

Subscribe to RSS
DOI: 10.1055/s-0042-1744440
Penile Ulcer as the Unusual Initial Presentation of Nasal NK/T Cell Lymphoma
Authors

Abstract
Extranodal natural killer (NK)/T cell lymphoma is a highly aggressive non-Hodgkin lymphoma that predominantly affects the upper aerodigestive tract. The nasal type accounts for ∼80% of cases of NK/T cell lymphomas. In advanced stages, the disease can disseminate to various sites such as skin, testis, eyes, gastrointestinal tract, and soft tissue. NK/T cell lymphoma presenting as lesion in penis is extremely rare. While reviewing the published literature, we found only three reported cases of NK/T cell lymphoma involving the penis. Among them, none was primary NK/T cell lymphoma of penis. We report a 60-year-old NK/T cell lymphoma patient who presented with destructive penile ulcer as the initial presenting symptom, who subsequently was found to have a nasal mass also with features of NK/T cell lymphoma. He underwent partial penectomy elsewhere and chemotherapy with steroid, methotrexate, ifosfamide, L-asparaginase, and etoposide protocol was given.
Key Message
Nasal natural killer (NK)/T cell presenting as penile lesion is an extremely unusual initial manifestation, and to our knowledge this is the first case to be reported from India. To conclude, it is imperative for the pathologists and the oncologists to rule out occult nasal lesion in every case of extranasal, extranodal NK/T cell lymphoma (ENKTL) before labeling it as primary ENKTL.
Introduction
NKTL, nasal type, is highly aggressive non-Hodgkin lymphoma that almost always has an extranodal presentation. It accounts for 5% of all lymphoid neoplasms and less than 10.4% of all T cell lymphomas.[1] [2] Extranasal sites of involvement are skin, testis, eyes, gastrointestinal tract, adrenal glands, lung, liver, spleen, breast, and central nervous system.[1] [3] Penile involvement whether primary or secondary is extremely rare and seldom reported in the literature. Only three cases have been reported worldwide in English literature till date and we report the fourth case of NKTL with penile involvement.
Case Presentation
A 60-year-old male patient presented with a penile ulcer for which he underwent biopsy followed by partial penectomy elsewhere ([Fig. 1A]).

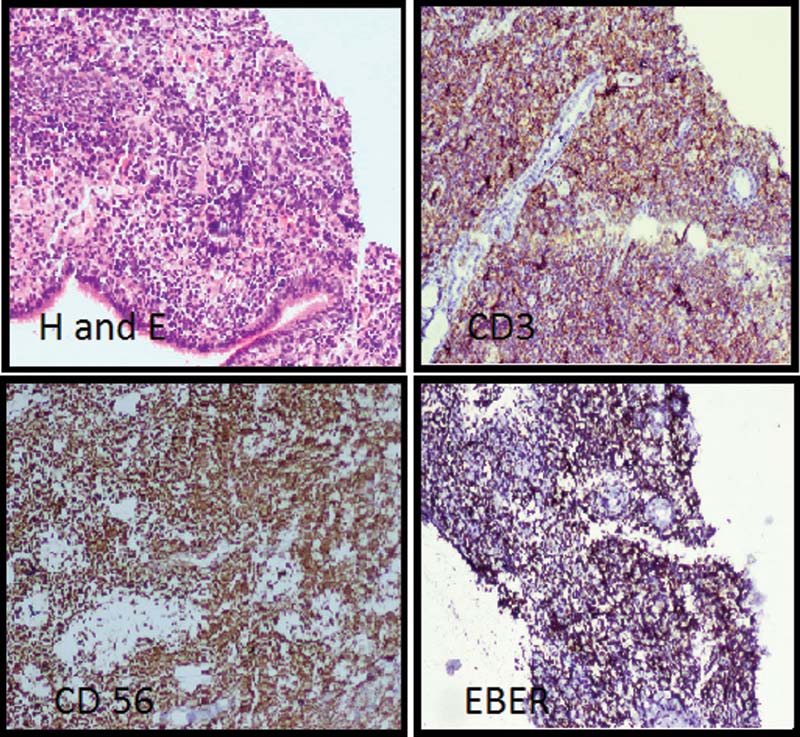
He had normal biochemical and hematological parameters, and general examination was otherwise unremarkable. The slides and the paraffin blocks of the lesion were submitted for review. Microscopic examination showed a neoplasm composed of small-to-medium sized tumor cells with irregular nuclei expressing leukocyte common antigen, CD3, CD56, cytotoxic granule-associated protein, granzyme B, and nuclear labeling for Epstein–Barr virus (EBV) encoded RNA by in situ hybridization. Proliferation index with Ki 67 was found to be 70% ([Fig. 1B–F]).
A diagnosis of ENKTL of the penis was rendered. The patient during the postoperative period complained of nasal obstruction, epistaxis, and blurred vision. Contrast-enhanced computed tomography of paranasal sinuses and magnetic resonance imaging brain and orbit revealed a lesion involving bilateral nasal cavity and sinuses with extension into bilateral orbits ([Fig. 2]).

Biopsy of the nasal lesion showed immunomorphology similar to the penile lesion ([Fig. 3]).
Bone marrow aspiration showed no involvement by lymphoma. A final diagnosis of primary nasal NKTL with penile involvement was made. An informed consent was taken from the patient for this case report. Patient received chemotherapy based on steroid, methotrexate, ifosfamide, L-asparaginase, and etoposide protocol and was lost to follow-up.
Discussion
Primary extranodal lymphoma is uncommon in the urogenital system with only a handful of cases being reported in the literature; however, penile involvement from systemic malignant lymphoma has frequently been reported. Lymphomatous involvement of penis has been more commonly seen in different subtypes of B cell type of non-Hodgkin lymphomas, Hodgkin lymphomas and very rarely proved to be of T cell origin.[4] Diffuse large B cell lymphomas form the major group among the penile B cell non-Hodgkin lymphomas. T cell lymphomas most commonly involving the penis are peripheral T cell lymphomas, not otherwise specified followed by anaplastic large cell lymphoma.[1] [5]
ENKTL belongs to mature T and NK cell neoplasms. Median age is 45 to 54 years with males affected more than females. It is more prevalent in Asians and the indigenous population of Mexico, Central and South America. ENKTL is a rare aggressive malignancy and has a strong association with EBV infection. The World Health Organization classification recognizes two main categories of NK cell-derived neoplasms, namely, ENKTL and nasal type and aggressive NK cell leukemia. Nasal NKTL almost always has an extranodal presentation. Nodal NKTL is very rare.[6] [7] Eighty percent of all NKTL arises from the upper aerodigestive tract. Bone marrow involvement occurs in less than 10% of patients. Penile involvement by lymphoma is extremely rare and primary penile NKTL is never reported in literature. ENKTL with small cells or mixed cell population accompanied by heavy infiltration of inflammatory cells may mimic an inflammatory process.[1] PubMed search identified 35 cases of penile lymphomas of which 22 were B cell type, 13 were T cell type, and among them only 3 were ENKTL secondarily involving the penis.
Conclusion
This case demonstrated a nasal-type NKTL presenting with an extremely unusual initial manifestation as a penile ulcer and to our knowledge not described earlier from India. It is imperative for the pathologists and the oncologists to rule out occult nasal lesion in every case of extranasal ENKTL before labeling it as primary ENKTL.
Conflict of Interest
Informed consent has been taken from the patient for the figure 2.
-
References
- 1 Swerdlow SH, Campo E, Harris NL. et al. WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues 2017, vol. 2. Revised 4th edition.. Lyon: IARC; 2017
- 2 Savage NM, Johnson RC, Natkunam Y. The spectrum of lymphoblastic, nodal and extranodal T-cell lymphomas: characteristic features and diagnostic dilemmas. Hum Pathol 2013; 44 (04) 451-471
- 3 Wang X, Gong Z, Li SX, Yan W, Song Y. Extranodal nasal-type natural killer/T-cell lymphoma with penile involvement: a case report and review of the literature. BMC Urol 2017; 17 (01) 77
- 4 Gallardo F, Pujol RM, Barranco C, Salar A. Progressive painless swelling of glans penis: uncommon clinical manifestation of systemic non-Hodgkin's lymphoma. Urology 2009; 73 (04) 929.e3-929.e5
- 5 Li Y, Fu X, Wu J. et al. Penile metastasis secondary to nasal-type extranodal natural killer/T-cell lymphoma: a case report and review of the literature. Oncol Lett 2018; 15 (05) 8034-8038
- 6 Gill H, Liang RH, Tse E. Extranodal natural-killer/t-cell lymphoma, nasal type. Adv Hematol 2010; 2010: 627401
- 7 Kwong YL, Kim WS, Lim ST. et al. SMILE for natural killer/T-cell lymphoma: analysis of safety and efficacy from the Asia Lymphoma Study Group. Blood 2012; 120 (15) 2973-2980
Address for correspondence
Publication History
Article published online:
09 June 2022
© 2022. Nitte (Deemed to be University). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Swerdlow SH, Campo E, Harris NL. et al. WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues 2017, vol. 2. Revised 4th edition.. Lyon: IARC; 2017
- 2 Savage NM, Johnson RC, Natkunam Y. The spectrum of lymphoblastic, nodal and extranodal T-cell lymphomas: characteristic features and diagnostic dilemmas. Hum Pathol 2013; 44 (04) 451-471
- 3 Wang X, Gong Z, Li SX, Yan W, Song Y. Extranodal nasal-type natural killer/T-cell lymphoma with penile involvement: a case report and review of the literature. BMC Urol 2017; 17 (01) 77
- 4 Gallardo F, Pujol RM, Barranco C, Salar A. Progressive painless swelling of glans penis: uncommon clinical manifestation of systemic non-Hodgkin's lymphoma. Urology 2009; 73 (04) 929.e3-929.e5
- 5 Li Y, Fu X, Wu J. et al. Penile metastasis secondary to nasal-type extranodal natural killer/T-cell lymphoma: a case report and review of the literature. Oncol Lett 2018; 15 (05) 8034-8038
- 6 Gill H, Liang RH, Tse E. Extranodal natural-killer/t-cell lymphoma, nasal type. Adv Hematol 2010; 2010: 627401
- 7 Kwong YL, Kim WS, Lim ST. et al. SMILE for natural killer/T-cell lymphoma: analysis of safety and efficacy from the Asia Lymphoma Study Group. Blood 2012; 120 (15) 2973-2980