

Subscribe to RSS
DOI: 10.1055/s-0042-1758469
Surgical Anatomy of Temporalis Muscle Transfer with Fascia Lata Augmentation for the Reanimation of the Paralyzed Face: A Cadaveric Study
Authors
Funding No funding was received for this article.
Abstract
Background The temporalis muscle flap transfer with fascia lata augmentation (FLA) is a promising method for smile reconstruction after facial palsy. International literature lacks a detailed anatomical analysis of the temporalis muscle (TPM) combined with fascia lata (FL) augmentation. This study aims to describe the muscle's properties and calculate the length of FL needed to perform the temporalis muscle flap transfer with FLA.
Methods Twenty nonembalmed male (m) and female (f) hemifacial cadavers were dissected to investigate the temporalis muscle's anatomy.
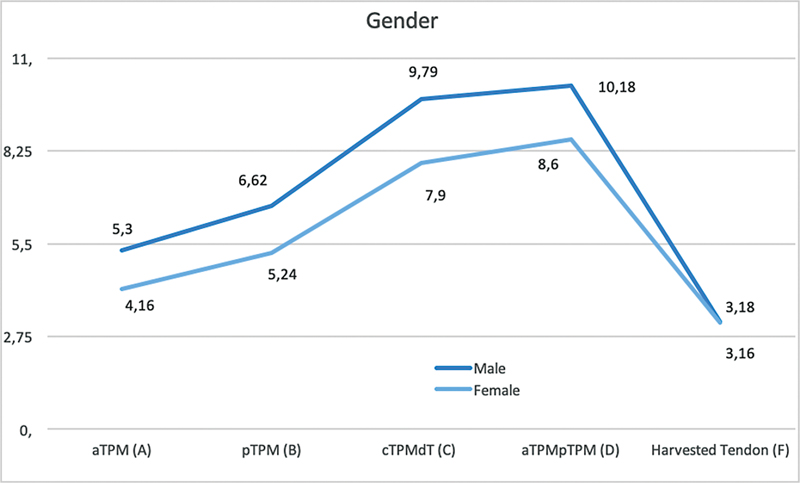
Results The calculated minimum length of FL needed is 7.03cm (f) and 5.99cm (m). The length of the harvested tendon is 3.16cm/± 1.32cm (f) and 3.18/± 0.73cm (m). The length of the anterior part of the temporalis muscle (aTPM) is 4.16/± 0.80cm (f) and 5.30/± 0.85cm (m). The length of the posterior part (pTPM) is 5.24/± 1.51cm (f) and 6.62/± 1.03cm (m). The length from the most anterior to the most posterior point (aTPMpTPM) is 8.60/± 0.98cm (f) and 10.18/± 0.79cm (m). The length from the most cranial point to the distal tendon (cTPMdT) is 7.90/± 0.43cm (f) and 9.79/± 1.11cm (m).
Conclusions This study gives basic information about the temporalis muscle and its anatomy to support existing and future surgical procedures in their performance. The recommended minimum length of FL to perform a temporalis muscle transfer with FLA is 7.03cm for female and 5.99cm for male, and minimum width of 3 cm. We recommend harvesting some extra centimeters to allow adjusting afterward.
Keywords
facial palsy - temporalis muscle - lengthening temporalis myoplasty - fascia lata augmentationIntroduction
Patients who suffer from facial palsy live under distracting conditions caused by their uncomfortable appearance and the lack of acceptance by society. The individuals between 15 to 45 years show the highest increase of incidence.[1] Most patients recover completely and spontaneously from facial palsy without any treatment, but generally, those patients only suffer from mild symptoms. In other cases, different pathways are established.
Beside the conservative treatment with corticosteroids,[2] there are several surgical methods of treatment available. Ranging from the cross-facial nerve graft to the “Babysitter-Procedure” introduced by Terzis, or a muscle transfer procedure, there are various possibilities to adjust the patient needs.[3] [4] [5]
Currently, the lengthening temporalis myoplasty (LTM), inspired by Gillies[6] and McLaughlin,[7] is a well-established operative method for the dynamic reconstruction of the lip function. This operative procedure was first described in 1997 by Daniel Labbé and has since been developed and modified multiple times.[8]
In 2002, Balaji reinvented the fascia lata augmentation (FLA), inspired by Labbé and McLaughlin.[9] [10] The FLA contains the exploration of the temporalis muscle using a very similar method to the LTM by Labbé, but instead of the total lengthening of the temporalis muscle, the author uses a harvested part of FL to bridge the gap between the tendinous part of the explored temporalis muscle and the points of insertion in the area of the labial commissure or the upper lip.[11] Overall, the procedure showed a predictable outcome with satisfying symmetry after 3 months.[9] In 2018, Jose et al modified this technique by not elevating the muscle completely, but transferring an orthodromic temporalis tendon with the extension of the FL. The coronoidectomy was performed and an 8 × 3 cm strip of FL was used in the description by Jose et al.[12] It also shows similarity to the orthodromic transfer of the temporalis muscle by Viterbo et al. Here, the authors used a 14 × 2.5 cm strip of FL to bridge the gap between the temporalis tendon and the oral commissure, the upper and the lower lip. Here, no coronoidectomy was performed.[13] [14]
In some point of view, the FLA can be referred to the mini-temporalis muscle transfer by Terzis and Olivares, where the muscle flap is lengthened with a strip of deep temporal fascia and periosteum. It was then described as a surgical procedure to upgrade both the aesthetic and motoric outcome after free muscle transfer.[15]
Modifications to reduce the operative steps and time are common, but it seems that the LTM enables the best outcome. A possible disadvantage of the procedures can be the inadequate length of the muscle, which can lead to too much tension. This results in motoric dysfunction slowed rehabilitation and displeasing aesthetical appearance. These factors decrease the potential outcome of the procedures. A recommendation for the necessary length of the muscle does not exist and the only evident information is the maximum length of muscle lengthening after LTM, which is described with 4.35 cm.[16] Since the temporalis muscle is limited to its original anatomical length, modifications aim to lengthen the muscle to reach the oral commissure, but not to create too much tension, was needed. From all the modifications, the FLA seems to be the only possible method for reaching the same level of “muscle lengthening,” because of the variable length of the harvested FL strip.[9] [11]
The international literature does not include a recommendation for the needed length of harvested FL or a comprehensive description of the TPM, although it is crucial to improve the surgical outcome of this procedure. This study aims to improve the existing procedure using FLA and other procedures where the distance can be bridged by autologous augmentation.
Materials and Methods
This anatomical study investigates the minimum length of FL needed to perform a FLA in the dynamic lip-reconstruction of the paralyzed face. The basic anatomical information of the TPM and its relation to different landmarks was assessed for a better understanding of the surgical procedures.
Twenty nonembalmed hemifacial cadavers (12 male/8 female) were included in the study. Dissections took place at the Center of Anatomy and Cell Biology of the Medical University of Vienna. The average age was 83 with a range from 64 to 96. Since the temporalis muscle is augmented during the FLA, the dissection was performed without coronoidectomy to remain the original anatomy.
After dissection, the following measurements were performed:
The distance between the medial inner margin of the zygomatic arch to the modiolus (mZAM); the distance between the lateral inner margin of the zygomatic arch to the modiolus (lZAM); the length of the harvested tendon (hT); the length of the anterior part of the TPM to the zygomatic arch (aTPM); the length of the posterior part of the TPM to the zygomatic arch (pTPM); the distance between the anterior and the posterior part of the TPM (aTPMpTPM); the distance between the most cranial point of origin of the TPM and the most distal point of the tendinous part of the TPM (cTPMdT); the length of the zygomatic arch; the distance between the tragus and the lateral orbital margin. The minimum length of FL is calculated using the mZAM, the lZAM and the hT. Since the tendinous part of the TPM begins when the muscle goes under the zygomatic arch, the length of the hT is subtracted from the mZAM and the lZAM to calculate the minimum fascia lata for the medial side (mcFL) and the minimum fascia lata for the lateral side (lcFL). The longer length is then used for the recommended length of FL. The parameters relevant to calculate the length of the FL, as well as the basic anatomical parameters of the TPM are shown in [Figs. 1] and [2]. All statistical analysis of the data was performed with Statistical Package for the Social Sciences (SPSS-Statistics Version 25). Normality was tested by using the Shapiro–Wilk test performed by SPSS. The normal distribution in total, female and male, as well as left and right was given in all samples, except in total cTPMdT. However, each gender among themselves in cTPMdT shows normal distribution.


Results
The mean mZAM for female and male is 9.73 cm and 9.17 cm with a standard deviation of 0.72 and 1.07 cm, respectively. The mean lZAM for female and male is 10.19 and 8.96 cm with a standard deviation of 0.86 and 1.18 cm, respectively. The results of mZAM and lZAM are shown in [Figs. 3] and [4]. There is a significant difference between the female and male in lZAM determinable calculated by using the independent t-test (p < 0.05).


The mean hT for female and male is 3.16 and 3.18 cm with a standard deviation of 1.32 and 0.73 cm, respectively.
For both genders, the mcFL and the lcFL were calculated using the mZAM, the lZAM, and the hT. The mean mcFL is 6.22 ± 1.24 cm and for lcFL 6.28 ± 1.29 cm in total. Separated by gender, the female and male group show a mean length of 6.56 and 5.99 cm with a standard deviation of 1.44 and 1.08 cm for mcFL, respectively. For the mean lcFl, the female and male group show a length of 7.03 and 5.78 cm with a standard deviation of 1.27 and 1.09 cm, respectively. The longer length is used for the recommendation ([Figs. 5] and [6]). According to the results measured, the mean FL for female and male is 7.03 and 5.99 cm with a standard deviation of 1.27 and 1.08 cm


The results of the other parameters are presented in [Fig. 7] and [Table 1]. No significant difference between the left and the right hemiface was given after statistical analysis of the parameters, except for the cTPMdT (p < 0.05). The mean cTPMdT for the left side is 8.49 cm with a standard deviation of 0.95 cm, whereas the right side is 9.58 cm with a standard deviation of 1.42 cm. The right side is 1.09 cm longer than the left side ([Fig. 8]).
Abbreviation: SD, standard deviation.

Discussion
For the dynamic reconstruction of the lip function, the FLA is a surgical method to reach the same level of “muscle lengthening” as the original method of LTM, since the length of the harvested FL strip is variable. Our results have shown different average lengths of FL when separated by gender, which is 7.03 cm for female and 5.99 cm for male.
Without further analysis of the data, the length of the calculated FL already showed a difference in the length of FL needed in traditional procedures. Compared with Jose et al,[12] who proposed a FL strip of 8 × 3 cm, or Viterbo, who even recommended the use of a FL strip of 14 × 2.5 cm,[13] [14] our recommendation for the length is much shorter. Bénateau et al describe a TPM tendon with a width of 4 to 6 cm,[17] which also differs from the FL strip described in a publication of Jose et al.[12] The moderate outcome with motoric dysfunctions and aesthetical deformation may result from an oversized FL strip. The calculation of the length of FL needed for the FLA has also led to an interesting analysis of the anatomical parameters. They could explain the different lengths of FL between the genders.
First, although the difference of mZAM between the genders is not significant in this study, it still shows that the female group's mZAM is average 0.56 cm longer than mZAM of the male group. The absence of significance can be the result of a rather short length of this parameter in general. The lZAM shows a significant difference of 1.23 cm (p < 0.05). Considering these results, the female group potentially needs a longer FL than the male group.
Second, the hT itself can be a few millimeters longer after total coronoidectomy. Bénateau et al described a width of 4 to 6 cm after detaching the tendon from the coronoid process.[17] Jose et al used a FL strip with a width of 3 cm,[12] which was more comparable with our experiences, since we adjusted the width of the FL to the width of the muscle's tendon. When harvesting a wider strip, the width should be adjusted to the tendon's width to avoid any unpleasant dysfunction for the patient. The tendon is an essential parameter for the FLA, as well as every other procedure. It describes the surface that can be used to suture the FL onto the TPM tendon. Since there is no significant difference between the female and the male group, the harvested tendon does not relatively affect the length of the FL.
The mcFL and the lcFL were calculated for both genders using the mZAM, the lZAM, and the hT. The results for mcFL and lcFL show very similar data. Both parameters show the gap between the tendon of the TPM and the modiolus, mcFL for the medial side, and lcFL for the lateral side. The greater length of mcFL compared with lcFL may be caused by the variability inside the male group. A significant difference of mcFL between the genders does not exist; however, it is given for lcFL (p < 0.05). These results confirm the mentioned theory that the female group shows a bigger gap between the tendon of the TPM and the modiolus on the medial side and the lateral side. Therefore, a longer FL is needed for the female group.
This data also shows the minimum of FL recommended for the FLA. For female patients, a minimum of 7.03 cm FL is needed, while for male patients, a minimum of 5.99 cm FL should be harvested for the dynamic lip-reconstruction with FLA. From our point of view, a longer strip can be harvested to have more variability to adjust the tension.
Compared with the maximum length of muscle lengthening after LTM, which is 4.35 cm,[16] our recommendation is longer, but this difference could be the result of the absence of coronoidectomy, which would allow for a longer harvested TPM tendon. But the harvested tendon, which has an average length of 3.17 cm without coronoidectomy, is still long enough to be sutured. There could also be a difference between the quality of an elevated TPM and a TPM, which has not been partially separated from its origin.
Separated in gender, there are significant differences shown in [Fig. 7].
The aTPM (p < 0.05), pTPM (p < 0.05), aTPMpTPM (p < 0.05), and cTPMdT (p < 0.05) are significantly longer in male specimens than in female specimens. This difference may be the result of different head-anatomy, which affects the length of mZAM and lZAM.
The aTPM is the muscle section that typically is not dissected or moved in published operative methods[9] [18] [19] except for the original procedure of LTM. Therefore, the aTPM represents the attached point of the TPM and has not much possibility to be lengthened. The use of a well-measured FL strip could prevent too much tension on the aTPM and therefore save the patient from a displeasing outcome.
Because of the elevation, the pTPM is more relevant for many published operative procedures, for example, for the FLA by Balaji or the modified LTM by Labbé.[9] [18] In the procedure described by Jose et al, the pTPM remains attached and is therefore treated similarly to the aTPM.[12]
The cTPMdT describes the maximum length of the TPM after detaching its tendon from the coronoid process. Since this study also considers supporting an operative procedure without muscle elevation, the cTPMdT is a very important parameter in estimating the length of FL that will be later sutured onto the TPM tendon. The parameter cTPMdT also contains the total tendinous part of the TPM.
Another point that should be considered is a significant difference of cTPMdT between the left and the right side. The mean cTPMdT for the left side is 8.49 ± 0.95 cm, whereas the right side is 9.58 ± 1.42 cm. The right side is approximately 1.09 cm significantly longer than the left side (p < 0.05). This could be the result of personal preference of the side used for mastication during the lifetime of the cadaver donors. However, there was no significant difference of the gap which must be bridged between the sides and therefore does not affect the length of the harvested FL.
Although the FLA can be referred to procedures like the mini-temporalis muscle transfer, which provides satisfying outcomes and has also been recently described as a single-stage procedure in high-risk patients,[20] the FLA can be more variable, since the length FL can be easier adjusted to the patient needs. The FLA also requires no segmental elevation of the temporalis muscle itself. The FLA can also be referred to the orthodromic temporalis muscle flap by Viterbo et al.[13] [14] The authors describe the requirement of a 14 × 2.5 cm FL strip. However, according to the results of the current study, we recommend a shorter FL strip to avoid a possible lack of tension and therefore displeasing results. Overall, the FLA is a good alternative with predictable and reliable outcomes in the treatment of facial palsy.[9]
Limitations of anatomic studies are inevitable, clinical and functional assessment of temporalis lengthening for surgical therapy was addressed in multiple conferences and discussions. The optimal method for facial reanimation procedure is to assess the outcome of functional results. Intraoperatively, insertion of free neuromuscular transplant or temporalis muscle transfers need to be overcorrected to overcome the complex tissue tension and gravity pull. If no overcorrection is performed, postoperatively it results in poor functional outcomes after a couple of months. The findings in our study give surgeons a good guideline and reference points for planning of the operation, and final clinical decision must be made intraoperatively.
Dynamic lip-reconstruction for the treatment of the paralyzed face consists of many important parameters a well-prepared surgeon must consider. Otherwise, this may result in moderate or poor outcomes for the patient. Although free muscle transplantation is the gold standard, a temporalis muscle transfer with FLA is a well-established alternative. This study recommends a minimum length of FL of 7.03 cm for female and 5.99 cm for male patients and a minimum width of 3 cm when performing a temporalis muscle transfer with FLA. A perioperative evaluation is still obligatory. It can be easier to harvest some extra centimeters to allow adjusting afterward and either to insert the temporalis on the upper lip or in the modiolus.
This newly acquired information regarding the temporalis muscle and the needed FL may help to further improve existing operative procedures and to support new methods in the surgical treatment of facial palsy.
This anatomic feasibility study has limitations:
First, an anatomic dissection is always different to a measurement in real patients. However, since the results are used by clinical physicians for the dynamic reconstruction of the paralyzed face, we used nonembalmed cadaver donors for the dissection. Posthumous changing caused by decay or freezing can only be minimized, but not completely prevented. Second, individuals with facial palsy between 15 and 45 years show the highest increase in incidence. They are also not limited by their original ethnicity. However, anatomic studies are limited to the origin of the specimen.
Third, anatomic studies are limited to the sample size due to resource reasons. For the current study, we were able to study the surgical anatomy in 20 hemifacial cadavers. The statistic power of sample size was recommended by statistic specialists.
Conflict of Interest
C.H.J.T. is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Patient Consent
In this study, we investigated the surgical anatomy of cadaver donors. The cadaver donors provided their consent in their lifetime that their bodies may be used for scientific purposes.
Ethical Approval
This study has been ethical approved by the ethical committee (IRB) of the Medical University of Vienna with the EK Nr. 1463/2018.
Authors' Contributions
Y.Z. was involved in conceptualization, data curation, formal analysis, investigation, methodology, visualization, and writing --original draft. J.S. contributed to conceptualization, investigation, methodology, and writing –review and editing. W.J.W., U.M.H., and L.R. helped in providing resources. ErdemYildiz helped in investigation. C.H.J.T. contributed to conceptualization, investigation, methodology, project administration, supervision, and writing –review and editing.
Presentation History
WRSM 2019
50th Annual meeting of the German Society of Plastic, Reconstructive and Aesthetic Surgery
58th Annual Meeting of the Austrian Society of Plastic, Aesthetic and Reconstructive Surgery
DAM 2021 (German speaking-group for Microsurgery)
-
References
- 1 Holland NJ, Weiner GM. Recent developments in Bell's palsy. BMJ 2004; 329 (7465): 553-557
- 2 Sullivan FM, Swan IR, Donnan PT. et al. Early treatment with prednisolone or acyclovir in Bell's palsy. N Engl J Med 2007; 357 (16) 1598-1607
- 3 Lee KK, Terzis JK. Management of acute extratemporal facial nerve palsy. Clin Plast Surg 1984; 11 (01) 203-210
- 4 Marre D, Hontanilla B. Gender differences in facial paralysis reanimation. Plast Reconstr Surg 2012; 129 (01) 190e-192e
- 5 Terzis JK, Tzafetta K. The “babysitter” procedure: minihypoglossal to facial nerve transfer and cross-facial nerve grafting. Plast Reconstr Surg 2009; 123 (03) 865-876
- 6 Gillies H. Experiences with Fascia Lata Grafts in the Operative Treatment of Facial Paralysis: (Section of Otology and Section of Laryngology). Proc R Soc Med 1934; 27 (10) 1372-1382
- 7 McLaughlin CR. Surgical support in permanent facial paralysis. Plast Reconstr Surg 1953; 11 (04) 302-314
- 8 Labbé D. [Lengthening of temporalis myoplasty and reanimation of lips. Technical notes]. Ann Chir Plast Esthet 1997; 42 (01) 44-47
- 9 Balaji SM. A modified temporalis transfer in facial reanimation. Int J Oral Maxillofac Surg 2002; 31 (06) 584-591
- 10 Poker A, Pescarini E, Nduka C, Kannan RY. McLaughlin's legacy in the current treatment of facial palsy. Br J Oral Maxillofac Surg 2019; 57 (08) 791-792
- 11 Dhirawani RB, Balaji SM, Singha S, Agrawal A. Temporalis muscle transfer with fascia lata sling: A novel technique for facial reanimation. Ann Maxillofac Surg 2018; 8 (02) 307-310
- 12 Jose A, Nagori SA, Roy ID, Roychoudhury A. Orthodromic transfer of the temporalis tendon with extension of the fascia lata to reanimate the smile in facial palsy. Br J Oral Maxillofac Surg 2018; 56 (09) 890-892
- 13 Viterbo F, de Paula Faleiros HR. Orthodromic transposition of the temporal muscle for facial paralysis: made easy and better. J Craniofac Surg 2005; 16 (02) 306-309
- 14 Viterbo F, Romão A, Brock RS, Joethy J. Facial reanimation utilizing combined orthodromic temporalis muscle flap and end-to-side cross-face nerve grafts. Aesthetic Plast Surg 2014; 38 (04) 788-795
- 15 Terzis JK, Olivares FS. Use of mini-temporalis transposition to improve free muscle outcomes for smile. Plast Reconstr Surg 2008; 122 (06) 1723-1732
- 16 Moubayed SP, Labbé D, Rahal A. Lengthening temporalis myoplasty for facial paralysis reanimation: an objective analysis of each surgical step. JAMA Facial Plast Surg 2015; 17 (03) 179-182
- 17 Bénateau H, Alix T, Labbé D, Elissalde JM, Salamé E. Anatomic study of the tendinous insertion lamina of the temporalis muscle. Surg Radiol Anat 2004; 26 (04) 281-284
- 18 Guerreschi P, Labbe D. Lengthening temporalis myoplasty: a surgical tool for dynamic labial commissure reanimation. Facial Plast Surg 2015; 31 (02) 123-127
- 19 Boahene KD, Farrag TY, Ishii L, Byrne PJ. Minimally invasive temporalis tendon transposition. Arch Facial Plast Surg 2011; 13 (01) 8-13
- 20 Mabvuure NT, Pinto-Lopes R, Fernandez-Diaz O, Tzafetta K. The mini-temporalis turnover flap for midface reanimation: Photogrammetric and patient-rated outcomes. J Plast Reconstr Aesthet Surg 2020; 73 (12) 2185-2195
Address for correspondence
Publication History
Received: 03 April 2022
Accepted: 12 August 2022
Article published online:
06 February 2023
© 2023. The Korean Society of Plastic and Reconstructive Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Holland NJ, Weiner GM. Recent developments in Bell's palsy. BMJ 2004; 329 (7465): 553-557
- 2 Sullivan FM, Swan IR, Donnan PT. et al. Early treatment with prednisolone or acyclovir in Bell's palsy. N Engl J Med 2007; 357 (16) 1598-1607
- 3 Lee KK, Terzis JK. Management of acute extratemporal facial nerve palsy. Clin Plast Surg 1984; 11 (01) 203-210
- 4 Marre D, Hontanilla B. Gender differences in facial paralysis reanimation. Plast Reconstr Surg 2012; 129 (01) 190e-192e
- 5 Terzis JK, Tzafetta K. The “babysitter” procedure: minihypoglossal to facial nerve transfer and cross-facial nerve grafting. Plast Reconstr Surg 2009; 123 (03) 865-876
- 6 Gillies H. Experiences with Fascia Lata Grafts in the Operative Treatment of Facial Paralysis: (Section of Otology and Section of Laryngology). Proc R Soc Med 1934; 27 (10) 1372-1382
- 7 McLaughlin CR. Surgical support in permanent facial paralysis. Plast Reconstr Surg 1953; 11 (04) 302-314
- 8 Labbé D. [Lengthening of temporalis myoplasty and reanimation of lips. Technical notes]. Ann Chir Plast Esthet 1997; 42 (01) 44-47
- 9 Balaji SM. A modified temporalis transfer in facial reanimation. Int J Oral Maxillofac Surg 2002; 31 (06) 584-591
- 10 Poker A, Pescarini E, Nduka C, Kannan RY. McLaughlin's legacy in the current treatment of facial palsy. Br J Oral Maxillofac Surg 2019; 57 (08) 791-792
- 11 Dhirawani RB, Balaji SM, Singha S, Agrawal A. Temporalis muscle transfer with fascia lata sling: A novel technique for facial reanimation. Ann Maxillofac Surg 2018; 8 (02) 307-310
- 12 Jose A, Nagori SA, Roy ID, Roychoudhury A. Orthodromic transfer of the temporalis tendon with extension of the fascia lata to reanimate the smile in facial palsy. Br J Oral Maxillofac Surg 2018; 56 (09) 890-892
- 13 Viterbo F, de Paula Faleiros HR. Orthodromic transposition of the temporal muscle for facial paralysis: made easy and better. J Craniofac Surg 2005; 16 (02) 306-309
- 14 Viterbo F, Romão A, Brock RS, Joethy J. Facial reanimation utilizing combined orthodromic temporalis muscle flap and end-to-side cross-face nerve grafts. Aesthetic Plast Surg 2014; 38 (04) 788-795
- 15 Terzis JK, Olivares FS. Use of mini-temporalis transposition to improve free muscle outcomes for smile. Plast Reconstr Surg 2008; 122 (06) 1723-1732
- 16 Moubayed SP, Labbé D, Rahal A. Lengthening temporalis myoplasty for facial paralysis reanimation: an objective analysis of each surgical step. JAMA Facial Plast Surg 2015; 17 (03) 179-182
- 17 Bénateau H, Alix T, Labbé D, Elissalde JM, Salamé E. Anatomic study of the tendinous insertion lamina of the temporalis muscle. Surg Radiol Anat 2004; 26 (04) 281-284
- 18 Guerreschi P, Labbe D. Lengthening temporalis myoplasty: a surgical tool for dynamic labial commissure reanimation. Facial Plast Surg 2015; 31 (02) 123-127
- 19 Boahene KD, Farrag TY, Ishii L, Byrne PJ. Minimally invasive temporalis tendon transposition. Arch Facial Plast Surg 2011; 13 (01) 8-13
- 20 Mabvuure NT, Pinto-Lopes R, Fernandez-Diaz O, Tzafetta K. The mini-temporalis turnover flap for midface reanimation: Photogrammetric and patient-rated outcomes. J Plast Reconstr Aesthet Surg 2020; 73 (12) 2185-2195