
May benefit more with combination therapy (e.g., statin and ezetimibe) Refer to preventive cardiologist to discuss PCSK9i[356] |
||
|
Elevated cystatin or reduced GFR |
Early referral to internal medicine and/or nephrology[358] |
||
|
Elevated systemic inflammatory markers |
Careful review of potential etiologies; consider supplementation with curcumin |
||
Abbreviations: ACE, angiotensin-converting enzyme; ARBs, angiotensin II receptor blocker; BP, blood pressure; CNS, central nervous system; CPAP, continuous positive airway pressure; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; GFR, glomerular filtration rate; HIIT, high-intensity interval training; IM, intramuscular; MTHFR, methylenetetrahydrofolate reductase; NAC, N-acetyl cysteine; PCSK9i, proprotein convertase subtilisin/kexin type 9 inhibitor; RBC, red blood cell; TMG, trimethylglycine; TRE, time-restricted eating.
#
Risk Factors and Interventions
Age
The most significant risk factor for AD is advanced age.[44] In fact, AD risk doubles every 5 years after the age of 65 years, and the number of Americans older than 65 years is projected to increase from 40.2 million in 2010 to 88.5 million in 2050.[60] [61] Although the aging process itself contributes to the risk of neurodegeneration, dementia is not a normal part of aging. As the brain ages, white matter volume decreases much more significantly than grey matter volume, but in those with AD, the rate of neuronal dysfunction, neuronal loss, and cognitive decline is accelerated.[62] [63] There are many molecular and systemic hallmarks of aging that correlate with susceptibility to neurodegenerative disease such as genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, and mitochondrial dysfunction.[64] Aging is also characterized by cellular senescence and chronic, low-grade systemic inflammation—a process colloquially referred to as “inflammaging”—which is strongly associated with AD.[65] [66] In acknowledgment of this theory, a recent study demonstrated the benefit of low/anti-inflammatory diet plans for older at-risk patients.[67] Other hallmarks of aging—deregulated nutrient sensing, stem cell exhaustion, altered intercellular communication—also correlate with susceptibility to neurodegenerative disease.[64]
#
Biological Sex
Research has suggested that the second most significant risk factor for AD is female sex. In fact, two-thirds of all AD patients are females, and postmenopausal women comprise over 60% of affected females.[68] [69] Research continues to discern the reasons for this disparity, but statistical models have shown that women still possess twice the risk of men even when accounting for gender-dependent mortality rates, age at death, and differences in lifespan.[70] [71] A growing body of evidence suggests differences in brain anatomy, function, and age-related morphological changes between women and men are involved.[71] The “estrogen hypothesis” posits that sex hormones, 17β-estradiol specifically, exert a neuroprotective effect on female brains. Estrogen dysfunction in the years leading up to and after menopause seems to exacerbate (or precipitate) the AD process in women in contrast to men of the same age.[72] Such research implicates the menopause transition (MT)—a midlife neuroendocrine transition state unique to females—in their higher risk for AD.[73] During the MT, the estrogen network uncouples from the brain's bioenergetic system, and the resulting hypometabolic state may serve as the substrate for neurological dysfunction. Women experiencing menopause may present neurological symptoms (disruption of estrogen-regulated systems like thermoregulation, sleep, and circadian rhythms), depression, and impairment in multiple cognitive domains.[74] Such unique circumstances for developing dementia warrant sex-specific recommendations when pursuing personalized risk reduction.
Research has been mixed as to the efficacy of hormone-replacement therapy (HRT) in protecting women from cognitive decline. Earlier studies generally showed a lack of benefit and even a potential harmful effect, whereas recent investigations indicate that the effectiveness of estrogen depends on multiple factors, such as the time of initiation of HRT, the individual's cognitive functioning at the time of HRT initiation, and the forms of hormones used.[75] [76] [77] [78] [79] [80] [81] [82] [83] [84] Hypertension—a major risk factor for both cognitive decline and cardiovascular diseases—increases significantly in women after menopause, which suggests an additional need for female-specific cardiovascular interventions.[85]
Furthermore, insulin resistance and/or type 2 diabetes mellitus (DM2) may pose a higher risk for females than for males, thus warranting more aggressive management.[86] In patients with added risk due to physical inactivity, women seem to benefit more from a greater ratio of cardiovascular-to-resistance training than men, and both sexes should receive sex-specific nutritional counseling.[87] [88] [89] [90] [91] [92] [93] [94] [95] Women also face an added risk from suboptimal cognitive activity or reserve, for which they can be recommended adult education and cognitive training or second language or musical training.[96] [97] [98] [99] While depression generally poses a higher risk for men, stress and anxiety pose a higher risk in women, and women may be more vulnerable to depression risk in the perimenopausal period.[100] [101] [102] [103] [104] For mental health purposes, both women and men may be recommended mindfulness training, meditation, periodic vacations, cognitive behavioral therapy, exercise counseling, and/or medication.[105] [106] [107] [108] [109] [110] [111] [112] [113] In a follow-up analysis to the CEDAR study, it was found that individualized multidomain interventions may offer equal cognitive benefits to both women and men when such sex-specific factors are employed, as well as better mitigation of calculated AD and CV risk in women compared to men.[114]
#
Genetics
The genetic architecture of AD is complex and an area of ongoing active investigation. While highly penetrant autosomal dominate mutations exist, they account for less than 1% of all AD cases and are associated with early-onset AD.[115] Late-onset AD has a more complicated etiology influenced by lifestyle factors, polygenetic heterogeneity, and epigenetic interactions.[116] [117] [118] Early risk reduction interventions, guided by risk stratification that considers genetics, allows for more personalized care.
As discussed, the ApoE gene is the most significant genetic risk factor. ApoE encodes a surface peptide found on plasma lipoproteins and is responsible for the transport, metabolism, and redistribution of lipids in the body, especially in the CNS.[41] The three ApoE variants have different affinities for lipoproteins and receptors, with ApoE2 and ApoE4 having a significant influence on lipid and lipoprotein levels.[119] In general, ApoE4 is associated with an increase in LDL-C and ApoB and, therefore, a higher cardiovascular risk.[120] [121] [122] [123] [124] [125] [126] [127] ApoE2, on the other hand, is associated with a three- to fourfold decrease in LDL-C compared to ApoE4. ApoE4 carriers may also be more susceptible to certain modifiable lifestyle factors than noncarriers. For example, individuals with the ApoE4 genotype who live a sedentary lifestyle, smoke, or consume alcohol possess a higher risk for developing AD than those who do not carry the ApoE4 allele.[128] [129] Given the propensity of ApoE4 carriers to develop hyperlipidemia and atherosclerosis, early referral to a preventive cardiology specialist may be warranted based on individual factors, such as family history, serum lipid markers, and other evidence of early atherosclerotic changes. Statin therapy may provide a greater therapeutic efficacy in ApoE4 homozygotes.[130]
Although ApoE4 increases risk of AD, research indicates that ApoE4 magnifies the impact of certain modifiable factors such as physical inactivity, obesity, tobacco use, alcohol consumption, and insulin resistance compared to those without ApoE4.[128] [131] [132] Addressing these factors may lead to a greater potential for success. Due to its differential effect on lipid metabolism, neuroinflammation, and glucose metabolism, ApoE4 may provide a highly targeted and distinct approach to AD prevention interventions (see [Table 2]).[133] Optimizing insulin sensitivity through low-glycemic index or low-carbohydrate diets should be a priority. Additionally, fatty fish is rich in the omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), and consumption and/or supplementation is especially critical for ApoE4 carriers. Higher doses of DHA may be required due to ApoE4-induced metabolic alterations and BBB dysfunction.[133] [134] [135] Studies show that the phenolic compounds oleocanthal and hydroxytyrosol found in extra virgin olive oil display anti-amyloid and anti-tau properties and may act on specific pathways adversely affected in ApoE4 carriers.[136] [137] [138] [139] ApoE4 carriers may be more susceptible to pesticide exposure, specifically dichlorodiphenyldichloroethylene (DDE), and thus should be educated on the need to wash all produce properly as well as the potential benefits of buying organic. Other factors including hypertension, vitamin D supplementation, cognitive engagement, and physical activity may also warrant greater attention and more specific recommendations (see [Table 2]).[21] [128] [140] [141]
#
Dietary Patterns
Several epidemiologic studies have reported an association between dietary patterns and risk for various forms of dementia, including AD.[142] [143] There are sufficient data for the recommendation of a Mediterranean diet (MeDi) and Mediterranean–DASH Intervention for Neurocognitive Delay (MIND) diet to support cognitive function and reduce dementia risk.[144] The MIND diet, similar to the Mediterranean diet but with further focus on lowering blood pressure (BP), emphasizes plant-based foods and encourages eating green leafy vegetables, berries, whole grains, fish, poultry, beans, nuts, wine, and olive oil. Research supporting the MIND diet consists of evidence from 900 dementia-free older adults, showing an association with reduced AD risk and slower rate of cognitive decline.[145] Certain aspects of a MeDi, such as its emphasis on an intake of lower glycemic carbohydrates, healthy fats, leafy vegetables, and lean proteins, are associated with delay in the onset of dementia and a decrease in AD risk.[146] [147] [148] [149] Higher adherence to the MeDi is associated with reduced risk in developing MCI and reduced risk for conversion of MCI to AD, while lower adherence to the MeDi is associated with progressive AD biomarker abnormalities in middle-aged adults.[150] [151] A meta-analysis of 26 different studies investigating different dietary habits and their subsequent AD risk showed that a healthy diet can decrease oxidative stress, inflammation, and accumulation of Aβ, therefore lowering AD risk.[152]
Inflammation is a risk factor for dementia and may be modulated by various nutritional patterns/interventions. As referenced prior, low inflammatory/anti-inflammatory diets are associated with a lower incidence of dementia.[67] Though restrictive and often difficult to adhere to, the ketogenic diet has been shown to decrease systemic inflammation and may have the potential to delay the progression of dementia.[153] [154]
Time-restricted eating and intermittent fasting may also be neuroprotective by promoting the process of autophagy in the brain.[155] [156] Studies report that intermittent fasting may attenuate the progression of dementia by improving cognitive dysfunction, inhibiting hippocampal neuronal damage against oxidative stress, reducing neuroinflammation, and increasing the production of neurotrophic factors.[157] [158] [159] However, the decision to recommend time-restricted eating or intermittent fasting needs to be based on individual factors such as comorbid conditions, body composition, and other personal needs and considerations.[160] Dietary recommendations are summarized in [Table 3].
#
Dietary Components, Vitamins, and Supplements
The use of vitamins and other nutritional supplements may also be considered using a precision medicine approach. An additional risk for dementia is elevated total plasma homocysteine, an amino acid metabolite which induces oxidative stress. Those with elevated homocysteine levels (generally >10 μmol/L) may benefit from a B-complex vitamin which contains B6, B12, and folate. Additionally, higher levels of both vitamin B6 and B12 have been associated with improved cognitive function in midlife and attenuated brain atrophy for those with elevated omega-3 fatty acid levels.[133] [161] Methylenetetrahydrofolate reductase (MTHFR) plays a critical role in folate metabolism, and two polymorphisms in the MTHFR gene, MTHFR-C667T and -A1298C, are associated with high serum homocysteine levels.[162] Those with MTHFR polymorphisms and elevated homocysteine may benefit from supplementation with a methylated B vitamin complex to allow for better metabolism of homocysteine, though further investigation is needed.[21] [163] [164]
Furthermore, vitamin D deficiency is a known risk factor for AD and potential supplementation for AD risk reduction may be considered.[59] [133] [165] [166] Generally, a vitamin D serum level of 30 nmol/L is considered a target for treatment, though recent studies have suggested a range of 50 to 70 nmol/L may be more beneficial.[167]
Omega-3 fatty acids (DHA and EPA) are essential polyunsaturated fats that support cardiovascular function, lower triglycerides, and reduce inflammation. By increasing cell membrane fluidity, they promote the synaptic plasticity essential for learning, memory, and other cognitive processes.[168] Regular consumption of fatty fish including salmon, albacore tuna, sardines, mackerel, lake trout, anchovies, and herring provides a rich source of omega-3 fatty acids, but for some supplementation may also be necessary. Most western diets are much higher in omega-6 compared to omega-3 due to consumption of plant oils like canola. Serum fatty acid balance tests can be used to guide treatment decisions with a target of a 4:1 ratio omega-3 to 6. Before recommending an omega-3 supplementation, risks and benefits should be discussed, and all patients on supplementation should be monitored for potential adverse effects, including bleeding and possible increased risk of atrial fibrillation based on some recent studies.[169] [170]
Oxidative stress can contribute to neurodegeneration and, hence, dietary consumption of antioxidants including green leafy vegetables and berries is recommended.[165] [171] Flavanols are another group of compounds with both antioxidant and anti-inflammatory properties that may have a role in delaying or preventing the onset of dementia.[172] Some dietary sources of flavanols include cocoa, kale, tomatoes, apples, blueberries, and tea. In a 2020 study, 921 cognitively normal elders were followed up for 6 years after which 220 participants (24%) developed AD.[172] Results showed that a higher flavanol intake was associated with a 48% decrease in risk for AD. Cocoa flavanols may also support memory function, BP regulation, and glucose metabolism, and supplementation may be considered based on these factors.[173] [174] [175] [176] [177] [178] [179] [180] [181]
Curcumin, also known as turmeric, is a polyphenolic compound with antioxidant, anti-inflammatory, and neuro- and chemoprotective properties that have traditionally been used as a remedy for many illnesses in India and China.[182] [183] Animal studies have definitively shown beneficial effects of curcumin on a molecular and behavioral level, but clinical studies remain mixed as to its cognitive benefits.[182] [184] Nevertheless, some evidence has shown that curcumin can improve cognitive functioning in patients with AD.[185] This benefit is thought to stem from curcumin's ability to cross the BBB and interfere with cellular signaling pathways and various molecular targets. Its antioxidant properties come from its ability to scavenge free radicals such as reactive oxygen species and reactive nitrogen species. Its anti-inflammatory benefits and other properties—decreasing Aβ plaques, delaying degradation of neurons, decreasing microglia formation—may also be responsible for any identified cognitive benefits.[185]
#
Alcohol
Light-to-moderate alcohol consumption has been associated with a decreased risk of AD, whereas heavy consumption may increase risk, and this relationship appears to be true for VaD as well.[186] [187] [188] [189] Surprisingly, some evidence has also found abstaining from drinking to be associated with a higher risk of AD. In fact, one longitudinal study found nondrinkers and heavy drinkers both be twice as likely to have MCI in old age as light drinkers, and another saw an increased risk of dementia only in nondrinkers and those who consumed more than 14 servings per week.[190] [191] A meta-analysis conducted on participants with AD, VaD, and other types of dementia found drinkers to have a reduced risk of AD and dementia in general—but not a reduced risk of cognitive decline—when compared to nondrinkers.[186] A variety of positive effects of alcohol on the CNS have been suggested, most having to do with reduction of cardiovascular risk factors.[189] Further research is required, however, to identify the effects of alcohol on dementia pathogenesis and progression.
Despite the detrimental effects of heavy alcohol consumption on cognition being widely agreed upon, the benefit of light-to-moderate drinking does continue to receive debate.[189] Varying dosage definitions, ages of participants, and lengths of studies may lead to different outcomes in epidemiological studies concerning low-to-moderate alcohol consumption and dementia risk, so more standardized investigation is necessary.[189]
Future investigation should also focus on differing effects of alcohol consumption on dementia risk between women and men, across socioeconomic statuses, and between other subgroups. For instance, the relationship between alcohol consumption and dementia risk seems to be modified by ApoE genotype, as consumption of any amount or type of alcohol has been found to increase AD risk for ApoE4 carriers.[132] One study conducted in individuals aged 65 and older without dementia at baseline found up to three servings of wine per day to be associated with a decreased risk of AD—but only for individuals without ApoE4.[188] This further emphasizes the importance of personalized interventions guided by accurate risk stratification.
#
Exercise
Several reviews and meta-analyses have concluded that regular physical activity has general therapeutic potential, but substantial variation exists in exercise benefits on cognitive health and dementia risk reduction at the individual level. As such, clinical evaluation and analysis of anthropometrics, biomarkers, and cognitive testing should be used to guide individualized recommended physical activity. For example, studies have shown that ApoE4 carriers see greater long-term benefits from increased exercise.[128] Such exercise interventions have shown to be more beneficial during the preclinical stage of AD than in later clinical stages.[192]
High-intensity interval training (HIIT), which entails short bursts of extreme exertion (85–95% maximum heart rate, depending on the protocol[193]) followed by recovery periods, has received increased attention in recent years thanks to its capacity for metabolic, cardiovascular, and pulmonary benefits coupled with the attraction of less time spent exercising.[194] It has been shown that HIIT may be more beneficial for ApoE4 carriers than noncarriers, and it is especially beneficial for individuals with elevated homocysteine due to MTHFR mutations.[129] [195] Furthermore, HIIT has the potential to decrease LDL, increase HDL, and improve insulin sensitivity more effectively than moderate-intensity aerobic training, and these factors carry influence on individual AD risk.[196] [197]
Compared to HIIT, lower-intensity steady-state cardiovascular training (also called zone 2 training) is traditionally defined as a more moderate intensity (∼65% maximum heart rate), longer duration aerobic exercise, but, on a cellular level, is defined as the range at which maximum ATP is produced in the mitochondria under aerobic conditions. The evidence seems to support the benefit of HIIT in improving aerobic capacity, but findings have been mixed as to whether HIIT or steady-state cardiovascular is more effective in improving VO2max (maximum rate of oxygen).[198] [199] [200] [201] It has been shown, though, that steady-state cardio is associated with more substantial decline in resting heart rate and body weight than HIIT due to a resultant increase in mitochondrial density and efficiency.[202] Therefore, while it should be a part of all exercise plans, it may be especially important on a regular basis (e.g., three times a week) and for longer durations (e.g., at least 45–60 minutes per session) in those with elevated visceral body fat. Other benefits include decrease in BP, lower risk of injury, and improvement in insulin resistance.[203]
Another commonly recommended type of exercise is resistance training (also called strength and weight training), which best improves lean muscle mass and metabolism. Resistance training has shown to reduce cardiovascular risk factors—which are associated with cognitive decline and dementia—and to promote neurotrophic factors that are beneficial for the brain.[204] The SMART (Study of Mental and Resistance Training) trial supported the positive impact of resistance training on cognition and occurrence of white matter lesions.[205] According to additional evidence, males may benefit from an equal-to-greater ratio of resistance to cardiovascular training, while females may benefit from a greater ratio of cardiovascular to resistance training, further highlighting the need for individualized and sex-specific exercise interventions.[206] The correct dose or amount of exercise, as determined by frequency, duration, and intensity, per patient should be informed by their comprehensive clinical evaluation. One randomized controlled trial conducted showed that resistance training three times per week for a total of 24 weeks significantly improved cognitive function among male seniors aged 65 to 75 years.[93] Another study found that once- and twice-weekly resistance training significantly improve executive functions in senior women.[92] Patients should be counseled on the need to consume adequate amounts of protein and carbohydrates surrounding strength training to mitigate the risk of losing rather than gaining muscle mass.
In all, physical activity reduces key cardiovascular and metabolic risk factors for dementia, such as hypertension (HTN) and insulin resistance, on top of providing benefits to cognitive health.[207] [208] The recommended dose and type of exercise should depend on longitudinal anthropometric assessments, and the individual abilities and responses of each patient.[129]
#
Hypertension
Midlife stage 1 and stage 2 systolic HTN is associated with an 18 and 25% increased risk of AD, respectively, though HTN has also been linked to worse cognitive function, behavioral symptoms, and hippocampal glucose metabolism.[209] Additionally, elevated BP and pulse pressure is associated with Aβ and p-tau deposition.[210] There are eight completed randomized controlled trials to date that have examined various approaches to BP lowering on dementia outcomes.[211] As of 2018, the data more collectively support a significant reduced risk of dementia with aggressive systolic BP lowering (at or below 120 mm Hg) compared to a standard systolic treatment goal (<140 mm Hg) with the results from the Systolic Blood Pressure Intervention Trial - Memory and Cognition in Decreased Hypertension (SPRINT-MIND) study.[212] Diastolic BP should also be targeted at or below 70 mm Hg based on this study. Although further study evaluating cerebrovascular-specific pathological endpoints such as MRI brain is needed, the totality of current evidence supports targeting a systolic BP of 120 mm Hg or lower without evidence of significant harm.[212] [213] Optimal pharmacological agents are unknown and may depend on personal factors, but data support use of angiotensin II receptor blockers (ARBs) such as candesartan and telmisartan and ACE inhibitors over diuretics, and avoidance of CNS-penetrating beta blockers.[212] [213] [214] [215] [216]
#
Hyperlipidemia
The identification of ApoE4 as the major genetic risk factor for AD helped elucidate the relationship between lipids and cholesterol and AD. Literature has confirmed the association between high LDL and dementia risk independent of the effects of ApoE status and some research suggests that midlife hyperlipidemia may be more impactful on AD risk later in life.[217] [218] [219] [220] However, studies also show low total cholesterol in late life can be detrimental for neural function and memory suggesting a delicate cholesterol balance in the brain.[221] [222] Desmosterol, a precursor of cholesterol, can be metabolized in the brain, and is important in the degradation of APP and has been shown to inhibit formation of Aβ. Lower desmosterol levels are found in plasma, brains, and CSF of AD patients compared to controls and this supports the emerging hypothesis that desmosterol may serve as a marker for cholesterol metabolism in the brain.[223] Statin use is associated with decreased risk of dementia in many studies and while inconclusive, some demonstrate a differential effect depending on pharmacodynamic properties. Few report that lipophilic statins may increase risk of dementia. At this stage, the mechanism of this increased risk is unknown but possibly may be due to increased penetration of the BBB, thereby blocking cholesterol production in the brain.[224] As statins therapy reduces desmosterol production, low levels of desmosterol may suggest that cholesterol synthesis is over-suppressed in the brain and could potentially guide treatment decisions.
#
Metabolic Comorbidities
The brain is a very highly metabolic tissue and depends heavily on glucose metabolism for neuronal synaptic transmission. Thus, alterations in glucose availability and utilization as found in conditions such as obesity, insulin resistance, and DM2 are postulated to lead to neurodegeneration and Aβ and tau protein phosphorylation.[225] [226] [227] The idea of glucose-mediated neurodegeneration has inspired investigation into the use of antidiabetic agents for treating AD. Specific interventions for those with insulin resistance and/or DM2 may include lifestyle counseling, pharmacological treatment with evidence supporting semaglutide and metformin, and supplements like cocoa flavanols.[173] [228]
#
Education and Cognitive Engagement
Having more years of education is associated with lower risk of dementia.[229] [230] This association is possibly due to the improvement of cognitive reserve with increased education but is also impacted by early life cognitive development (which is related to genetics, socioeconomic status, psychosocial, and other variables). Early life educational attainment was found to have a protective effect on total brain volume, specifically during the MCI stage of AD.[231] Consistent cognitive engagement throughout life such as learning a new language or how to play an instrument is associated with improved cognitive function.[98] [99] [232] [233] Studies also show that those with a history of reading, writing, and playing games had lower levels of amyloid deposition on PET imaging suggesting that cognitive engagement may influence the onset or progression of AD.[234]
#
Social Interaction
Social isolation and loneliness—major sources of mental and psychosocial stress—are also risk factors for dementia. Research shows that social isolation may be associated with neuronal degeneration, while a rich social life may slow cognitive aging and be neuroprotective against AD.[235] Though the exact mechanisms linking isolation to dementia are not completely understood, it has been proposed that production of Aβ, the p-tau protein, and increases in oxidative stress and inflammation are involved.[236] [237] [238] Social enrichment in older adults has been associated with increased levels of BDNF, which increases neuroplasticity and promotes synaptic consolidation.[239] Several studies on the association between social support and dementia have shown that this association may differ between women and men. In one study, social activities were associated with less memory decline in men in their midlife and old age, but this relationship was not found in women.[240] In another, support from co-residing with family members and being married was protective among men, while community engagement was protective for women.[241] Social enrichment interventions may be most beneficial when they are also mentally engaging, associated with physical activity, or provide a sense of purpose and can even be technology-based.[242] [243] [244]
#
Mental Health and Stress
Findings suggest that depression, anxiety, and chronic stress are associated with dementia and AD development among asymptomatic patients. Stress raises cortisol and acutely may have a positive effect on cognition. However, prolonged cortisol elevation due to chronic stress and rumination leads to a detrimental effect on memory, may accelerate brain aging, and may contribute to neurodegeneration.[245] Depression-related symptoms in AD adults have been shown to affect dementia risk through neurodegeneration in AD-related brain regions; however, this is shown independently of amyloid and p-tau risk.[246] Anxiety has shown to predict individual risk of both AD and VaD, and prolonged stressful experiences have been associated with conversion from MCI to dementia.[247] [248] In one 35-year longitudinal study, risk of dementia increased in women who reported frequent or constant stress, and reporting stress at one, two, or three examinations correlated with a sequentially higher dementia risk in participants.[249] The relationship between stress and dementia is made even more evident by the possible twofold higher risk of dementia incurred by posttraumatic stress disorder (PTSD).[250] [251] Research also shows depression-associated risk may be more substantial in males, while stress and anxiety-associated risk may be more substantial in females.[100] [101] [102] [252] [253] Decreasing the threat posed by these psychological conditions is yet another avenue for preventing or delaying the onset of dementia.[254] [255] In addition to positive effects on mood, evidence suggests that some therapies (such as Lexapro) carry anti-amyloid benefits.[256] Individualized recommendations may include mindfulness training, meditation, periodic vacations, cognitive behavioral therapy, exercise counseling, and medication.[98] [107] [108] [110] [111] [112] [113] [257] [258] [259] [260]
#
Sleep
Evidence from several observational studies demonstrates that both too short and too long sleep duration are associated with cognitive decline and risk of dementia.[261] [262] [263] In older adults, changes in sleep duration and patterns are also associated with increased risk of dementia, but are also a marker for early AD pathology.[264] [265] [266] [267] [268] [269] [270] In a study of more than 2,800 participants, those who slept less than 5 hours per night were twice as likely to develop dementia—and twice as likely to die—compared to those who slept 6 to 8 hours per night.[271] Data from a 30-year Europe cohort of almost 8,000 participants showed a 30% increase in dementia risk in those who slept for 6 hours or less at ages 50, 60, and 70 years independent of other confounding factors and ApoE genotype.[272] Clearance of Aβ is ascribed to the glymphatic system which operates most efficiency during slow wave sleep.[273] In fact, in one study, Aβ accumulation imaging increased by 5% in healthy controls after a single night of sleep deprivation.[274] Others have demonstrated similar findings in the CSF.[275] Additionally, rapid eye movement (REM) stage sleep is essential for memory consolidation and reduction in REM sleep is associated with dementia risk.[276]
While sleep need is highly individualized, most healthy adults require 7 to 8 uninterrupted hours of sleep.[277] Guidance on good sleep hygiene practice should be provided including avoiding caffeine consumption after 1 pm; restricting food, alcohol, and the use of electronics before bed; maintaining a consistent sleep schedule every day; and optimizing sleep environment.[21] Anticholinergics, benzodiazepines, and z-hypnotics should be limited due to their associated dementia risk.[278] [279]
Referral for management of comorbid conditions that affect sleep quality such as nocturia due to benign prostate hypertrophy may be required. Another highly prevalent and treatable condition is obstructive sleep apnea (OSA).[280] OSA is associated with increased AD risk with women suffering the adverse effects more than men despite the less frequent presentation of moderate-to-severe OSA in women.[280] In one study, patients with OSA were found to have a 1.70 times greater risk for dementia within 5 years of diagnosis compared to age- and sex-matched patients without OSA.[281] Another study conducted in 2021 found significant associations between OSA and brain white matter hyperintensities (WMHs)—commonly observed in older people and significantly associated with AD—which indicates a novel pathological mechanism linking OSA and dementia.[282] As such, screening for symptoms of OSA should be included as a part of a comprehensive AD risk reduction plan.
#
Other Medical Conditions
Other significant risk factors for dementia include hearing loss, past traumatic head injuries, and smoking. Hearing impairment significantly increases the risk of AD and other cognitive disorders (though this association is not causal and requires further investigation), and the progression of dementia is faster in those with hearing loss than without it.[283] [284] [285] As such, when applicable, audiometry evaluation should be considered. Furthermore, robust evidence indicates that approximately 30% of patients who die from traumatic brain injuries (TBIs) have Aβ plaques in their brains—the pathological hallmark of AD—signaling an association between head injuries and neurodegenerative disease.[286] While accidents are unavoidable, risk may be mitigated by wearing a helmet during high-risk activities and a seat belt in motor vehicles. Cigarette smoking also confers an increased risk of AD—an effect that has tended to be stable over time—and heavy consumption in middle-aged smokers can increase the risk of dementia by more than 100% compared to non-smokers.[287] [288] For this and other adverse effects on overall health, smokers should be counseled on smoking cessation and provided other cessation support resources.
Periodontal disease affects 70% of adults 65 and older and is another modifiable medical condition that may be associated with dementia.[289] [290] [291] [292] [293] In a recent analysis by NIA scientists, gum disease was associated with the development of all-cause dementia and especially VaD.[291] It has been proposed that Porphyromonas gingivalis, the bacteria that most commonly causes gum disease, can lead to the production of Aβ. Inflammation may serve as another connecting link between periodontitis and dementia.[294] [295] [296] [297] Patients should be educated on the importance of proper oral hygiene and following up regularly with their dentist. Bidirectional care integration between dental and medical providers may best help mitigate patient's risk. Further clinical research is needed in this emerging area, and this may be best served by collaborations among medical and dental providers and oral systemic health experts.[298]
#
#
Future Directions and Conclusion
Although the evidence supporting dementia prevention is substantial, many areas need further investigation. Individualized multidomain clinical care for AD prevention has already demonstrated benefit, as can be seen with the Alzheimer's Prevention Clinic (APC) at Weill Cornell Medical College/New York - Presbyterian, which was founded in 2013. The APC framework applies evidence-based principles of clinical precision medicine to tailor individualized recommendations.[20] [21] The National Institutes of Health defines precision medicine as “an emerging approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyle for each person.”[299] [300] In adaptation of this approach for use in a clinical setting, clinical precision medicine informs risk stratification and personalized intervention via comprehensive and longitudinal assessment of patients' anthropometrics, blood biomarkers, cognition, genetics, and family and clinical history.[21]
Moving forward, the utility of the clinical precision medicine approach will benefit from the expansion of genomic sequencing and direct-to-consumer testing, as AD risk and clinical course is thought to be impacted by the polygenetic factors.[301] The interest in broader-scale genetic data to guide clinical decision-making has occurred in other medical specialties as well, and the comorbid risk factors for dementia have their own environmental and genetic contributors.[301] [302] [303] [304] It is hoped that self-provided genomic data, including whole genome sequencing and other at-home commercial qualitative genotyping, can be incorporated more regularly into medical practice to better identify disease risk and inform individualized risk reduction strategies. It is important to recognize the limitations that persist in the field of precision medicine, as progress and accessibility continues to be constrained by high costs, fear of genetic discrimination, access and availability of genetic testing, and inadequate and unprepared infrastructure.[305] [306]
Already many AD risk factors cluster around inequalities and inequities, which occur primarily in Black, Asian, Hispanic, and other marginalized ethnic groups and vulnerable populations.[11] To continue to progress within the field of dementia prevention, we must address these disparities. The differences in AD prevalence and pathophysiology between racial and ethnic groups are due to various factors, such as genetic variants associated with certain groups, but also with other environmental factors such as socioeconomic status, diet, or medical comorbidities, which are heavily influenced by inequity.[307] [308] [309] For instance, chronic health conditions that are associated with higher AD risk, such as cardiovascular disease and diabetes, disproportionately affect Black and Hispanic populations.[15] Worldwide, multisite research collaborations are required to construct a large and diverse cohort, and the APC framework may be applied. Further research is additionally needed to determine the comparative effectiveness of prevention interventions and ongoing follow-up is necessary to assess long-term effectiveness on the development of AD and other dementias.[21] [59]
Preventive care for dementia has not been routinely integrated into clinical practice in the United States, largely because it is not covered by Centers for Medicare/Medicaid Services and, therefore, private insurance policies. Considering the economic burden of dementia, its public health impact, the emergence of blood-based amyloid biomarkers, and growth of preventative practices, it is worthwhile to invest in and expand clinical prevention efforts for the benefit of tens of millions of patients in need. In 2022, a consortium of six clinical research sites in the United States (Weill Cornell Medicine/New York - Presbyterian in New York City, NY; Florida Atlantic University in Boca Raton, FL; Cleveland Clinic Lou Ruvo Center in Las Vegas, NV; Norton Neuroscience Institute in Louisville, KY; Alzheimer's Prevention Clinic and Research Center in San Juan, PR; Atria Medical in New York City, NY) and three globally (McGill University in Montreal, Canada; Jersey Memory Service in Jersey, United Kingdom; University of New South Wales/University of Notre Dame, St. Vincent's Hospital in Sydney, Australia) formalized plans to harmonize measures collected and better accomplish this goal.
#
#
Conflict of Interest
None declared.
-
References
- 1 Chin JH, Vora N. The global burden of neurologic diseases. Neurology 2014; 83 (04) 349-351
- 2 Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia: review. JAMA 2019; 322 (16) 1589-1599
- 3 Dementia [online]. Accessed November 14, 2022 at: https://www.who.int/news-room/fact-sheets/detail/dementia
- 4 Hurd MD, Martorell P, Delavande A, Mullen KJ, Langa KM. Monetary costs of dementia in the United States. N Engl J Med 2013; 368 (14) 1326-1334
- 5 Wimo A, Jönsson L, Bond J, Prince M, Winblad B, International AD. Alzheimer Disease International. The worldwide economic impact of dementia 2010. Alzheimers Dement 2013; 9 (01) 1-11.e3
- 6 Wimo A, Guerchet M, Ali G-C. et al. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement 2017; 13 (01) 1-7
- 7 Sosa-Ortiz AL, Acosta-Castillo I, Prince MJ. Epidemiology of dementias and Alzheimer's disease. Arch Med Res 2012; 43 (08) 600-608
- 8 Zucchella C, Sinforiani E, Tamburin S. et al. The multidisciplinary approach to Alzheimer's disease and dementia. A narrative review of non-pharmacological treatment. Front Neurol 2018; 9: 1058
- 9 Cummings J. New approaches to symptomatic treatments for Alzheimer's disease. Mol Neurodegener 2021; 16 (01) 2
- 10 World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines. 2019
- 11 Livingston G, Huntley J, Sommerlad A. et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020; 396 (10248): 413-446
- 12 Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM. Forecasting the global burden of Alzheimer's disease. Alzheimers Dement 2007; 3 (03) 186-191
- 13 Zissimopoulos J, Crimmins E, St Clair P. The value of delaying Alzheimer's disease onset. Forum Health Econ Policy 2014; 18 (01) 25-39
- 14 World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025. 2017
- 15 2021 Alzheimer's disease facts and figures. Alzheimers Dement 2021; 17 (03) 327-406
- 16 Risacher SL, Anderson WH, Charil A. et al; Alzheimer's Disease Neuroimaging Initiative. Alzheimer disease brain atrophy subtypes are associated with cognition and rate of decline. Neurology 2017; 89 (21) 2176-2186
- 17 Ossenkoppele R, Schonhaut DR, Schöll M. et al. Tau PET patterns mirror clinical and neuroanatomical variability in Alzheimer's disease. Brain 2016; 139 (Pt 5): 1551-1567
- 18 Vogel JW, Young AL, Oxtoby NP. et al; Alzheimer's Disease Neuroimaging Initiative. Four distinct trajectories of tau deposition identified in Alzheimer's disease. Nat Med 2021; 27 (05) 871-881
- 19 Ferreira D, Nordberg A, Westman E. Biological subtypes of Alzheimer disease: a systematic review and meta-analysis. Neurology 2020; 94 (10) 436-448
- 20 Seifan A, Isaacson R. The Alzheimer's Prevention Clinic at Weill Cornell Medical College/New York - Presbyterian Hospital: Risk Stratification and Personalized Early Intervention. J Prev Alzheimers Dis 2015; 2 (04) 254-266
- 21 Isaacson RS, Ganzer CA, Hristov H. et al. The clinical practice of risk reduction for Alzheimer's disease: a precision medicine approach. Alzheimers Dement 2018; 14 (12) 1663-1673
- 22 Duong S, Patel T, Chang F. Dementia: what pharmacists need to know. Can Pharm J 2017; 150 (02) 118-129
- 23 Nelson PT, Jicha GA, Kryscio RJ. et al. Low sensitivity in clinical diagnoses of dementia with Lewy bodies. J Neurol 2010; 257 (03) 359-366
- 24 Lindau M, Almkvist O, Kushi J. et al. First symptoms–frontotemporal dementia versus Alzheimer's disease. Dement Geriatr Cogn Disord 2000; 11 (05) 286-293
- 25 Devenney EM, Ahmed RM, Halliday G, Piguet O, Kiernan MC, Hodges JR. Psychiatric disorders in C9orf72 kindreds: study of 1,414 family members. Neurology 2018; 91 (16) e1498-e1507
- 26 Boeve BF, Silber MH, Ferman TJ, Lucas JA, Parisi JE. Association of REM sleep behavior disorder and neurodegenerative disease may reflect an underlying synucleinopathy. Mov Disord 2001; 16 (04) 622-630
- 27 Walker IM, Fullard ME, Morley JF, Duda JE. Olfaction as an early marker of Parkinson's disease and Alzheimer's disease. In: Swaab DF, Buijs RM, Kreier F, Lucassen PJ, Salehi A. eds. Handbook of Clinical Neurology. Elsevier; 2021: 317-329
- 28 Hsu F-C, Yuan M, Bowden DW. et al. Adiposity is inversely associated with hippocampal volume in African Americans and European Americans with diabetes. J Diabetes Complications 2016; 30 (08) 1506-1512
- 29 Power MC, Rawlings A, Sharrett AR. et al. Association of midlife lipids with 20-year cognitive change: a cohort study. Alzheimers Dement 2018; 14 (02) 167-177
- 30 Sniderman A, Langlois M, Cobbaert C. Update on apolipoprotein B. Curr Opin Lipidol 2021; 32 (04) 226-230
- 31 Pencina MJ, Pencina KM, Lloyd-Jones D, Catapano AL, Thanassoulis G, Sniderman AD. The expected 30-year benefits of early versus delayed primary prevention of cardiovascular disease by lipid lowering. Circulation 2020; 142 (09) 827-837
- 32 Slot RER, Van Harten AC, Kester MI. et al. Apolipoprotein A1 in cerebrospinal fluid and plasma and progression to Alzheimer's disease in non-demented elderly. J Alzheimers Dis 2017; 56 (02) 687-697
- 33 Mirza SS, de Bruijn RF, Koudstaal PJ. et al. The N-terminal pro B-type natriuretic peptide, and risk of dementia and cognitive decline: a 10-year follow-up study in the general population. J Neurol Neurosurg Psychiatry 2016; 87 (04) 356-362
- 34 de Nazareth AM. Type 2 diabetes mellitus in the pathophysiology of Alzheimer's disease. Dement Neuropsychol 2017; 11 (02) 105-113
- 35 Takeda S, Sato N, Uchio-Yamada K. et al. Diabetes-accelerated memory dysfunction via cerebrovascular inflammation and Abeta deposition in an Alzheimer mouse model with diabetes. Proc Natl Acad Sci U S A 2010; 107 (15) 7036-7041
- 36 Hackett K, Krikorian R, Giovannetti T. et al. Utility of the NIH Toolbox for assessment of prodromal Alzheimer's disease and dementia. Alzheimers Dement (Amst) 2018; 10: 764-772
- 37 Papp KV, Rentz DM, Orlovsky I, Sperling RA, Mormino EC. Optimizing the preclinical Alzheimer's cognitive composite with semantic processing: The PACC5. Alzheimers Dement (N Y) 2017; 3 (04) 668-677
- 38 Langbaum JB, Ellison NN, Caputo A. et al. The Alzheimer's Prevention Initiative Composite Cognitive Test: a practical measure for tracking cognitive decline in preclinical Alzheimer's disease. Alzheimers Res Ther 2020; 12 (01) 66
- 39 Mollenhauer B, Förstl H, Deuschl G, Storch A, Oertel W, Trenkwalder C. Lewy body and parkinsonian dementia: common, but often misdiagnosed conditions. Dtsch Arztebl Int 2010; 107 (39) 684-691
- 40 Silverberg NB, Ryan LM, Carrillo MC. et al. Assessment of cognition in early dementia. Alzheimers Dement 2011; 7 (03) e60-e76
- 41 Saunders AM, Trowers MK, Shimkets RA. et al. The role of apolipoprotein E in Alzheimer's disease: pharmacogenomic target selection. Biochim Biophys Acta 2000; 1502 (01) 85-94
- 42 Is Alzheimer's Genetic? [online]. Accessed November 14, 2022 at: https://www.alz.org/alzheimers-dementia/what-is-alzheimers/causes-and-risk-factors/genetics
- 43 Wu L, Zhao L. ApoE2 and Alzheimer's disease: time to take a closer look. Neural Regen Res 2016; 11 (03) 412-413
- 44 Scheltens P, De Strooper B, Kivipelto M. et al. Alzheimer's disease. Lancet 2021; 397 (10284): 1577-1590
- 45 Emrani S, Arain HA, DeMarshall C, Nuriel T. APOE4 is associated with cognitive and pathological heterogeneity in patients with Alzheimer's disease: a systematic review. Alzheimers Res Ther 2020; 12 (01) 141
- 46 Carrieri G, Bonafè M, De Luca M. et al. Mitochondrial DNA haplogroups and APOE4 allele are non-independent variables in sporadic Alzheimer's disease. Hum Genet 2001; 108 (03) 194-198
- 47 Erickson CM, Schultz SA, Oh JM. et al. KLOTHO heterozygosity attenuates APOE4-related amyloid burden in preclinical AD. Neurology 2019; 92 (16) e1878-e1889
- 48 Wang Y, Brinton RD. Triad of risk for late onset Alzheimer's: mitochondrial haplotype, APOE genotype and chromosomal sex. Front Aging Neurosci 2016; 8: 232
- 49 Belloy ME, Napolioni V, Han SS, Le Guen Y, Greicius MD. Alzheimer's Disease Neuroimaging Initiative. Association of klotho-VS heterozygosity with risk of Alzheimer disease in individuals who carry APOE4. JAMA Neurol 2020; 77 (07) 849-862
- 50 Dubal DB, Yokoyama JS. Longevity gene KLOTHO and Alzheimer disease - a better fate for individuals who carry APOE ε4. JAMA Neurol 2020; 77 (07) 798-800
- 51 Dubal DB, Yokoyama JS, Zhu L. et al. Life extension factor klotho enhances cognition. Cell Rep 2014; 7 (04) 1065-1076
- 52 Neitzel J, Franzmeier N, Rubinski A. et al; Alzheimer's Disease Neuroimaging Initiative (ADNI). KL-VS heterozygosity is associated with lower amyloid-dependent tau accumulation and memory impairment in Alzheimer's disease. Nat Commun 2021; 12 (01) 3825
- 53 Symposia—Oral Communications—Late Breaking News. J Prev Alzheimers Dis 2021; 8: S1-S72
- 54 Blumenthal JA, Smith PJ, Mabe S. et al. Lifestyle and neurocognition in older adults with cognitive impairments: a randomized trial. Neurology 2019; 92 (03) e212-e223
- 55 Isaacson RS, Hristov H, Saif N. et al. Individualized clinical management of patients at risk for Alzheimer's dementia. Alzheimers Dement 2019; 15 (12) 1588-1602
- 56 Richard E, Van den Heuvel E, Moll van Charante EP. et al. Prevention of dementia by intensive vascular care (PreDIVA): a cluster-randomized trial in progress. Alzheimer Dis Assoc Disord 2009; 23 (03) 198-204
- 57 Vellas B, Carrie I, Gillette-Guyonnet S. et al. MAPT Study: a multidomain approach for preventing Alzheimer's disease: design and baseline data. J Prev Alzheimers Dis 2014; 1 (01) 13-22
- 58 Sink KM, Espeland MA, Castro CM. et al; LIFE Study Investigators. Effect of a 24-month physical activity intervention vs health education on cognitive outcomes in sedentary older adults: the LIFE randomized trial. JAMA 2015; 314 (08) 781-790
- 59 Schelke MW, Attia P, Palenchar DJ. et al. Mechanisms of risk reduction in the clinical practice of Alzheimer's disease prevention. Front Aging Neurosci 2018; 10: 96-96
- 60 Han J-Y, Han S-H. Primary prevention of Alzheimer's disease: is it an attainable goal?. J Korean Med Sci 2014; 29 (07) 886-892
- 61 Vincent GK, Velkoff VA. The Next Four Decades: The Older Population in the United States: 2010 to 2050. USCB; 2010
- 62 Salat DH, Kaye JA, Janowsky JS. Prefrontal gray and white matter volumes in healthy aging and Alzheimer disease. Arch Neurol 1999; 56 (03) 338-344
- 63 Murman DL. The impact of age on cognition. Semin Hear 2015; 36 (03) 111-121
- 64 Hou Y, Dan X, Babbar M. et al. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol 2019; 15 (10) 565-581
- 65 Xia X, Jiang Q, McDermott J, Han JJ. Aging and Alzheimer's disease: comparison and associations from molecular to system level. Aging Cell 2018; 17 (05) e12802-e12802
- 66 Krstic D, Madhusudan A, Doehner J. et al. Systemic immune challenges trigger and drive Alzheimer-like neuropathology in mice. J Neuroinflammation 2012; 9: 151-151
- 67 Charisis S, Ntanasi E, Yannakoulia M. et al. Diet inflammatory index and dementia incidence: a population-based study. Neurology 2021; 97 (24) e2381-e2391
- 68 Andrew MK, Tierney MC. The puzzle of sex, gender and Alzheimer's disease: Why are women more often affected than men?. Womens Health (Lond) 2018; 14: 1745506518817995
- 69 Brookmeyer R, Gray S, Kawas C. Projections of Alzheimer's disease in the United States and the public health impact of delaying disease onset. Am J Public Health 1998; 88 (09) 1337-1342
- 70 Viña J, Lloret A. Why women have more Alzheimer's disease than men: gender and mitochondrial toxicity of amyloid-β peptide. J Alzheimers Dis 2010; 20 (Suppl. 02) S527-S533
- 71 Carter CL, Resnick EM, Mallampalli M, Kalbarczyk A. Sex and gender differences in Alzheimer's disease: recommendations for future research. J Womens Health (Larchmt) 2012; 21 (10) 1018-1023
- 72 Rahman A, Jackson H, Hristov H. et al. Sex and gender driven modifiers of Alzheimer's: the role for estrogenic control across age, race, medical, and lifestyle risks. Front Aging Neurosci 2019; 11: 315
- 73 Scheyer O, Rahman A, Hristov H. et al. Female sex and Alzheimer's risk: the menopause connection. J Prev Alzheimers Dis 2018; 5 (04) 225-230
- 74 Mosconi L, Rahman A, Diaz I. et al. Increased Alzheimer's risk during the menopause transition: a 3-year longitudinal brain imaging study. PLoS One 2018; 13 (12) e0207885
- 75 Maki PM. Critical window hypothesis of hormone therapy and cognition: a scientific update on clinical studies. Menopause 2013; 20 (06) 695-709
- 76 Brinton RD. Impact of estrogen therapy on Alzheimer's disease: a fork in the road?. CNS Drugs 2004; 18 (07) 405-422
- 77 Vinogradova Y, Dening T, Hippisley-Cox J, Taylor L, Moore M, Coupland C. Use of menopausal hormone therapy and risk of dementia: nested case-control studies using QResearch and CPRD databases. BMJ 2021; 374 (2182): n2182
- 78 Shumaker SA, Legault C, Kuller L. et al; Women's Health Initiative Memory Study. Conjugated equine estrogens and incidence of probable dementia and mild cognitive impairment in postmenopausal women: Women's Health Initiative Memory Study. JAMA 2004; 291 (24) 2947-2958
- 79 Shumaker SA, Legault C, Rapp SR. et al; WHIMS Investigators. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women's Health Initiative Memory Study: a randomized controlled trial. JAMA 2003; 289 (20) 2651-2662
- 80 Henderson VW, St John JA, Hodis HN. et al. Cognitive effects of estradiol after menopause: a randomized trial of the timing hypothesis. Neurology 2016; 87 (07) 699-708
- 81 Song YJ, Li SR, Li XW. et al. The effect of estrogen replacement therapy on Alzheimer's disease and Parkinson's disease in postmenopausal women: a meta-analysis. Front Neurosci 2020; 14: 157
- 82 Zandi PP, Carlson MC, Plassman BL. et al; Cache County Memory Study Investigators. Hormone replacement therapy and incidence of Alzheimer disease in older women: the Cache County Study. JAMA 2002; 288 (17) 2123-2129
- 83 Kantarci K, Lowe VJ, Lesnick TG. et al. Early postmenopausal transdermal 17β-estradiol therapy and amyloid-β deposition. J Alzheimers Dis 2016; 53 (02) 547-556
- 84 LeBlanc ES, Janowsky J, Chan BK, Nelson HD. Hormone replacement therapy and cognition: systematic review and meta-analysis. JAMA 2001; 285 (11) 1489-1499
- 85 Blacher J, Kretz S, Sorbets E, Lelong H, Vallée A, Lopez-Sublet M. [Epidemiology of hypertension: differences between women and men]. Presse Med 2019; 48 (11, Pt 1): 1240-1243
- 86 Hayden KM, Zandi PP, Lyketsos CG. et al; Cache County Investigators. Vascular risk factors for incident Alzheimer disease and vascular dementia: the Cache County study. Alzheimer Dis Assoc Disord 2006; 20 (02) 93-100
- 87 Baker LD, Frank LL, Foster-Schubert K. et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010; 67 (01) 71-79
- 88 Hörder H, Johansson L, Guo X. et al. Midlife cardiovascular fitness and dementia: a 44-year longitudinal population study in women. Neurology 2018; 90 (15) e1298-e1305
- 89 Fallah N, Mitnitski A, Middleton L, Rockwood K. Modeling the impact of sex on how exercise is associated with cognitive changes and death in older Canadians. Neuroepidemiology 2009; 33 (01) 47-54
- 90 Eggermont L, Swaab D, Luiten P, Scherder E. Exercise, cognition and Alzheimer's disease: more is not necessarily better. Neurosci Biobehav Rev 2006; 30 (04) 562-575
- 91 Kwak YS, Um SY, Son TG, Kim DJ. Effect of regular exercise on senile dementia patients. Int J Sports Med 2008; 29 (06) 471-474
- 92 Liu-Ambrose T, Nagamatsu LS, Graf P, Beattie BL, Ashe MC, Handy TC. Resistance training and executive functions: a 12-month randomized controlled trial. Arch Intern Med 2010; 170 (02) 170-178
- 93 Cassilhas RC, Viana VA, Grassmann V. et al. The impact of resistance exercise on the cognitive function of the elderly. Med Sci Sports Exerc 2007; 39 (08) 1401-1407
- 94 Best JR, Chiu BK, Liang Hsu C, Nagamatsu LS, Liu-Ambrose T. Long-term effects of resistance exercise training on cognition and brain volume in older women: results from a randomized controlled trial. J Int Neuropsychol Soc 2015; 21 (10) 745-756
- 95 Weuve J, Kang JH, Manson JE, Breteler MM, Ware JH, Grodstein F. Physical activity, including walking, and cognitive function in older women. JAMA 2004; 292 (12) 1454-1461
- 96 Letenneur L, Launer LJ, Andersen K. et al; EURODEM Incidence Research Group. Education and the risk for Alzheimer's disease: sex makes a difference. EURODEM pooled analyses. Am J Epidemiol 2000; 151 (11) 1064-1071
- 97 Flicker L, Almeida OP, Acres J. et al. Predictors of impaired cognitive function in men over the age of 80 years: results from the Health in Men Study. Age Ageing 2005; 34 (01) 77-80
- 98 Olatunji BO, Kauffman BY, Meltzer S, Davis ML, Smits JA, Powers MB. Cognitive-behavioral therapy for hypochondriasis/health anxiety: a meta-analysis of treatment outcome and moderators. Behav Res Ther 2014; 58: 65-74
- 99 Ihle A, Oris M, Fagot D, Baeriswyl M, Guichard E, Kliegel M. The association of leisure activities in middle adulthood with cognitive performance in old age: the moderating role of educational level. Gerontology 2015; 61 (06) 543-550
- 100 Borenstein AR, Copenhaver CI, Mortimer JA. Early-life risk factors for Alzheimer disease. Alzheimer Dis Assoc Disord 2006; 20 (01) 63-72
- 101 Wilson RS, Begeny CT, Boyle PA, Schneider JA, Bennett DA. Vulnerability to stress, anxiety, and development of dementia in old age. Am J Geriatr Psychiatry 2011; 19 (04) 327-334
- 102 Peavy GM, Lange KL, Salmon DP. et al. The effects of prolonged stress and APOE genotype on memory and cortisol in older adults. Biol Psychiatry 2007; 62 (05) 472-478
- 103 Bromberger JT, Kravitz HM, Chang YF, Cyranowski JM, Brown C, Matthews KA. Major depression during and after the menopausal transition: Study of Women's Health Across the Nation (SWAN). Psychol Med 2011; 41 (09) 1879-1888
- 104 Szoeke CE, Robertson JS, Rowe CC. et al. The Women's Healthy Ageing Project: fertile ground for investigation of healthy participants 'at risk' for dementia. Int Rev Psychiatry 2013; 25 (06) 726-737
- 105 Khalsa DS. Stress, meditation, and Alzheimer's disease prevention: where the evidence stands. J Alzheimers Dis 2015; 48 (01) 1-12
- 106 Khalsa DS, Newberg AB. Spiritual fitness: a new dimension in Alzheimer's disease prevention. J Alzheimers Dis 2021; 80 (02) 505-519
- 107 Salmoirago-Blotcher E, Trivedi D, Dunsiger S. et al. Exploring effects of aerobic exercise and mindfulness training on cognitive function in older adults at risk of dementia: a feasibility, proof-of-concept study. Am J Alzheimers Dis Other Demen 2021;36:15333175211039094
- 108 Ng TKS, Fam J, Feng L. et al. Mindfulness improves inflammatory biomarker levels in older adults with mild cognitive impairment: a randomized controlled trial. Transl Psychiatry 2020; 10 (01) 21-21
- 109 Innes KE, Selfe TK. Meditation as a therapeutic intervention for adults at risk for Alzheimer's disease - potential benefits and underlying mechanisms. Front Psychiatry 2014; 5: 40-40
- 110 Epel ES, Puterman E, Lin J. et al. Meditation and vacation effects have an impact on disease-associated molecular phenotypes. Transl Psychiatry 2016; 6 (08) e880
- 111 Reid LD, Avens FE, Walf AA. Cognitive behavioral therapy (CBT) for preventing Alzheimer's disease. Behav Brain Res 2017; 334: 163-177
- 112 Wegner M, Helmich I, Machado S, Nardi AE, Arias-Carrion O, Budde H. Effects of exercise on anxiety and depression disorders: review of meta- analyses and neurobiological mechanisms. CNS Neurol Disord Drug Targets 2014; 13 (06) 1002-1014
- 113 Hoge EA, Chen MM, Orr E. et al. Loving-Kindness Meditation practice associated with longer telomeres in women. Brain Behav Immun 2013; 32: 159-163
- 114 Saif N, Hristov H, Akiyoshi K. et al. Sex-driven differences in the effectiveness of individualized clinical management of Alzheimer's disease risk. J Prev Alzheimers Dis 2022; 9 (04) 731-742
- 115 Bateman RJ, Aisen PS, De Strooper B. et al. Autosomal-dominant Alzheimer's disease: a review and proposal for the prevention of Alzheimer's disease. Alzheimers Res Ther 2011; 3 (01) 1
- 116 Cruts M, Van Broeckhoven C. Presenilin mutations in Alzheimer's disease. Hum Mutat 1998; 11 (03) 183-190
- 117 St George-Hyslop PH, Haines JL, Farrer LA. et al; FAD Collaborative Study Group. Genetic linkage studies suggest that Alzheimer's disease is not a single homogeneous disorder. Nature 1990; 347 (6289): 194-197
- 118 Winblad B, Amouyel P, Andrieu S. et al. Defeating Alzheimer's disease and other dementias: a priority for European science and society. Lancet Neurol 2016; 15 (05) 455-532
- 119 Khalil YA, Rabès JP, Boileau C, Varret M. APOE gene variants in primary dyslipidemia. Atherosclerosis 2021; 328: 11-22
- 120 Liu C-C, Liu C-C, Kanekiyo T, Xu H, Bu G. Apolipoprotein E and Alzheimer disease: risk, mechanisms and therapy. Nat Rev Neurol 2013; 9 (02) 106-118
- 121 Mahley RW, Rall Jr SC. Apolipoprotein E: far more than a lipid transport protein. Annu Rev Genomics Hum Genet 2000; 1: 507-537
- 122 Lahoz C, Schaefer EJ, Cupples LA. et al. Apolipoprotein E genotype and cardiovascular disease in the Framingham Heart Study. Atherosclerosis 2001; 154 (03) 529-537
- 123 Yassine HN, Finch CE. APOE alleles and diet in brain aging and Alzheimer's disease. Front Aging Neurosci 2020; 12: 150
- 124 Carvalho-Wells AL, Jackson KG, Lockyer S, Lovegrove JA, Minihane AM. APOE genotype influences triglyceride and C-reactive protein responses to altered dietary fat intake in UK adults. Am J Clin Nutr 2012; 96 (06) 1447-1453
- 125 Duong MT, Nasrallah IM, Wolk DA, Chang CCY, Chang T-Y. Cholesterol, atherosclerosis, and APOE in vascular contributions to cognitive impairment and dementia (VCID): potential mechanisms and therapy. Front Aging Neurosci 2021; 13: 647990
- 126 Bennet AM, Di Angelantonio E, Ye Z. et al. Association of apolipoprotein E genotypes with lipid levels and coronary risk. JAMA 2007; 298 (11) 1300-1311
- 127 Granér M, Kahri J, Varpula M. et al. Apolipoprotein E polymorphism is associated with both carotid and coronary atherosclerosis in patients with coronary artery disease. Nutr Metab Cardiovasc Dis 2008; 18 (04) 271-277
- 128 Berkowitz CL, Mosconi L, Rahman A, Scheyer O, Hristov H, Isaacson RS. Clinical application of APOE in Alzheimer's prevention: a precision medicine approach. J Prev Alzheimers Dis 2018; 5 (04) 245-252
- 129 Saif N, Sadek G, Bellara S, Hristov H, Isaacson RS. Brain health & dementia risk reduction. Pract Neurol 2019; 89-104
- 130 Geifman N, Brinton RD, Kennedy RE, Schneider LS, Butte AJ. Evidence for benefit of statins to modify cognitive decline and risk in Alzheimer's disease. Alzheimers Res Ther 2017; 9 (01) 10
- 131 Zhao N, Liu CC, Van Ingelgom AJ. et al. Apolipoprotein E4 impairs neuronal insulin signaling by trapping insulin receptor in the endosomes. Neuron 2017; 96 (01) 115-129.e5
- 132 Kivipelto M, Rovio S, Ngandu T. et al. Apolipoprotein E epsilon4 magnifies lifestyle risks for dementia: a population-based study. J Cell Mol Med 2008; 12 (6B): 2762-2771
- 133 Norwitz NG, Saif N, Ariza IE, Isaacson RS. Precision nutrition for Alzheimer's prevention in ApoE4 carriers. Nutrients 2021; 13 (04) 1362
- 134 Arellanes IC, Choe N, Solomon V. et al. Brain delivery of supplemental docosahexaenoic acid (DHA): a randomized placebo-controlled clinical trial. EBioMedicine 2020; 59: 102883
- 135 Yassine HN, Cordova I, He X. et al. Refining omega-3 supplementation trials in APOE4 carriers for dementia prevention. Alzheimers Dement 2020; 16: e039029
- 136 Nardiello P, Pantano D, Lapucci A, Stefani M, Casamenti F. Diet supplementation with hydroxytyrosol ameliorates brain pathology and restores cognitive functions in a mouse model of amyloid-β deposition. J Alzheimers Dis 2018; 63 (03) 1161-1172
- 137 Abuznait AH, Qosa H, Busnena BA, El Sayed KA, Kaddoumi A. Olive-oil-derived oleocanthal enhances β-amyloid clearance as a potential neuroprotective mechanism against Alzheimer's disease: in vitro and in vivo studies. ACS Chem Neurosci 2013; 4 (06) 973-982
- 138 Monti MC, Margarucci L, Tosco A, Riccio R, Casapullo A. New insights on the interaction mechanism between tau protein and oleocanthal, an extra-virgin olive-oil bioactive component. Food Funct 2011; 2 (07) 423-428
- 139 Daccache A, Lion C, Sibille N. et al. Oleuropein and derivatives from olives as tau aggregation inhibitors. Neurochem Int 2011; 58 (06) 700-707
- 140 Norton S, Matthews FE, Barnes DE, Yaffe K, Brayne C. Potential for primary prevention of Alzheimer's disease: an analysis of population-based data. Lancet Neurol 2014; 13 (08) 788-794
- 141 Maddock J, Cavadino A, Power C, Hyppönen E. 25-Hydroxyvitamin D, APOE ɛ4 genotype and cognitive function: findings from the 1958 British birth cohort. Eur J Clin Nutr 2015; 69 (04) 505-508
- 142 Aridi YS, Walker JL, Wright ORL. The Association between the Mediterranean dietary pattern and cognitive health: a systematic review. Nutrients 2017; 9 (07) 674
- 143 Samadi M, Moradi S, Moradinazar M, Mostafai R, Pasdar Y. Dietary pattern in relation to the risk of Alzheimer's disease: a systematic review. Neurol Sci 2019; 40 (10) 2031-2043
- 144 Bartochowski Z, Conway J, Wallach Y, Chakkamparambil B, Alakkassery S, Grossberg GT. Dietary interventions to prevent or delay Alzheimer's disease: what the evidence shows. Curr Nutr Rep 2020; 9 (03) 210-225
- 145 Cherian L, Wang Y, Fakuda K, Leurgans S, Aggarwal N, Morris M. Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) diet slows cognitive decline after stroke. J Prev Alzheimers Dis 2019; 6 (04) 267-273
- 146 Taylor MK, Sullivan DK, Swerdlow RH. et al. A high-glycemic diet is associated with cerebral amyloid burden in cognitively normal older adults. Am J Clin Nutr 2017; 106 (06) 1463-1470
- 147 Morris MC, Tangney CC. Dietary fat composition and dementia risk. Neurobiol Aging 2014; 35 (Suppl. 02) S59-S64
- 148 Zielińska MA, Białecka A, Pietruszka B, Hamułka J. Vegetables and fruit, as a source of bioactive substances, and impact on memory and cognitive function of elderly. Postepy Hig Med Dosw 2017; 71 (00) 267-280
- 149 Shinto L. Eating seafood and cognitive decline in older adults. Neurology 2016; 86 (22) e231-e233
- 150 Berti V, Walters M, Sterling J. et al. Mediterranean diet and 3-year Alzheimer brain biomarker changes in middle-aged adults. Neurology 2018; 90 (20) e1789-e1798
- 151 Scarmeas N, Stern Y, Mayeux R, Manly JJ, Schupf N, Luchsinger JA. Mediterranean diet and mild cognitive impairment. Arch Neurol 2009; 66 (02) 216-225
- 152 Wu L, Sun D. Adherence to Mediterranean diet and risk of developing cognitive disorders: An updated systematic review and meta-analysis of prospective cohort studies. Sci Rep 2017; 7: 41317-41317
- 153 Xie G, Zhou Q, Qiu CZ. et al. Ketogenic diet poses a significant effect on imbalanced gut microbiota in infants with refractory epilepsy. World J Gastroenterol 2017; 23 (33) 6164-6171
- 154 Ota M, Matsuo J, Ishida I. et al. Effect of a ketogenic meal on cognitive function in elderly adults: potential for cognitive enhancement. Psychopharmacology (Berl) 2016; 233 (21-22): 3797-3802
- 155 Alirezaei M, Kemball CC, Flynn CT, Wood MR, Whitton JL, Kiosses WB. Short-term fasting induces profound neuronal autophagy. Autophagy 2010; 6 (06) 702-710
- 156 Jamshed H, Beyl RA, Della Manna DL, Yang ES, Ravussin E, Peterson CM. Early time-restricted feeding improves 24-hour glucose levels and affects markers of the circadian clock, aging, and autophagy in humans. Nutrients 2019; 11 (06) 1234
- 157 Hu Y, Yang Y, Zhang M, Deng M, Zhang JJ. Intermittent fasting pretreatment prevents cognitive impairment in a rat model of chronic cerebral hypoperfusion. J Nutr 2017; 147 (07) 1437-1445
- 158 Hu Y, Zhang M, Chen Y, Yang Y, Zhang JJ. Postoperative intermittent fasting prevents hippocampal oxidative stress and memory deficits in a rat model of chronic cerebral hypoperfusion. Eur J Nutr 2019; 58 (01) 423-432
- 159 Schafer MJ, Dolgalev I, Alldred MJ, Heguy A, Ginsberg SD. Calorie restriction suppresses age-dependent hippocampal transcriptional signatures. PLoS One 2015; 10 (07) e0133923
- 160 Corley BT, Carroll RW, Hall RM, Weatherall M, Parry-Strong A, Krebs JD. Intermittent fasting in Type 2 diabetes mellitus and the risk of hypoglycaemia: a randomized controlled trial. Diabet Med 2018; 35 (05) 588-594
- 161 Qin B, Xun P, Jacobs Jr DR. et al. Intake of niacin, folate, vitamin B-6, and vitamin B-12 through young adulthood and cognitive function in midlife: the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Clin Nutr 2017; 106 (04) 1032-1040
- 162 Román GC. MTHFR gene mutations: a potential marker of late-onset Alzheimer's disease?. J Alzheimers Dis 2015; 47 (02) 323-327
- 163 Schelke MW, Hackett K, Chen JL. et al. Nutritional interventions for Alzheimer's prevention: a clinical precision medicine approach. Ann N Y Acad Sci 2016; 1367 (01) 50-56
- 164 Velazquez R, Ferreira E, Knowles S. et al. Lifelong choline supplementation ameliorates Alzheimer's disease pathology and associated cognitive deficits by attenuating microglia activation. Aging Cell 2019; 18 (06) e13037
- 165 Ballaz SJ, Rebec GV. Neurobiology of vitamin C: expanding the focus from antioxidant to endogenous neuromodulator. Pharmacol Res 2019; 146: 104321
- 166 Masaki KH, Losonczy KG, Izmirlian G. et al. Association of vitamin E and C supplement use with cognitive function and dementia in elderly men. Neurology 2000; 54 (06) 1265-1272
- 167 Banerjee A, Khemka VK, Ganguly A, Roy D, Ganguly U, Chakrabarti S. Vitamin D and Alzheimer's disease: neurocognition to therapeutics. Int J Alzheimers Dis 2015; 2015: 192747
- 168 Wu A, Ying Z, Gomez-Pinilla F. Docosahexaenoic acid dietary supplementation enhances the effects of exercise on synaptic plasticity and cognition. Neuroscience 2008; 155 (03) 751-759
- 169 Barry AR, Dixon DL. Omega-3 fatty acids for the prevention of atherosclerotic cardiovascular disease. Pharmacotherapy 2021; 41 (12) 1056-1065
- 170 Doshi R, Majmundar M, Kumar A, Patel K, Vallabhajosyula S, Kalra A. Association of new-onset atrial fibrillation in patients taking high-dose fish oil. Eur J Intern Med 2021; 94: 110-111
- 171 Mecocci P, Boccardi V, Cecchetti R. et al. A long journey into aging, brain aging, and Alzheimer's disease following the oxidative stress tracks. J Alzheimers Dis 2018; 62 (03) 1319-1335
- 172 Holland TM, Agarwal P, Wang Y. et al. Dietary flavonols and risk of Alzheimer dementia. Neurology 2020; 94 (16) e1749-e1756
- 173 Mastroiacovo D, Kwik-Uribe C, Grassi D. et al. Cocoa flavanol consumption improves cognitive function, blood pressure control, and metabolic profile in elderly subjects: the Cocoa, Cognition, and Aging (CoCoA) study – a randomized controlled trial. Am J Clin Nutr 2015; 101 (03) 538-548
- 174 Brickman AM, Khan UA, Provenzano FA. et al. Enhancing dentate gyrus function with dietary flavanols improves cognition in older adults. Nat Neurosci 2014; 17 (12) 1798-1803
- 175 Sansone R, Rodriguez-Mateos A, Heuel J. et al; Flaviola Consortium, European Union 7th Framework Program. Cocoa flavanol intake improves endothelial function and Framingham Risk Score in healthy men and women: a randomised, controlled, double-masked trial: the Flaviola Health Study. Br J Nutr 2015; 114 (08) 1246-1255
- 176 Davison K, Coates AM, Buckley JD, Howe PR. Effect of cocoa flavanols and exercise on cardiometabolic risk factors in overweight and obese subjects. Int J Obes 2008; 32 (08) 1289-1296
- 177 Sansone R, Ottaviani JI, Rodriguez-Mateos A. et al. Methylxanthines enhance the effects of cocoa flavanols on cardiovascular function: randomized, double-masked controlled studies. Am J Clin Nutr 2017; 105 (02) 352-360
- 178 Fisher ND, Hughes M, Gerhard-Herman M, Hollenberg NK. Flavanol-rich cocoa induces nitric-oxide-dependent vasodilation in healthy humans. J Hypertens 2003; 21 (12) 2281-2286
- 179 Heiss C, Kleinbongard P, Dejam A. et al. Acute consumption of flavanol-rich cocoa and the reversal of endothelial dysfunction in smokers. J Am Coll Cardiol 2005; 46 (07) 1276-1283
- 180 Fisher ND, Hollenberg NK. Aging and vascular responses to flavanol-rich cocoa. J Hypertens 2006; 24 (08) 1575-1580
- 181 Desideri G, Kwik-Uribe C, Grassi D. et al. Benefits in cognitive function, blood pressure, and insulin resistance through cocoa flavanol consumption in elderly subjects with mild cognitive impairment: the Cocoa, Cognition, and Aging (CoCoA) study. Hypertension 2012; 60 (03) 794-801
- 182 Voulgaropoulou SD, van Amelsvoort TAMJ, Prickaerts J, Vingerhoets C. The effect of curcumin on cognition in Alzheimer's disease and healthy aging: a systematic review of pre-clinical and clinical studies. Brain Res 2019; 1725: 146476
- 183 Ghosh S, Banerjee S, Sil PC. The beneficial role of curcumin on inflammation, diabetes and neurodegenerative disease: a recent update. Food Chem Toxicol 2015; 83: 111-124
- 184 Brondino N, Re S, Boldrini A. et al. Curcumin as a therapeutic agent in dementia: a mini systematic review of human studies. ScientificWorldJournal 2014; 2014: 174282
- 185 Mishra S, Palanivelu K. The effect of curcumin (turmeric) on Alzheimer's disease: an overview. Ann Indian Acad Neurol 2008; 11 (01) 13-19
- 186 Anstey KJ, Mack HA, Cherbuin N. Alcohol consumption as a risk factor for dementia and cognitive decline: meta-analysis of prospective studies. Am J Geriatr Psychiatry 2009; 17 (07) 542-555
- 187 Mukamal KJ, Kuller LH, Fitzpatrick AL, Longstreth Jr WT, Mittleman MA, Siscovick DS. Prospective study of alcohol consumption and risk of dementia in older adults. JAMA 2003; 289 (11) 1405-1413
- 188 Luchsinger JA, Tang MX, Siddiqui M, Shea S, Mayeux R. Alcohol intake and risk of dementia. J Am Geriatr Soc 2004; 52 (04) 540-546
- 189 Schwarzinger M, Pollock BG, Hasan OSM, Dufouil C, Rehm J. QalyDays Study Group. Contribution of alcohol use disorders to the burden of dementia in France 2008-13: a nationwide retrospective cohort study. Lancet Public Health 2018; 3 (03) e124-e132
- 190 Anttila T, Helkala EL, Viitanen M. et al. Alcohol drinking in middle age and subsequent risk of mild cognitive impairment and dementia in old age: a prospective population based study. BMJ 2004; 329 (7465): 539
- 191 Sabia S, Fayosse A, Dumurgier J. et al. Alcohol consumption and risk of dementia: 23 year follow-up of Whitehall II cohort study. BMJ 2018; 362: k2927
- 192 Brini S, Sohrabi HR, Peiffer JJ. et al. Physical activity in preventing Alzheimer's disease and cognitive decline: a narrative review. Sports Med 2018; 48 (01) 29-44
- 193 Ito S. High-intensity interval training for health benefits and care of cardiac diseases - The key to an efficient exercise protocol. World J Cardiol 2019; 11 (07) 171-188
- 194 Weston M, Taylor KL, Batterham AM, Hopkins WG. Effects of low-volume high-intensity interval training (HIT) on fitness in adults: a meta-analysis of controlled and non-controlled trials. Sports Med 2014; 44 (07) 1005-1017
- 195 Tokgöz S, Claassen JAHR. Exercise as potential therapeutic target to modulate Alzheimer's disease pathology in APOE ε4 carriers: a systematic review. Cardiol Ther 2021; 10 (01) 67-88
- 196 Racil G, Ben Ounis O, Hammouda O. et al. Effects of high vs. moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Eur J Appl Physiol 2013; 113 (10) 2531-2540
- 197 Søgaard D, Lund MT, Scheuer CM. et al. High-intensity interval training improves insulin sensitivity in older individuals. Acta Physiol (Oxf) 2018; 222 (04) e13009
- 198 Elliott AD, Rajopadhyaya K, Bentley DJ, Beltrame JF, Aromataris EC. Interval training versus continuous exercise in patients with coronary artery disease: a meta-analysis. Heart Lung Circ 2015; 24 (02) 149-157
- 199 Garber CE, Blissmer B, Deschenes MR. et al; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 2011; 43 (07) 1334-1359
- 200 Kodama S, Saito K, Tanaka S. et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA 2009; 301 (19) 2024-2035
- 201 Foster C, Farland CV, Guidotti F. et al. The effects of high intensity interval training vs steady state training on aerobic and anaerobic capacity. J Sports Sci Med 2015; 14 (04) 747-755
- 202 Liou K, Ho S, Fildes J, Ooi SY. High intensity interval versus moderate intensity continuous training in patients with coronary artery disease: a meta-analysis of physiological and clinical parameters. Heart Lung Circ 2016; 25 (02) 166-174
- 203 Luks HJ. Zone 2 Heart Rate Training For Longevity and Performance. 2022 Accessed November 14, 2022 at: https://www.howardluksmd.com/zone-2-hr-training-live-longer-less-injury/
- 204 Liu-Ambrose T, Barha CK, Best JR. Physical activity for brain health in older adults. Appl Physiol Nutr Metab 2018; 43 (11) 1105-1112
- 205 Suo C, Singh MF, Gates N. et al. Therapeutically relevant structural and functional mechanisms triggered by physical and cognitive exercise. Mol Psychiatry 2016; 21 (11) 1633-1642
- 206 Barha CK, Davis JC, Falck RS, Nagamatsu LS, Liu-Ambrose T. Sex differences in exercise efficacy to improve cognition: a systematic review and meta-analysis of randomized controlled trials in older humans. Front Neuroendocrinol 2017; 46: 71-85
- 207 Baumgart M, Snyder HM, Carrillo MC, Fazio S, Kim H, Johns H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: a population-based perspective. Alzheimers Dement 2015; 11 (06) 718-726
- 208 Barnes DE, Yaffe K. The projected effect of risk factor reduction on Alzheimer's disease prevalence. Lancet Neurol 2011; 10 (09) 819-828
- 209 Lennon MJ, Makkar SR, Crawford JD, Sachdev PS. Midlife hypertension and Alzheimer's disease: a systematic review and meta-analysis. J Alzheimers Dis 2019; 71 (01) 307-316
- 210 Hughes TM, Sink KM. Hypertension and its role in cognitive function: current evidence and challenges for the future. Am J Hypertens 2016; 29 (02) 149-157
- 211 Peters R, Warwick J, Anstey KJ, Anderson CS. Blood pressure and dementia: what the SPRINT-MIND trial adds and what we still need to know. Neurology 2019; 92 (21) 1017-1018
- 212 Williamson JD, Pajewski NM, Auchus AP. et al; SPRINT MIND Investigators for the SPRINT Research Group. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA 2019; 321 (06) 553-561
- 213 Nasrallah IM, Gaussoin SA, Pomponio R. et al; SPRINT Research Group. Association of intensive vs standard blood pressure control with magnetic resonance imaging biomarkers of Alzheimer disease: secondary analysis of the SPRINT MIND Randomized Trial. JAMA Neurol 2021; 78 (05) 568-577
- 214 Hajjar I, Okafor M, McDaniel D. et al. Effects of candesartan vs lisinopril on neurocognitive function in older adults with executive mild cognitive impairment: a randomized clinical trial. JAMA Netw Open 2020; 3 (08) e2012252-e2012252
- 215 Liu C-H, Sung P-S, Li Y-R. et al. Telmisartan use and risk of dementia in type 2 diabetes patients with hypertension: a population-based cohort study. PLoS Med 2021; 18 (07) e1003707
- 216 Holm H, Ricci F, Di Martino G. et al. Beta-blocker therapy and risk of vascular dementia: a population-based prospective study. Vascul Pharmacol 2020; 125-126: 106649
- 217 Wingo TS, Cutler DJ, Wingo AP. et al. Association of early-onset Alzheimer disease with elevated low-density lipoprotein cholesterol levels and rare genetic coding variants of APOB. JAMA Neurol 2019; 76 (07) 809-817
- 218 Iwagami M, Qizilbash N, Gregson J. et al. Blood cholesterol and risk of dementia in more than 1·8 million people over two decades: a retrospective cohort study. Lancet Healthy Longev 2021; 2 (08) e498-e506
- 219 Feringa FM, van der Kant R. Cholesterol and Alzheimer's disease; from risk genes to pathological effects. Front Aging Neurosci 2021; 13: 690372
- 220 Anstey KJ, Ashby-Mitchell K, Peters R. Updating the evidence on the association between serum cholesterol and risk of late-life dementia: review and meta-analysis. J Alzheimers Dis 2017; 56 (01) 215-228
- 221 Loera-Valencia R, Goikolea J, Parrado-Fernandez C, Merino-Serrais P, Maioli S. Alterations in cholesterol metabolism as a risk factor for developing Alzheimer's disease: potential novel targets for treatment. J Steroid Biochem Mol Biol 2019; 190: 104-114
- 222 Vance JE. Dysregulation of cholesterol balance in the brain: contribution to neurodegenerative diseases. Dis Model Mech 2012; 5 (06) 746-755
- 223 Proitsi P, Kim M, Whiley L. et al. Association of blood lipids with Alzheimer's disease: a comprehensive lipidomics analysis. Alzheimers Dement 2017; 13 (02) 140-151
- 224 Li R, Wang T-J, Lyu P-Y. et al. Effects of plasma lipids and statins on cognitive function. Chin Med J (Engl) 2018; 131 (04) 471-476
- 225 Li X, Song D, Leng SX. Link between type 2 diabetes and Alzheimer's disease: from epidemiology to mechanism and treatment. Clin Interv Aging 2015; 10: 549-560
- 226 Tabassum S, Misrani A, Yang L. Exploiting common aspects of obesity and Alzheimer's disease. Front Hum Neurosci 2020; 14: 602360
- 227 Terzo S, Amato A, Mulè F. From obesity to Alzheimer's disease through insulin resistance. J Diabetes Complications 2021; 35 (11) 108026
- 228 Bendlin BB. Antidiabetic therapies and Alzheimer disease. Dialogues Clin Neurosci 2019; 21 (01) 83-91
- 229 Angevaare MJ, Vonk JMJ, Bertola L. et al. Predictors of incident mild cognitive impairment and its course in a diverse community-based population. Neurology 2022; 98 (01) e15-e26
- 230 Sharp ES, Gatz M. Relationship between education and dementia: an updated systematic review. Alzheimer Dis Assoc Disord 2011; 25 (04) 289-304
- 231 Wada M, Noda Y, Shinagawa S. et al; Alzheimer's Disease Neuroimaging Initiative. Effect of education on Alzheimer's disease-related neuroimaging biomarkers in healthy controls, and participants with mild cognitive impairment and Alzheimer's disease: a cross-sectional study. J Alzheimers Dis 2018; 63 (02) 861-869
- 232 Leggieri M, Thaut MH, Fornazzari L. et al. Music intervention approaches for Alzheimer's disease: a review of the literature. Front Neurosci 2019; 13: 132
- 233 Bae S, Lee S, Harada K. et al. Engagement in lifestyle activities is associated with increased Alzheimer's disease-associated cortical thickness and cognitive performance in older adults. J Clin Med 2020; 9 (05) 1424
- 234 Landau SM, Marks SM, Mormino EC. et al. Association of lifetime cognitive engagement and low β-amyloid deposition. Arch Neurol 2012; 69 (05) 623-629
- 235 Friedler B, Crapser J, McCullough L. One is the deadliest number: the detrimental effects of social isolation on cerebrovascular diseases and cognition. Acta Neuropathol 2015; 129 (04) 493-509
- 236 Huang H, Wang L, Cao M. et al. Isolation housing exacerbates Alzheimer's disease-like pathophysiology in aged APP/PS1 mice. Int J Neuropsychopharmacol 2015; 18 (07) pyu116
- 237 Hsiao YH, Chen PS, Chen SH, Gean PW. The involvement of Cdk5 activator p35 in social isolation-triggered onset of early Alzheimer's disease-related cognitive deficit in the transgenic mice. Neuropsychopharmacology 2011; 36 (09) 1848-1858
- 238 Powell ND, Sloan EK, Bailey MT. et al. Social stress up-regulates inflammatory gene expression in the leukocyte transcriptome via β-adrenergic induction of myelopoiesis. Proc Natl Acad Sci U S A 2013; 110 (41) 16574-16579
- 239 Miranda M, Morici JF, Zanoni MB, Bekinschtein P. Brain-derived neurotrophic factor: a key molecule for memory in the healthy and the pathological brain. Front Cell Neurosci 2019; 13: 363-363
- 240 Anstey KJ, Peters R, Mortby ME. et al. Association of sex differences in dementia risk factors with sex differences in memory decline in a population-based cohort spanning 20-76 years. Sci Rep 2021; 11 (01) 7710
- 241 Murata C, Saito T, Saito M, Kondo K. The association between social support and incident dementia: a 10-year follow-up study in Japan. Int J Environ Res Public Health 2019; 16 (02) 239
- 242 Ruthirakuhan M, Luedke AC, Tam A, Goel A, Kurji A, Garcia A. Use of physical and intellectual activities and socialization in the management of cognitive decline of aging and in dementia: a review. J Aging Res 2012; 2012: 384875-384875
- 243 Cotterell N, Buffel T, Phillipson C. Preventing social isolation in older people. Maturitas 2018; 113: 80-84
- 244 Kaufman Y. Stress, Memory, and Meaning. B'Or Ha'Torah 2012;22;
- 245 Ouanes S, Popp J. High cortisol and the risk of dementia and Alzheimer's disease: a review of the literature. Front Aging Neurosci 2019; 11: 43-43
- 246 Donovan NJ, Hsu DC, Dagley AS. et al. Depressive symptoms and biomarkers of Alzheimer's disease in cognitively normal older adults. J Alzheimers Dis 2015; 46 (01) 63-73
- 247 Peavy GM, Jacobson MW, Salmon DP. et al. The influence of chronic stress on dementia-related diagnostic change in older adults. Alzheimer Dis Assoc Disord 2012; 26 (03) 260-266
- 248 Becker E, Orellana Rios CL, Lahmann C, Rücker G, Bauer J, Boeker M. Anxiety as a risk factor of Alzheimer's disease and vascular dementia. Br J Psychiatry 2018; 213 (05) 654-660
- 249 Johansson L, Guo X, Waern M. et al. Midlife psychological stress and risk of dementia: a 35-year longitudinal population study. Brain 2010; 133 (Pt 8): 2217-2224
- 250 Yaffe K, Vittinghoff E, Lindquist K. et al. Posttraumatic stress disorder and risk of dementia among US veterans. Arch Gen Psychiatry 2010; 67 (06) 608-613
- 251 Rafferty LA, Cawkill PE, Stevelink SAM, Greenberg K, Greenberg N. Dementia, post-traumatic stress disorder and major depressive disorder: a review of the mental health risk factors for dementia in the military veteran population. Psychol Med 2018; 48 (09) 1400-1409
- 252 Fuhrer R, Dufouil C, Dartigues JF. PAQUID Study. Exploring sex differences in the relationship between depressive symptoms and dementia incidence: prospective results from the PAQUID Study. J Am Geriatr Soc 2003; 51 (08) 1055-1063
- 253 Dal Forno G, Palermo MT, Donohue JE, Karagiozis H, Zonderman AB, Kawas CH. Depressive symptoms, sex, and risk for Alzheimer's disease. Ann Neurol 2005; 57 (03) 381-387
- 254 Burke SL, Cadet T, Alcide A, O'Driscoll J, Maramaldi P. Psychosocial risk factors and Alzheimer's disease: the associative effect of depression, sleep disturbance, and anxiety. Aging Ment Health 2018; 22 (12) 1577-1584
- 255 Dafsari FS, Jessen F. Depression - an underrecognized target for prevention of dementia in Alzheimer's disease. Transl Psychiatry 2020; 10 (01) 160
- 256 Cirrito JR, Wallace CE, Yan P. et al. Effect of escitalopram on Aβ levels and plaque load in an Alzheimer mouse model. Neurology 2020; 95 (19) e2666-e2674
- 257 Hüttenrauch M, Lopez-Noguerola JS, Castro-Obregón S. Connecting mind-body therapy-mediated effects to pathological features of Alzheimer's disease. J Alzheimers Dis 2021; 82 (s1): S65-S90
- 258 Sumathi R, Umapriya M, Ganesh AS. Meditation Helps to Overcome Alzheimer's? A Review Based on Psychiatric Reasons. Zeichen Journal 2021;7(03)
- 259 Damian AE. Reserve and Mindfulness Meditation: Preventative Therapies for Alzheimer's Disease—An Integrative Review [Psy.D.]. Ann Arbor, CA: Institute of Integral Studies; 2018
- 260 eun Lee G, ho Kim S, chul Jung I, won Kang H. Meditation for Alzheimer's disease: systematic review and meta-analysis. J of Oriental Neuropsychiatry 2019; 30 (03) 237-249
- 261 Fan L, Xu W, Cai Y, Hu Y, Wu C. Sleep duration and the risk of dementia: a systematic review and meta-analysis of prospective cohort studies. J Am Med Dir Assoc 2019; 20 (12) 1480-1487.e5
- 262 Yaffe K, Falvey CM, Hoang T. Connections between sleep and cognition in older adults. Lancet Neurol 2014; 13 (10) 1017-1028
- 263 Westwood AJ, Beiser A, Jain N. et al. Prolonged sleep duration as a marker of early neurodegeneration predicting incident dementia. Neurology 2017; 88 (12) 1172-1179
- 264 Lu Y, Sugawara Y, Zhang S, Tomata Y, Tsuji I. Changes in sleep duration and the risk of incident dementia in the elderly Japanese: the Ohsaki Cohort 2006 Study. Sleep 2018; 41 (10) 41
- 265 Hahn EA, Wang HX, Andel R, Fratiglioni L. A change in sleep pattern may predict Alzheimer disease. Am J Geriatr Psychiatry 2014; 22 (11) 1262-1271
- 266 Lucey BP. It's complicated: the relationship between sleep and Alzheimer's disease in humans. Neurobiol Dis 2020; 144: 105031
- 267 Irwin MR, Vitiello MV. Implications of sleep disturbance and inflammation for Alzheimer's disease dementia. Lancet Neurol 2019; 18 (03) 296-306
- 268 Wang C, Holtzman DM. Bidirectional relationship between sleep and Alzheimer's disease: role of amyloid, tau, and other factors. Neuropsychopharmacology 2020; 45 (01) 104-120
- 269 Minakawa EN, Wada K, Nagai Y. Sleep disturbance as a potential modifiable risk factor for Alzheimer's disease. Int J Mol Sci 2019; 20 (04) 803
- 270 Mander BA. Local sleep and Alzheimer's disease pathophysiology. Front Neurosci 2020; 14: 525970-525970
- 271 Robbins R, Quan SF, Weaver MD, Bormes G, Barger LK, Czeisler CA. Examining sleep deficiency and disturbance and their risk for incident dementia and all-cause mortality in older adults across 5 years in the United States. Aging (Albany NY) 2021; 13 (03) 3254-3268
- 272 Sabia S, Fayosse A, Dumurgier J. et al. Association of sleep duration in middle and old age with incidence of dementia. Nat Commun 2021; 12 (01) 2289
- 273 Nedergaard M, Goldman SA. Glymphatic failure as a final common pathway to dementia. Science 2020; 370 (6512): 50-56
- 274 Shokri-Kojori E, Wang GJ, Wiers CE. et al. β-Amyloid accumulation in the human brain after one night of sleep deprivation. Proc Natl Acad Sci U S A 2018; 115 (17) 4483-4488
- 275 Ooms S, Overeem S, Besse K, Rikkert MO, Verbeek M, Claassen JA. Effect of 1 night of total sleep deprivation on cerebrospinal fluid β-amyloid 42 in healthy middle-aged men: a randomized clinical trial. JAMA Neurol 2014; 71 (08) 971-977
- 276 Pase MP, Himali JJ, Grima NA. et al. Sleep architecture and the risk of incident dementia in the community. Neurology 2017; 89 (12) 1244-1250
- 277 Erickson KI, Banducci SE, Weinstein AM. et al. The brain-derived neurotrophic factor Val66Met polymorphism moderates an effect of physical activity on working memory performance. Psychol Sci 2013; 24 (09) 1770-1779
- 278 Tseng L-Y, Huang S-T, Peng L-N, Chen L-K, Hsiao F-Y. Benzodiazepines, z-hypnotics, and risk of dementia: special considerations of half-lives and concomitant use. Neurotherapeutics 2020; 17 (01) 156-164
- 279 Gray SL, Anderson ML, Dublin S. et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med 2015; 175 (03) 401-407
- 280 Liguori C, Maestri M, Spanetta M. et al. Sleep-disordered breathing and the risk of Alzheimer's disease. Sleep Med Rev 2021; 55: 101375
- 281 Chang W-P, Liu M-E, Chang W-C. et al. Sleep apnea and the risk of dementia: a population-based 5-year follow-up study in Taiwan. PLoS One 2013; 8 (10) e78655-e78655
- 282 Zacharias HU, Weihs A, Habes M. et al. Association between obstructive sleep apnea and brain white matter hyperintensities in a population-based cohort in Germany. JAMA Netw Open 2021; 4 (10) e2128225-e2128225
- 283 Mitchell BL, Thorp JG, Evans DM, Nyholt DR, Martin NG, Lupton MK. Exploring the genetic relationship between hearing impairment and Alzheimer's disease. Alzheimers Dement (Amst) 2020; 12 (01) e12108
- 284 Zheng Y, Fan S, Liao W, Fang W, Xiao S, Liu J. Hearing impairment and risk of Alzheimer's disease: a meta-analysis of prospective cohort studies. Neurol Sci 2017; 38 (02) 233-239
- 285 Bagheri F, Borhaninejad V, Rashedi V. Alzheimer's disease and hearing loss among older adults: a literature review. Int J Psychol Behav Sci 2018; 8 (05) 77-80
- 286 Sivanandam TM, Thakur MK. Traumatic brain injury: a risk factor for Alzheimer's disease. Neurosci Biobehav Rev 2012; 36 (05) 1376-1381
- 287 Panicio CFT, Maluta H, Salata FL, Brambilla RR, Dominato AAG. Smoking as a triggering factor for Alzheimer's disease: an integrative review. Res, Soc Dev 2020; 9: e4389119971
- 288 Niu H, Qu Y, Li Z. et al. Smoking and risk for Alzheimer disease: a meta-analysis based on both case-control and cohort study. J Nerv Ment Dis 2018; 206 (09) 680-685
- 289 Kamer AR, Craig RG, Niederman R, Fortea J, de Leon MJ. Periodontal disease as a possible cause for Alzheimer's disease. Periodontol 2000 2020; 83 (01) 242-271
- 290 Chen C-K, Wu Y-T, Chang Y-C. Association between chronic periodontitis and the risk of Alzheimer's disease: a retrospective, population-based, matched-cohort study. Alzheimers Res Ther 2017; 9 (01) 56
- 291 Beydoun MA, Beydoun HA, Hossain S, El-Hajj ZW, Weiss J, Zonderman AB. Clinical and bacterial markers of periodontitis and their association with incident all-cause and Alzheimer's disease dementia in a large national survey. J Alzheimers Dis 2020; 75 (01) 157-172
- 292 Kamer AR, Pushalkar S, Gulivindala D. et al. Periodontal dysbiosis associates with reduced CSF Aβ42 in cognitively normal elderly. Alzheimers Dement (Amst) 2021; 13 (01) e12172
- 293 Periodontal Disease [online]. Accessed November 14, 2022 at: https://www.cdc.gov/oralhealth/conditions/periodontal-disease.html
- 294 Abbayya K, Puthanakar NY, Naduwinmani S, Chidambar YS. Association between periodontitis and Alzheimer's disease. N Am J Med Sci 2015; 7 (06) 241-246
- 295 Sadrameli M, Bathini P, Alberi L. Linking mechanisms of periodontitis to Alzheimer's disease. Curr Opin Neurol 2020; 33 (02) 230-238
- 296 Liccardo D, Marzano F, Carraturo F. et al. Potential bidirectional relationship between periodontitis and Alzheimer's disease. Front Physiol 2020; 11: 683
- 297 Choi S, Kim K, Chang J. et al. Association of chronic periodontitis on Alzheimer's disease or vascular dementia. J Am Geriatr Soc 2019; 67 (06) 1234-1239
- 298 Rice AO. Alzheimer's disease and oral-systemic health: bidirectional care integration improving outcomes. Front Oral Health 2021; 2: 674329
- 299 Kraus N. Biological impact of music and software-based auditory training. J Commun Disord 2012; 45 (06) 403-410
- 300 What is precision medicine? [online]. Accessed November 14, 2022 at: https://medlineplus.gov/genetics/understanding/precisionmedicine/definition/
- 301 Ashley EA, Butte AJ, Wheeler MT. et al. Clinical assessment incorporating a personal genome. Lancet 2010; 375 (9725): 1525-1535
- 302 Berg JS, Amendola LM, Eng C. et al; Members of the CSER Actionability and Return of Results Working Group. Processes and preliminary outputs for identification of actionable genes as incidental findings in genomic sequence data in the Clinical Sequencing Exploratory Research Consortium. Genet Med 2013; 15 (11) 860-867
- 303 Burns DK, Chiang C, Welsh-Bohmer KA. et al. The TOMMORROW study: design of an Alzheimer's disease delay-of-onset clinical trial. Alzheimers Dement (N Y) 2019; 5: 661-670
- 304 Cacabelos R. Pharmacogenomics in Alzheimer's disease. Methods Mol Biol 2008; 448: 213-357
- 305 Krissaane I, De Niz C, Gutiérrez-Sacristán A. et al. Scalability and cost-effectiveness analysis of whole genome-wide association studies on Google Cloud Platform and Amazon Web Services. J Am Med Inform Assoc 2020; 27 (09) 1425-1430
- 306 Phil Huber JO. Limitations Persist in Growth of Precision Medicine. 2021 Accessed November 14, 2022 at: https://www.drugtopics.com/view/limitations-persist-in-growth-of-precision-medicine
- 307 Lleó A, Suárez-Calvet M. Race and Alzheimer disease biomarkers: a neglected race. Neurol Genet 2021; 7 (02) e574
- 308 Schindler SE, Cruchaga C, Joseph A. et al. African Americans have differences in CSF soluble TREM2 and associated genetic variants. Neurol Genet 2021; 7 (02) e571
- 309 Vega IE, Cabrera LY, Wygant CM, Velez-Ortiz D, Counts SE. Alzheimer's disease in the Latino community: intersection of genetics and social determinants of health. J Alzheimers Dis 2017; 58 (04) 979-992
- 310 Kalaria RN. The pathology and pathophysiology of vascular dementia. Neuropharmacology 2018; 134 (Pt B): 226-239
- 311 Panegyres PK, Chen H-Y. Differences between early and late onset Alzheimer's disease. Am J Neurodegener Dis 2013; 2 (04) 300-306
- 312 Stoker TB, Greenland JC. eds. Parkinson's Disease: Pathogenesis and Clinical Aspects. Brisbane (AU): Codon Publications Copyright © 2018 Codon Publications; 2018
- 313 Podcasy JL, Epperson CN. Considering sex and gender in Alzheimer disease and other dementias. Dialogues Clin Neurosci 2016; 18 (04) 437-446
- 314 Armstrong MJ, Litvan I, Lang AE. et al. Criteria for the diagnosis of corticobasal degeneration. Neurology 2013; 80 (05) 496-503
- 315 Ruitenberg A, Ott A, van Swieten JC, Hofman A, Breteler MM. Incidence of dementia: does gender make a difference?. Neurobiol Aging 2001; 22 (04) 575-580
- 316 Reekes TH, Higginson CI, Ledbetter CR, Sathivadivel N, Zweig RM, Disbrow EA. Sex specific cognitive differences in Parkinson disease. NPJ Parkinsons Dis 2020; 6: 7
- 317 Park HK, Ilango SD, Litvan I. Environmental risk factors for progressive supranuclear palsy. J Mov Disord 2021; 14 (02) 103-113
- 318 Constantinides VC, Paraskevas GP, Paraskevas PG, Stefanis L, Kapaki E. Corticobasal degeneration and corticobasal syndrome: a review. Clin Park Relat Disord 2019; 1: 66-71
- 319 Graff-Radford J, Yong KXX, Apostolova LG. et al. New insights into atypical Alzheimer's disease in the era of biomarkers. Lancet Neurol 2021; 20 (03) 222-234
- 320 Graham NL, Emery T, Hodges JR. Distinctive cognitive profiles in Alzheimer's disease and subcortical vascular dementia. J Neurol Neurosurg Psychiatry 2004; 75 (01) 61-71
- 321 Joubert S, Gour N, Guedj E. et al. Early-onset and late-onset Alzheimer's disease are associated with distinct patterns of memory impairment. Cortex 2016; 74: 217-232
- 322 Park HK, Choi SH, Park SA. et al. Cognitive profiles and neuropsychiatric symptoms in Korean early-onset Alzheimer's disease patients: a CREDOS study. J Alzheimers Dis 2015; 44 (02) 661-673
- 323 Koedam ELGE, Lauffer V, van der Vlies AE, van der Flier WM, Scheltens P, Pijnenburg YAL. Early-versus late-onset Alzheimer's disease: more than age alone. J Alzheimers Dis 2010; 19 (04) 1401-1408
- 324 Deleon J, Miller BL. Frontotemporal dementia. In: Geschwind DH, Paulson HL, Klein C. eds. Handbook of Clinical Neurology. Elsevier; 2018: 409-430
- 325 Vasilevskaya A, Taghdiri F, Multani N. et al. PET tau imaging and motor impairments differ between corticobasal syndrome and progressive supranuclear palsy with and without Alzheimer's disease biomarkers. Front Neurol 2020; 11: 574
- 326 Gao X, Simon KC, Han J, Schwarzschild MA, Ascherio A. Family history of melanoma and Parkinson disease risk. Neurology 2009; 73 (16) 1286-1291
- 327 Rogalski E, Johnson N, Weintraub S, Mesulam M. Increased frequency of learning disability in patients with primary progressive aphasia and their first-degree relatives. Arch Neurol 2008; 65 (02) 244-248
- 328 Culebras A, Anwar S. Sleep apnea is a risk factor for stroke and vascular dementia. Curr Neurol Neurosci Rep 2018; 18 (08) 53
- 329 Shi L, Chen S-J, Ma M-Y. et al. Sleep disturbances increase the risk of dementia: a systematic review and meta-analysis. Sleep Med Rev 2018; 40: 4-16
- 330 Falgàs N, Walsh CM, Neylan TC, Grinberg LT. Deepen into sleep and wake patterns across Alzheimer's disease phenotypes. Alzheimers Dement 2021; 17 (08) 1403-1406
- 331 Sani TP, Bond RL, Marshall CR. et al. Sleep symptoms in syndromes of frontotemporal dementia and Alzheimer's disease: a proof-of-principle behavioural study. eNeurologicalSci 2019; 17: 100212-100212
- 332 Walsh CM, Ruoff L, Walker K. et al. Sleepless night and day, the plight of progressive supranuclear palsy. Sleep 2017; 40 (11) 40
- 333 Smith EE. Clinical presentations and epidemiology of vascular dementia. Clin Sci (Lond) 2017; 131 (11) 1059-1068
- 334 Tanaka H, Hashimoto M, Fukuhara R. et al. Relationship between dementia severity and behavioural and psychological symptoms in early-onset Alzheimer's disease. Psychogeriatrics 2015; 15 (04) 242-247
- 335 Cheran G, Silverman H, Manoochehri M. et al. Psychiatric symptoms in preclinical behavioural-variant frontotemporal dementia in MAPT mutation carriers. J Neurol Neurosurg Psychiatry 2018; 89 (05) 449-455
- 336 Wittwer JE, Webster KE, Menz HB. A longitudinal study of measures of walking in people with Alzheimer's disease. Gait Posture 2010; 32 (01) 113-117
- 337 Dai MH, Zheng H, Zeng LD, Zhang Y. The genes associated with early-onset Alzheimer's disease. Oncotarget 2017; 9 (19) 15132-15143
- 338 Bandres-Ciga S, Diez-Fairen M, Kim JJ, Singleton AB. Genetics of Parkinson's disease: an introspection of its journey towards precision medicine. Neurobiol Dis 2020; 137: 104782
- 339 Greaves CV, Rohrer JD. An update on genetic frontotemporal dementia. J Neurol 2019; 266 (08) 2075-2086
- 340 Sha SJ, Boxer A. Treatment implications of C9ORF72. Alzheimers Res Ther 2012; 4 (06) 46-46
- 341 Richardson JR, Roy A, Shalat SL. et al. Elevated serum pesticide levels and risk for Alzheimer disease. JAMA Neurol 2014; 71 (03) 284-290
- 342 Perez-Lasierra JL, Casajús JA, Casasnovas JA. et al. Can physical activity reduce the risk of cognitive decline in apolipoprotein e4 carriers? A systematic review. Int J Environ Res Public Health 2021; 18 (14) 7238
- 343 Macaron T, Giudici KV, Bowman GL. et al. Associations of omega-3 fatty acids with brain morphology and volume in cognitively healthy older adults: a narrative review. Ageing Res Rev 2021; 67: 101300
- 344 Jernerén F, Elshorbagy AK, Oulhaj A, Smith SM, Refsum H, Smith AD. Brain atrophy in cognitively impaired elderly: the importance of long-chain ω-3 fatty acids and B vitamin status in a randomized controlled trial. Am J Clin Nutr 2015; 102 (01) 215-221
- 345 Annweiler C, Llewellyn DJ, Beauchet O. Low serum vitamin D concentrations in Alzheimer's disease: a systematic review and meta-analysis. J Alzheimers Dis 2013; 33 (03) 659-674
- 346 Annweiler C, Montero-Odasso M, Llewellyn DJ, Richard-Devantoy S, Duque G, Beauchet O. Meta-analysis of memory and executive dysfunctions in relation to vitamin D. J Alzheimers Dis 2013; 37 (01) 147-171
- 347 Smith AD, Smith SM, de Jager CA. et al. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One 2010; 5 (09) e12244
- 348 Price BR, Wilcock DM, Weekman EM. Hyperhomocysteinemia as a risk factor for vascular contributions to cognitive impairment and dementia. Front Aging Neurosci 2018; 10: 350-350
- 349 Crooks VC, Lubben J, Petitti DB, Little D, Chiu V. Social network, cognitive function, and dementia incidence among elderly women. Am J Public Health 2008; 98 (07) 1221-1227
- 350 Sutin AR, Stephan Y, Luchetti M, Terracciano A. Loneliness and risk of dementia. J Gerontol B Psychol Sci Soc Sci 2020; 75 (07) 1414-1422
- 351 Zebhauser A, Hofmann-Xu L, Baumert J. et al. How much does it hurt to be lonely? Mental and physical differences between older men and women in the KORA-Age Study. Int J Geriatr Psychiatry 2014; 29 (03) 245-252
- 352 Kuiper JS, Zuidersma M, Oude Voshaar RC. et al. Social relationships and risk of dementia: a systematic review and meta-analysis of longitudinal cohort studies. Ageing Res Rev 2015; 22: 39-57
- 353 Craig MC, Maki PM, Murphy DGM. The Women's Health Initiative Memory Study: findings and implications for treatment. Lancet Neurol 2005; 4 (03) 190-194
- 354 Yoo JE, Shin DW, Han K. et al. Female reproductive factors and the risk of dementia: a nationwide cohort study. Eur J Neurol 2020; 27 (08) 1448-1458
- 355 Rasgon NL, Geist CL, Kenna HA, Wroolie TE, Williams KE, Silverman DH. Prospective randomized trial to assess effects of continuing hormone therapy on cerebral function in postmenopausal women at risk for dementia. PLoS One 2014; 9 (03) e89095
- 356 Kato ET, Cannon CP, Blazing MA. et al. Efficacy and Safety of Adding Ezetimibe to Statin Therapy Among Women and Men: Insight From IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial). J Am Heart Assoc 2017; 6 (11) 6
- 357 Chu CS, Tseng PT, Stubbs B. et al. Use of statins and the risk of dementia and mild cognitive impairment: A systematic review and meta-analysis. Sci Rep 2018; 8 (01) 5804
- 358 Seliger SL, Siscovick DS, Stehman-Breen CO. et al. Moderate renal impairment and risk of dementia among older adults: the Cardiovascular Health Cognition Study. J Am Soc Nephrol 2004; 15 (07) 1904-1911
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
28. November 2022
© 2022. Thieme. All rights reserved.
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Chin JH, Vora N. The global burden of neurologic diseases. Neurology 2014; 83 (04) 349-351
- 2 Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia: review. JAMA 2019; 322 (16) 1589-1599
- 3 Dementia [online]. Accessed November 14, 2022 at: https://www.who.int/news-room/fact-sheets/detail/dementia
- 4 Hurd MD, Martorell P, Delavande A, Mullen KJ, Langa KM. Monetary costs of dementia in the United States. N Engl J Med 2013; 368 (14) 1326-1334
- 5 Wimo A, Jönsson L, Bond J, Prince M, Winblad B, International AD. Alzheimer Disease International. The worldwide economic impact of dementia 2010. Alzheimers Dement 2013; 9 (01) 1-11.e3
- 6 Wimo A, Guerchet M, Ali G-C. et al. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement 2017; 13 (01) 1-7
- 7 Sosa-Ortiz AL, Acosta-Castillo I, Prince MJ. Epidemiology of dementias and Alzheimer's disease. Arch Med Res 2012; 43 (08) 600-608
- 8 Zucchella C, Sinforiani E, Tamburin S. et al. The multidisciplinary approach to Alzheimer's disease and dementia. A narrative review of non-pharmacological treatment. Front Neurol 2018; 9: 1058
- 9 Cummings J. New approaches to symptomatic treatments for Alzheimer's disease. Mol Neurodegener 2021; 16 (01) 2
- 10 World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines. 2019
- 11 Livingston G, Huntley J, Sommerlad A. et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020; 396 (10248): 413-446
- 12 Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM. Forecasting the global burden of Alzheimer's disease. Alzheimers Dement 2007; 3 (03) 186-191
- 13 Zissimopoulos J, Crimmins E, St Clair P. The value of delaying Alzheimer's disease onset. Forum Health Econ Policy 2014; 18 (01) 25-39
- 14 World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025. 2017
- 15 2021 Alzheimer's disease facts and figures. Alzheimers Dement 2021; 17 (03) 327-406
- 16 Risacher SL, Anderson WH, Charil A. et al; Alzheimer's Disease Neuroimaging Initiative. Alzheimer disease brain atrophy subtypes are associated with cognition and rate of decline. Neurology 2017; 89 (21) 2176-2186
- 17 Ossenkoppele R, Schonhaut DR, Schöll M. et al. Tau PET patterns mirror clinical and neuroanatomical variability in Alzheimer's disease. Brain 2016; 139 (Pt 5): 1551-1567
- 18 Vogel JW, Young AL, Oxtoby NP. et al; Alzheimer's Disease Neuroimaging Initiative. Four distinct trajectories of tau deposition identified in Alzheimer's disease. Nat Med 2021; 27 (05) 871-881
- 19 Ferreira D, Nordberg A, Westman E. Biological subtypes of Alzheimer disease: a systematic review and meta-analysis. Neurology 2020; 94 (10) 436-448
- 20 Seifan A, Isaacson R. The Alzheimer's Prevention Clinic at Weill Cornell Medical College/New York - Presbyterian Hospital: Risk Stratification and Personalized Early Intervention. J Prev Alzheimers Dis 2015; 2 (04) 254-266
- 21 Isaacson RS, Ganzer CA, Hristov H. et al. The clinical practice of risk reduction for Alzheimer's disease: a precision medicine approach. Alzheimers Dement 2018; 14 (12) 1663-1673
- 22 Duong S, Patel T, Chang F. Dementia: what pharmacists need to know. Can Pharm J 2017; 150 (02) 118-129
- 23 Nelson PT, Jicha GA, Kryscio RJ. et al. Low sensitivity in clinical diagnoses of dementia with Lewy bodies. J Neurol 2010; 257 (03) 359-366
- 24 Lindau M, Almkvist O, Kushi J. et al. First symptoms–frontotemporal dementia versus Alzheimer's disease. Dement Geriatr Cogn Disord 2000; 11 (05) 286-293
- 25 Devenney EM, Ahmed RM, Halliday G, Piguet O, Kiernan MC, Hodges JR. Psychiatric disorders in C9orf72 kindreds: study of 1,414 family members. Neurology 2018; 91 (16) e1498-e1507
- 26 Boeve BF, Silber MH, Ferman TJ, Lucas JA, Parisi JE. Association of REM sleep behavior disorder and neurodegenerative disease may reflect an underlying synucleinopathy. Mov Disord 2001; 16 (04) 622-630
- 27 Walker IM, Fullard ME, Morley JF, Duda JE. Olfaction as an early marker of Parkinson's disease and Alzheimer's disease. In: Swaab DF, Buijs RM, Kreier F, Lucassen PJ, Salehi A. eds. Handbook of Clinical Neurology. Elsevier; 2021: 317-329
- 28 Hsu F-C, Yuan M, Bowden DW. et al. Adiposity is inversely associated with hippocampal volume in African Americans and European Americans with diabetes. J Diabetes Complications 2016; 30 (08) 1506-1512
- 29 Power MC, Rawlings A, Sharrett AR. et al. Association of midlife lipids with 20-year cognitive change: a cohort study. Alzheimers Dement 2018; 14 (02) 167-177
- 30 Sniderman A, Langlois M, Cobbaert C. Update on apolipoprotein B. Curr Opin Lipidol 2021; 32 (04) 226-230
- 31 Pencina MJ, Pencina KM, Lloyd-Jones D, Catapano AL, Thanassoulis G, Sniderman AD. The expected 30-year benefits of early versus delayed primary prevention of cardiovascular disease by lipid lowering. Circulation 2020; 142 (09) 827-837
- 32 Slot RER, Van Harten AC, Kester MI. et al. Apolipoprotein A1 in cerebrospinal fluid and plasma and progression to Alzheimer's disease in non-demented elderly. J Alzheimers Dis 2017; 56 (02) 687-697
- 33 Mirza SS, de Bruijn RF, Koudstaal PJ. et al. The N-terminal pro B-type natriuretic peptide, and risk of dementia and cognitive decline: a 10-year follow-up study in the general population. J Neurol Neurosurg Psychiatry 2016; 87 (04) 356-362
- 34 de Nazareth AM. Type 2 diabetes mellitus in the pathophysiology of Alzheimer's disease. Dement Neuropsychol 2017; 11 (02) 105-113
- 35 Takeda S, Sato N, Uchio-Yamada K. et al. Diabetes-accelerated memory dysfunction via cerebrovascular inflammation and Abeta deposition in an Alzheimer mouse model with diabetes. Proc Natl Acad Sci U S A 2010; 107 (15) 7036-7041
- 36 Hackett K, Krikorian R, Giovannetti T. et al. Utility of the NIH Toolbox for assessment of prodromal Alzheimer's disease and dementia. Alzheimers Dement (Amst) 2018; 10: 764-772
- 37 Papp KV, Rentz DM, Orlovsky I, Sperling RA, Mormino EC. Optimizing the preclinical Alzheimer's cognitive composite with semantic processing: The PACC5. Alzheimers Dement (N Y) 2017; 3 (04) 668-677
- 38 Langbaum JB, Ellison NN, Caputo A. et al. The Alzheimer's Prevention Initiative Composite Cognitive Test: a practical measure for tracking cognitive decline in preclinical Alzheimer's disease. Alzheimers Res Ther 2020; 12 (01) 66
- 39 Mollenhauer B, Förstl H, Deuschl G, Storch A, Oertel W, Trenkwalder C. Lewy body and parkinsonian dementia: common, but often misdiagnosed conditions. Dtsch Arztebl Int 2010; 107 (39) 684-691
- 40 Silverberg NB, Ryan LM, Carrillo MC. et al. Assessment of cognition in early dementia. Alzheimers Dement 2011; 7 (03) e60-e76
- 41 Saunders AM, Trowers MK, Shimkets RA. et al. The role of apolipoprotein E in Alzheimer's disease: pharmacogenomic target selection. Biochim Biophys Acta 2000; 1502 (01) 85-94
- 42 Is Alzheimer's Genetic? [online]. Accessed November 14, 2022 at: https://www.alz.org/alzheimers-dementia/what-is-alzheimers/causes-and-risk-factors/genetics
- 43 Wu L, Zhao L. ApoE2 and Alzheimer's disease: time to take a closer look. Neural Regen Res 2016; 11 (03) 412-413
- 44 Scheltens P, De Strooper B, Kivipelto M. et al. Alzheimer's disease. Lancet 2021; 397 (10284): 1577-1590
- 45 Emrani S, Arain HA, DeMarshall C, Nuriel T. APOE4 is associated with cognitive and pathological heterogeneity in patients with Alzheimer's disease: a systematic review. Alzheimers Res Ther 2020; 12 (01) 141
- 46 Carrieri G, Bonafè M, De Luca M. et al. Mitochondrial DNA haplogroups and APOE4 allele are non-independent variables in sporadic Alzheimer's disease. Hum Genet 2001; 108 (03) 194-198
- 47 Erickson CM, Schultz SA, Oh JM. et al. KLOTHO heterozygosity attenuates APOE4-related amyloid burden in preclinical AD. Neurology 2019; 92 (16) e1878-e1889
- 48 Wang Y, Brinton RD. Triad of risk for late onset Alzheimer's: mitochondrial haplotype, APOE genotype and chromosomal sex. Front Aging Neurosci 2016; 8: 232
- 49 Belloy ME, Napolioni V, Han SS, Le Guen Y, Greicius MD. Alzheimer's Disease Neuroimaging Initiative. Association of klotho-VS heterozygosity with risk of Alzheimer disease in individuals who carry APOE4. JAMA Neurol 2020; 77 (07) 849-862
- 50 Dubal DB, Yokoyama JS. Longevity gene KLOTHO and Alzheimer disease - a better fate for individuals who carry APOE ε4. JAMA Neurol 2020; 77 (07) 798-800
- 51 Dubal DB, Yokoyama JS, Zhu L. et al. Life extension factor klotho enhances cognition. Cell Rep 2014; 7 (04) 1065-1076
- 52 Neitzel J, Franzmeier N, Rubinski A. et al; Alzheimer's Disease Neuroimaging Initiative (ADNI). KL-VS heterozygosity is associated with lower amyloid-dependent tau accumulation and memory impairment in Alzheimer's disease. Nat Commun 2021; 12 (01) 3825
- 53 Symposia—Oral Communications—Late Breaking News. J Prev Alzheimers Dis 2021; 8: S1-S72
- 54 Blumenthal JA, Smith PJ, Mabe S. et al. Lifestyle and neurocognition in older adults with cognitive impairments: a randomized trial. Neurology 2019; 92 (03) e212-e223
- 55 Isaacson RS, Hristov H, Saif N. et al. Individualized clinical management of patients at risk for Alzheimer's dementia. Alzheimers Dement 2019; 15 (12) 1588-1602
- 56 Richard E, Van den Heuvel E, Moll van Charante EP. et al. Prevention of dementia by intensive vascular care (PreDIVA): a cluster-randomized trial in progress. Alzheimer Dis Assoc Disord 2009; 23 (03) 198-204
- 57 Vellas B, Carrie I, Gillette-Guyonnet S. et al. MAPT Study: a multidomain approach for preventing Alzheimer's disease: design and baseline data. J Prev Alzheimers Dis 2014; 1 (01) 13-22
- 58 Sink KM, Espeland MA, Castro CM. et al; LIFE Study Investigators. Effect of a 24-month physical activity intervention vs health education on cognitive outcomes in sedentary older adults: the LIFE randomized trial. JAMA 2015; 314 (08) 781-790
- 59 Schelke MW, Attia P, Palenchar DJ. et al. Mechanisms of risk reduction in the clinical practice of Alzheimer's disease prevention. Front Aging Neurosci 2018; 10: 96-96
- 60 Han J-Y, Han S-H. Primary prevention of Alzheimer's disease: is it an attainable goal?. J Korean Med Sci 2014; 29 (07) 886-892
- 61 Vincent GK, Velkoff VA. The Next Four Decades: The Older Population in the United States: 2010 to 2050. USCB; 2010
- 62 Salat DH, Kaye JA, Janowsky JS. Prefrontal gray and white matter volumes in healthy aging and Alzheimer disease. Arch Neurol 1999; 56 (03) 338-344
- 63 Murman DL. The impact of age on cognition. Semin Hear 2015; 36 (03) 111-121
- 64 Hou Y, Dan X, Babbar M. et al. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol 2019; 15 (10) 565-581
- 65 Xia X, Jiang Q, McDermott J, Han JJ. Aging and Alzheimer's disease: comparison and associations from molecular to system level. Aging Cell 2018; 17 (05) e12802-e12802
- 66 Krstic D, Madhusudan A, Doehner J. et al. Systemic immune challenges trigger and drive Alzheimer-like neuropathology in mice. J Neuroinflammation 2012; 9: 151-151
- 67 Charisis S, Ntanasi E, Yannakoulia M. et al. Diet inflammatory index and dementia incidence: a population-based study. Neurology 2021; 97 (24) e2381-e2391
- 68 Andrew MK, Tierney MC. The puzzle of sex, gender and Alzheimer's disease: Why are women more often affected than men?. Womens Health (Lond) 2018; 14: 1745506518817995
- 69 Brookmeyer R, Gray S, Kawas C. Projections of Alzheimer's disease in the United States and the public health impact of delaying disease onset. Am J Public Health 1998; 88 (09) 1337-1342
- 70 Viña J, Lloret A. Why women have more Alzheimer's disease than men: gender and mitochondrial toxicity of amyloid-β peptide. J Alzheimers Dis 2010; 20 (Suppl. 02) S527-S533
- 71 Carter CL, Resnick EM, Mallampalli M, Kalbarczyk A. Sex and gender differences in Alzheimer's disease: recommendations for future research. J Womens Health (Larchmt) 2012; 21 (10) 1018-1023
- 72 Rahman A, Jackson H, Hristov H. et al. Sex and gender driven modifiers of Alzheimer's: the role for estrogenic control across age, race, medical, and lifestyle risks. Front Aging Neurosci 2019; 11: 315
- 73 Scheyer O, Rahman A, Hristov H. et al. Female sex and Alzheimer's risk: the menopause connection. J Prev Alzheimers Dis 2018; 5 (04) 225-230
- 74 Mosconi L, Rahman A, Diaz I. et al. Increased Alzheimer's risk during the menopause transition: a 3-year longitudinal brain imaging study. PLoS One 2018; 13 (12) e0207885
- 75 Maki PM. Critical window hypothesis of hormone therapy and cognition: a scientific update on clinical studies. Menopause 2013; 20 (06) 695-709
- 76 Brinton RD. Impact of estrogen therapy on Alzheimer's disease: a fork in the road?. CNS Drugs 2004; 18 (07) 405-422
- 77 Vinogradova Y, Dening T, Hippisley-Cox J, Taylor L, Moore M, Coupland C. Use of menopausal hormone therapy and risk of dementia: nested case-control studies using QResearch and CPRD databases. BMJ 2021; 374 (2182): n2182
- 78 Shumaker SA, Legault C, Kuller L. et al; Women's Health Initiative Memory Study. Conjugated equine estrogens and incidence of probable dementia and mild cognitive impairment in postmenopausal women: Women's Health Initiative Memory Study. JAMA 2004; 291 (24) 2947-2958
- 79 Shumaker SA, Legault C, Rapp SR. et al; WHIMS Investigators. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women's Health Initiative Memory Study: a randomized controlled trial. JAMA 2003; 289 (20) 2651-2662
- 80 Henderson VW, St John JA, Hodis HN. et al. Cognitive effects of estradiol after menopause: a randomized trial of the timing hypothesis. Neurology 2016; 87 (07) 699-708
- 81 Song YJ, Li SR, Li XW. et al. The effect of estrogen replacement therapy on Alzheimer's disease and Parkinson's disease in postmenopausal women: a meta-analysis. Front Neurosci 2020; 14: 157
- 82 Zandi PP, Carlson MC, Plassman BL. et al; Cache County Memory Study Investigators. Hormone replacement therapy and incidence of Alzheimer disease in older women: the Cache County Study. JAMA 2002; 288 (17) 2123-2129
- 83 Kantarci K, Lowe VJ, Lesnick TG. et al. Early postmenopausal transdermal 17β-estradiol therapy and amyloid-β deposition. J Alzheimers Dis 2016; 53 (02) 547-556
- 84 LeBlanc ES, Janowsky J, Chan BK, Nelson HD. Hormone replacement therapy and cognition: systematic review and meta-analysis. JAMA 2001; 285 (11) 1489-1499
- 85 Blacher J, Kretz S, Sorbets E, Lelong H, Vallée A, Lopez-Sublet M. [Epidemiology of hypertension: differences between women and men]. Presse Med 2019; 48 (11, Pt 1): 1240-1243
- 86 Hayden KM, Zandi PP, Lyketsos CG. et al; Cache County Investigators. Vascular risk factors for incident Alzheimer disease and vascular dementia: the Cache County study. Alzheimer Dis Assoc Disord 2006; 20 (02) 93-100
- 87 Baker LD, Frank LL, Foster-Schubert K. et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010; 67 (01) 71-79
- 88 Hörder H, Johansson L, Guo X. et al. Midlife cardiovascular fitness and dementia: a 44-year longitudinal population study in women. Neurology 2018; 90 (15) e1298-e1305
- 89 Fallah N, Mitnitski A, Middleton L, Rockwood K. Modeling the impact of sex on how exercise is associated with cognitive changes and death in older Canadians. Neuroepidemiology 2009; 33 (01) 47-54
- 90 Eggermont L, Swaab D, Luiten P, Scherder E. Exercise, cognition and Alzheimer's disease: more is not necessarily better. Neurosci Biobehav Rev 2006; 30 (04) 562-575
- 91 Kwak YS, Um SY, Son TG, Kim DJ. Effect of regular exercise on senile dementia patients. Int J Sports Med 2008; 29 (06) 471-474
- 92 Liu-Ambrose T, Nagamatsu LS, Graf P, Beattie BL, Ashe MC, Handy TC. Resistance training and executive functions: a 12-month randomized controlled trial. Arch Intern Med 2010; 170 (02) 170-178
- 93 Cassilhas RC, Viana VA, Grassmann V. et al. The impact of resistance exercise on the cognitive function of the elderly. Med Sci Sports Exerc 2007; 39 (08) 1401-1407
- 94 Best JR, Chiu BK, Liang Hsu C, Nagamatsu LS, Liu-Ambrose T. Long-term effects of resistance exercise training on cognition and brain volume in older women: results from a randomized controlled trial. J Int Neuropsychol Soc 2015; 21 (10) 745-756
- 95 Weuve J, Kang JH, Manson JE, Breteler MM, Ware JH, Grodstein F. Physical activity, including walking, and cognitive function in older women. JAMA 2004; 292 (12) 1454-1461
- 96 Letenneur L, Launer LJ, Andersen K. et al; EURODEM Incidence Research Group. Education and the risk for Alzheimer's disease: sex makes a difference. EURODEM pooled analyses. Am J Epidemiol 2000; 151 (11) 1064-1071
- 97 Flicker L, Almeida OP, Acres J. et al. Predictors of impaired cognitive function in men over the age of 80 years: results from the Health in Men Study. Age Ageing 2005; 34 (01) 77-80
- 98 Olatunji BO, Kauffman BY, Meltzer S, Davis ML, Smits JA, Powers MB. Cognitive-behavioral therapy for hypochondriasis/health anxiety: a meta-analysis of treatment outcome and moderators. Behav Res Ther 2014; 58: 65-74
- 99 Ihle A, Oris M, Fagot D, Baeriswyl M, Guichard E, Kliegel M. The association of leisure activities in middle adulthood with cognitive performance in old age: the moderating role of educational level. Gerontology 2015; 61 (06) 543-550
- 100 Borenstein AR, Copenhaver CI, Mortimer JA. Early-life risk factors for Alzheimer disease. Alzheimer Dis Assoc Disord 2006; 20 (01) 63-72
- 101 Wilson RS, Begeny CT, Boyle PA, Schneider JA, Bennett DA. Vulnerability to stress, anxiety, and development of dementia in old age. Am J Geriatr Psychiatry 2011; 19 (04) 327-334
- 102 Peavy GM, Lange KL, Salmon DP. et al. The effects of prolonged stress and APOE genotype on memory and cortisol in older adults. Biol Psychiatry 2007; 62 (05) 472-478
- 103 Bromberger JT, Kravitz HM, Chang YF, Cyranowski JM, Brown C, Matthews KA. Major depression during and after the menopausal transition: Study of Women's Health Across the Nation (SWAN). Psychol Med 2011; 41 (09) 1879-1888
- 104 Szoeke CE, Robertson JS, Rowe CC. et al. The Women's Healthy Ageing Project: fertile ground for investigation of healthy participants 'at risk' for dementia. Int Rev Psychiatry 2013; 25 (06) 726-737
- 105 Khalsa DS. Stress, meditation, and Alzheimer's disease prevention: where the evidence stands. J Alzheimers Dis 2015; 48 (01) 1-12
- 106 Khalsa DS, Newberg AB. Spiritual fitness: a new dimension in Alzheimer's disease prevention. J Alzheimers Dis 2021; 80 (02) 505-519
- 107 Salmoirago-Blotcher E, Trivedi D, Dunsiger S. et al. Exploring effects of aerobic exercise and mindfulness training on cognitive function in older adults at risk of dementia: a feasibility, proof-of-concept study. Am J Alzheimers Dis Other Demen 2021;36:15333175211039094
- 108 Ng TKS, Fam J, Feng L. et al. Mindfulness improves inflammatory biomarker levels in older adults with mild cognitive impairment: a randomized controlled trial. Transl Psychiatry 2020; 10 (01) 21-21
- 109 Innes KE, Selfe TK. Meditation as a therapeutic intervention for adults at risk for Alzheimer's disease - potential benefits and underlying mechanisms. Front Psychiatry 2014; 5: 40-40
- 110 Epel ES, Puterman E, Lin J. et al. Meditation and vacation effects have an impact on disease-associated molecular phenotypes. Transl Psychiatry 2016; 6 (08) e880
- 111 Reid LD, Avens FE, Walf AA. Cognitive behavioral therapy (CBT) for preventing Alzheimer's disease. Behav Brain Res 2017; 334: 163-177
- 112 Wegner M, Helmich I, Machado S, Nardi AE, Arias-Carrion O, Budde H. Effects of exercise on anxiety and depression disorders: review of meta- analyses and neurobiological mechanisms. CNS Neurol Disord Drug Targets 2014; 13 (06) 1002-1014
- 113 Hoge EA, Chen MM, Orr E. et al. Loving-Kindness Meditation practice associated with longer telomeres in women. Brain Behav Immun 2013; 32: 159-163
- 114 Saif N, Hristov H, Akiyoshi K. et al. Sex-driven differences in the effectiveness of individualized clinical management of Alzheimer's disease risk. J Prev Alzheimers Dis 2022; 9 (04) 731-742
- 115 Bateman RJ, Aisen PS, De Strooper B. et al. Autosomal-dominant Alzheimer's disease: a review and proposal for the prevention of Alzheimer's disease. Alzheimers Res Ther 2011; 3 (01) 1
- 116 Cruts M, Van Broeckhoven C. Presenilin mutations in Alzheimer's disease. Hum Mutat 1998; 11 (03) 183-190
- 117 St George-Hyslop PH, Haines JL, Farrer LA. et al; FAD Collaborative Study Group. Genetic linkage studies suggest that Alzheimer's disease is not a single homogeneous disorder. Nature 1990; 347 (6289): 194-197
- 118 Winblad B, Amouyel P, Andrieu S. et al. Defeating Alzheimer's disease and other dementias: a priority for European science and society. Lancet Neurol 2016; 15 (05) 455-532
- 119 Khalil YA, Rabès JP, Boileau C, Varret M. APOE gene variants in primary dyslipidemia. Atherosclerosis 2021; 328: 11-22
- 120 Liu C-C, Liu C-C, Kanekiyo T, Xu H, Bu G. Apolipoprotein E and Alzheimer disease: risk, mechanisms and therapy. Nat Rev Neurol 2013; 9 (02) 106-118
- 121 Mahley RW, Rall Jr SC. Apolipoprotein E: far more than a lipid transport protein. Annu Rev Genomics Hum Genet 2000; 1: 507-537
- 122 Lahoz C, Schaefer EJ, Cupples LA. et al. Apolipoprotein E genotype and cardiovascular disease in the Framingham Heart Study. Atherosclerosis 2001; 154 (03) 529-537
- 123 Yassine HN, Finch CE. APOE alleles and diet in brain aging and Alzheimer's disease. Front Aging Neurosci 2020; 12: 150
- 124 Carvalho-Wells AL, Jackson KG, Lockyer S, Lovegrove JA, Minihane AM. APOE genotype influences triglyceride and C-reactive protein responses to altered dietary fat intake in UK adults. Am J Clin Nutr 2012; 96 (06) 1447-1453
- 125 Duong MT, Nasrallah IM, Wolk DA, Chang CCY, Chang T-Y. Cholesterol, atherosclerosis, and APOE in vascular contributions to cognitive impairment and dementia (VCID): potential mechanisms and therapy. Front Aging Neurosci 2021; 13: 647990
- 126 Bennet AM, Di Angelantonio E, Ye Z. et al. Association of apolipoprotein E genotypes with lipid levels and coronary risk. JAMA 2007; 298 (11) 1300-1311
- 127 Granér M, Kahri J, Varpula M. et al. Apolipoprotein E polymorphism is associated with both carotid and coronary atherosclerosis in patients with coronary artery disease. Nutr Metab Cardiovasc Dis 2008; 18 (04) 271-277
- 128 Berkowitz CL, Mosconi L, Rahman A, Scheyer O, Hristov H, Isaacson RS. Clinical application of APOE in Alzheimer's prevention: a precision medicine approach. J Prev Alzheimers Dis 2018; 5 (04) 245-252
- 129 Saif N, Sadek G, Bellara S, Hristov H, Isaacson RS. Brain health & dementia risk reduction. Pract Neurol 2019; 89-104
- 130 Geifman N, Brinton RD, Kennedy RE, Schneider LS, Butte AJ. Evidence for benefit of statins to modify cognitive decline and risk in Alzheimer's disease. Alzheimers Res Ther 2017; 9 (01) 10
- 131 Zhao N, Liu CC, Van Ingelgom AJ. et al. Apolipoprotein E4 impairs neuronal insulin signaling by trapping insulin receptor in the endosomes. Neuron 2017; 96 (01) 115-129.e5
- 132 Kivipelto M, Rovio S, Ngandu T. et al. Apolipoprotein E epsilon4 magnifies lifestyle risks for dementia: a population-based study. J Cell Mol Med 2008; 12 (6B): 2762-2771
- 133 Norwitz NG, Saif N, Ariza IE, Isaacson RS. Precision nutrition for Alzheimer's prevention in ApoE4 carriers. Nutrients 2021; 13 (04) 1362
- 134 Arellanes IC, Choe N, Solomon V. et al. Brain delivery of supplemental docosahexaenoic acid (DHA): a randomized placebo-controlled clinical trial. EBioMedicine 2020; 59: 102883
- 135 Yassine HN, Cordova I, He X. et al. Refining omega-3 supplementation trials in APOE4 carriers for dementia prevention. Alzheimers Dement 2020; 16: e039029
- 136 Nardiello P, Pantano D, Lapucci A, Stefani M, Casamenti F. Diet supplementation with hydroxytyrosol ameliorates brain pathology and restores cognitive functions in a mouse model of amyloid-β deposition. J Alzheimers Dis 2018; 63 (03) 1161-1172
- 137 Abuznait AH, Qosa H, Busnena BA, El Sayed KA, Kaddoumi A. Olive-oil-derived oleocanthal enhances β-amyloid clearance as a potential neuroprotective mechanism against Alzheimer's disease: in vitro and in vivo studies. ACS Chem Neurosci 2013; 4 (06) 973-982
- 138 Monti MC, Margarucci L, Tosco A, Riccio R, Casapullo A. New insights on the interaction mechanism between tau protein and oleocanthal, an extra-virgin olive-oil bioactive component. Food Funct 2011; 2 (07) 423-428
- 139 Daccache A, Lion C, Sibille N. et al. Oleuropein and derivatives from olives as tau aggregation inhibitors. Neurochem Int 2011; 58 (06) 700-707
- 140 Norton S, Matthews FE, Barnes DE, Yaffe K, Brayne C. Potential for primary prevention of Alzheimer's disease: an analysis of population-based data. Lancet Neurol 2014; 13 (08) 788-794
- 141 Maddock J, Cavadino A, Power C, Hyppönen E. 25-Hydroxyvitamin D, APOE ɛ4 genotype and cognitive function: findings from the 1958 British birth cohort. Eur J Clin Nutr 2015; 69 (04) 505-508
- 142 Aridi YS, Walker JL, Wright ORL. The Association between the Mediterranean dietary pattern and cognitive health: a systematic review. Nutrients 2017; 9 (07) 674
- 143 Samadi M, Moradi S, Moradinazar M, Mostafai R, Pasdar Y. Dietary pattern in relation to the risk of Alzheimer's disease: a systematic review. Neurol Sci 2019; 40 (10) 2031-2043
- 144 Bartochowski Z, Conway J, Wallach Y, Chakkamparambil B, Alakkassery S, Grossberg GT. Dietary interventions to prevent or delay Alzheimer's disease: what the evidence shows. Curr Nutr Rep 2020; 9 (03) 210-225
- 145 Cherian L, Wang Y, Fakuda K, Leurgans S, Aggarwal N, Morris M. Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) diet slows cognitive decline after stroke. J Prev Alzheimers Dis 2019; 6 (04) 267-273
- 146 Taylor MK, Sullivan DK, Swerdlow RH. et al. A high-glycemic diet is associated with cerebral amyloid burden in cognitively normal older adults. Am J Clin Nutr 2017; 106 (06) 1463-1470
- 147 Morris MC, Tangney CC. Dietary fat composition and dementia risk. Neurobiol Aging 2014; 35 (Suppl. 02) S59-S64
- 148 Zielińska MA, Białecka A, Pietruszka B, Hamułka J. Vegetables and fruit, as a source of bioactive substances, and impact on memory and cognitive function of elderly. Postepy Hig Med Dosw 2017; 71 (00) 267-280
- 149 Shinto L. Eating seafood and cognitive decline in older adults. Neurology 2016; 86 (22) e231-e233
- 150 Berti V, Walters M, Sterling J. et al. Mediterranean diet and 3-year Alzheimer brain biomarker changes in middle-aged adults. Neurology 2018; 90 (20) e1789-e1798
- 151 Scarmeas N, Stern Y, Mayeux R, Manly JJ, Schupf N, Luchsinger JA. Mediterranean diet and mild cognitive impairment. Arch Neurol 2009; 66 (02) 216-225
- 152 Wu L, Sun D. Adherence to Mediterranean diet and risk of developing cognitive disorders: An updated systematic review and meta-analysis of prospective cohort studies. Sci Rep 2017; 7: 41317-41317
- 153 Xie G, Zhou Q, Qiu CZ. et al. Ketogenic diet poses a significant effect on imbalanced gut microbiota in infants with refractory epilepsy. World J Gastroenterol 2017; 23 (33) 6164-6171
- 154 Ota M, Matsuo J, Ishida I. et al. Effect of a ketogenic meal on cognitive function in elderly adults: potential for cognitive enhancement. Psychopharmacology (Berl) 2016; 233 (21-22): 3797-3802
- 155 Alirezaei M, Kemball CC, Flynn CT, Wood MR, Whitton JL, Kiosses WB. Short-term fasting induces profound neuronal autophagy. Autophagy 2010; 6 (06) 702-710
- 156 Jamshed H, Beyl RA, Della Manna DL, Yang ES, Ravussin E, Peterson CM. Early time-restricted feeding improves 24-hour glucose levels and affects markers of the circadian clock, aging, and autophagy in humans. Nutrients 2019; 11 (06) 1234
- 157 Hu Y, Yang Y, Zhang M, Deng M, Zhang JJ. Intermittent fasting pretreatment prevents cognitive impairment in a rat model of chronic cerebral hypoperfusion. J Nutr 2017; 147 (07) 1437-1445
- 158 Hu Y, Zhang M, Chen Y, Yang Y, Zhang JJ. Postoperative intermittent fasting prevents hippocampal oxidative stress and memory deficits in a rat model of chronic cerebral hypoperfusion. Eur J Nutr 2019; 58 (01) 423-432
- 159 Schafer MJ, Dolgalev I, Alldred MJ, Heguy A, Ginsberg SD. Calorie restriction suppresses age-dependent hippocampal transcriptional signatures. PLoS One 2015; 10 (07) e0133923
- 160 Corley BT, Carroll RW, Hall RM, Weatherall M, Parry-Strong A, Krebs JD. Intermittent fasting in Type 2 diabetes mellitus and the risk of hypoglycaemia: a randomized controlled trial. Diabet Med 2018; 35 (05) 588-594
- 161 Qin B, Xun P, Jacobs Jr DR. et al. Intake of niacin, folate, vitamin B-6, and vitamin B-12 through young adulthood and cognitive function in midlife: the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Clin Nutr 2017; 106 (04) 1032-1040
- 162 Román GC. MTHFR gene mutations: a potential marker of late-onset Alzheimer's disease?. J Alzheimers Dis 2015; 47 (02) 323-327
- 163 Schelke MW, Hackett K, Chen JL. et al. Nutritional interventions for Alzheimer's prevention: a clinical precision medicine approach. Ann N Y Acad Sci 2016; 1367 (01) 50-56
- 164 Velazquez R, Ferreira E, Knowles S. et al. Lifelong choline supplementation ameliorates Alzheimer's disease pathology and associated cognitive deficits by attenuating microglia activation. Aging Cell 2019; 18 (06) e13037
- 165 Ballaz SJ, Rebec GV. Neurobiology of vitamin C: expanding the focus from antioxidant to endogenous neuromodulator. Pharmacol Res 2019; 146: 104321
- 166 Masaki KH, Losonczy KG, Izmirlian G. et al. Association of vitamin E and C supplement use with cognitive function and dementia in elderly men. Neurology 2000; 54 (06) 1265-1272
- 167 Banerjee A, Khemka VK, Ganguly A, Roy D, Ganguly U, Chakrabarti S. Vitamin D and Alzheimer's disease: neurocognition to therapeutics. Int J Alzheimers Dis 2015; 2015: 192747
- 168 Wu A, Ying Z, Gomez-Pinilla F. Docosahexaenoic acid dietary supplementation enhances the effects of exercise on synaptic plasticity and cognition. Neuroscience 2008; 155 (03) 751-759
- 169 Barry AR, Dixon DL. Omega-3 fatty acids for the prevention of atherosclerotic cardiovascular disease. Pharmacotherapy 2021; 41 (12) 1056-1065
- 170 Doshi R, Majmundar M, Kumar A, Patel K, Vallabhajosyula S, Kalra A. Association of new-onset atrial fibrillation in patients taking high-dose fish oil. Eur J Intern Med 2021; 94: 110-111
- 171 Mecocci P, Boccardi V, Cecchetti R. et al. A long journey into aging, brain aging, and Alzheimer's disease following the oxidative stress tracks. J Alzheimers Dis 2018; 62 (03) 1319-1335
- 172 Holland TM, Agarwal P, Wang Y. et al. Dietary flavonols and risk of Alzheimer dementia. Neurology 2020; 94 (16) e1749-e1756
- 173 Mastroiacovo D, Kwik-Uribe C, Grassi D. et al. Cocoa flavanol consumption improves cognitive function, blood pressure control, and metabolic profile in elderly subjects: the Cocoa, Cognition, and Aging (CoCoA) study – a randomized controlled trial. Am J Clin Nutr 2015; 101 (03) 538-548
- 174 Brickman AM, Khan UA, Provenzano FA. et al. Enhancing dentate gyrus function with dietary flavanols improves cognition in older adults. Nat Neurosci 2014; 17 (12) 1798-1803
- 175 Sansone R, Rodriguez-Mateos A, Heuel J. et al; Flaviola Consortium, European Union 7th Framework Program. Cocoa flavanol intake improves endothelial function and Framingham Risk Score in healthy men and women: a randomised, controlled, double-masked trial: the Flaviola Health Study. Br J Nutr 2015; 114 (08) 1246-1255
- 176 Davison K, Coates AM, Buckley JD, Howe PR. Effect of cocoa flavanols and exercise on cardiometabolic risk factors in overweight and obese subjects. Int J Obes 2008; 32 (08) 1289-1296
- 177 Sansone R, Ottaviani JI, Rodriguez-Mateos A. et al. Methylxanthines enhance the effects of cocoa flavanols on cardiovascular function: randomized, double-masked controlled studies. Am J Clin Nutr 2017; 105 (02) 352-360
- 178 Fisher ND, Hughes M, Gerhard-Herman M, Hollenberg NK. Flavanol-rich cocoa induces nitric-oxide-dependent vasodilation in healthy humans. J Hypertens 2003; 21 (12) 2281-2286
- 179 Heiss C, Kleinbongard P, Dejam A. et al. Acute consumption of flavanol-rich cocoa and the reversal of endothelial dysfunction in smokers. J Am Coll Cardiol 2005; 46 (07) 1276-1283
- 180 Fisher ND, Hollenberg NK. Aging and vascular responses to flavanol-rich cocoa. J Hypertens 2006; 24 (08) 1575-1580
- 181 Desideri G, Kwik-Uribe C, Grassi D. et al. Benefits in cognitive function, blood pressure, and insulin resistance through cocoa flavanol consumption in elderly subjects with mild cognitive impairment: the Cocoa, Cognition, and Aging (CoCoA) study. Hypertension 2012; 60 (03) 794-801
- 182 Voulgaropoulou SD, van Amelsvoort TAMJ, Prickaerts J, Vingerhoets C. The effect of curcumin on cognition in Alzheimer's disease and healthy aging: a systematic review of pre-clinical and clinical studies. Brain Res 2019; 1725: 146476
- 183 Ghosh S, Banerjee S, Sil PC. The beneficial role of curcumin on inflammation, diabetes and neurodegenerative disease: a recent update. Food Chem Toxicol 2015; 83: 111-124
- 184 Brondino N, Re S, Boldrini A. et al. Curcumin as a therapeutic agent in dementia: a mini systematic review of human studies. ScientificWorldJournal 2014; 2014: 174282
- 185 Mishra S, Palanivelu K. The effect of curcumin (turmeric) on Alzheimer's disease: an overview. Ann Indian Acad Neurol 2008; 11 (01) 13-19
- 186 Anstey KJ, Mack HA, Cherbuin N. Alcohol consumption as a risk factor for dementia and cognitive decline: meta-analysis of prospective studies. Am J Geriatr Psychiatry 2009; 17 (07) 542-555
- 187 Mukamal KJ, Kuller LH, Fitzpatrick AL, Longstreth Jr WT, Mittleman MA, Siscovick DS. Prospective study of alcohol consumption and risk of dementia in older adults. JAMA 2003; 289 (11) 1405-1413
- 188 Luchsinger JA, Tang MX, Siddiqui M, Shea S, Mayeux R. Alcohol intake and risk of dementia. J Am Geriatr Soc 2004; 52 (04) 540-546
- 189 Schwarzinger M, Pollock BG, Hasan OSM, Dufouil C, Rehm J. QalyDays Study Group. Contribution of alcohol use disorders to the burden of dementia in France 2008-13: a nationwide retrospective cohort study. Lancet Public Health 2018; 3 (03) e124-e132
- 190 Anttila T, Helkala EL, Viitanen M. et al. Alcohol drinking in middle age and subsequent risk of mild cognitive impairment and dementia in old age: a prospective population based study. BMJ 2004; 329 (7465): 539
- 191 Sabia S, Fayosse A, Dumurgier J. et al. Alcohol consumption and risk of dementia: 23 year follow-up of Whitehall II cohort study. BMJ 2018; 362: k2927
- 192 Brini S, Sohrabi HR, Peiffer JJ. et al. Physical activity in preventing Alzheimer's disease and cognitive decline: a narrative review. Sports Med 2018; 48 (01) 29-44
- 193 Ito S. High-intensity interval training for health benefits and care of cardiac diseases - The key to an efficient exercise protocol. World J Cardiol 2019; 11 (07) 171-188
- 194 Weston M, Taylor KL, Batterham AM, Hopkins WG. Effects of low-volume high-intensity interval training (HIT) on fitness in adults: a meta-analysis of controlled and non-controlled trials. Sports Med 2014; 44 (07) 1005-1017
- 195 Tokgöz S, Claassen JAHR. Exercise as potential therapeutic target to modulate Alzheimer's disease pathology in APOE ε4 carriers: a systematic review. Cardiol Ther 2021; 10 (01) 67-88
- 196 Racil G, Ben Ounis O, Hammouda O. et al. Effects of high vs. moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Eur J Appl Physiol 2013; 113 (10) 2531-2540
- 197 Søgaard D, Lund MT, Scheuer CM. et al. High-intensity interval training improves insulin sensitivity in older individuals. Acta Physiol (Oxf) 2018; 222 (04) e13009
- 198 Elliott AD, Rajopadhyaya K, Bentley DJ, Beltrame JF, Aromataris EC. Interval training versus continuous exercise in patients with coronary artery disease: a meta-analysis. Heart Lung Circ 2015; 24 (02) 149-157
- 199 Garber CE, Blissmer B, Deschenes MR. et al; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 2011; 43 (07) 1334-1359
- 200 Kodama S, Saito K, Tanaka S. et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA 2009; 301 (19) 2024-2035
- 201 Foster C, Farland CV, Guidotti F. et al. The effects of high intensity interval training vs steady state training on aerobic and anaerobic capacity. J Sports Sci Med 2015; 14 (04) 747-755
- 202 Liou K, Ho S, Fildes J, Ooi SY. High intensity interval versus moderate intensity continuous training in patients with coronary artery disease: a meta-analysis of physiological and clinical parameters. Heart Lung Circ 2016; 25 (02) 166-174
- 203 Luks HJ. Zone 2 Heart Rate Training For Longevity and Performance. 2022 Accessed November 14, 2022 at: https://www.howardluksmd.com/zone-2-hr-training-live-longer-less-injury/
- 204 Liu-Ambrose T, Barha CK, Best JR. Physical activity for brain health in older adults. Appl Physiol Nutr Metab 2018; 43 (11) 1105-1112
- 205 Suo C, Singh MF, Gates N. et al. Therapeutically relevant structural and functional mechanisms triggered by physical and cognitive exercise. Mol Psychiatry 2016; 21 (11) 1633-1642
- 206 Barha CK, Davis JC, Falck RS, Nagamatsu LS, Liu-Ambrose T. Sex differences in exercise efficacy to improve cognition: a systematic review and meta-analysis of randomized controlled trials in older humans. Front Neuroendocrinol 2017; 46: 71-85
- 207 Baumgart M, Snyder HM, Carrillo MC, Fazio S, Kim H, Johns H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: a population-based perspective. Alzheimers Dement 2015; 11 (06) 718-726
- 208 Barnes DE, Yaffe K. The projected effect of risk factor reduction on Alzheimer's disease prevalence. Lancet Neurol 2011; 10 (09) 819-828
- 209 Lennon MJ, Makkar SR, Crawford JD, Sachdev PS. Midlife hypertension and Alzheimer's disease: a systematic review and meta-analysis. J Alzheimers Dis 2019; 71 (01) 307-316
- 210 Hughes TM, Sink KM. Hypertension and its role in cognitive function: current evidence and challenges for the future. Am J Hypertens 2016; 29 (02) 149-157
- 211 Peters R, Warwick J, Anstey KJ, Anderson CS. Blood pressure and dementia: what the SPRINT-MIND trial adds and what we still need to know. Neurology 2019; 92 (21) 1017-1018
- 212 Williamson JD, Pajewski NM, Auchus AP. et al; SPRINT MIND Investigators for the SPRINT Research Group. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA 2019; 321 (06) 553-561
- 213 Nasrallah IM, Gaussoin SA, Pomponio R. et al; SPRINT Research Group. Association of intensive vs standard blood pressure control with magnetic resonance imaging biomarkers of Alzheimer disease: secondary analysis of the SPRINT MIND Randomized Trial. JAMA Neurol 2021; 78 (05) 568-577
- 214 Hajjar I, Okafor M, McDaniel D. et al. Effects of candesartan vs lisinopril on neurocognitive function in older adults with executive mild cognitive impairment: a randomized clinical trial. JAMA Netw Open 2020; 3 (08) e2012252-e2012252
- 215 Liu C-H, Sung P-S, Li Y-R. et al. Telmisartan use and risk of dementia in type 2 diabetes patients with hypertension: a population-based cohort study. PLoS Med 2021; 18 (07) e1003707
- 216 Holm H, Ricci F, Di Martino G. et al. Beta-blocker therapy and risk of vascular dementia: a population-based prospective study. Vascul Pharmacol 2020; 125-126: 106649
- 217 Wingo TS, Cutler DJ, Wingo AP. et al. Association of early-onset Alzheimer disease with elevated low-density lipoprotein cholesterol levels and rare genetic coding variants of APOB. JAMA Neurol 2019; 76 (07) 809-817
- 218 Iwagami M, Qizilbash N, Gregson J. et al. Blood cholesterol and risk of dementia in more than 1·8 million people over two decades: a retrospective cohort study. Lancet Healthy Longev 2021; 2 (08) e498-e506
- 219 Feringa FM, van der Kant R. Cholesterol and Alzheimer's disease; from risk genes to pathological effects. Front Aging Neurosci 2021; 13: 690372
- 220 Anstey KJ, Ashby-Mitchell K, Peters R. Updating the evidence on the association between serum cholesterol and risk of late-life dementia: review and meta-analysis. J Alzheimers Dis 2017; 56 (01) 215-228
- 221 Loera-Valencia R, Goikolea J, Parrado-Fernandez C, Merino-Serrais P, Maioli S. Alterations in cholesterol metabolism as a risk factor for developing Alzheimer's disease: potential novel targets for treatment. J Steroid Biochem Mol Biol 2019; 190: 104-114
- 222 Vance JE. Dysregulation of cholesterol balance in the brain: contribution to neurodegenerative diseases. Dis Model Mech 2012; 5 (06) 746-755
- 223 Proitsi P, Kim M, Whiley L. et al. Association of blood lipids with Alzheimer's disease: a comprehensive lipidomics analysis. Alzheimers Dement 2017; 13 (02) 140-151
- 224 Li R, Wang T-J, Lyu P-Y. et al. Effects of plasma lipids and statins on cognitive function. Chin Med J (Engl) 2018; 131 (04) 471-476
- 225 Li X, Song D, Leng SX. Link between type 2 diabetes and Alzheimer's disease: from epidemiology to mechanism and treatment. Clin Interv Aging 2015; 10: 549-560
- 226 Tabassum S, Misrani A, Yang L. Exploiting common aspects of obesity and Alzheimer's disease. Front Hum Neurosci 2020; 14: 602360
- 227 Terzo S, Amato A, Mulè F. From obesity to Alzheimer's disease through insulin resistance. J Diabetes Complications 2021; 35 (11) 108026
- 228 Bendlin BB. Antidiabetic therapies and Alzheimer disease. Dialogues Clin Neurosci 2019; 21 (01) 83-91
- 229 Angevaare MJ, Vonk JMJ, Bertola L. et al. Predictors of incident mild cognitive impairment and its course in a diverse community-based population. Neurology 2022; 98 (01) e15-e26
- 230 Sharp ES, Gatz M. Relationship between education and dementia: an updated systematic review. Alzheimer Dis Assoc Disord 2011; 25 (04) 289-304
- 231 Wada M, Noda Y, Shinagawa S. et al; Alzheimer's Disease Neuroimaging Initiative. Effect of education on Alzheimer's disease-related neuroimaging biomarkers in healthy controls, and participants with mild cognitive impairment and Alzheimer's disease: a cross-sectional study. J Alzheimers Dis 2018; 63 (02) 861-869
- 232 Leggieri M, Thaut MH, Fornazzari L. et al. Music intervention approaches for Alzheimer's disease: a review of the literature. Front Neurosci 2019; 13: 132
- 233 Bae S, Lee S, Harada K. et al. Engagement in lifestyle activities is associated with increased Alzheimer's disease-associated cortical thickness and cognitive performance in older adults. J Clin Med 2020; 9 (05) 1424
- 234 Landau SM, Marks SM, Mormino EC. et al. Association of lifetime cognitive engagement and low β-amyloid deposition. Arch Neurol 2012; 69 (05) 623-629
- 235 Friedler B, Crapser J, McCullough L. One is the deadliest number: the detrimental effects of social isolation on cerebrovascular diseases and cognition. Acta Neuropathol 2015; 129 (04) 493-509
- 236 Huang H, Wang L, Cao M. et al. Isolation housing exacerbates Alzheimer's disease-like pathophysiology in aged APP/PS1 mice. Int J Neuropsychopharmacol 2015; 18 (07) pyu116
- 237 Hsiao YH, Chen PS, Chen SH, Gean PW. The involvement of Cdk5 activator p35 in social isolation-triggered onset of early Alzheimer's disease-related cognitive deficit in the transgenic mice. Neuropsychopharmacology 2011; 36 (09) 1848-1858
- 238 Powell ND, Sloan EK, Bailey MT. et al. Social stress up-regulates inflammatory gene expression in the leukocyte transcriptome via β-adrenergic induction of myelopoiesis. Proc Natl Acad Sci U S A 2013; 110 (41) 16574-16579
- 239 Miranda M, Morici JF, Zanoni MB, Bekinschtein P. Brain-derived neurotrophic factor: a key molecule for memory in the healthy and the pathological brain. Front Cell Neurosci 2019; 13: 363-363
- 240 Anstey KJ, Peters R, Mortby ME. et al. Association of sex differences in dementia risk factors with sex differences in memory decline in a population-based cohort spanning 20-76 years. Sci Rep 2021; 11 (01) 7710
- 241 Murata C, Saito T, Saito M, Kondo K. The association between social support and incident dementia: a 10-year follow-up study in Japan. Int J Environ Res Public Health 2019; 16 (02) 239
- 242 Ruthirakuhan M, Luedke AC, Tam A, Goel A, Kurji A, Garcia A. Use of physical and intellectual activities and socialization in the management of cognitive decline of aging and in dementia: a review. J Aging Res 2012; 2012: 384875-384875
- 243 Cotterell N, Buffel T, Phillipson C. Preventing social isolation in older people. Maturitas 2018; 113: 80-84
- 244 Kaufman Y. Stress, Memory, and Meaning. B'Or Ha'Torah 2012;22;
- 245 Ouanes S, Popp J. High cortisol and the risk of dementia and Alzheimer's disease: a review of the literature. Front Aging Neurosci 2019; 11: 43-43
- 246 Donovan NJ, Hsu DC, Dagley AS. et al. Depressive symptoms and biomarkers of Alzheimer's disease in cognitively normal older adults. J Alzheimers Dis 2015; 46 (01) 63-73
- 247 Peavy GM, Jacobson MW, Salmon DP. et al. The influence of chronic stress on dementia-related diagnostic change in older adults. Alzheimer Dis Assoc Disord 2012; 26 (03) 260-266
- 248 Becker E, Orellana Rios CL, Lahmann C, Rücker G, Bauer J, Boeker M. Anxiety as a risk factor of Alzheimer's disease and vascular dementia. Br J Psychiatry 2018; 213 (05) 654-660
- 249 Johansson L, Guo X, Waern M. et al. Midlife psychological stress and risk of dementia: a 35-year longitudinal population study. Brain 2010; 133 (Pt 8): 2217-2224
- 250 Yaffe K, Vittinghoff E, Lindquist K. et al. Posttraumatic stress disorder and risk of dementia among US veterans. Arch Gen Psychiatry 2010; 67 (06) 608-613
- 251 Rafferty LA, Cawkill PE, Stevelink SAM, Greenberg K, Greenberg N. Dementia, post-traumatic stress disorder and major depressive disorder: a review of the mental health risk factors for dementia in the military veteran population. Psychol Med 2018; 48 (09) 1400-1409
- 252 Fuhrer R, Dufouil C, Dartigues JF. PAQUID Study. Exploring sex differences in the relationship between depressive symptoms and dementia incidence: prospective results from the PAQUID Study. J Am Geriatr Soc 2003; 51 (08) 1055-1063
- 253 Dal Forno G, Palermo MT, Donohue JE, Karagiozis H, Zonderman AB, Kawas CH. Depressive symptoms, sex, and risk for Alzheimer's disease. Ann Neurol 2005; 57 (03) 381-387
- 254 Burke SL, Cadet T, Alcide A, O'Driscoll J, Maramaldi P. Psychosocial risk factors and Alzheimer's disease: the associative effect of depression, sleep disturbance, and anxiety. Aging Ment Health 2018; 22 (12) 1577-1584
- 255 Dafsari FS, Jessen F. Depression - an underrecognized target for prevention of dementia in Alzheimer's disease. Transl Psychiatry 2020; 10 (01) 160
- 256 Cirrito JR, Wallace CE, Yan P. et al. Effect of escitalopram on Aβ levels and plaque load in an Alzheimer mouse model. Neurology 2020; 95 (19) e2666-e2674
- 257 Hüttenrauch M, Lopez-Noguerola JS, Castro-Obregón S. Connecting mind-body therapy-mediated effects to pathological features of Alzheimer's disease. J Alzheimers Dis 2021; 82 (s1): S65-S90
- 258 Sumathi R, Umapriya M, Ganesh AS. Meditation Helps to Overcome Alzheimer's? A Review Based on Psychiatric Reasons. Zeichen Journal 2021;7(03)
- 259 Damian AE. Reserve and Mindfulness Meditation: Preventative Therapies for Alzheimer's Disease—An Integrative Review [Psy.D.]. Ann Arbor, CA: Institute of Integral Studies; 2018
- 260 eun Lee G, ho Kim S, chul Jung I, won Kang H. Meditation for Alzheimer's disease: systematic review and meta-analysis. J of Oriental Neuropsychiatry 2019; 30 (03) 237-249
- 261 Fan L, Xu W, Cai Y, Hu Y, Wu C. Sleep duration and the risk of dementia: a systematic review and meta-analysis of prospective cohort studies. J Am Med Dir Assoc 2019; 20 (12) 1480-1487.e5
- 262 Yaffe K, Falvey CM, Hoang T. Connections between sleep and cognition in older adults. Lancet Neurol 2014; 13 (10) 1017-1028
- 263 Westwood AJ, Beiser A, Jain N. et al. Prolonged sleep duration as a marker of early neurodegeneration predicting incident dementia. Neurology 2017; 88 (12) 1172-1179
- 264 Lu Y, Sugawara Y, Zhang S, Tomata Y, Tsuji I. Changes in sleep duration and the risk of incident dementia in the elderly Japanese: the Ohsaki Cohort 2006 Study. Sleep 2018; 41 (10) 41
- 265 Hahn EA, Wang HX, Andel R, Fratiglioni L. A change in sleep pattern may predict Alzheimer disease. Am J Geriatr Psychiatry 2014; 22 (11) 1262-1271
- 266 Lucey BP. It's complicated: the relationship between sleep and Alzheimer's disease in humans. Neurobiol Dis 2020; 144: 105031
- 267 Irwin MR, Vitiello MV. Implications of sleep disturbance and inflammation for Alzheimer's disease dementia. Lancet Neurol 2019; 18 (03) 296-306
- 268 Wang C, Holtzman DM. Bidirectional relationship between sleep and Alzheimer's disease: role of amyloid, tau, and other factors. Neuropsychopharmacology 2020; 45 (01) 104-120
- 269 Minakawa EN, Wada K, Nagai Y. Sleep disturbance as a potential modifiable risk factor for Alzheimer's disease. Int J Mol Sci 2019; 20 (04) 803
- 270 Mander BA. Local sleep and Alzheimer's disease pathophysiology. Front Neurosci 2020; 14: 525970-525970
- 271 Robbins R, Quan SF, Weaver MD, Bormes G, Barger LK, Czeisler CA. Examining sleep deficiency and disturbance and their risk for incident dementia and all-cause mortality in older adults across 5 years in the United States. Aging (Albany NY) 2021; 13 (03) 3254-3268
- 272 Sabia S, Fayosse A, Dumurgier J. et al. Association of sleep duration in middle and old age with incidence of dementia. Nat Commun 2021; 12 (01) 2289
- 273 Nedergaard M, Goldman SA. Glymphatic failure as a final common pathway to dementia. Science 2020; 370 (6512): 50-56
- 274 Shokri-Kojori E, Wang GJ, Wiers CE. et al. β-Amyloid accumulation in the human brain after one night of sleep deprivation. Proc Natl Acad Sci U S A 2018; 115 (17) 4483-4488
- 275 Ooms S, Overeem S, Besse K, Rikkert MO, Verbeek M, Claassen JA. Effect of 1 night of total sleep deprivation on cerebrospinal fluid β-amyloid 42 in healthy middle-aged men: a randomized clinical trial. JAMA Neurol 2014; 71 (08) 971-977
- 276 Pase MP, Himali JJ, Grima NA. et al. Sleep architecture and the risk of incident dementia in the community. Neurology 2017; 89 (12) 1244-1250
- 277 Erickson KI, Banducci SE, Weinstein AM. et al. The brain-derived neurotrophic factor Val66Met polymorphism moderates an effect of physical activity on working memory performance. Psychol Sci 2013; 24 (09) 1770-1779
- 278 Tseng L-Y, Huang S-T, Peng L-N, Chen L-K, Hsiao F-Y. Benzodiazepines, z-hypnotics, and risk of dementia: special considerations of half-lives and concomitant use. Neurotherapeutics 2020; 17 (01) 156-164
- 279 Gray SL, Anderson ML, Dublin S. et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med 2015; 175 (03) 401-407
- 280 Liguori C, Maestri M, Spanetta M. et al. Sleep-disordered breathing and the risk of Alzheimer's disease. Sleep Med Rev 2021; 55: 101375
- 281 Chang W-P, Liu M-E, Chang W-C. et al. Sleep apnea and the risk of dementia: a population-based 5-year follow-up study in Taiwan. PLoS One 2013; 8 (10) e78655-e78655
- 282 Zacharias HU, Weihs A, Habes M. et al. Association between obstructive sleep apnea and brain white matter hyperintensities in a population-based cohort in Germany. JAMA Netw Open 2021; 4 (10) e2128225-e2128225
- 283 Mitchell BL, Thorp JG, Evans DM, Nyholt DR, Martin NG, Lupton MK. Exploring the genetic relationship between hearing impairment and Alzheimer's disease. Alzheimers Dement (Amst) 2020; 12 (01) e12108
- 284 Zheng Y, Fan S, Liao W, Fang W, Xiao S, Liu J. Hearing impairment and risk of Alzheimer's disease: a meta-analysis of prospective cohort studies. Neurol Sci 2017; 38 (02) 233-239
- 285 Bagheri F, Borhaninejad V, Rashedi V. Alzheimer's disease and hearing loss among older adults: a literature review. Int J Psychol Behav Sci 2018; 8 (05) 77-80
- 286 Sivanandam TM, Thakur MK. Traumatic brain injury: a risk factor for Alzheimer's disease. Neurosci Biobehav Rev 2012; 36 (05) 1376-1381
- 287 Panicio CFT, Maluta H, Salata FL, Brambilla RR, Dominato AAG. Smoking as a triggering factor for Alzheimer's disease: an integrative review. Res, Soc Dev 2020; 9: e4389119971
- 288 Niu H, Qu Y, Li Z. et al. Smoking and risk for Alzheimer disease: a meta-analysis based on both case-control and cohort study. J Nerv Ment Dis 2018; 206 (09) 680-685
- 289 Kamer AR, Craig RG, Niederman R, Fortea J, de Leon MJ. Periodontal disease as a possible cause for Alzheimer's disease. Periodontol 2000 2020; 83 (01) 242-271
- 290 Chen C-K, Wu Y-T, Chang Y-C. Association between chronic periodontitis and the risk of Alzheimer's disease: a retrospective, population-based, matched-cohort study. Alzheimers Res Ther 2017; 9 (01) 56
- 291 Beydoun MA, Beydoun HA, Hossain S, El-Hajj ZW, Weiss J, Zonderman AB. Clinical and bacterial markers of periodontitis and their association with incident all-cause and Alzheimer's disease dementia in a large national survey. J Alzheimers Dis 2020; 75 (01) 157-172
- 292 Kamer AR, Pushalkar S, Gulivindala D. et al. Periodontal dysbiosis associates with reduced CSF Aβ42 in cognitively normal elderly. Alzheimers Dement (Amst) 2021; 13 (01) e12172
- 293 Periodontal Disease [online]. Accessed November 14, 2022 at: https://www.cdc.gov/oralhealth/conditions/periodontal-disease.html
- 294 Abbayya K, Puthanakar NY, Naduwinmani S, Chidambar YS. Association between periodontitis and Alzheimer's disease. N Am J Med Sci 2015; 7 (06) 241-246
- 295 Sadrameli M, Bathini P, Alberi L. Linking mechanisms of periodontitis to Alzheimer's disease. Curr Opin Neurol 2020; 33 (02) 230-238
- 296 Liccardo D, Marzano F, Carraturo F. et al. Potential bidirectional relationship between periodontitis and Alzheimer's disease. Front Physiol 2020; 11: 683
- 297 Choi S, Kim K, Chang J. et al. Association of chronic periodontitis on Alzheimer's disease or vascular dementia. J Am Geriatr Soc 2019; 67 (06) 1234-1239
- 298 Rice AO. Alzheimer's disease and oral-systemic health: bidirectional care integration improving outcomes. Front Oral Health 2021; 2: 674329
- 299 Kraus N. Biological impact of music and software-based auditory training. J Commun Disord 2012; 45 (06) 403-410
- 300 What is precision medicine? [online]. Accessed November 14, 2022 at: https://medlineplus.gov/genetics/understanding/precisionmedicine/definition/
- 301 Ashley EA, Butte AJ, Wheeler MT. et al. Clinical assessment incorporating a personal genome. Lancet 2010; 375 (9725): 1525-1535
- 302 Berg JS, Amendola LM, Eng C. et al; Members of the CSER Actionability and Return of Results Working Group. Processes and preliminary outputs for identification of actionable genes as incidental findings in genomic sequence data in the Clinical Sequencing Exploratory Research Consortium. Genet Med 2013; 15 (11) 860-867
- 303 Burns DK, Chiang C, Welsh-Bohmer KA. et al. The TOMMORROW study: design of an Alzheimer's disease delay-of-onset clinical trial. Alzheimers Dement (N Y) 2019; 5: 661-670
- 304 Cacabelos R. Pharmacogenomics in Alzheimer's disease. Methods Mol Biol 2008; 448: 213-357
- 305 Krissaane I, De Niz C, Gutiérrez-Sacristán A. et al. Scalability and cost-effectiveness analysis of whole genome-wide association studies on Google Cloud Platform and Amazon Web Services. J Am Med Inform Assoc 2020; 27 (09) 1425-1430
- 306 Phil Huber JO. Limitations Persist in Growth of Precision Medicine. 2021 Accessed November 14, 2022 at: https://www.drugtopics.com/view/limitations-persist-in-growth-of-precision-medicine
- 307 Lleó A, Suárez-Calvet M. Race and Alzheimer disease biomarkers: a neglected race. Neurol Genet 2021; 7 (02) e574
- 308 Schindler SE, Cruchaga C, Joseph A. et al. African Americans have differences in CSF soluble TREM2 and associated genetic variants. Neurol Genet 2021; 7 (02) e571
- 309 Vega IE, Cabrera LY, Wygant CM, Velez-Ortiz D, Counts SE. Alzheimer's disease in the Latino community: intersection of genetics and social determinants of health. J Alzheimers Dis 2017; 58 (04) 979-992
- 310 Kalaria RN. The pathology and pathophysiology of vascular dementia. Neuropharmacology 2018; 134 (Pt B): 226-239
- 311 Panegyres PK, Chen H-Y. Differences between early and late onset Alzheimer's disease. Am J Neurodegener Dis 2013; 2 (04) 300-306
- 312 Stoker TB, Greenland JC. eds. Parkinson's Disease: Pathogenesis and Clinical Aspects. Brisbane (AU): Codon Publications Copyright © 2018 Codon Publications; 2018
- 313 Podcasy JL, Epperson CN. Considering sex and gender in Alzheimer disease and other dementias. Dialogues Clin Neurosci 2016; 18 (04) 437-446
- 314 Armstrong MJ, Litvan I, Lang AE. et al. Criteria for the diagnosis of corticobasal degeneration. Neurology 2013; 80 (05) 496-503
- 315 Ruitenberg A, Ott A, van Swieten JC, Hofman A, Breteler MM. Incidence of dementia: does gender make a difference?. Neurobiol Aging 2001; 22 (04) 575-580
- 316 Reekes TH, Higginson CI, Ledbetter CR, Sathivadivel N, Zweig RM, Disbrow EA. Sex specific cognitive differences in Parkinson disease. NPJ Parkinsons Dis 2020; 6: 7
- 317 Park HK, Ilango SD, Litvan I. Environmental risk factors for progressive supranuclear palsy. J Mov Disord 2021; 14 (02) 103-113
- 318 Constantinides VC, Paraskevas GP, Paraskevas PG, Stefanis L, Kapaki E. Corticobasal degeneration and corticobasal syndrome: a review. Clin Park Relat Disord 2019; 1: 66-71
- 319 Graff-Radford J, Yong KXX, Apostolova LG. et al. New insights into atypical Alzheimer's disease in the era of biomarkers. Lancet Neurol 2021; 20 (03) 222-234
- 320 Graham NL, Emery T, Hodges JR. Distinctive cognitive profiles in Alzheimer's disease and subcortical vascular dementia. J Neurol Neurosurg Psychiatry 2004; 75 (01) 61-71
- 321 Joubert S, Gour N, Guedj E. et al. Early-onset and late-onset Alzheimer's disease are associated with distinct patterns of memory impairment. Cortex 2016; 74: 217-232
- 322 Park HK, Choi SH, Park SA. et al. Cognitive profiles and neuropsychiatric symptoms in Korean early-onset Alzheimer's disease patients: a CREDOS study. J Alzheimers Dis 2015; 44 (02) 661-673
- 323 Koedam ELGE, Lauffer V, van der Vlies AE, van der Flier WM, Scheltens P, Pijnenburg YAL. Early-versus late-onset Alzheimer's disease: more than age alone. J Alzheimers Dis 2010; 19 (04) 1401-1408
- 324 Deleon J, Miller BL. Frontotemporal dementia. In: Geschwind DH, Paulson HL, Klein C. eds. Handbook of Clinical Neurology. Elsevier; 2018: 409-430
- 325 Vasilevskaya A, Taghdiri F, Multani N. et al. PET tau imaging and motor impairments differ between corticobasal syndrome and progressive supranuclear palsy with and without Alzheimer's disease biomarkers. Front Neurol 2020; 11: 574
- 326 Gao X, Simon KC, Han J, Schwarzschild MA, Ascherio A. Family history of melanoma and Parkinson disease risk. Neurology 2009; 73 (16) 1286-1291
- 327 Rogalski E, Johnson N, Weintraub S, Mesulam M. Increased frequency of learning disability in patients with primary progressive aphasia and their first-degree relatives. Arch Neurol 2008; 65 (02) 244-248
- 328 Culebras A, Anwar S. Sleep apnea is a risk factor for stroke and vascular dementia. Curr Neurol Neurosci Rep 2018; 18 (08) 53
- 329 Shi L, Chen S-J, Ma M-Y. et al. Sleep disturbances increase the risk of dementia: a systematic review and meta-analysis. Sleep Med Rev 2018; 40: 4-16
- 330 Falgàs N, Walsh CM, Neylan TC, Grinberg LT. Deepen into sleep and wake patterns across Alzheimer's disease phenotypes. Alzheimers Dement 2021; 17 (08) 1403-1406
- 331 Sani TP, Bond RL, Marshall CR. et al. Sleep symptoms in syndromes of frontotemporal dementia and Alzheimer's disease: a proof-of-principle behavioural study. eNeurologicalSci 2019; 17: 100212-100212
- 332 Walsh CM, Ruoff L, Walker K. et al. Sleepless night and day, the plight of progressive supranuclear palsy. Sleep 2017; 40 (11) 40
- 333 Smith EE. Clinical presentations and epidemiology of vascular dementia. Clin Sci (Lond) 2017; 131 (11) 1059-1068
- 334 Tanaka H, Hashimoto M, Fukuhara R. et al. Relationship between dementia severity and behavioural and psychological symptoms in early-onset Alzheimer's disease. Psychogeriatrics 2015; 15 (04) 242-247
- 335 Cheran G, Silverman H, Manoochehri M. et al. Psychiatric symptoms in preclinical behavioural-variant frontotemporal dementia in MAPT mutation carriers. J Neurol Neurosurg Psychiatry 2018; 89 (05) 449-455
- 336 Wittwer JE, Webster KE, Menz HB. A longitudinal study of measures of walking in people with Alzheimer's disease. Gait Posture 2010; 32 (01) 113-117
- 337 Dai MH, Zheng H, Zeng LD, Zhang Y. The genes associated with early-onset Alzheimer's disease. Oncotarget 2017; 9 (19) 15132-15143
- 338 Bandres-Ciga S, Diez-Fairen M, Kim JJ, Singleton AB. Genetics of Parkinson's disease: an introspection of its journey towards precision medicine. Neurobiol Dis 2020; 137: 104782
- 339 Greaves CV, Rohrer JD. An update on genetic frontotemporal dementia. J Neurol 2019; 266 (08) 2075-2086
- 340 Sha SJ, Boxer A. Treatment implications of C9ORF72. Alzheimers Res Ther 2012; 4 (06) 46-46
- 341 Richardson JR, Roy A, Shalat SL. et al. Elevated serum pesticide levels and risk for Alzheimer disease. JAMA Neurol 2014; 71 (03) 284-290
- 342 Perez-Lasierra JL, Casajús JA, Casasnovas JA. et al. Can physical activity reduce the risk of cognitive decline in apolipoprotein e4 carriers? A systematic review. Int J Environ Res Public Health 2021; 18 (14) 7238
- 343 Macaron T, Giudici KV, Bowman GL. et al. Associations of omega-3 fatty acids with brain morphology and volume in cognitively healthy older adults: a narrative review. Ageing Res Rev 2021; 67: 101300
- 344 Jernerén F, Elshorbagy AK, Oulhaj A, Smith SM, Refsum H, Smith AD. Brain atrophy in cognitively impaired elderly: the importance of long-chain ω-3 fatty acids and B vitamin status in a randomized controlled trial. Am J Clin Nutr 2015; 102 (01) 215-221
- 345 Annweiler C, Llewellyn DJ, Beauchet O. Low serum vitamin D concentrations in Alzheimer's disease: a systematic review and meta-analysis. J Alzheimers Dis 2013; 33 (03) 659-674
- 346 Annweiler C, Montero-Odasso M, Llewellyn DJ, Richard-Devantoy S, Duque G, Beauchet O. Meta-analysis of memory and executive dysfunctions in relation to vitamin D. J Alzheimers Dis 2013; 37 (01) 147-171
- 347 Smith AD, Smith SM, de Jager CA. et al. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One 2010; 5 (09) e12244
- 348 Price BR, Wilcock DM, Weekman EM. Hyperhomocysteinemia as a risk factor for vascular contributions to cognitive impairment and dementia. Front Aging Neurosci 2018; 10: 350-350
- 349 Crooks VC, Lubben J, Petitti DB, Little D, Chiu V. Social network, cognitive function, and dementia incidence among elderly women. Am J Public Health 2008; 98 (07) 1221-1227
- 350 Sutin AR, Stephan Y, Luchetti M, Terracciano A. Loneliness and risk of dementia. J Gerontol B Psychol Sci Soc Sci 2020; 75 (07) 1414-1422
- 351 Zebhauser A, Hofmann-Xu L, Baumert J. et al. How much does it hurt to be lonely? Mental and physical differences between older men and women in the KORA-Age Study. Int J Geriatr Psychiatry 2014; 29 (03) 245-252
- 352 Kuiper JS, Zuidersma M, Oude Voshaar RC. et al. Social relationships and risk of dementia: a systematic review and meta-analysis of longitudinal cohort studies. Ageing Res Rev 2015; 22: 39-57
- 353 Craig MC, Maki PM, Murphy DGM. The Women's Health Initiative Memory Study: findings and implications for treatment. Lancet Neurol 2005; 4 (03) 190-194
- 354 Yoo JE, Shin DW, Han K. et al. Female reproductive factors and the risk of dementia: a nationwide cohort study. Eur J Neurol 2020; 27 (08) 1448-1458
- 355 Rasgon NL, Geist CL, Kenna HA, Wroolie TE, Williams KE, Silverman DH. Prospective randomized trial to assess effects of continuing hormone therapy on cerebral function in postmenopausal women at risk for dementia. PLoS One 2014; 9 (03) e89095
- 356 Kato ET, Cannon CP, Blazing MA. et al. Efficacy and Safety of Adding Ezetimibe to Statin Therapy Among Women and Men: Insight From IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial). J Am Heart Assoc 2017; 6 (11) 6
- 357 Chu CS, Tseng PT, Stubbs B. et al. Use of statins and the risk of dementia and mild cognitive impairment: A systematic review and meta-analysis. Sci Rep 2018; 8 (01) 5804
- 358 Seliger SL, Siscovick DS, Stehman-Breen CO. et al. Moderate renal impairment and risk of dementia among older adults: the Cardiovascular Health Cognition Study. J Am Soc Nephrol 2004; 15 (07) 1904-1911