

RSS-Feed abonnieren
DOI: 10.1055/s-0042-1754383
Doppler Ultrasound Testing Suggests Hemorrhoids in Females may be a Consequence of Impaired Blood Flow Associated with Pelvic Organ Prolapse
Authors
Funding No financial support has been received.

Abstract
Background It has been observed that there is a high incidence of hemorrhoids in female patients with pelvic organ prolapse. Also, in these patients, hemorrhoidal disease improves after the surgical correction of the pelvic organ prolapse.
Objective Our hypothesis was that a cause-effect relationship between pelvic organ prolapse, and hemorrhoids might be the key. The objective of this study was to find an element which connects these two conditions.
Study Design We conducted a pilot study which consisted of two parts. An initial part, in which we asked several patients with grades III and IV pelvic organ prolapse and hemorrhoids, who have undergone surgery for prolapse, to determine the impact of the surgical restoration of the prolapsed organs on their hemorrhoidal disease. For the second part, on several patients with uncorrected uterine prolapse grades III and IV, we determined the resistive index of the hemorrhoidal branches within the rectal wall before and after manual reduction of the prolapse.
Results First, more than 50% of patients who underwent uterine prolapse correction described an improvement of their hemorrhoidal disease of over 50%. Second, the resistive index of the hemorrhoidal branches was significantly lower after manual reduction of the prolapse. We consider that obstructed veins due to pelvic organ prolapse might induce the dilation of the hemorrhoids. The direct measurement of the resistive index of the hemorrhoidal branches allows us to directly assess the increased resistance in the rectal vascular system.
Conclusion Venous stasis and impaired vascular flow might be the pathophysiological explanation for the association between pelvic organ prolapse and hemorrhoids. In these patients, the pathogenic treatment should aim at the restoration of a normal blood flow (prolapse surgical cure) instead of focusing on hemorrhoids only.
Introduction
A great number of women is affected by pelvic organ prolapse (POP), a condition characterized by the descent of the pelvic organs, especially the uterus, into the vaginal canal. Another common disorder, which affects more women than men is represented by hemorrhoids.[1] It has been observed that large uterine prolapse and hemorrhoids often coexist, and we assume that there may be a cause-effect relationship that can explain this association. Also, the surgical treatment of POP leads in most cases to clinical improvement of the hemorrhoids, which further sustains this argument.
The exact pathophysiology of the hemorrhoidal development is not yet fully understood. The sliding anal canal theory is widely accepted, and it sustains that the connective tissue which composes the anal cushions deteriorate, therefore causing their descent and venous dilatation.[2] In one of the few reviews concerning hemorrhoids, Zhifei Sun et al. described abnormal venous dilatation in the anal cushions.[3]
Another take on the problem would be to consider venous dilatation of the anal cushions not only as a structural problem concerning the connective tissue within their wall, but also as a consequence of impaired blood flow. This would explain the rapid improvement of the hemorrhoidal disease almost immediately after surgery for POP.
Other authors have described the effect that POP has on the pelvic vessels. In 1993, Petros and Ulmsten explained that due to high laxity of the cardinal and uterosacral ligaments, the uterus descends into the vaginal canal causing obstruction of the pelvic vessels and venous dilatation.[4] Paradisi et al. mentioned, in 2010, that the protrusion of the anterior rectal wall toward its lumen impairs rectal blood flow.[5] Another conclusion was taken by Abendstein, who stated that high laxity is one of the main causes for hemorrhoids, which, combined with pelvic venous stasis, can explain their high incidence in women with POP.[6] The same author published an article on the relationship between loose ligaments involved in POP and rectal intussusception.[7]
In terms of symptomatology, large uterine prolapse and hemorrhoids have multiple similarities. Pruritus can be due to irritation of the hemorrhoidal epithelium as well as the vaginal epithelium. Bleeding is a common symptom of hemorrhoidal disease, but it can also occur due to the erosion of the prolapsed uterus. Also, rectal fullness or the feeling of incomplete evacuation can be explained by both pathologies.
Materials and Methods
We conducted a pilot study that consisted of two parts. First, we analyzed the impact of prolapse surgery on the hemorrhoidal disease, from the patients' perspective. Second, we tried to objectively assess how the reduction of the prolapse affects the hemorrhoids. The sample consisted of 113 women, who had POP surgeries between 2011 and 2015 at the hospital. The inclusion criteria of the patients involved high grade uterine prolapse, associated with hemorrhoids. More exactly, the POP cases included degrees III and IV, and, in addition, the condition needed to show a significant improvement of the hemorrhoids after the POP surgery. However, since there is no standard classification concerning hemorrhoids, we subjectively established which of the patients achieved an improvement of over 75%, 50%, or less than 50%. Our subjectivity was based also on the perceived hemorrhoidal symptomatology of the women before and after surgery. As such, the patients were asked to fill in a questionnaire that measured their symptomatic perception on a 5-point Likert scale, ranging from 1 - no symptomatology to 5 - high symptomatology.
So, the symptomatic improvement after surgery was determined both clinically, after surgery by the surgeon, as well as by the patient herself, in providing a perceived efficiency of the surgery.
Despite taking into consideration the subjective method of assessing the improvement of hemorrhoids after the POP surgery, we also looked for a potential mechanism that may explain it in more objective terms. We believe that high grade uterine prolapse impairs the pelvic venous blood flow, which contributes greatly to the hemorrhoidal disease. The measurable parameter that may offer this possibility is the resistive index (RI) of the arterial vessels, located within the anal canal, where, in fact, the hemorrhoidal branches are located.
Taking into consideration the literature about RI, we have conducted ultrasound examinations to women with POP degrees III and IV, before and after the reduction of prolapse. Resistive index is a calculated flow parameter derived from the maximum, minimum and mean Doppler frequency shifts during a cardiac cycle (RI = peak systolic velocity – end diastolic velocity/peak systolic velocity). Peak systolic velocity is the maximum speed, achieved during the cardiac systole and end-diastolic velocity is the minimum speed, achieved during the diastole. As a vessel narrows and resistance to flow increases, the RI will increase.
We performed an ultrasound examination to a second sample of 51 patients with grades III and IV POP admitted to our clinic between 2016 and 2019. The ultrasound examination was performed using a Voluson E8 with a 5-mHz vaginal probe. The probe was transrectally introduced, and the flow of the arterial vessels was measured between 3 and 9 o'clock, vessels which we assumed to be hemorrhoidal branches. Pulse Doppler was used to measure the RI mean values of the right and left arterial vessels. Consequently, the prolapse was manually reduced, and a new mean of RI values was registered.
Data was collected and analyzed using the IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA) The data collected included demographic information, such as the age of the patients, as well as qualitative information about the classification of the POP. The mean age of the patients and the mean RI values before and after the POP reduction were determined. The RI values were checked for normal distribution using the Shapiro-Wilk tests. To assess if there was a difference between the values registered for the RI with the prolapse and the RI values after the POP reduction, the paired t-test was used, as well as the size effect to measure the impact of the surgery on the POP. According to Cohen (1988), effect values around 0.20 are considered low, effect values around 0.50 are considered moderate, while effect values around 0.80 are high.
A repeated measure analysis of variance (ANOVA) was conducted so as to identify if there were any differences between the RI values classified after the POP stage as well as the effect of the interaction between POP and RI.
All tests were considered statistically significant at a p-value < 0.05.
Results
For the first part of our study, we had a total number of 253 patients who underwent surgery for POP in our hospital between 2011 and 2015, including all grades of POP. ([Fig. 1])

From the 114 patients who were diagnosed with grades III and IV POP, 90 of them were also suffering from hemorrhoidal disease. ([Fig. 2])

After prolapse surgery, the patients were asked to subjectively assess the grade of improvement it had on their hemorrhoidal disease. The results showed that 40% felt an improvement of more than 75% regarding their hemorrhoidal disease, 20% felt an improvement of over 50%, and 20% showed improvement of less than 50%. ([Fig. 3])

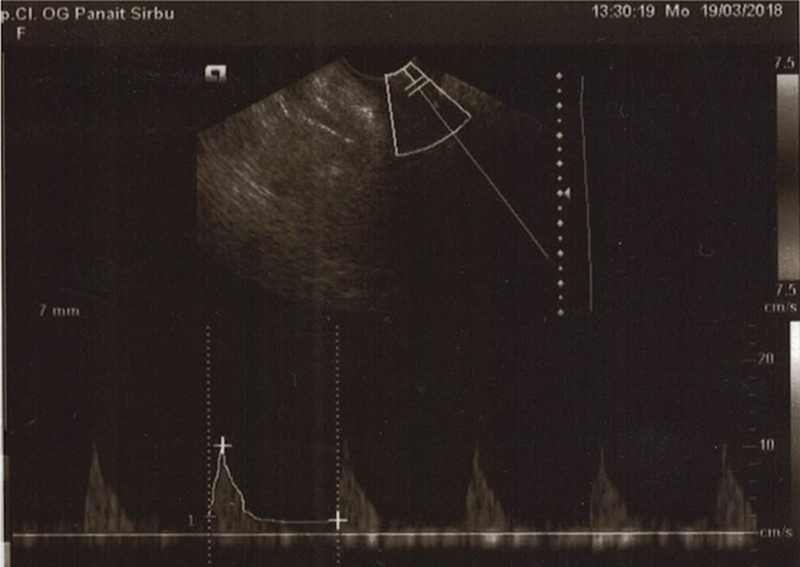
We then continued with our second part of the study, trying to find a measurable parameter to explain this improvement. Doppler measurements were performed on the hemorrhoidal arterial branches within the rectal wall ([Figs. 4] and [5]).

The mean age of the patients was 67.43 (±10.67). There were 27 (52.9%) patients with POP grade III and 24 (47.1%) patients with POP grade IV ([Fig. 6]).

The RI with POP was 0.89 (±0.06), and the RI with POP reduction was 0.81 (±0.05) ([Fig. 7]).

The Shapiro-Wilk tests of normality (p > 0.05) revealed that the RI with prolapse and the RI with prolapse reduction had normal distributions ([Table 1] and [Fig. 8]).
|
Shapiro-Wilk |
|||
|---|---|---|---|
|
Statistic |
df |
p-value |
|
|
RI with prolapse |
0.964 |
51 |
0.124 |
|
RI with prolapse reduction |
0.978 |
51 |
0.458 |
Abbreviations: df, degrees of freedom; RI, resistive index.

A paired t-test was conducted to assess whether there is a significant difference between the before and after RI registered values. According to the results in [Table 2], there was a statistically significant difference between RI with a prolapse and RI with a prolapse reduction, t (50) = 11,476, p = 0.001 ([Table 2]). This outcome also suggests that the mean RI of the POP reduction is smaller than the RI of the POP before reduction (95% CI 0.07–0.10). The effect size of the reduction was higher than 0.80, suggesting a significant improvement in the patients' conditions, after the POP reduction ([Fig. 9]).

Abbreviations: df, degrees of freedom; RI, resistive index.
According to the POP classification, the mean age of the patients with POP grade III was 64.52 years (±10.72) and for the patients with POP grade IV was 70.71 years (±9.81). For POP grade III, the mean RI value for the patients with prolapse was 0.86 (±0.05), and the mean RI value of the patients with prolapse reduction was 0.79 (±0.04), whereas for POP grade IV, the mean RI values for the patients with prolapse was 0.93 (±0.04) and the mean RI value of the patients with prolapse reduction was 0.83 (±0.04) ([Fig. 10]).

As the previous results have showed, the repeated measures ANOVA confirmed there is a statistically significant difference between the RI values with the prolapse and the RI values with the prolapse reduction. However, the repeated measures ANOVA also revealed there is a statistically significant difference between the POP stages (F (1.49) = 26.55, p = 0.001), and the effect size was low (d = 0.35). Regarding the interaction POP x RI, the repeated measures ANOVA indicated there is a statistically significant difference in the evolution of POP stages and the RI values with the prolapse and with the prolapse reduction (F (1.49) = 4.25, p = 0.04). In [Fig. 11], it may be observed that POP grade III has lower registered values for both RI with prolapse and RI with prolapse reduction, suggesting that the patients with POP grade III will have lower RI values after the POP reduction in comparison with the patients with the POP grade IV.

Conclusions
Vascular resistance within the rectal wall is significantly lowered after reduction of POP; therefore, pelvic blood circulation is improved. Also, the greater the POP grade, the greater the resistive index is improved, so the impact the prolapse has on the pelvic circulation is proportional with the severity of the prolapse.
Clinical improvement of the hemorrhoidal disease after POP surgery can suggest that POP is an etiological factor in the development of hemorrhoids and treatment of the prolapse might be sufficient for both pathologies.
Age might also be an important prognostic factor. The higher the age, the more advanced the POP disease might be.
Discussion
Concerning the patients' subjective perception on the clinical impact of the hemorrhoids, our questionnaires showed that more than 50% of the patients that underwent surgery for POP report significant symptom relief for the hemorrhoidal disease after anatomical restoration of the prolapsed uterus.
One of our most important results is that the mean RI of the hemorrhoidal branches is lower when the prolapse is manually reduced. The simple reduction of the prolapse has a visible effect on the rectal arterial velocimetry. The difference has statistical significance, leading to the assumption that, with the reduction of the prolapse, there is significant improvement of the venous flow within the rectal wall. Furthermore, a greater RI improvement is observed after the reduction of a grade IV POP than of grade III. The arterial system is characterized by high degrees of pressure, as opposed to the venous system, which is more distensible. Considering that we can influence the arterial parameters by reducing the prolapse, we can only assume that the impact on venous flow is at least as important.
The rapid improvement of the hemorrhoids suggests that there is an initial pathogenic mechanism which is being reversed. We can, therefore, speculate that there is a dynamic etiological factor involved in the development of the hemorrhoidal disease, which can be represented by the pressure variation of the vascular system.
Surgical reduction of POP can reduce flow resistance within the pelvic circulatory system and can alleviate hemorrhoidal disease. In such cases, we can assume that hemorrhoids should be addressed only after excluding POP or after its correction. We can think of hemorrhoids not only as a single disease, but also as a consequence of another affliction. This can explain hemorrhoidal relapse after its correction, considering that its etiological factor is not removed.
Our study was aimed only at grades III and IV POP. It might be of use to study the impact of lower grades of POP on hemorrhoidal disease. Also, there are other clinical situations that can increase flow resistance in the pelvic circulation, such as pelvic tumors, which should be excluded as well.
Conflict of Interests
The authors report no conflict of interests.
Statement
The aim of this study was to find an explanation for the high incidence of hemorrhoids in female patients with high-grade POP and for the rapid improvement of the hemorrhoidal disease after prolapse surgery.
The study has the following key findings: hemorrhoidal disease improves significantly after POP surgery and venous flow is improved within the rectal wall after the reduction of the prolapse, which indicates that POP can be considered an etiological factor for hemorrhoidal disease.
Our findings can lead to a new approach involving hemorrhoidal treatment in female patients, such as excluding or surgically correcting POP before addressing the hemorrhoidal disease.
Consent
Informed consent and ethics committee approval have been received.
-
References
- 1 Lee KY, Lee JI, Park YY. et al. Hemorrhoids Are Associated with Urinary Incontinence. J Womens Health (Larchmt) 2020; 29 (11) 1464-1468
- 2 Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World J Gastroenterol 2012; 18 (17) 2009-2017
- 3 Sun Z, Migaly J. Review of Hemorrhoid Disease: Presentation and Management. Clin Colon Rectal Surg 2016; 29 (01) 22-29
- 4 Petros PE, Ulmsten UI. An integral theory and its method for the diagnosis and management of female urinary incontinence. Scand J Urol Nephrol Suppl 1993; 153: 1-93
- 5 Paradisi G, Petros P. Cure of hemorrhoids following a TFS posterior sling and TFS perineal body repair—A case report. Pelviperineology 2010; 29: 62-63
- 6 Abendstein B, Petros PE, Richardson PA, Goeschen K, Dodero D. The surgical anatomy of rectocele and anterior rectal wall intussusception. Int Urogynecol J Pelvic Floor Dysfunct 2008; 19 (05) 705-710
- 7 Abendstein B, Brugger C, Furtschegger A, Rieger M, Petros P. Role of the uterosacral ligaments in the causation of rectal intussusception, abnormal bowel emptying and fecal incontinence. A prospective study. Pelviperineology 2015; 34: 2-20
Address for correspondence
Publikationsverlauf
Eingereicht: 25. April 2022
Angenommen: 07. Juni 2022
Artikel online veröffentlicht:
20. Juli 2022
© 2022. Sociedade Brasileira de Coloproctologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Lee KY, Lee JI, Park YY. et al. Hemorrhoids Are Associated with Urinary Incontinence. J Womens Health (Larchmt) 2020; 29 (11) 1464-1468
- 2 Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World J Gastroenterol 2012; 18 (17) 2009-2017
- 3 Sun Z, Migaly J. Review of Hemorrhoid Disease: Presentation and Management. Clin Colon Rectal Surg 2016; 29 (01) 22-29
- 4 Petros PE, Ulmsten UI. An integral theory and its method for the diagnosis and management of female urinary incontinence. Scand J Urol Nephrol Suppl 1993; 153: 1-93
- 5 Paradisi G, Petros P. Cure of hemorrhoids following a TFS posterior sling and TFS perineal body repair—A case report. Pelviperineology 2010; 29: 62-63
- 6 Abendstein B, Petros PE, Richardson PA, Goeschen K, Dodero D. The surgical anatomy of rectocele and anterior rectal wall intussusception. Int Urogynecol J Pelvic Floor Dysfunct 2008; 19 (05) 705-710
- 7 Abendstein B, Brugger C, Furtschegger A, Rieger M, Petros P. Role of the uterosacral ligaments in the causation of rectal intussusception, abnormal bowel emptying and fecal incontinence. A prospective study. Pelviperineology 2015; 34: 2-20