

Subscribe to RSS
DOI: 10.1055/s-0042-1744443
Bidirectional Endoscopy—A Trend for Future in COVID Era
Authors

Abstract
Background and Study Aims In the coronavirus disease 2019 (COVID-19) pandemic, patients undergoing esophagogastroduodenoscopy (EGD) and colonoscopy on the same day (bidirectional endoscopy [BDE]) have increased. The aims of the study were to compare the procedure times, benefits, and safety of same-day BDE and conventional serial endoscopic examination (SEE).
Patients and Methods All the patients undergoing evaluation with either BDE or SEE were prospectively enrolled at Ramaiah Medical College and Hospitals, Bangalore, from 1st December 2020 to 31st May 2021. EGD was immediately followed by colonoscopy in BDE. In SEE, EGD was followed by colonoscopy in 1 or 2 days. Clinical data and results were collected and evaluated.
Results Two hundred consecutive patients who consented for BDE were enrolled in the study. The mean ± standard deviation (range) age of the patients was 45 ± 14.5 (22–60) years. Majority (124 [62%]) were men. The outcome measures of Boston Bowel Preparation Scale with the excellent/good preparation score and polyp detection rate were similar in both groups (p = 0.4). The total procedure time was significantly higher in the SEE group than in the BDE (p < 0.001). There were no adverse events noted in the study. The overall patient experience and satisfaction were higher in BDE than in SEE without any difference in the quality of the procedures (p < 0.001). Patients with weight loss and anemia were more likely to have a positive test result than the patients with abdominal pain and diarrhea.
Conclusions In conclusion, same-day BDE is advised for patients with anemia and weight loss which can reduce the number of hospital visits and improve patient satisfaction in COVID times.
Introduction
The coronavirus disease (COVID-19) pandemic has changed endoscopic practice with the need for COVID-19 testing, screening questionnaire, and use of personal protective equipment with the hope for the “old normal” as a distant dream.[1] Esophagogastroduodenoscopy (EGD) can be a covert vector for the spread of COVID-19 infection as it generates aerosols or by direct contact with body and fecal fluids. The use of a dual-purpose easily assembled aerosol chamber during EGD provides adequate safety to both patients and health care personnel.[2] Same-day bidirectional endoscopy (BDE) is a combination of EGD and colonoscopy performed on the same day. BDE is useful for overlapping indications, such as evaluation of anemia, positive stool occult blood test, gastrointestinal bleeding, weight loss, abdominal pain, and patients requiring EGD for upper gastrointestinal symptoms and simultaneously undergoing colon cancer screening.[3] [4] Bundling both EGD and colonoscopy on the same day is convenient for patients, reduces the number of hospital visits, medical costs, and missed workdays.[5] In same-day BDE, EGD followed by colonoscopy is better sequence due to lower sedative dose, faster recovery time, and air insufflation in colonoscopy which could lead to reduced tolerance to subsequent EGD.[6] Same-day BDE accounts only for 10% of all cases referred for gastrointestinal EGDs in a national EGD database.[3] Anecdotally, many patients and endoscopists prefer to have both procedures performed on the same day.[7] Stress-sensitive gut–brain disorders like functional dyspepsia and irritable bowel syndrome had increased hospital visits due to the deterioration of gastrointestinal symptoms noted in the COVID-19 pandemic.[8]
There are no published studies comparing simultaneous EGD and colonoscopy procedures during COVID time. This study aims to determine differences in procedure times between simultaneous EGD–colonoscopy (BDE) and conventional serial EGD–colonoscopy examination (SEE) as an alternative during the COVID-19 era and to assess the benefits and safety of BDE.
Methods
Data were collected prospectively for all the patients who underwent BDE and SEE at M.S. Ramaiah Medical College and Hospitals, Bengaluru, between 1st December 2020 and 31st May 2021. The study was approved by Institute Ethical Committee.
The following data points were captured: gender, age, comorbidities, indications and findings on BDE and SEE, dose of midazolam used, and follow-up data on patient satisfaction. The patients underwent the procedures after required informed consent. All the procedures were performed by the same endoscopic team under supervised sedation with midazolam or total intravenous anesthesia (TIVA) using propofol or fentanyl.
Sample Size
The present study was based on the EGD and colonoscopy time observed in the study by Lucendo et al, to get 80% power, 95% confidence level, and 5% error with 0.40 effect size, a minimum sample size of 98 subjects was required.[6]
Subjects
Study participants were prospectively categorized into two groups. Group A (BDE) or “simultaneous” group consisted of 100 consecutive patients each who underwent same-day EGD and colonoscopy. Group B (SEE) or “serial” group consisted of 100 consecutive patients who underwent procedures on different days—a day or two apart was used for comparison. The selection of patients is mentioned in the flow diagram ([Fig. 1]).

During the same time period, a total of 1924 EGDs and 575 colonoscopies were performed. BDEs comprised 249 (9.9%) of total procedures. During the same time period, in 2019, out of 2,700 EGDs and 640 colonoscopies only 85(2.6%) of procedures were BDEs.
All the patients had gastroenterology consultation and were judged to qualify for the performance of BDE/SEE as part of their diagnostic evaluation. The procedure indications were either abdominal pain, iron deficiency anemia (IDA), chronic diarrhea, or gastrointestinal bleeding. Inclusion criteria were as follows: age > 18 years and less than 60 years, scheduled EGD and a colonoscopy on the same consultation, and use of conscious sedation with midazolam or TIVA with propofol and/or fentanyl. All the procedures were done in the EGD suite only as outpatients. Exclusion criteria included procedures done in the intensive care unit, procedures at least 3 days apart, therapeutic procedures like endoscopic variceal band ligation or dilation, pregnant women, known obstructive/cancerous lesions, previous surgery of the digestive tract, refusal to participate, and those with no decision-making capacity.
The endoscopic procedures as EGD and colonoscopy were performed during the same sedation time by two final-year gastroenterology trainees. All the personnel had adequate personal protective equipment with the N95 mask. All the patients were negative for COVID-19 on real-time reverse transcriptase polymerase chain reaction (RTPCR) test performed less than 48 hours prior to the endoscopic procedure. The patients were scheduled for a time slot, and social distancing was followed. The EGDs were performed using an aerosol chamber to maintain the barrier between the patient and health care personnel.
Procedure
BDE/SEE was performed using Olympus GIF-H180 and CF Q 180A scopes. All the patients had clear liquid diet (glucose, lime juice, and coconut water) the previous night of the scheduled colonoscopy procedure. In SEE and BDE, all the patients had consumed the standard 2 L of polyethylene glycol (PEG) between 6:00 and 8:00 am on the day of procedure. In BDE, all the patients were nil by mouth for 4 hours prior to EGD. The sequence for BDE/SEE was EGD followed by colonoscopy. A complete upper endoscopic examination was performed and included the inspection of the esophagus, stomach with retro-flexion, and examination of the duodenum with photo documentation. Colonoscopy was also considered complete if the base of the cecum was reached with the identification of landmarks, including the appendicular orifice and the ileocecal valve with photo documentation. All procedures used room air for insufflation rather than carbon dioxide. Patients were placed in the left lateral decubitus position, under midazolam/TIVA, and were continuously monitored by the EGD nurse. Post-procedure, patients were transferred to the recovery room, and post-procedural symptoms were recorded by the recovery room nurse.
Outcome Measures
The primary outcome was to compare the mean difference in procedure times between the two study groups. The secondary outcomes were mucosal visualization on the procedures and patient satisfaction at the end of both procedures.
EGD time: Time elapsed in minutes between the insertion of the gastroscope into the mouth and the extraction from the mouth/completion of the procedure.
Colonoscopy time: Time elapsed in minutes between the insertion of the colonoscope into the lower rectum and the extraction from the lower rectum/completion of the procedure.
Total procedure time: Time elapsed in minutes between the start of the EGD procedure and the completion of colonoscopy procedure on the procedure table and the waiting time in the EGD suite.
Boston Bowel Preparation Scale (BBPS): BBPS was used to score the level of colon cleansing. In the study, excellent bowel preparation was defined as the BBPS score of 8 or higher, good preparation as a total score of 7, fair preparation as a total score of 6, and a total score of 5 or less indicates poor preparation.
Cecal intubation rate: The total number of times the colonoscope reached cecum and the completion of the procedure.
Post-procedure symptoms survey: Nausea, drowsiness, abdominal bloating, dizziness, and tolerability were scored by patients using a 10 cm visual analog scale from 1 to 10 (1: none and 10: extreme). The discomfort perceived by the patient as assessed by the endoscopist was rated after every EGD and recorded on a 10-point Likert scale: 0: no discomfort; 5: need for incremental dose of sedation; and 10: termination of the procedure.
Statistical Analysis
Data were reported as mean ± standard deviation (SD) for continuous variables and frequencies (percentages) for categorical variables. All analyses were performed using the SPSS statistical analysis software version 17.0 (SPSS Inc., Chicago, IL, United States). The chi-square test was used to compare the findings between the two procedures. All tests were two-sided, and statistical significance was defined as a p-value less than 0.05.
Results
Two hundred and forty-nine BDE procedures were performed throughout the study period. The flow chart depicts the final number included in the study ([Fig. 1]). The demographic data of the study group are presented in [Table 1]. The mean ± SD (range) age of the patients was 45 ± 14.5 (22–60) years. Majority (124 [62%]) were men. There were no significant differences between the study groups regarding the age, gender, diabetes, indications for procedure (abdominal pain, anemia, diarrhea, and weight loss), and the findings on EGD, colonoscopy, and both procedures ([Table 1]).
Abbreviations: BDE, bidirectional endoscopy; SD, standard deviation; SEE, serial endoscopic examination; TIVA, total intravenous anesthesia.
[Table 2] summarizes the procedure-related factors between the two groups. The usage of midazolam, TIVA sedation, and performance of either gastric or colonic biopsies were similar in both groups. The majority of the BDE procedures (82%) and serial group procedures (64%) were done in the forenoon. The most common endoscopic findings were gastroduodenal erosions in 118, followed by reflux esophagitis in 29, peptic ulcers in 10, and malignancy in three patients. The most common colonoscopic findings were terminal ileal ulcers in 40 patients, followed by polyps in 26, colonic ulcers/erosions in 24, and diverticulosis in 10 patients.
Abbreviations: BDE, bidirectional endoscopy; NS: not significant; SEE, serial endoscopic examination; TIVA, total intravenous anesthesia.
[Table 3] shows the quality of endoscopic procedures between the study groups. Cecal intubation was achieved in all the patients in both groups. BBPS with the excellent/good preparation score was similar in both groups. There was no significant difference in polyp detection rate, complications, and standard reporting format for the procedure. There were no procedure or sedation-related complications in any patient in both groups.
Abbreviations: BDE, bidirectional endoscopy; NS: not significant; SEE, serial endoscopic examination.
There was no gastric fluid residue even after 4 hours after the colonoscopy preparation in BDE patients. During the study period, none of the health care staff in the EGD suite turned COVID positive with the use of an aerosol chamber.
[Table 4] shows the mean procedure times between the two groups. The duration required to complete EGD and colonoscopy was similar between the two groups. The total procedure time was significantly higher in the serial group than BDE.
Abbreviations: BDE, bidirectional endoscopy; SD, standard deviation; SEE, serial endoscopic examination.
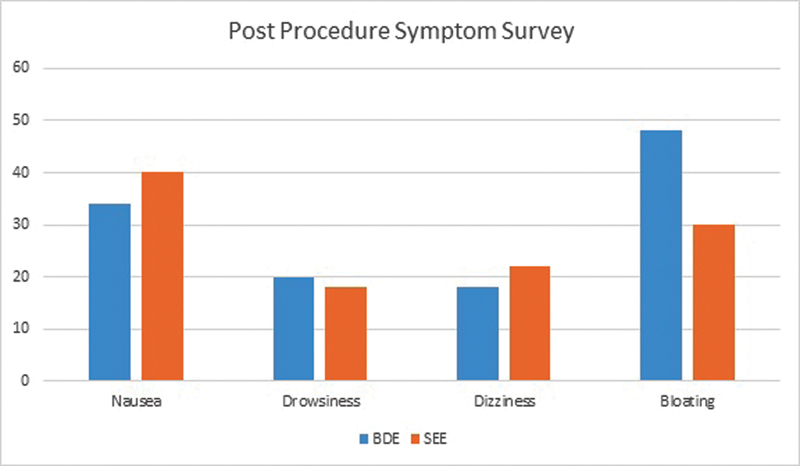
[Table 5] and [Fig. 2] summarize the results of the questionnaire of the post-procedure symptom survey. The subjective discomfort/pain and experience of the symptoms of nausea, drowsiness, dizziness, and bloating were scored by the patient. The subjective discomfort scores were similar between the two groups for both EGD and colonoscopy. Bloating was more common in BDE (48) than in SEE (30). But overall discomfort assessments by both the patients and endoscopist were significantly higher in the serial procedure group (SEE) than in the simultaneous group (BDE).
Abbreviations: BDE, bidirectional endoscopy; SD, standard deviation; SEE, serial endoscopic examination.
[Table 6] displays the prevalence of findings on EGD, colonoscopy, and both procedures. Patients presenting with weight loss and anemia were more likely to have a finding on BDE/SEE than the patients with abdominal pain and diarrhea.
Discussion
Gastrointestinal EGD is a high-risk procedure for COVID-19 transmission due to close proximity of patient, generation of aerosols, contact with contaminated equipment, and suctioning of body fluids. The risk of transmission can be reduced by the screening of the patients, use of double surgical masks, and strict high-level disinfection and reprocessing guidelines.[9]
In the consecutive sample of 200 patients with gastrointestinal symptoms, there was no increased procedure or sedation risk when both procedures were performed either simultaneously or serially. In our study, 9.9% of the total procedures underwent BDE which has improved patient convenience. The study group had a specific clinically important indication for BDE. The most common reasons for BDE were abdominal pain, anemia, weight loss, or diarrhea.
While abdominal pain and diarrhea (116 patients) were the most common presenting symptoms, significant findings on EGDs were noted in those presenting with either weight loss or anemia. American Gastroenterology Association (AGA) guidelines strongly recommend to perform BDE on asymptomatic men and post-menopausal women with IDA. AGA also suggests BDE over iron replacement alone in asymptomatic premenopausal women with IDA (ferritin cut off <45 ng/mL).[10] Patients with either gastrointestinal bleeding or IDA are more likely to have clinical findings on BDE. But the utility of BDE in other indications has remained controversial. Several studies recommend benefits of performing EGD in patients with positive fecal occult blood and a negative colonoscopy.[3]
The diagnostic yield of BDE in various studies varies between 63 and 68% with 40% yield in either EGD or colonoscopy alone. Approximately, 10% of patients have both upper and lower lesions at the same time.[11] In the current study, if colonoscopy was negative, the yield of EGD was approximately 51 to 80% and 22 to 62% in colonoscopy with negative findings in EGD. Also, the diagnostic yield of BDE with findings on both EGD and colonoscopy was noted in 40 (20%) cases and normal findings were noted in 20 (10%) of cases. Forty (10%) of patients had lesions, and 20 (10%) had no lesions in both upper and lower lesions at the same time.
In studies, the procedural time of EGD and colonoscopy and total procedural time (combination of EGD and colonoscopy times) did not show any statistical difference.[5] In our study, there was no difference in EGD and colonoscopy procedural times. The total procedural time was significantly different in our study due to the inclusion of procedural waiting time.
In same-day BDE, EGD first followed by colonoscopy is the favored order of the procedures due to lower discomfort scores in earlier meta-analysis.[5] Abdominal bloating caused by colonoscopy first in BDE might reduce tolerance to subsequent EGD.[12] In our study, all the procedures in BDE were performed as EGD first with an aerosol chamber followed by colonoscopy. During the procedures, room air was used to expand/inflate the bowel instead of carbon dioxide though the latter has revealed lesser post-procedure patient discomfort.
The patient discomfort scores in BDE in earlier studies varied from 0.6 to 4.7 as compared with 1.2 to 2.5 score in this study.[5] Given the absence of guidelines in COVID time, we undertook the current study and proved that same-day BDE is better tolerated than serial BDE with decreased total procedure time and increased patient satisfaction/comfort.
In a study, bundling of both procedures encompassed only 11.2% of total procedures. But the non-bundled procedures were associated with increased costs related to physician, sedation, and loss of workdays for the patient. They documented lower prevalence of same-day BDE in patients with higher comorbidities.[13] The BDE is usually done in EGD units with under-anesthesia procedures (as both can be done under the same sedation), blood product transfusion in patients with blood dyscrasias, and positivity for retrovirus (performed at the end of the day, followed by sterilization of the room). Similar to retroviral cases, patients during the COVID-19 pandemic should also be considered for BDE to reduce exposure to health care providers. A negative COVID RTPCR within 48 hours is a prerequisite for the EGD procedure, and BDE is better as RTPCR need not be repeated as the procedures are done on the same day.
In our study, there were no adverse events either due to the procedure or sedation as the mean age group was 45 years. In same-day BDE, old age >70 years and the addition of pethidine with midazolam were independent risk factors for hypoxia. The use of midazolam alone and performing EGD and colonoscopy on separate days in elderly might be a better option.[14]
The major strength of the study is that in COVID times the prospective performance of both procedures on the same day has not been documented in previous studies. The limitations of the study are similar to any single-center study: small sample size, selection bias, non-blinding of the endoscopist, zero complication rate, dosage of anesthetic drugs, and lack of randomization. The procedures were performed in all COVID-19-negative patients, and the main focus was on EGD findings, use of an aerosol chamber, and patient satisfaction.
Conclusions
In conclusion, the same-day BDE is advised for patients with anemia and weight loss which can reduce the number of hospital visits and improve patient satisfaction in COVID times.
Conflict of Interest
None declared.
-
References
- 1 Pohl H. Endoscopy during COVID—what have we learned?. Endoscopy 2021; 53 (02) 171-172
- 2 Goenka M, Afzalpurkar S, Jajodia S, Shah BB, Tiwary I, Sengupta S. Dual purpose easily assembled aerosol chamber designed for safe endoscopy and intubation during the COVID pandemic. VideoGIE 2020; 5 (11) 505-506
- 3 Urquhart J, Eisen G, Faigel DO, Mattek N, Holub J, Lieberman DA. A closer look at same-day bidirectional endoscopy. Gastrointest Endosc 2009; 69 (02) 271-277
- 4 Zuckerman G, Benitez J. A prospective study of bidirectional endoscopy (colonoscopy and upper endoscopy) in the evaluation of patients with occult gastrointestinal bleeding. Am J Gastroenterol 1992; 87 (01) 62-66
- 5 Choi GJ, Oh HC, Seong HK, Kim JW, Ko JS, Kang H. Comparison of procedural sequence in same-day bidirectional endoscopy: a systematic review and meta-analysis. Korean J Intern Med (Korean Assoc Intern Med) 2020; 35 (02) 331-341
- 6 Lucendo AJ, Arias Á, González-Castillo S. et al. Same-day bidirectional endoscopy with nonanesthesiologist administration of propofol: safety and cost-effectiveness compared with separated exams. Eur J Gastroenterol Hepatol 2014; 26 (03) 301-308
- 7 Cho JH, Kim JH, Lee YC, Song SY, Lee SK. Comparison of procedural sequences in same-day bidirectional endoscopy without benzodiazepine and propofol sedation: starting at the bottom or the top. J Gastroenterol Hepatol 2010; 25 (05) 899-904
- 8 Oshima T, Siah KTH, Yoshimoto T. et al. Impacts of the COVID-19 pandemic on functional dyspepsia and irritable bowel syndrome: A population-based survey. J Gastroenterol Hepatol 2021; 36 (07) 1820-1827
- 9 Rana SS. Risk of COVID-19 transmission during gastrointestinal endoscopy. J Digest Endosc. 2020; 11 (01) 27-30
- 10 Ko CW, Siddique S, Patel A. et al. Gastrointestinal evaluation of iron deficiency anaemia. Gastroenterology 2020; 159: 1096
- 11 Ketz F, Buisson A, Levassort M, Pautas É. Bidirectional endoscopy in the assessment of iron deficiency in the elderly. Gériatr Psychol Neuropsychiatr Vieil 2021; (e-pub ahead of print)
- 12 Kurien M, Din S, Dear KL, Elphick DA. Same day bidirectional endoscopy—does the order of the procedures matter?. Gut 2011; 60: A192
- 13 El-Serag HB, Xu F, Biyani P, Cooper GS. Bundling in medicare patients undergoing bidirectional endoscopy: how often does it happen?. Clin Gastroenterol Hepatol 2014; 12 (01) 58-63
- 14 Nishizawa T, Sakitani K, Suzuki H. et al. Adverse events associated with bidirectional endoscopy with midazolam and pethidine. J Clin Biochem Nutr 2020; 66 (01) 78-81
Address for correspondence
Publication History
Article published online:
05 July 2022
© 2022. Society of Gastrointestinal Endoscopy of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Pohl H. Endoscopy during COVID—what have we learned?. Endoscopy 2021; 53 (02) 171-172
- 2 Goenka M, Afzalpurkar S, Jajodia S, Shah BB, Tiwary I, Sengupta S. Dual purpose easily assembled aerosol chamber designed for safe endoscopy and intubation during the COVID pandemic. VideoGIE 2020; 5 (11) 505-506
- 3 Urquhart J, Eisen G, Faigel DO, Mattek N, Holub J, Lieberman DA. A closer look at same-day bidirectional endoscopy. Gastrointest Endosc 2009; 69 (02) 271-277
- 4 Zuckerman G, Benitez J. A prospective study of bidirectional endoscopy (colonoscopy and upper endoscopy) in the evaluation of patients with occult gastrointestinal bleeding. Am J Gastroenterol 1992; 87 (01) 62-66
- 5 Choi GJ, Oh HC, Seong HK, Kim JW, Ko JS, Kang H. Comparison of procedural sequence in same-day bidirectional endoscopy: a systematic review and meta-analysis. Korean J Intern Med (Korean Assoc Intern Med) 2020; 35 (02) 331-341
- 6 Lucendo AJ, Arias Á, González-Castillo S. et al. Same-day bidirectional endoscopy with nonanesthesiologist administration of propofol: safety and cost-effectiveness compared with separated exams. Eur J Gastroenterol Hepatol 2014; 26 (03) 301-308
- 7 Cho JH, Kim JH, Lee YC, Song SY, Lee SK. Comparison of procedural sequences in same-day bidirectional endoscopy without benzodiazepine and propofol sedation: starting at the bottom or the top. J Gastroenterol Hepatol 2010; 25 (05) 899-904
- 8 Oshima T, Siah KTH, Yoshimoto T. et al. Impacts of the COVID-19 pandemic on functional dyspepsia and irritable bowel syndrome: A population-based survey. J Gastroenterol Hepatol 2021; 36 (07) 1820-1827
- 9 Rana SS. Risk of COVID-19 transmission during gastrointestinal endoscopy. J Digest Endosc. 2020; 11 (01) 27-30
- 10 Ko CW, Siddique S, Patel A. et al. Gastrointestinal evaluation of iron deficiency anaemia. Gastroenterology 2020; 159: 1096
- 11 Ketz F, Buisson A, Levassort M, Pautas É. Bidirectional endoscopy in the assessment of iron deficiency in the elderly. Gériatr Psychol Neuropsychiatr Vieil 2021; (e-pub ahead of print)
- 12 Kurien M, Din S, Dear KL, Elphick DA. Same day bidirectional endoscopy—does the order of the procedures matter?. Gut 2011; 60: A192
- 13 El-Serag HB, Xu F, Biyani P, Cooper GS. Bundling in medicare patients undergoing bidirectional endoscopy: how often does it happen?. Clin Gastroenterol Hepatol 2014; 12 (01) 58-63
- 14 Nishizawa T, Sakitani K, Suzuki H. et al. Adverse events associated with bidirectional endoscopy with midazolam and pethidine. J Clin Biochem Nutr 2020; 66 (01) 78-81