
RSS-Feed abonnieren
DOI: 10.1055/s-0042-1757742
Thoracic Vascular Variants and Anomalies: Imaging Findings, Review of the Embryology, and Clinical Features
- Abstract
- Introduction
- Embryology
- Aortic Arch Variants
- Superior Vena Cava Abnormalities
- Azygos System Abnormalities
- References
Abstract
Thoracic vascular malformations are a set of complex congenital abnormalities that result in major alterations of the patient's anatomy. It can be discovered incidentally or the anomalies may generate heart failure with a right-to-left shunt, dysphagia, dyspnea, stridor, cough, recurrent bronchopulmonary infections, hypoxemia, paradoxical emboli, and occasionally apneas and massive hemothorax.
The knowledge of the embryology, and the normal development of the vascular structures of the thorax, allows to understand these abnormalities—and thus helps in making an accurate diagnosis—with its possible complications, symptoms, and treatments for the patient. The following is a review of the most common thoracic vascular malformations and their imaging findings.
#
Introduction
Chest computed tomography is a tool that is commonly used to study many symptoms and diseases. A strong grasp of anatomy and anatomical variants is necessary to adequately interpret images. Anatomical variants can cause erroneous diagnoses and can cause complications during surgical interventions. A review of vascular variants in the thorax is therefore justifiable.
#
Embryology
Embryology of the Aortic Arch
The development of the aortic arch is a complex process that occurs in the third week of fetal life, and leads to a variety of pathological anomalies and congenital variants.[1]
Each primitive aorta has a ventral and a dorsal segment; both ventral segments fuse to form the aortic sac and the dorsal segments fuse in the midline to form the descending aorta.[1] Six pairs of primitive arches form between the dorsal and ventral segments, and the dorsal aorta gives rise to several intersegmental arteries. The primitive arches appear and disappear one after another in craniocaudal order and not all are present at the same time.
The arch is formed as the primitive arch returns. The mechanism of persistence, development, and regression is not fully understood; however, it seems that the migration of neural crest cells plays an important role in this regression.[1]
The first and second arches return except for small portions that configure the maxillary and stapedial arteries, respectively. In humans, the fifth aortic arches are unusual and they do not form or are seen only temporarily.[2]
The third, fourth, and sixth arches are the most important in vascular development. The third pair of arches forms the common carotid arteries and part of the internal carotid arteries. The fourth left arch forms part of the left definitive aortic arch[2] and the right proximal subclavian artery. The dorsal aorta gives rise to the distal subclavian artery.[2] The right subclavian artery fuses with the right common carotid artery forming the brachiocephalic artery.[2]
The left subclavian artery is formed by the seventh left intersegmental artery.
The right and left pulmonary arteries are derived from the sixth aortic arch. The left sixth arch forms the ductus arteriosus. In the first month of life, the ductus arteriosus obliterates and becomes the ligamentum arteriosus.[2]
Although the appearance of the arches is sequential, a theory of a double aortic arch (DAA) system with bilateral arches and two ductus arteriosus surrounding the trachea and esophagus is proposed.[2] The development of the normal left aortic arch with a left descending aorta occurs when the right aortic arch (RAA) regresses. However, this model does not explain the lateral position of the descending aorta.[1]
#
Embryology of the Superior Vena Cava (SVC) and Brachiocephalic Vein
The normal thoracic venous system includes two subclavian veins and two brachiocephalic veins that drain into the superior vena cava (SVC), which finally drains into the right atrium. Embryologically, these veins are derived from a pair of anterior veins and a pair of common cardinal veins (the common cardinal vein results from the union of the anterior cardinal vein and the posterior cardinal vein before entering the venous sinus).[3] [4]
In the seventh week of fetal life, the cardinal veins give rise to the main venous drainage system of the embryo. The anterior cardinal veins drain the cephalic part of the embryo, and the posterior cardinal veins the remaining part. These veins come together before entering the venous sinus forming the common cardinal veins. The anterior cardinal veins configure an anastomosis that will later be the left brachiocephalic vein[3] ([Fig. 1]).

The SVC, the right brachiocephalic trunk, and the right jugular vein originate from the right cardinal system.[3]
The left anterior cardinal venous system disappears at the level of the anastomosis forming the ligament of the left vena cava and persists above this level as the left SVC and internal jugular vein. The left common cardinal vein becomes the oblique vein of the left atrium (vein of Marshall) and drains into the coronary sinus. The anastomosis between the anterior cardinal veins gives rise to the left brachiocephalic trunk.[3]
#
#
Aortic Arch Variants
Bovine Arch
The most common variant of the branching pattern of the aortic arch is the bovine arch. In this variant, the left common carotid artery and the brachiocephalic artery originate from a common trunk. It is considered a normal anatomical variant, but may have implications in the context of thoracic surgery or interventions[1] ([Fig. 2]).

#
Isolated Vertebral Artery
The supra-aortic vessels have several known branching patterns, including the isolated left vertebral artery (LVA), which originates directly from the aortic arch and is the most common anatomical variant of the vertebral artery with an incidence close to 4%.[5] The LVA generally originates from the subclavian artery and enters the intracranial space through the dura at the first cervical vertebra. The aberrant origin of the LVA may lead to a dissection of the isolated vertebral artery[6] ([Fig. 3]) and this may lead to ischemic stroke.
#
Coarctation of the Aorta
Aortic coarctation is a common congenital heart disease, representing 6 to 8% of cases of congenital heart disease, and the fifth most common anomaly in this group of patients. It consists of an obstructive lesion of the aorta adjacent to the ductus arteriosus or ligament and occurs most frequently just distal to the origin of the left subclavian artery. Most cases of aortic coarctation are sporadic; however, there is a clear genetic component in at least 4% of the children of women with aortic coarctation. The bicuspid aortic valve is the most frequently associated anomaly and has been described in up to 75% of patients with aortic coarctation.[7]
The clinical manifestations depend on age. In the best of cases, coarctation generates mild to moderate perfusion alterations after complete closure of the duct. Collateral circulation develops gradually, thus attenuating the clinical manifestations. Patients usually present in adulthood with hypertension, bleeding intracranial aneurysms, left ventricular hypertrophy, and congestive heart failure.[7]
Cardiac resonance and magnetic resonance (MR) angiography are used in the diagnosis and postsurgical follow-up of patients with coarctation of the aorta. These techniques offer morphological and functional information, and can be performed with or without contrast. Contrast-enhanced MR imaging (MRI) is the ideal technique in patients with a known history of kidney disease. Phase contrast and steady-state free precession sequences are useful for objective and subjective evaluation of pressure gradients, which are important parameters for surgical and endovascular planning.[7] MRI allows the evaluation of the postsurgical anatomy, the characterization of the residual or recurrent obstruction, the relationship of the obstruction with the vessels of the aortic arch, and the presence of collateral vessels; it also allows the evaluation of the myocardial mass of the left ventricle, evaluation of the systolic function, and assessment of the severity of the obstruction. Patients undergoing procedures to correct coarctation require several follow-up images, so radiation-free studies such as MRI offer an advantage over tomography.[7]
Imaging Findings
-
Chest radiography: Notch in the lower portion of the ribs (due to hypertrophy of the intercostal arteries).
-
CT angiography: It is used to define the exact location and severity of the narrowing. Focal stenosis is seen in the posterior region of the aorta just distal to the origin of the left subclavian artery[7] ([Fig. 4]).

#
#
Innominate Artery Compression Syndrome
The innominate or brachiocephalic artery compression syndrome is an uncommon cause of tracheal stenosis that occurs in the pediatric population.[8] [9] The brachiocephalic artery has its normal origin on the left of the trachea; it travels anterior to the trachea and reaches the right arm. The diagnosis is suggested by several findings: an origin of the brachiocephalic artery on the left of the trachea, tracheal stenosis on dynamic imaging or bronchoscopy at the level where the brachiocephalic artery crosses, and obstructive symptoms.[9] [10] Symptomatic patients often present with respiratory stridor, cough, recurrent bronchopulmonary infections, and occasionally apneas.[9]
Imaging Findings
CT and MRI have been helpful in delineating vascular anatomy in multiple planes.[9] Is one cause of posterior displacement of the trachea. ([Fig. 5]).

#
#
Vascular Rings
These account as 1% of congenital vascular malformations and are called vascular rings when the trachea and esophagus are surrounded by vascular structures derived from the primitive arches.[11] These vessels can completely surround the respiratory and digestive structure or only cause compression without surrounding it in a complete ring.[11]
The vessels derived from the primitive arches are: the aortic arch, the branches of the aortic arch and the pulmonary arteries, the ductus arteriosus, and the ligamentum arteriosum. Thus, the most common vascular rings are the DAA, RAA with aberrant left subclavian, left aortic arch with aberrant right subclavian, and anomalous origin of the left pulmonary artery.[11]
The vascular rings are classified as complete and incomplete. The complete rings are: DAA, RAA with aberrant left subclavian artery with duct, left aortic arch with right descending aorta with right duct, RAA with left descending aorta with duct, and left aortic arch with aberrant right subclavian artery with right duct. The incomplete rings are the pulmonary sling and innominate artery compression syndrome.[11]
#
Double Aortic Arch
The DAA has been reported as the most symptomatic vascular ring, in up to 60% of cases. The majority of patients are symptomatic because it results in the compression of the trachea and esophagus, and the patients may present with cyanosis, tachypnea, stridor, and dysphagia.[11]
It results when a co-dominance of the RAA and left aortic arch is present from the persistence of the fourth primitive aortic arches. In 81% of the cases there is a dominance of the RAA, in 16% the left arch is dominant, and in 3% it is co-dominant. When the RAA is dominant, it presents with a descending left aorta and a left arteriosus ligament; the left arch may have a small diameter or be atretic, with a fibrous tract usually ipsilateral to the descending aorta and located distal to the origin of the subclavian artery[11] ([Fig. 6]).

Imaging Findings
CT and MRI: Two aortic arches are found that originate from the ascending aorta and extend to each side of the esophagus and trachea.[11] The dominant arch is larger and opposite to the descending aorta. As each arch gives rise to the subclavian arteries and the common carotid arteries separately, the sign of “four arteries” can also be found in the axial images: two ventral carotid arteries and two dorsal subclavian arteries separated uniformly, forming a trapezoidal figure around the trachea.[11]
#
#
Right Aortic Arch (RAA)
This vascular ring is present when there is a combination of a RAA and an aberrant left subclavian artery, the latter of which originates as the last vessel of the aorta and it often has a dilatation known as Kommerell diverticulum (which is a bulbous configuration forming at the base of this aberrant left subclavian artery with the right-sided aortic arch). The abnormality with an aberrant left subclavian artery is not usually accompanied by cardiac anomalies; the other type with a mirror image of the supra-aortic trunk commonly is associated with cardiac anomalies (98%).
Most patients are asymptomatic because the ring has little compressive effect because it is an incomplete ring. If there is a left arteriosus ligament a complete vascular ring is formed, which may cause more symptoms.[11]
There are several forms of the RAA: RAA with aberrant left subclavian artery, RAA with mirror branching with permeable retroesophageal artery ductus arteriosus, and left aortic arch with right descending aorta and right canal.[11]
Imaging Findings
CT and MRI: The subclavian artery originates as the last emergence and crosses the mediastinum from right to left, posterior to the esophagus, forming an incomplete vascular ring[11] ([Figs. 7] and [8]).


#
#
Right Aortic Arch with Left Descending Aorta
It is also called retroesophageal circumflex aortic arch.[1] It is one of the rarest vascular rings.[1] Stenosis is generated above the carina (T4–T5) when the aorta crosses to the left, posterior to the esophagus.[1] [12] When the midline is crossed, a diverticulum originates within the left duct or ligament arteriosus that connects with the pulmonary artery and completes the vascular ring.[1] [12]
Supra-aortic vessels can originate as follows: left brachiocephalic artery, right common carotid artery, right subclavian artery or left common carotid artery, right common carotid artery, right subclavian artery, and aberrant left subclavian artery.[1] [12]
This anomaly occurs due to a lack of regression of the left dorsal aorta or regression of the left fourth arch.[1]
Treatment in very symptomatic cases is surgical.
#
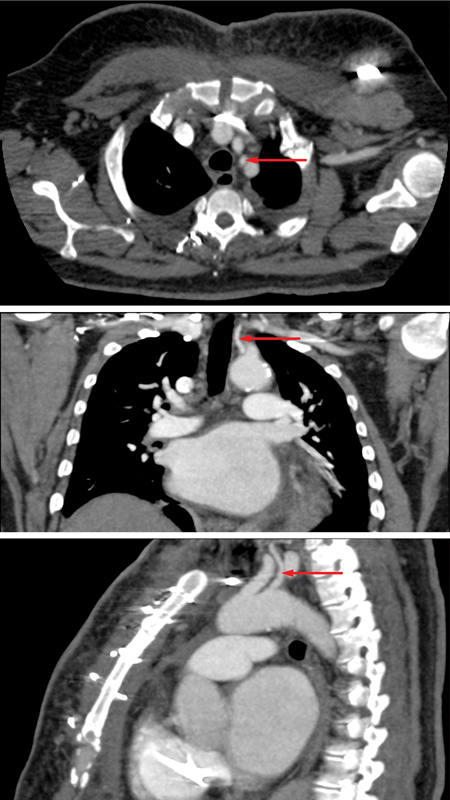
Left Aortic Arch with Aberrant Right Subclavian
This is the most common congenital anomaly of the aortic arch with a prevalence in the general population of 0.5 to 2%. The right subclavian artery originates in the proximal descending thoracic aorta, as the last branch of the arch.[11] As seen in the RAA with aberrant left subclavian, the origin of the aberrant vessel can be dilated and form a Kommerell diverticulum.[11]
Its configuration generates a compression of the esophagus, in an incomplete vascular ring, with only three sides of the trachea and esophagus compressed by the malformation. This configuration is associated with dysphagia lusoria.[11]
Imaging Findings
CT and MRI: The subclavian artery originates as the last arch emergence and has an oblique retroesophageal course from left to right and from bottom to top[11] ([Fig. 9]).

#
#
#
Superior Vena Cava Abnormalities
Superior Vena Cava Duplication
This embryological alteration has an incidence of 3% and is present in congenital heart disease in up to 11% of patients.[13]
The SVC is formed from the confluence of the left and right brachiocephalic veins in the superior mediastinum at the level of the first costal cartilage, then enters the right atrium in the middle mediastinum at the level of the third costal cartilage; the left vena cava usually drains into the right atrium through the coronary sinus.[14] In the first 2 months of fetal development,[14] SVC originates from the common cardinal veins and the right anterior vein. The cardinal veins include the anterior cardinal vein (which drains the cephalic portion of the body) and the posterior cardinal vein (which drains the rest of the embryo); these join on each side to form the common cardinal vein before entering the venous sinus.[15] The nonregression of the left anterior cardinal vein leads to a duplication of the SVC[16] ([Fig. 1]).
Imaging Findings
CT: There will be two SVCs, one on each side. Most of the times the right SVC is smaller than the left one and the left brachiocephalic vein is absent,[15] but this configuration does not always happen and the left SVC can be smaller ([Fig. 10]).

#
#
Persistence of the Left Superior Vena Cava (PLSVC)
It is a rare congenital anomaly, with a prevalence of 0.3 to 0.5% of the general population and is present in up to 12% of patients with congenital heart disease.[17] The patient may present with a normal right SVC and if so, there is a fusion of the right and left vena cava, without the left innominate vein.[17]
The clinical significance of PLSVC arose from the drainage site and associated abnormalities.
A PLSVC with right atrial drainage will have expansion of the coronary sinus, which may cause compression of the atrioventricular node and the bundle of His, with secondary cardiac arrhythmias and compression of the left atrium with decreased cardiac output.[18]
Left atrial drainage through the PLSVC is sometimes asymptomatic because it does not cause a significant right-to-left shunt.[18]
Imaging Findings
When left SVC is present, it is located left to the aortic arch, normally draining to the right atrium through the coronary sinus (which will be enlarged, this being an indirect indicator of the presence of this malformation). In some cases, it empties into the left atrium generating a right-to-left shunt[17] ([Fig. 11]).

#
#
#
Azygos System Abnormalities
Azygos Fissure (Azygous Lobe)
It is found in 1% of the population. It occurs when the right posterior cardinal vein (one of the precursors to azygos) fails to migrate above the right lung apex and instead, it traverses the pulmonary parenchyma with some pleural layers trapping a portion of the lobe. This portion is not independent and receives arterial and bronchial input from the apical or posterior segment of the right pulmonary lobe.[19]
Imaging Findings
X-ray: The azygos lobe is usually delimited on radiography by the azygos fissure (a thin convex line that crosses the apex of the right lung) and the mediastinum.
CT: The azygos fissure extends from the lateral aspect of the vertebral body (posterior) to the right brachycephalic vein and SVC (anterior). The azygos vein will appear as a thick structure that is continued by the fissure and will end in the SVC or less frequently in the right brachycephalic vein. The aortic arch position will be higher[20] ([Fig. 12]).

#
#
#
#
Conflict of Interest
The authors have no conflicts of interest to declare.
Acknowledgment
We thank Dr. Ana Maria Alvarado (radiologist), for sharing the images of the DAA.
-
References
- 1 Hanneman K, Newman B, Chan F. Congenital variants and anomalies of the aortic arch. Radiographics 2017; 37 (01) 32-51
- 2 Maldonado JA, Henry T, Gutiérrez FR. Congenital thoracic vascular anomalies. Radiol Clin North Am 2010; 48 (01) 85-115
- 3 Ruano CA, Marinho-da-Silva A, Donato P. Congenital thoracic venous anomalies in adults: morphologic MR imaging. Curr Probl Diagn Radiol 2015; 44 (04) 337-345
- 4 Sonavane SK, Milner DM, Singh SP, Abdel Aal AK, Shahir KS, Chaturvedi A. Comprehensive imaging review of the superior vena cava. Radiographics 2015; 35 (07) 1873-1892
- 5 van der Weijde E, Bakker OJ, Sonker U, Heijmen RH. Isolated left vertebral artery and its consequences for aortic arch repair. J Vasc Surg Cases Innov Tech 2019; 5 (03) 369-371
- 6 Yuan S-M. Aberrant origin of vertebral artery and its clinical implications. Rev Bras Cir Cardiovasc 2016; 31 (01) 52-59
- 7 Karaosmanoglu AD, Khawaja RDA, Onur MR, Kalra MK. CT and MRI of aortic coarctation: pre- and postsurgical findings. AJR Am J Roentgenol 2015; 204 (03) W224-33
- 8 Karacan A, Türkvatan A, Karacan K. Anatomical variations of aortic arch branching: evaluation with computed tomographic angiography. Cardiol Young 2014; 24 (03) 485-493
- 9 Kurochka S, Marques P, Carvalho R, Sanches M, Moreira A. Innominate artery compression syndrome of the trachea. 10/08/2011. https://www.eurorad.org/case/9331 Accessed July 5, 2022
- 10 Fawcett SL, Gomez AC, Hughes JA, Set P. Anatomical variation in the position of the brachiocephalic trunk (innominate artery) with respect to the trachea: a computed tomography-based study and literature review of innominate artery compression syndrome. Clin Anat 2010; 23 (01) 61-69
- 11 Abad P, Mesa S, Uribe R, Alvarado AM, Isaza S. Anillos vasculares, hallazgos por resonancia magnética. Rev Colomb Radiol 2018; 29 (03) 4949-4956
- 12 Priya S, Thomas R, Nagpal P, Sharma A, Steigner M. Congenital anomalies of the aortic arch. Cardiovasc Diagn Ther 2018; 8 (Suppl. 01) S26-S44
- 13 Hutchison SJ, Merchant N. Principles of Cardiac and Vascular Computed Tomography. Philadelphia, PA: Saunders/Elsevier; 2015
- 14 Demos TC, Posniak HV, Pierce KL, Olson MC, Muscato M. Venous anomalies of the thorax. AJR Am J Roentgenol 2004; 182 (05) 1139-1150
- 15 Farazi-Chongouki C, Dalianoudis I, Ninos A. et al. Double superior vena cava: presentation of two cases and review of the literature. Acta Chir Belg 2019; 119 (05) 316-321
- 16 Taha Ali TF, Ghareep A-N. Anatomical variant of large mediastinal veins: incidental findings on MDCT chest. Egypt J Radiol Nucl Med 2017; 48 (01) 81-86
- 17 Urhan Giraldo ÁV, Uribe González R. Persistencia de la vena cava superior izquierda: presentación de un caso. Rev Colomb Radiol 2017; 28: 4486-91
- 18 Azizova A, Onder O, Arslan S, Ardali S, Hazirolan T. Persistent left superior vena cava: clinical importance and differential diagnoses. Insights Imaging 2020; 11 (01) 110
- 19 Mata J, Cáceres J, Alegret X, Coscojuela P, De Marcos JA. Imaging of the azygos lobe: normal anatomy and variations. AJR Am J Roentgenol 1991; 156 (05) 931-937
- 20 Lin F, Xu Y, Liu L. Pulmonary azygous lobe. QJM 2018; 111 (02) 137-137
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
28. November 2022
© 2022. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Hanneman K, Newman B, Chan F. Congenital variants and anomalies of the aortic arch. Radiographics 2017; 37 (01) 32-51
- 2 Maldonado JA, Henry T, Gutiérrez FR. Congenital thoracic vascular anomalies. Radiol Clin North Am 2010; 48 (01) 85-115
- 3 Ruano CA, Marinho-da-Silva A, Donato P. Congenital thoracic venous anomalies in adults: morphologic MR imaging. Curr Probl Diagn Radiol 2015; 44 (04) 337-345
- 4 Sonavane SK, Milner DM, Singh SP, Abdel Aal AK, Shahir KS, Chaturvedi A. Comprehensive imaging review of the superior vena cava. Radiographics 2015; 35 (07) 1873-1892
- 5 van der Weijde E, Bakker OJ, Sonker U, Heijmen RH. Isolated left vertebral artery and its consequences for aortic arch repair. J Vasc Surg Cases Innov Tech 2019; 5 (03) 369-371
- 6 Yuan S-M. Aberrant origin of vertebral artery and its clinical implications. Rev Bras Cir Cardiovasc 2016; 31 (01) 52-59
- 7 Karaosmanoglu AD, Khawaja RDA, Onur MR, Kalra MK. CT and MRI of aortic coarctation: pre- and postsurgical findings. AJR Am J Roentgenol 2015; 204 (03) W224-33
- 8 Karacan A, Türkvatan A, Karacan K. Anatomical variations of aortic arch branching: evaluation with computed tomographic angiography. Cardiol Young 2014; 24 (03) 485-493
- 9 Kurochka S, Marques P, Carvalho R, Sanches M, Moreira A. Innominate artery compression syndrome of the trachea. 10/08/2011. https://www.eurorad.org/case/9331 Accessed July 5, 2022
- 10 Fawcett SL, Gomez AC, Hughes JA, Set P. Anatomical variation in the position of the brachiocephalic trunk (innominate artery) with respect to the trachea: a computed tomography-based study and literature review of innominate artery compression syndrome. Clin Anat 2010; 23 (01) 61-69
- 11 Abad P, Mesa S, Uribe R, Alvarado AM, Isaza S. Anillos vasculares, hallazgos por resonancia magnética. Rev Colomb Radiol 2018; 29 (03) 4949-4956
- 12 Priya S, Thomas R, Nagpal P, Sharma A, Steigner M. Congenital anomalies of the aortic arch. Cardiovasc Diagn Ther 2018; 8 (Suppl. 01) S26-S44
- 13 Hutchison SJ, Merchant N. Principles of Cardiac and Vascular Computed Tomography. Philadelphia, PA: Saunders/Elsevier; 2015
- 14 Demos TC, Posniak HV, Pierce KL, Olson MC, Muscato M. Venous anomalies of the thorax. AJR Am J Roentgenol 2004; 182 (05) 1139-1150
- 15 Farazi-Chongouki C, Dalianoudis I, Ninos A. et al. Double superior vena cava: presentation of two cases and review of the literature. Acta Chir Belg 2019; 119 (05) 316-321
- 16 Taha Ali TF, Ghareep A-N. Anatomical variant of large mediastinal veins: incidental findings on MDCT chest. Egypt J Radiol Nucl Med 2017; 48 (01) 81-86
- 17 Urhan Giraldo ÁV, Uribe González R. Persistencia de la vena cava superior izquierda: presentación de un caso. Rev Colomb Radiol 2017; 28: 4486-91
- 18 Azizova A, Onder O, Arslan S, Ardali S, Hazirolan T. Persistent left superior vena cava: clinical importance and differential diagnoses. Insights Imaging 2020; 11 (01) 110
- 19 Mata J, Cáceres J, Alegret X, Coscojuela P, De Marcos JA. Imaging of the azygos lobe: normal anatomy and variations. AJR Am J Roentgenol 1991; 156 (05) 931-937
- 20 Lin F, Xu Y, Liu L. Pulmonary azygous lobe. QJM 2018; 111 (02) 137-137