

Subscribe to RSS
DOI: 10.1055/s-0042-1758682
Treatment Outcomes of Adenoid Cystic Carcinomas of the Head and Neck Region—A Single-Institution Experience
Authors
Funding None.

Abstract

Objectives This study was undertaken to evaluate the characteristics and treatment outcomes of patients with adenoid cystic carcinomas of the head and neck region treated at a tertiary cancer center in south India.
Materials and Methods This was a retrospective study done on patients treated at the institute between 2004 and 2011. Clinicopathological details and treatment outcomes were captured from the treatment records to estimate the treatment outcomes and factors affecting them.
Results There were a total of 140 patients with mean age of presentation of 46 years and a median follow-up of 65 months. The most common single site of presentation was the oral cavity. One-hundred eighteen patients (84.3%) underwent primary surgical resection in which 38% had negative surgical margins. Ninety-nine patients were given adjuvant radiotherapy and 18 patients received radical radiotherapy, mostly for surgically inaccessible and inoperable tumors.
Median time to recurrence and distant metastasis was 37 and 34 months, respectively. The overall survival and disease-free survival estimate using the Kaplan–Meier method were 92.3 and 71.9%, respectively, at 5 years. Surgical removal of the primary tumor and the nodal stage had the most significant impact on the overall survival outcomes of these patients.
Conclusion Surgery remains the most impactful treatment modality in the management of these rare epithelial tumors. The use of adjuvant radiotherapy may help to tackle the issues of perineural spread and inadequate surgical margins in technically difficult sites. Radical radiotherapy also has impressive response rates.
Keywords
Adenoid Cystic Carcinoma of head and neck region - treatment outcomes - role of surgery - adjuvant radiotherapy - radical radiotherapy - factors affecting outcomesIntroduction
Adenoid cystic carcinomas are rare epithelial neoplasms arising from the salivary gland tissues that constitute 4% of all epithelial salivary neoplasms and 1% of all head and neck malignancies.[1] [2] [3]
The entity of adenoid cystic carcinoma was first described in 1853 and 1854 by three Frenchmen (Robin, Lorain, and Laboulbene) in their articles, where the typical cylindrical appearance of the tumor was identified. It was Billroth who later coined the term Cylindroma in 1859 and is often credited with the first reporting of these tumors.[1]
The most common site of origin of this tumor is the minor salivary gland of oral cavity especially the palate and the tongue.[2] [3] They are characteristically slow growing but locally invasive and exhibit neurotropism, that is, the propensity to have perineural spread. Their natural history is characterized by indolent growth and late relapses mainly in the form of systemic relapse and poor long-term survival outcomes.[4]
Most of the published literature on these cancers includes small series or single institution reports. Majority of localized tumors are managed with primary surgical resection. The common occurrence of these tumors in areas where complete surgical resection is difficult and technically demanding makes attainment of negative surgical margins very difficult. The extent and nature of surgery are often dictated by the location of tumor and surgical expertise. The role of radiotherapy, however, is less clear with most centers opting to give postoperative radiation considering the high propensity of local relapse and the mostly theoretical ability of radiotherapy to address perineural spread.
This study was undertaken to evaluate the characteristics and treatment outcomes of patients with this unusual tumor treated at a tertiary cancer center in south India.
Materials and Methods
This is a retrospective study of adenoid cystic carcinoma of the head and neck region, registered at the Institution between 2004 and 2011.This study was approved by the institutional review board. The study population was identified from the institutional database using the International Classification of Diseases codes corresponding to adenoid cystic carcinoma of the various head and neck subsites. The case records of these patients were comprehensively reviewed and demographic, clinicopathological details and treatment outcomes were captured on a structured proforma. No central pathology review at the institution was done for all patients since a significant number of patients had undergone surgery at local hospitals. However, a majority had review of the pathology slides and blocks at the institution. Staging was done based on American Joint Committee on Cancer staging system 7th edition criteria and the original pathology report.
A total of 192 patients had registered with a diagnosis of adenoid cystic carcinoma, out of which only the 140 patients who decided to pursue further treatment at this institution were included in the analysis. The patients whose follow-up details were not available were contacted telephonically or via post and all attempts on updating the follow-up were made. Those patients whose follow-up could not be updated after these measures were censored for statistical analysis.
Statistical Analysis
The continuous variables were summarized using mean and standard deviation and categorical variables were reported using frequencies and percentages. The overall survival (OS) and disease-free survival (DFS) were estimated using Kaplan–Meier method. Survival probabilities obtained by using the Kaplan–Meier method were compared using log-rank test and the risk of various prognostic factors on OS and DFS were estimated using Cox regression analysis. The risk of various prognostic factors on recurrence was estimated using logistic regression. A p-value less than 0.05 is considered to be significant. All estimates were calculated from the date of the pathological diagnosis.
Results
A total of 140 patients with biopsy proven adenoid cystic carcinoma of the head and neck region, treated between 2004 and 2011 were included in this analysis.
Among the 140 of patients, 57.9% were females. Majority of the patients presented in the third and fourth decade of life, with the mean age at presentation being 46.5 years (range: 16–84 years). Among the 15 patients who were diagnosed at age less than 30 years, 7 had disease in one of the major salivary glands.
The demographic details and the disease characteristics of the patients are summarized in [Table 1].
Abbreviation: PNS, paranasal sinus.
Tumor Characteristics and Staging
The most common site of presentation was in one of the major salivary glands (either the parotid or submandibular gland, with a frequency of 29.3% of the total cases), followed by oral cavity (28.6%) and sinonasal subsite (22.9%). The most common single site of tumor presentation was the oral cavity. The rare primary locations of the tumor included the larynx, eye lid, external auditory canal, parapharyngeal location, and lacrimal gland.
Nearly 49% of the patients presented with stage I or II disease. Forty nine (35%) patients had stage IV disease, out of which three had metastatic disease at diagnosis. Regional adenopathy was present in 16 patients (11.4%). Majority of patients of patients with regional adenopathy had the primary tumor in the oral cavity (43%) followed by patients with oropharyngeal primary (18%).
Treatment Characteristics
Surgery
A total of 118 patients (84.3%) underwent primary surgical resection.
Forty-five out of the 118 patients (38%) had negative surgical margins. Among the 66 patients who had positive margins, majority had unplanned excisions from the referring centers and did not have further surgery at our institution or were patients who had a paranasal sinus primary. Further histopathology details including the microscopic pattern and presence of perineural spread were largely unavailable from the records.
Surgery alone was done for 19 patients and more than 80% (16) among them had early-stage disease and margin negative excision (12). Five patients developed recurrence in this subgroup and all were local recurrences. Four out of them had initial margin positive excision and were not given adjuvant radiotherapy for various reasons including patient refusal, and they were successfully salvaged with further surgery with or without radiotherapy.
Radiotherapy
Radiotherapy was used in the treatment of 120 patients. Ninety-nine patients were given radiation in the adjuvant setting. Radical radiotherapy was given to 18 patients who had inoperable disease or in whom surgery was not contemplated due to medical reasons. Adjuvant radiotherapy dose schedules were mostly ranging between 50 and 60 Gy in 2 Gy equivalents and for radical radiotherapy 60 to 70 Gy equivalent schedules were used. Thirteen patients, among those who received radical radiotherapy, had complete response (72.2%) and four patients had partial response at 3 months of radiotherapy completion. One patient was documented to have stable disease at first follow-up. Among the patients who had complete response, nine patients developed recurrences. Three patients had isolated local recurrence, three patients failed in regional nodes alone, and three failed systemically. Among the patients who developed metastatic disease, two also had recurrence at the primary site.
Chemotherapy
None of the patients were given chemotherapy in the neoadjuvant, concurrent or adjuvant setting and the use of chemotherapy was only for palliation in the recurrent/metastatic setting.
Survival Outcomes
The median follow-up period of this study was 65 months (range: 1–150 months).
The median time to recurrence for all patients was 37 months and the median time to distant metastasis was 34 months after completing the initial treatment.
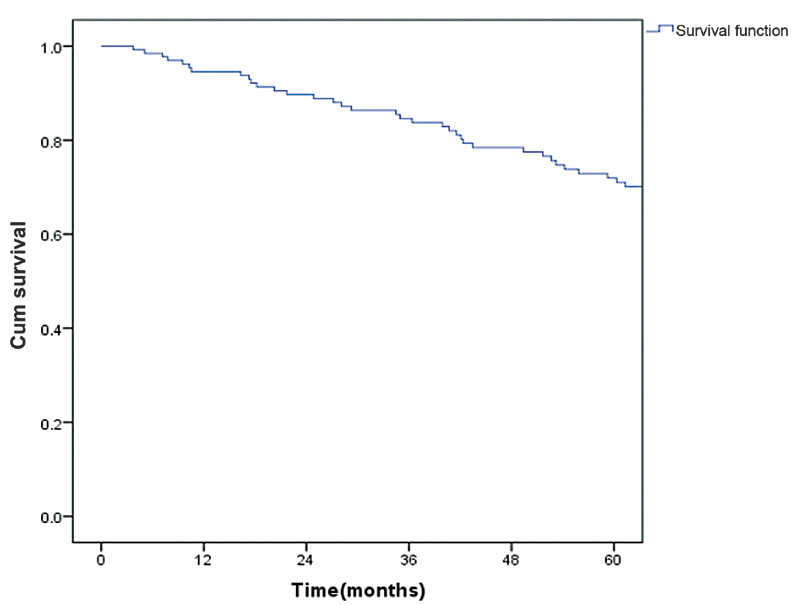
The OS estimate using the Kaplan–Meier method 92.3% at 5 years (standard error [SE]: 2.5%; [Fig. 1]).

The DFS was estimated to be 71.9% at 5 years (SE: 4.2%; [Fig. 2]).
Surgical removal of the primary tumor and the nodal stage had the most significant impact on the OS outcomes of these patients ([Table 2]).
Abbreviations: CI, confidence interval; HR, hazard ratio.
Even though sex of the patient did not have a significant impact on survival, it was observed that female patients did slightly better than the male counterparts in terms of 5 years survival (95.6 vs. 87.5%; p = 0.218). T Stage of tumor, site of primary, and use of radiotherapy were not demonstrated to have any statistically significant impact on the survival outcomes ([Table 2]).
The impact of surgery and nodal stage on OS was maintained on multivariate analysis also (hazard ratio [HR]: 8.36; 95% confidence interval [CI]: 2.33–30.04; p = 0.001 and HR: -5.43; 95% CI: 1.47–20.01 p = 0.011 for surgery and nodal stage, respectively). Surgical removal of tumors, T stage and N stage had the most profound and statistically significant impact on DFS ([Table 3]).
Abbreviations: CI, confidence interval; HR, hazard ratio.
The influence of surgery and nodal staging in survival were maintained in the multivariate analysis also. Impact of the location of the primary tumor on survival outcome was evaluated and no meaningful impact could be demonstrated, even though oral cavity and major salivary gland primaries did slightly better than other sites ([Table 4]).
Abbreviations: PNS, paranasal sinus; SE, standard error; SM, submandibular.
Discussion
The published data on adenoid cystic carcinoma is sparse, mainly since they constitute only approximately 1% of all head and neck malignancies. The management of this tumor has always posed many clinical challenges, considering the long clinical history, initial indolent growth nature along with relentless and progressive clinical course thereafter.
Retrospective reviews and single institution reports constitute most of the available literature on these rare cancers. One of the largest series published so far is the European data of more than 2,000 patients form the EUROCARE database comprising patients from 32 population-based cancer registries from 17 countries across Europe.[5] They have extensively reported on the demographics, clinical presentations, and survival outcomes. Over 40% of patients were more than 60 years of age in this series. In concordance with the EUROCARE data that found a female preponderance of 56%, we have also found that nearly 58% of the patients were females. Most other reviews, however, fail to show any specific sex predilection for these tumors.[6] [7]
Most common site of origin of these rare tumors is the minor salivary gland located within the oral cavity.[8] [9] Oral cavity was the most common single site of origin of these tumors in the present series too, with 28.6% of the patients presenting with a primary in one of the oral cavity subsites. Nearly 50% of patients in this series presented with stage I or II disease and regional node positivity was seen in 11.4% of patients. This stage distribution as well as the node positivity rates are comparable to most other reports where the node positivity rates were found to be typically between 10 and 15%.[1] [8] Majority of the patients with regional adenopathy at presentation had the primary tumor located in the oral cavity. A relatively higher rate of regional node positivity of around 19% for adenoid cystic carcinoma of the oral cavity has been reported by Agarwal et al from Mumbai, India.[10]
Surgery remains the primary management option for most salivary gland carcinomas with the type and extent of surgery depending on various factors like histology, tumor site, regional lymphadenopathy, and expertise of the operating surgeon. More than 80% of patients in this study underwent primary resection of the tumor. More than half (55.8%) of the operated patients had positive surgical margins. Most of these were patients who underwent unplanned excisions at local hospitals and were not subsequently considered for further surgery or had the primary in locations like the paranasal sinus where obtaining negative margins of excision is often difficult. The rates of margin positivity reported in literature are also around 50%, and this is mostly because of the common occurrence of primary tumors in sites with complex anatomical relations and difficult surgical accessibility.[11] [12]
The role of complete surgical excision of adenoid cystic carcinomas of head and neck subsite remains undisputed. However, there has been much debate on the use of postoperative radiotherapy for these tumors, even though most centers prefer to use adjuvant radiotherapy.[10] [11] A few series have tried to look into the benefit of postoperative radiotherapy in the patients who underwent initial excision and the conclusions have been quite variable. Most authors have been equivocal on the role of factors like stage of the tumor, nodal involvement, and presence of perineural invasion in influencing outcomes ([Table 5]).
|
Author |
n |
Outcome |
Statistical inference |
Factors affecting outcome |
|||
|---|---|---|---|---|---|---|---|
|
S alone |
S + PORT |
||||||
|
OS |
LC/DFS |
OS |
LC/DFS |
||||
|
Silverman et al[14] |
75 |
5 years—82.3% 10 years—67.9% |
(LC) 5 years—85.6% 10 years—79.0% |
5 years—79.8% 10 years—60.5% |
(LC) 5 years—84.9% 10 years—71.6% |
No significant difference between two groups |
PORT LC benefit: • T4 stage • Margin + |
|
Kokemueller et al[15] |
74 |
Not reported separately |
No benefit with PORT |
LC • PNI • Tumor size • Margins |
|||
|
Chen et al[12] |
140 |
10 years—65% |
(LC) 5 years—80% 10 years—61% |
10 years—60% |
(LC) 5 years—92% 10 years— 84% |
Significant local control benefit |
LC • T4 stage • PNI • Omission of RT • Major nerve involvement |
|
Gomez et al[11] |
59 |
No surgery group |
5 years—87% 10 years—65% |
(DFS) 5 years—76% 10 years—40% |
DFS: • T4 stage • Gross clinical nerve involvement OS: • N+ • T4 stage |
||
|
Agarwal et al[10] |
76 |
Not analyzed separately 97% underwent surgery; 68.9% had post OP RT |
– |
5 years LC—57.9% 5 years DFS—47.1% |
– |
LC and DFS: • PNI • T-stage • Primary site |
|
|
Present study |
140 |
Not analyzed separately 84.3% underwent primary surgery 84% of operated patients got adjuvant RT |
– |
5 years DFS— 71.9% |
5 years OS—92.3% |
Factors affecting outcome: • Surgery • Stage |
|
Abbreviations: DFS, disease-free survival; LC, local control; n, number of patients; OS, overall survival; PNI, perineural involvement; PORT, postoperative RT; S, surgery.
Of the 118 patients who underwent surgical resection in this study, 99 patients were given postoperative radiotherapy. Surgical excision of tumor was demonstrated to be one of the strongest predictors for OS and DFS ([Tables 2] and [3]) and this underlines the importance of surgical excision in these tumors. We have obtained a 5-year OS estimate of 92.3% and DFS estimate of 71.9% in this series. The OS figures are much higher than most reported series. This disparity could be partly attributed to the fact that more than 80% of patients received adjuvant radiotherapy after surgery irrespective of the tumor stage and post op margins. This could also be a reflection of the poor patient follow-up especially after a few years of completing treatment.
Radical radiotherapy remains a good treatment option for those patients with localized but inoperable disease due to medical reasons, or technical inoperability as a result of the tumor extent and location. Mendenhall et al reported 10-year OS and local control rates of 65 and 75%, respectively, for patients treated with radiation alone for localized salivary gland carcinoma.[11] Chen et al reported 10-year OS and distant metastasis-free rates of 46 and 67%, respectively, for patients with salivary gland carcinomas including a significant proportion of adenoid cystic carcinomas treated at the UCSF University of California, San Francisco Medical Center. Patients with higher T stage and use of radiation dose less than 66 Gy were found to be predictors of poor outcome.[12] A possible dose response relation, especially for adenoid cystic carcinoma, was reported by Parsons et al who reported that use of radiotherapy dose greater than 70 Gy resulted in better outcomes when patients were treated with radiotherapy alone.[12]
Eighteen patients in this series were given radical radiotherapy. The complete response rate among these patients was 72.2%. Radiotherapy dose ranged from 60 to 70 Gy in 2Gy equivalent. This further supports the theory that these tumors might be more radiosensitive than traditionally believed and careful selection of patients, treatment techniques, and radiotherapy dose could result in good treatment results thereby opening more avenues for organ preservation.
The median time to recurrence for all patients in this study was 37 months and the median time to distant metastasis was 34 months after the initial treatment. Majority of the recurrences were either local (14.8%) or systemic with or without local recurrence (14.8%). Gomez et al reported a much larger median time to distant failure of 5.9 years in their series.[11] Improvement in local control with adequate surgery and optimal use of postoperative radiotherapy can in turn lead to higher rates of metastatic disease and this can have an impact on the survival over time.
Surgical excision of tumor and nodal positivity was the only two factors that showed a significant association with survival outcomes in both univariate and multivariate analysis in this study. Although not statistically significant, patients with negative surgical margins did better than those with margin positive excision with 5-year survival of 81.4 versus 71.7% (p = 0.174). The impact of other variables like sex, T stage, and use of radiotherapy was much negligible. The impact of the radiotherapy volume especially the inclusion of the skull base to address the perineural spread of the disease is yet to be addressed. The radiotherapy volume in most of the patients in this series includes treating up to the skull base and nodal irradiation was limited to patients with node positive disease. Various authors have highlighted the predictive role of T4 stage, positive surgical margins, perineural involvement, and use of radiotherapy for local recurrences. Nodal involvement and site of primary lesion have been found to be predictor of poor survival in some series.[10] [11] [13] Perez and Fa'bio, in their large series of 129 patients with adenoid cystic carcinoma of the head and neck region, reported the prognostic role of age (>45 years), period of complaints less than 18 months, presence of paresthesia, T stage, N stage, M stage, composite clinical stage, solid histological subtype, incomplete surgical resection to be predictors of poor survival at 5 and 10 years. They also highlighted the prognostic importance of molecular markers like expressions of p53, Ki-67, PCNA (proliferating cell nuclear antigen), CEA (carcinoembryonic antigen) in predicting lower survival even though these results did not attain the statistical significance.[8]
The superior survival outcomes of adenoid cystic carcinomas localized to the oral cavity and the major salivary glands have been reported in large series like the publications of Ciccolallo et al and Perez and Fa'bio.[8] [9] This superiority can be attributed to the ability to perform complete surgical resections for the tumors arising in these regions and the relative technical ease of these surgeries compared with surgeries for other subsites like the paranasal sinus, laryngopharynx, and other uncommon areas of minor salivary glands. Even though no statistically meaningful impact of the location of the primary tumor could be demonstrated in this study, the adenoid cystic carcinomas arising from the oral cavity and major salivary glands did better than other subsites with less easy surgical access.
Limitations of the Study
This is a retrospective review and well-planned randomized studies may be required to draw conclusions on role of surgery and use of radiotherapy.
This study also has poor rates of follow-up especially beyond 3 years of treatment start and the survival is hence overestimated.
Conclusion
Adenoid cystic carcinomas are rare neoplasms arising from the salivary glands, and are mostly found to arise in the minor salivary glands located in the oral cavity and in the major salivary glands. They have a characteristically prolonged clinical course with initial indolent growth and later punctuated with relapses and metastasis. Surgery remains the main modality of treatment and postoperative radiotherapy may have an important role in attaining good survival outcomes for these patients. Contrary to classical teaching, these tumors may be radiosensitive, and inoperable patients may have good local control and survival with radiotherapy alone, with optimal choice of treatment technique and delivery of adequate tumoricidal dose.
Conflict of Interest
None declared.
-
References
- 1 Billroth T. Observations on tumors of the salivary glands. Arch Path Anat 1859; 17: 357-375
- 2 Jones AS, Beasley NJ, Houghton DJ, Helliwell TR, Husband DJ. Tumours of the minor salivary glands. Clin Otolaryngol Allied Sci 1998; 23 (01) 27-33
- 3 Sultan I, Rodriguez-Galindo C, Al-Sharabati S, Guzzo M, Casanova M, Ferrari A. Salivary gland carcinomas in children and adolescents: a population-based study, with comparison to adult cases. Head Neck 2011; 33 (10) 1476-1481
- 4 Larson DL, Rodin AE, Roberts DK, O'Steen WK, Rapperport AS, Lewis SR. Perineural lymphatics: myth or fact. Am J Surg 1966; 112 (04) 488-492
- 5 Ciccolallo L, Licitra L, Cantú G, Gatta G. EUROCARE Working Group. Survival from salivary glands adenoid cystic carcinoma in European populations. Oral Oncol 2009; 45 (08) 669-674
- 6 da Cruz Perez DE, de Abreu Alves F, Nishimoto IN, de Almeida OP, Kowalski LP. Prognostic factors in head and neck adenoid cystic carcinoma. Oral Oncol 2006; 42: 139-146
- 7 Agarwal JP, Jain S, Gupta T. et al. Intraoral adenoid cystic carcinoma: prognostic factors and outcome. Oral Oncol 2008; 44 (10) 986-993
- 8 Matsuba HM, Simpson JR, Mauney M, Thawley SE. Adenoid cystic salivary gland carcinoma: a clinicopathologic correlation. Head Neck Surg 1986; 8 (03) 200-204
- 9 Gomez DR, Hoppe BS, Wolden SL. et al. Outcomes and prognostic variables in adenoid cystic carcinoma of the head and neck: a recent experience. Int J Radiat Oncol Biol Phys 2008; 70 (05) 1365-1372
- 10 Chen AM, Bucci MK, Weinberg V. et al. Adenoid cystic carcinoma of the head and neck treated by surgery with or without postoperative radiation therapy: prognostic features of recurrence. Int J Radiat Oncol Biol Phys 2006; 66 (01) 152-159
- 11 Mendenhall WM, Morris CG, Amdur RJ, Werning JW, Villaret DB. Radiotherapy alone or combined with surgery for salivary gland carcinoma. Cancer 2005; 103 (12) 2544-2550
- 12 Parsons JT, Mendenhall WM, Stringer SP, Cassisi NJ, Million RR. Management of minor salivary gland carcinomas. Int J Radiat Oncol Biol Phys 1996; 35 (03) 443-454
- 13 Chen AM, Bucci MK, Quivey JM, Garcia J, Eisele DW, Fu KK. Long-term outcome of patients treated by radiation therapy alone for salivary gland carcinomas. Int J Radiat Oncol Biol Phys 2006; 66 (04) 1044-1050
- 14 Rapidis AD, Givalos N, Gakiopoulou H. et al. Adenoid cystic carcinoma of the head and neck. Clinicopathological analysis of 23 patients and review of the literature. Oral Oncol 2005; 41 (03) 328-335
- 15 Kokemueller H, Eckardt A, Brachvogel P, Hausamen JE. Adenoid cystic carcinoma of the head and neck–a 20 years experience. Int J Oral Maxillofac Surg 2004; 33 (01) 25-31
Address for correspondence
Publication History
Article published online:
31 December 2022
© 2022. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Billroth T. Observations on tumors of the salivary glands. Arch Path Anat 1859; 17: 357-375
- 2 Jones AS, Beasley NJ, Houghton DJ, Helliwell TR, Husband DJ. Tumours of the minor salivary glands. Clin Otolaryngol Allied Sci 1998; 23 (01) 27-33
- 3 Sultan I, Rodriguez-Galindo C, Al-Sharabati S, Guzzo M, Casanova M, Ferrari A. Salivary gland carcinomas in children and adolescents: a population-based study, with comparison to adult cases. Head Neck 2011; 33 (10) 1476-1481
- 4 Larson DL, Rodin AE, Roberts DK, O'Steen WK, Rapperport AS, Lewis SR. Perineural lymphatics: myth or fact. Am J Surg 1966; 112 (04) 488-492
- 5 Ciccolallo L, Licitra L, Cantú G, Gatta G. EUROCARE Working Group. Survival from salivary glands adenoid cystic carcinoma in European populations. Oral Oncol 2009; 45 (08) 669-674
- 6 da Cruz Perez DE, de Abreu Alves F, Nishimoto IN, de Almeida OP, Kowalski LP. Prognostic factors in head and neck adenoid cystic carcinoma. Oral Oncol 2006; 42: 139-146
- 7 Agarwal JP, Jain S, Gupta T. et al. Intraoral adenoid cystic carcinoma: prognostic factors and outcome. Oral Oncol 2008; 44 (10) 986-993
- 8 Matsuba HM, Simpson JR, Mauney M, Thawley SE. Adenoid cystic salivary gland carcinoma: a clinicopathologic correlation. Head Neck Surg 1986; 8 (03) 200-204
- 9 Gomez DR, Hoppe BS, Wolden SL. et al. Outcomes and prognostic variables in adenoid cystic carcinoma of the head and neck: a recent experience. Int J Radiat Oncol Biol Phys 2008; 70 (05) 1365-1372
- 10 Chen AM, Bucci MK, Weinberg V. et al. Adenoid cystic carcinoma of the head and neck treated by surgery with or without postoperative radiation therapy: prognostic features of recurrence. Int J Radiat Oncol Biol Phys 2006; 66 (01) 152-159
- 11 Mendenhall WM, Morris CG, Amdur RJ, Werning JW, Villaret DB. Radiotherapy alone or combined with surgery for salivary gland carcinoma. Cancer 2005; 103 (12) 2544-2550
- 12 Parsons JT, Mendenhall WM, Stringer SP, Cassisi NJ, Million RR. Management of minor salivary gland carcinomas. Int J Radiat Oncol Biol Phys 1996; 35 (03) 443-454
- 13 Chen AM, Bucci MK, Quivey JM, Garcia J, Eisele DW, Fu KK. Long-term outcome of patients treated by radiation therapy alone for salivary gland carcinomas. Int J Radiat Oncol Biol Phys 2006; 66 (04) 1044-1050
- 14 Rapidis AD, Givalos N, Gakiopoulou H. et al. Adenoid cystic carcinoma of the head and neck. Clinicopathological analysis of 23 patients and review of the literature. Oral Oncol 2005; 41 (03) 328-335
- 15 Kokemueller H, Eckardt A, Brachvogel P, Hausamen JE. Adenoid cystic carcinoma of the head and neck–a 20 years experience. Int J Oral Maxillofac Surg 2004; 33 (01) 25-31