

RSS-Feed abonnieren
DOI: 10.1055/s-0042-1750306
Efficacy of Emergent STA–MCA Bypass for Acute Atherosclerotic ICA Stenosis/Occlusion with Concomitant Chronic Contralateral ICA Occlusion/Stenosis: Two Case Reports
Autor*innen
Funding None.

Abstract
Recombinant tissue-type plasminogen activator with/without endovascular regimen is sometimes not effective for the treatment of acute hemodynamic stroke. Emergent superficial temporal artery-middle cerebral artery (STA–MCA) bypass has been reportedly effective in patients with progressive hemodynamic stroke; however, the effectiveness of urgent STA–MCA bypass for acute internal carotid artery (ICA) stenosis/occlusion with concomitant contralateral chronic ICA stenosis/occlusion, that is considered the worst hemodynamic situations, is unclear. Two cases of acute left ICA stenosis with concomitant right chronic ICA occlusion wherein both developed hemodynamic infarction and were initially treated by maximal medical treatment. Nevertheless, the patients' symptoms had gradually worsened, thus we performed emergency STA–MCA bypass for both cases. Postoperatively, deterioration of imaging and neurological findings was successfully stopped and the patients' condition gradually stabilized. An urgent STA–MCA bypass can be considered as a last resort to prevent progressive neurological deterioration for patients with progressive infarction due to ICA stenosis/occlusion concomitant with contralateral ICA stenosis/occlusion.
Introduction
The safety and efficacy of endovascular mechanical thrombectomy with or without recombinant tissue-type plasminogen activator infusion have already been established for acute embolic major intracranial arterial occlusion.[1] [2] However, it is not necessarily effective for atherosclerotic occlusion. Therefore, maximal medical treatments such as dual antiplatelet therapy, fluid replacement, and even induced hypertension should be administered to overcome hemodynamic ischemia. When symptoms progressively worsen even with maximum treatment, emergent bypass would be the last resort.
Although emergent superficial temporal artery-middle cerebral artery (STA–MCA) bypass for acute-phase progressive stroke due to atherosclerotic internal carotid artery (ICA)/middle cerebral artery (MCA) occlusion has attending innate risks such as worsening cerebral edema and/or hemorrhagic infarction, some reports have demonstrated its effectiveness in reversing or terminating progressive symptoms, even on maximal medical treatment.[3] However, only a few reports have been conducted on emergent STA–MCA bypass in acute atherosclerotic ICA stenosis/occlusion with concomitant chronic contralateral ICA occlusion/stenosis, apparently one of the worst hemodynamic situations.
In this report, we introduce the outline, clinical features, and surgical strategy implemented for two cases with progressive stroke due to ipsilateral acute ICA occlusion/stenosis with concomitant contralateral chronic ICA stenosis/occlusion, which were successfully managed with an emergent STA–MCA bypass during the acute period to prevent the progression of infarction.
Case History
Case 1
A 49-year-old man was referred to our institution with complaints of worsening right-hand clumsiness/gait disturbance due to right hemiparesis with a manual muscle test (MMT) score of 1/5 and complete motor aphasia.
Magnetic resonance imaging (MRI) revealed an acute ischemic lesion in the left premotor cortex on diffusion-weighted imaging (DWI) and contralateral right old prefrontal infarction on fluid-attenuated inversion recovery imaging. Magnetic resonance angiography (MRA) revealed a very faint left intracranial ICA signal and almost no signal from the right intracranial ICA ([Fig. 1]).

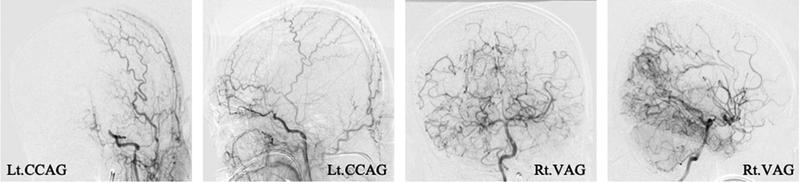
Digital subtraction angiography (DSA) revealed a left ICA occlusion immediately after the ophthalmic artery, possibly due to acute occlusion with engrafted thrombus on the preexisting atherosclerotic severe stenosis and right chronic cervical ICA occlusion. The areas surrounding the bilateral anterior cerebral artery (ACA) and MCA were opacified by crossflow from the left posterior communicating artery and leptomeningeal anastomosis from the bilateral posterior cerebral artery (PCA) ([Fig. 2]).
Maximal medical treatment with argatroban, clopidogrel, and aspirin combination therapy was initiated, in conjunction with edaravone (30 mg twice daily) and sodium dextran sulfate (500 mL daily) injection.
However, the patient's symptoms gradually worsened, and a repeat DWI on day 4 of admission revealed acute ischemic lesions had extended up to the prefrontal cortex and deep white matter ([Fig. 3]). After a thorough discussion, emergent STA–MCA bypass was performed ([Video 1]).
Video 1 We provide a video that shows the actual surgery on a patient who underwent urgent bypass for progressive cerebral infarction with internal carotid artery (ICA) occlusion associated with contralateral ICA occlusion.

Since severe hemodynamic impairment had been expected, edaravone (30 mg) was administered immediately before cross-clumping the recipient artery,[4] and minocycline (200 mg/day for 5 days) was given for neuroprotection perioperatively.[5] The intraoperative mean blood pressure was maintained at 80 to 100% of preoperative blood pressure. Shortening the anastomosing and operation times is also extremely essential during the emergent STA–MCA bypass for patients with contralateral ICA stenosis/occlusion because their ischemic resistance is extremely low. For that purpose, reliable and efficient hand movement during anastomosis is essential. These steps can be viewed on the operative video provided ([Video 1]).
Arterial spin labeling (ASL) MRI on postoperative day (POD) 1 showed increased blood flow on the operated side; however, clinical signs of cerebral hyperperfusion (CH) did not become symptomatic by strictly controlling the systolic blood pressure at less than 130 mm Hg until the ASL findings stabilized on POD 5. Postoperatively, no additional ischemic lesions were observed on repeat DWI, the exacerbation of clinical symptoms ceased, and the patient's condition gradually stabilized.
Approximately 1 month after admission, STA–MCA bypass surgery was also performed for contralateral ICA occlusion. Finally, after rehabilitation, the patient's right hemiparesis recovered from MMT 1/5 to MMT 3/5 with independent/voluntary movement of his right-hand fingers. Additionally, simple spontaneous utterances such as “yes” and “no” were observed, and the patient was transferred to a rehabilitation hospital for further improvement with a modified Rankin Scale (mRS) score of 4. [Fig. 4] shows MRI findings performed immediately before discharge.

Case 2
A 62-year-old man with a history of the occipital artery (OA)–MCA bypass surgery for right ICA occlusion 8 years prior was admitted to our institution with disturbed consciousness, severe dysarthria, and right hemiparesis with an MMT score of 4/5.
Upon presentation (day 0), DWI showed only a faint acute ischemic lesion along the left watershed area and the right old prefrontal infarction, whereas MRA demonstrated an old right ICA occlusion, a severe left C2 stenosis, and a visible distal left MCA signal ([Fig. 5]). On day 1, DSA showed a chronic right ICA occlusion and moderately developed right OA–MCA bypass. However, the right ACA area was poorly opacified in the right common carotid artery angiography and supplied by collateral flow from the right posterior pericallosal artery, indicating the low ischemic resistance of the right cerebellar hemisphere. The left supraclinoid ICA showed severe stenosis with a slightly delayed distal left MCA opacification. Bilateral ACA areas were poorly visualized. On right vertebral angiography, leptomeningeal anastomosis from bilateral PCA perfused the bilateral MCA area only moderately ([Fig. 6]). On day 2, MRA demonstrated progressive worsening of the left ICA stenosis with an extremely poor signal of the distal left MCA ([Fig. 7]), whereas DWI showed only small ischemic lesions scattered along the left watershed.



Besides the usual aspirin and cilostazol therapy, daily injections of argatroban, edaravone (30 mg twice daily), and sodium dextran sulfate (500 mL) were administered. Despite the maximal medical treatment, the patient's clinical symptoms, especially the progressively worsening disturbed consciousness, suggested that the left C2 near the occlusion is in a critical state because of the extremely poor crossflow caused by contralateral chronic ICA occlusion. Therefore, emergent revascularization STA–MCA bypass was conducted on day 3, and perioperative management was administrated similarly as in Case 1.
Postoperatively, the patient's consciousness, hemiparesis, and dysarthria gradually improved. ASL demonstrated focal hyperperfusion around the recipient area of the STA–MCA bypass, although vigorous blood pressure control prevented it to become symptomatic. The patient was discharged after rehabilitation with an mRS 1 and was still due to return for a follow-up visit at the time of this writing. [Fig. 8] shows MRI findings at discharge.

Discussion
The effect of STA–MCA bypass on the management of chronic hemodynamic ischemia has not yet been proven. The Carotid Occlusion Surgery Study (COSS) reported that the STA–MCA bypass is not superior to the best medical treatment because of its high incidences of perioperative complications.[6] [7] [8] However, in Japan, STA–MCA bypass for ICA occlusion, MCA occlusion, or severe stenosis has been proven effective as protection from possible ischemic stroke for some patients who meet the requirements, including decreased vascular reactivity in the acetazolamide test; increased oxygen uptake rate in positron emission tomography (PET), elapsing over 3 months since the last attack; and absence of extensive infarction.[9] The method is still used as a means of preventing ischemic stroke in patients with severe hemodynamic insufficiency.
Apart from the STA–MCA bypass for chronic occlusion, one of the possible indications for emergent STA–MCA bypass might be acute atherosclerotic ICA/MCA occlusion with progressive stroke despite maximal medical treatment and severe hemodynamic insufficiency.[10]
However, urgent bypass surgery for extremely hemodynamically unstable acute cerebral infarction is expected to have a much higher risk of perioperative complications compared with that of chronic preventive bypass surgery such as a COSS candidate. Thus, more cases should be evaluated to elucidate the emergency bypass candidate with a severely impaired hemodynamic situation and in whom the risk of sticking to the best medical treatment outweighs the risk of emergent bypass.[11] [12]
To date, several retrospective case series have described promising results of emergent STA–MCA bypass surgery in patients with progressive symptoms.[13] [14] Kimura et al reported favorable outcomes in a cohort with mild symptoms as indicated by lower preoperative National Institutes of Health Stroke Scale (NIHSS) scores.
Among patients with medically intractable progressive stroke, acute ipsilateral ICA occlusion associated with contralateral chronic ICA occlusion might be the most difficult situation for an emergent STA–MCA bypass.[15] The majority of these patients have more severe cerebral circulatory failure or low cerebrovascular reserve because of the lack of cross-collateral flow; hence, the risk of developing cerebral infarction is higher because of general anesthetic management, temporary clumping of the recipient, and blood pressure control immediately after surgery, among others. Most patients also presented with relatively severe symptoms such as preoperative neurological findings; thus, they tended to have poor clinical outcomes even after an emergent surgery.[3]
To overcome bypass surgery in progressive stroke under a significant hemodynamic insufficiency, some pharmacological affirmative majors that have been reported were followed. Free-radical scavenger (edaravone) was administered immediately before cross-clumping of the recipient artery to prevent CH after carotid endarterectomy, especially with preexisting severe hemodynamic insufficiency.[4] We continued free-radical scavenger infusion for several days postoperatively. Moreover, minocycline (200 mg/day for 5 days), which is reported to alleviate the focal hyperperfusion and clinical symptom after the bypass surgery for moyamoya disease,[5] was administered for neuroprotection perioperatively. Both of our cases showed hyperperfusion in postoperative and preoperative ASL. Hence, although the clinical symptoms remained similar or somewhat worse immediately after surgery, we confirmed that this is due to hyperperfusion and thereby reperfusion itself would be sufficient. Thus, besides the above two antihyperperfusion majors, postoperative blood pressure was maintained as low as less than sBP130. Additionally, a single-agent administration of clopidogrel 75 mL was continued as a perioperative antiplatelet agent.
Moreover, Kobayashi et al[16] reported the outcome of acute STA–MCA bypass for high-grade stenosis in a contralateral ICA or symptomatic ICA occlusion complicated by an occlusive lesion in four patients. All of them underwent emergent STA–MCA bypass because of perfusion that was larger than the infarct area on PET cerebral blood flow and higher brain dysfunctions observed after the onset of minor stroke. According to this report, of the four patients, three (75%) developed perioperative cerebral infarction and two developed postoperative hyperperfusion. Therefore, the incidence of perioperative complications was high. However, each patient had a perioperative cerebral infarction in an area away from the anastomotic site, especially in the ACA area, indicating that the watershed shift might have been generated via a bypass flow competing with a faint antegrade flow that originally existed. Symptoms due to similar ischemic lesions were also identified to be transient and improved in the chronic phase. Thus, although the risk of a minor infarction resulting from hemodynamic changes due to blood flow load exists, the risk of a major hemodynamic infarction caused by surgery under general anesthesia is likely to be low. Hypoperfusion symptoms were also transient, and all of them were improved via strict blood pressure control.
In our two patients, no new developments were observed in the perioperative cerebral infarction, and no postoperative symptomatic hyperperfusion syndromes were observed. Hence, the risk of perioperative complications in acute bypass surgery remains high; however, studies on some cohorts have demonstrated that urgent bypass is superior to medical treatment. No article has reported the outcomes of medical monotherapy for progressive cerebral infarction associated with bilateral ICA occlusion and compared treatment outcomes between medical monotherapy and surgical therapy.[17] [18] Although the kind of cohort suitable for urgent bypass remains unclear, at least in our two patients, cerebral infarction progression was prevented, indicating that the efficacy of an urgent bypass may be superior to conservative treatment by significantly improving the surgical technique and perioperative management.
The unified surgical technique is adopted, not limited to urgent bypass, in our facility, which allows for a stable performance within 5 hours of anesthetic time and 20 minutes of clamping time during inoculation. Regarding the recipient artery, a larger diameter is selected at the frontal lobe in the perisylvian area and the M4 segment on the temporal lobe. Especially for the frontal lobe, the M4 segment toward the frontoparietal lesion is targeted. For the actual surgical technique, refer to the page and video of the surgical procedure. Considering the abovementioned measures, a safer emergent STA–MCA bypass surgery can be performed.
Indications for emergent STA-MCA bypass surgery should be considered when symptoms progress despite maximum medical treatment.
In particular, emergent STA-MCA bypass surgery is not considered dangerous just because of contralateral ICA stenosis/occlusion.
Rather, even with severe hemodynamics, the benefits of emergent STA-MCA bypass surgery may outweigh those of maximum medical treatment.
However, the hemodynamics, indications for each case need to be considered.
Conclusion
An emergent STA–MCA bypass can be considered as a last resort for preventing progressive neurological deterioration in patients with progressive infarction due to ICA stenosis/occlusion concomitant with contralateral ICA stenosis/occlusion.
Given that only two cases had been examined herein, our results cannot be generalized to other patients, suggesting the need for further accumulation of cases.
Conflict of Interest
None declared.
-
References
- 1 Nogueira RG, Jadhav AP, Haussen DC. , et al; DAWN Trial Investigators. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med 2018; 378 (01) 11-21
- 2 Saver JL, Goyal M, Bonafe A. , et al; SWIFT PRIME Investigators. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med 2015; 372 (24) 2285-2295 https://www.nejm.org/doi/10.1056/NEJMoa1415061 Accessed May 4, 2022 10.1056/NEJMoa1415061
- 3 Kimura T, Ichikawa Y, Inoue T. Safety and clinical outcomes of urgent superficial temporal artery-middle cerebral artery bypass-a single-institution retrospective analysis. Acta Neurochir (Wien) 2020; 162 (06) 1325-1331
- 4 Ogasawara K, Inoue T, Kobayashi M, Endo H, Fukuda T, Ogawa A. Pretreatment with the free radical scavenger edaravone prevents cerebral hyperperfusion after carotid endarterectomy. Neurosurgery 2004; 55 (05) 1060-1067
- 5 Fujimura M, Niizuma K, Inoue T. , et al. Minocycline prevents focal neurological deterioration due to cerebral hyperperfusion after extracranial-intracranial bypass for moyamoya disease. Neurosurgery 2014; 74 (02) 163-170 , discussion 170
- 6 Esposito G, Amim-Hangini S, Regli L. Role of and indications for bypass surgery after Carotid Occlusion Surgery Study (COSS). Stroke 2016; 47 (01) 282-290
- 7 EC/IC Bypass Study Group. Failure of extracranial-intracranial arterial bypass to reduce the risk of ischemic stroke. Results of an international randomized trial. N Engl J Med 1985; 313 (19) 1191-1200
- 8 Group EBS. The International Cooperative Study of Extracranial/Intracranial Arterial Anastomosis (EC/IC Bypass Study): methodology and entry characteristics. The EC/IC Bypass Study group. Stroke 1985; 16 (03) 397-406
- 9 Kataoka H, Miyamoto S, Ogasawara K. , et al; JET-2 Investigators. Results of prospective cohort study on symptomatic cerebrovascular occlusive disease showing mild hemodynamic compromise [Japanese Extracranial-Intracranial Bypass Trial (JET)-2 Study]. Neurol Med Chir (Tokyo) 2015; 55 (06) 460-468
- 10 Giuseppe E. , et al. Role of and Indications for Bypass Surgery after Carotid Occlusion Surgery Study (COSS)?.
- 11 Rice CJ, Cho SM, Taqui A. , et al. Early versus delayed extracranial-intracranial bypass surgery in symptomatic atherosclerotic occlusion. Neurosurgery 2019; 85 (05) 656-663
- 12 Yasumichi T, Rihei T, Jyoji N. Indication for acute extracranial -intracranial arterial bypass in middle cerebral artery occlusive disease and its results.
- 13 Choi JH, Park HS. Emergent double-barrel bypass shortly after intravenous administration of recombinant tissue plasminogen activator for acute ischemic stroke. J Cerebrovasc Endovasc Neurosurg 2016; 18 (03) 258-263
- 14 Horiuchi T, Nitta J, Ishizaka S, Kanaya K, Yanagawa T, Hongo K. Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke. Neurosurg Rev 2013; 36 (04) 559-564 , discussion 564–565
- 15 Ishishita Y, Kimura T, Morita A. Urgent superficial temporal artery to middle cerebral artery bypass shortly after intravenous rt-PA. Br J Neurosurg 2012; 26 (05) 773-775
- 16 Shinya K, Tatsuya I, Junta M. Outcomes of STA-MCA bypass for symptomatic internal carotid artery occlusion with a contralateral severe stenotic or occlusive internal carotid artery lesion.
- 17 Lai SL, Chen YC, Weng HH, Chen ST, Hsu SP, Lee TH. Bilateral common carotid artery occlusion–a case report and literature review. J Neurol Sci 2005; 238 1-2 101-104
- 18 Bypass STA-MCA. in Bilateral Carotid Artery Occlusion: Clinical Results and Long-Term Effect on Cerebrovascular Reserve Capacity: Neurological Research. Vol. 16. Accessed May 4, 2022: https://www.tandfonline.com/doi/abs/10.1080/01616412.1994.11740204
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
27. September 2022
© 2022. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Nogueira RG, Jadhav AP, Haussen DC. , et al; DAWN Trial Investigators. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med 2018; 378 (01) 11-21
- 2 Saver JL, Goyal M, Bonafe A. , et al; SWIFT PRIME Investigators. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med 2015; 372 (24) 2285-2295 https://www.nejm.org/doi/10.1056/NEJMoa1415061 Accessed May 4, 2022 10.1056/NEJMoa1415061
- 3 Kimura T, Ichikawa Y, Inoue T. Safety and clinical outcomes of urgent superficial temporal artery-middle cerebral artery bypass-a single-institution retrospective analysis. Acta Neurochir (Wien) 2020; 162 (06) 1325-1331
- 4 Ogasawara K, Inoue T, Kobayashi M, Endo H, Fukuda T, Ogawa A. Pretreatment with the free radical scavenger edaravone prevents cerebral hyperperfusion after carotid endarterectomy. Neurosurgery 2004; 55 (05) 1060-1067
- 5 Fujimura M, Niizuma K, Inoue T. , et al. Minocycline prevents focal neurological deterioration due to cerebral hyperperfusion after extracranial-intracranial bypass for moyamoya disease. Neurosurgery 2014; 74 (02) 163-170 , discussion 170
- 6 Esposito G, Amim-Hangini S, Regli L. Role of and indications for bypass surgery after Carotid Occlusion Surgery Study (COSS). Stroke 2016; 47 (01) 282-290
- 7 EC/IC Bypass Study Group. Failure of extracranial-intracranial arterial bypass to reduce the risk of ischemic stroke. Results of an international randomized trial. N Engl J Med 1985; 313 (19) 1191-1200
- 8 Group EBS. The International Cooperative Study of Extracranial/Intracranial Arterial Anastomosis (EC/IC Bypass Study): methodology and entry characteristics. The EC/IC Bypass Study group. Stroke 1985; 16 (03) 397-406
- 9 Kataoka H, Miyamoto S, Ogasawara K. , et al; JET-2 Investigators. Results of prospective cohort study on symptomatic cerebrovascular occlusive disease showing mild hemodynamic compromise [Japanese Extracranial-Intracranial Bypass Trial (JET)-2 Study]. Neurol Med Chir (Tokyo) 2015; 55 (06) 460-468
- 10 Giuseppe E. , et al. Role of and Indications for Bypass Surgery after Carotid Occlusion Surgery Study (COSS)?.
- 11 Rice CJ, Cho SM, Taqui A. , et al. Early versus delayed extracranial-intracranial bypass surgery in symptomatic atherosclerotic occlusion. Neurosurgery 2019; 85 (05) 656-663
- 12 Yasumichi T, Rihei T, Jyoji N. Indication for acute extracranial -intracranial arterial bypass in middle cerebral artery occlusive disease and its results.
- 13 Choi JH, Park HS. Emergent double-barrel bypass shortly after intravenous administration of recombinant tissue plasminogen activator for acute ischemic stroke. J Cerebrovasc Endovasc Neurosurg 2016; 18 (03) 258-263
- 14 Horiuchi T, Nitta J, Ishizaka S, Kanaya K, Yanagawa T, Hongo K. Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke. Neurosurg Rev 2013; 36 (04) 559-564 , discussion 564–565
- 15 Ishishita Y, Kimura T, Morita A. Urgent superficial temporal artery to middle cerebral artery bypass shortly after intravenous rt-PA. Br J Neurosurg 2012; 26 (05) 773-775
- 16 Shinya K, Tatsuya I, Junta M. Outcomes of STA-MCA bypass for symptomatic internal carotid artery occlusion with a contralateral severe stenotic or occlusive internal carotid artery lesion.
- 17 Lai SL, Chen YC, Weng HH, Chen ST, Hsu SP, Lee TH. Bilateral common carotid artery occlusion–a case report and literature review. J Neurol Sci 2005; 238 1-2 101-104
- 18 Bypass STA-MCA. in Bilateral Carotid Artery Occlusion: Clinical Results and Long-Term Effect on Cerebrovascular Reserve Capacity: Neurological Research. Vol. 16. Accessed May 4, 2022: https://www.tandfonline.com/doi/abs/10.1080/01616412.1994.11740204