Keywords
MRI - great toe - thumb - hallucis - pollicis
Introduction
With evolution, quadrupeds progressed to develop two hands and two feet. Driven by
functional necessity, thumb evolved to become opposable for maintaining hand dexterity,
and great toe evolved to optimize weight bearing, balance, and bipedal locomotion.[1] Therefore, there are anatomical tendoligamentous modifications at the level of carpometacarpal
(CM) joint and metacarpophalangeal (MCP) of thumb compared with tarsometatarsal (TM)
joint, and metatarsophalangeal (MTP) joint of great toe. Understanding the anatomical
modifications is essential to analyze the anatomy and biomechanics of these joint
on magnetic resonance imaging (MRI) that will aid in comprehensive evaluation of the
patterns of injury in these joints.
In addition to limited range of movements in the joints of great toe, another major
difference between great toe and thumb is that the coronal plane of thumb is nearly
at right angle to that of the rest of the fingers and rotated medially, whereas the
great toe lies in the same coronal plane as the rest of the toe[2] ([Fig. 1]).
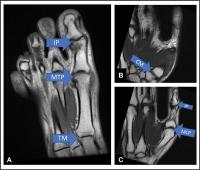 Fig. 1 Overview of the joints of great toe and thumb. (A) Axial T1-weighted (T1W) magnetic resonance (MR) image shows that the great toe lies
in the same plane as the rest of the toe. The tarsometatarsal (TM) joint, metatarsophalangeal
(MTP) joint, and interphalangeal (IP) joint are marked. (B and C). Serial sagittal T1W MR image of the thumb shows that the thumb lies at almost ninety
degrees to the plane of the rest of the fingers and is rotated medially. The first
carpometacarpal (CM) joint, metacarpophalangeal (MCP) joint, and IP joint are marked.
Fig. 1 Overview of the joints of great toe and thumb. (A) Axial T1-weighted (T1W) magnetic resonance (MR) image shows that the great toe lies
in the same plane as the rest of the toe. The tarsometatarsal (TM) joint, metatarsophalangeal
(MTP) joint, and interphalangeal (IP) joint are marked. (B and C). Serial sagittal T1W MR image of the thumb shows that the thumb lies at almost ninety
degrees to the plane of the rest of the fingers and is rotated medially. The first
carpometacarpal (CM) joint, metacarpophalangeal (MCP) joint, and IP joint are marked.
In the current pictorial review, we will illustrate the radiological anatomy of thumb
and great toe on 3T MRI. The capsuloligamentous anatomy and tendinous attachments
will be described at the level of TM/CM joint, MTP/MCP, and interphalangeal (IP) joints
highlighting similarities and dissimilarities at each level.
For the great toe MRI, the patient is placed in supine position, the plantar surface
of foot flat against bottom of foot coil, and the foot at 90 degrees to leg. The sequences,
planes, and scan parameters are summarized in [Table 1] and the planning is summarized in [Fig. 2]. For the thumb MRI, patient is placed in prone position with elevated arm (super-man
position), with the thumb placed in fully extended position at the center of the scanner.
The sequences, planes, and scan parameters are summarized in [Table 2] and the planning is summarized in [Fig. 3].
Table 1
Scan sequences and parameters of great toe
|
Sequence
|
Plane
|
Slice thickness
|
FOV (cmx cm)
|
|
PDFS
|
Axial
|
2–3
|
8 × 16
|
|
PDFS
|
Coronal
|
2–3
|
12 × 10
|
|
PDFS
|
Sagittal
|
2–3
|
18 × 10
|
|
T1W
|
Sagittal
|
2–3
|
18 × 10
|
|
T2W
|
Coronal
|
2–3
|
12 × 10
|
Abbreviations: FOV, field of view; PDFS, fat suppressed proton density; T1W, T1-weighted.
 Fig. 2 Planning of magnetic resonance imaging great toe. (A) First, the localizer was used to plan axial images perpendicular to the long axis
of the metatarsal and proximal phalanx. (B) The coronal slices were planned on the sagittal plane, parallel to the to the long
axis of the metatarsal and proximal phalanx. (C) Using axial images, sagittal scan was planned perpendicular to the line joining
the two sesamoids.
Fig. 2 Planning of magnetic resonance imaging great toe. (A) First, the localizer was used to plan axial images perpendicular to the long axis
of the metatarsal and proximal phalanx. (B) The coronal slices were planned on the sagittal plane, parallel to the to the long
axis of the metatarsal and proximal phalanx. (C) Using axial images, sagittal scan was planned perpendicular to the line joining
the two sesamoids.
Table 2
Scan sequences and parameters of thumb
|
Sequence
|
Plane
|
Slice thickness
|
FOV (cmxcm)
|
|
PDFS
|
Axial
|
2–3
|
8 × 8
|
|
PDFS
|
Coronal
|
2–3
|
10 × 12
|
|
PDFS
|
Sagittal
|
2–3
|
10 × 12
|
|
T1W
|
Sagittal
|
2–3
|
10 × 12
|
|
T2W
|
Coronal
|
2–3
|
10 × 12
|
Abbreviations: FOV, field of view; PDFS, fat suppressed proton density; T1W, T1-weighted.
 Fig. 3 Planning of magnetic resonance imaging thumb. (A) First, localizer was used to plan axial images perpendicular to the long axis of
the proximal phalanx. (B) Using axial images, coronal scan was planned parallel to the line joining the two
sesamoids (outlined with yellow circle). (C) Using axial images, sagittal scan was planned perpendicular to the line joining
the two sesamoids.
Fig. 3 Planning of magnetic resonance imaging thumb. (A) First, localizer was used to plan axial images perpendicular to the long axis of
the proximal phalanx. (B) Using axial images, coronal scan was planned parallel to the line joining the two
sesamoids (outlined with yellow circle). (C) Using axial images, sagittal scan was planned perpendicular to the line joining
the two sesamoids.
Tarsometatarsal/Carpometacarpal Joints
Great Toe
The first TM joint of foot forms the medial column of the Lisfranc's joint that provides
stability to the mid foot and forefoot. It is an arthrodial joint between the distal
articular surface of the medial cuneiform and the base of first metatarsal, allowing
flexion and extension with limited abduction and rotation. The dorsomedial ligament
connects the dorsal surface of the medial cuneiform to that of base of first metatarsal,
the dorsal Lisfranc's ligament extends from the dorsolateral side of medial cuneiform
to the medial surface of base of second metatarsal, and the dorsal intercuneiform
ligament connects the medial and intermediate cuneiforms. The plantar TM ligament
and the plantar Lisfranc's complex connects plantar surface of medial cuneiform to
plantar surface of base of first, second, and third metatarsal, respectively. The
tendon of tibialis anterior attaches on the medioplantar aspect of the base of first
metatarsal and the distal end of medial cuneiform, whereas the peroneus longus attaches
on the lateral aspect of the same[3]
[4] ([Fig. 4]).
 Fig. 4 Ligaments around first tarsometatatarsal joint. (A) Diagrammatic representation of the three dorsal ligaments: dorsomedial ligament
(dC1-M1) that is between dorsal surface of medial cuneiform (C1) and the dorsal surface
of the base of first metatarsal (M1), proper Lisfranc's ligament (dC1-M2) between
the dorsal surface of medial cuneiform (C1) and base of second metatarsal (M2) and
the intercuneiform ligament (dC1-C2) between the dorsal surfaces of the medial (C1)
and intermediate cuneiform (C2). (B) Diagrammatic representation of the three plantar ligaments: plantar tarsometatarsal
ligament (pC1-M1) between plantar surface of medial cuneiform (C1) to base of first
metatarsal (M1) and the proper plantar Lisfranc's ligament's complex (pC1-M2/M3) extending
between medial cuneiform and plantar surface of base of second (M2) and third metatarsal
(M3). (C) Sagittal fat suppressed proton density (PDFS) weighted magnetic resonance image
shows dorsomedial ligament (thin green arrow) and plantar tarsometatarsal ligament
(thin yellow arrow). (D–G) Serial axial PDFS image from dorsal to plantar aspect shows proper dorsal ligament
(thick green arrows, (D) and intercuneiform ligament (green arrow heads, D). pC1-M2 (thick yellow arrow, E) and pC1-M3 (yellow arrow heads, F) components of proper plantar Lisfranc ligament. The tendon of tibialis anterior
(white arrows, F) can be seen attaching to the base of distal phalanx and the adjacent proximal aspect
of medial cuneiform. The tendon of the peroneus longus (black arrows, G) can be seen attaching to the lateral aspect of base of the first metatarsal.
Fig. 4 Ligaments around first tarsometatatarsal joint. (A) Diagrammatic representation of the three dorsal ligaments: dorsomedial ligament
(dC1-M1) that is between dorsal surface of medial cuneiform (C1) and the dorsal surface
of the base of first metatarsal (M1), proper Lisfranc's ligament (dC1-M2) between
the dorsal surface of medial cuneiform (C1) and base of second metatarsal (M2) and
the intercuneiform ligament (dC1-C2) between the dorsal surfaces of the medial (C1)
and intermediate cuneiform (C2). (B) Diagrammatic representation of the three plantar ligaments: plantar tarsometatarsal
ligament (pC1-M1) between plantar surface of medial cuneiform (C1) to base of first
metatarsal (M1) and the proper plantar Lisfranc's ligament's complex (pC1-M2/M3) extending
between medial cuneiform and plantar surface of base of second (M2) and third metatarsal
(M3). (C) Sagittal fat suppressed proton density (PDFS) weighted magnetic resonance image
shows dorsomedial ligament (thin green arrow) and plantar tarsometatarsal ligament
(thin yellow arrow). (D–G) Serial axial PDFS image from dorsal to plantar aspect shows proper dorsal ligament
(thick green arrows, (D) and intercuneiform ligament (green arrow heads, D). pC1-M2 (thick yellow arrow, E) and pC1-M3 (yellow arrow heads, F) components of proper plantar Lisfranc ligament. The tendon of tibialis anterior
(white arrows, F) can be seen attaching to the base of distal phalanx and the adjacent proximal aspect
of medial cuneiform. The tendon of the peroneus longus (black arrows, G) can be seen attaching to the lateral aspect of base of the first metatarsal.
The Lisfranc's ligament is responsible for anterolateral stabilization of midfoot
and forefoot. As anterolateral stabilization is not required in thumb, the corresponding
Lisfranc's akin ligament is not seen in the thumb.[5]
Thumb
The first CM joint is an incongruous saddle joint between trapezium and first metacarpal
with a wide range of motion, including flexion, extension, abduction, adduction, and
circumduction, contributing to the apposable and prehensile capability of the human
thumb. There are five main ligaments around this joint, divided into dorsal and volar
group. The ligaments of the dorsal group include dorsoradial ligament (DRL), posterior
oblique ligament (POL), collectively called dorsal carpometacarpal ligament complex
as-well-as intermetatarsal ligament (IML). They are best visualized in the sagittal
plane, except IML that is seen on oblique coronal reformatted image across the first
web space. DRL is a capsular ligament that extends from the dorsoradial tubercle of
trapezium to the dorsolateral surface of base of first metacarpal, attaching deep
to the attachment of abductor pollicis longus (APL) tendon. POL is also a capsular
ligament, attached more ulnar to the DRL. IML connects the base of the first and second
metacarpals. The volar trapeziometacarpal ligament includes the anterior oblique ligament
(AOL—superficial capsular and deep intracapsular components) extending from the volar
tubercle of trapezium to the volar tubercle of the base of first metacarpal and the
ulnar collateral ligament, a thin ligament on the ulnar aspect of AOL that is often
difficult to appreciate, separately from AOL, on MRI.[6]
[7] The tendon of APL attaches to the radial aspect of base of the first metacarpal[3] ([Fig. 5] and [Table 3]).
 Fig. 5 Ligaments and tendons around the trapeziometacarpal joint. (A) Diagrammatic representation of thumb in coronal plane shows the components of dorsal
first carpometacarpal ligaments. The dorsoradial ligament (DRL) is a capsular thickening
between the dorsal surface of the trapezium (T) to the dorsoradial surface of the
base of the first metacarpal (m1) deep to the abductor pollicis longus (APL) tendon.
The posterior oblique ligament (POL) is also a capsular ligament between the trapezium
and base of first metacarpal, positioned more ulnar to the attachment of the DRL.
The intermetacarpal ligament (IML) extends from the ulnar side of the base of first
metacarpal (m1) to the radial side of the base of the second metacarpal (m2). (B) Diagrammatic representation of thumb in coronal plane shows components of volar
first carpometacarpal ligaments. The thicker anterior oblique ligament (AOL) has superficial
and deep components, extending from the volar tubercule of trapezium (T) to the volar
tubercle of the first metacarpal (m1). The ulnar collateral ligament (UCL) is a thinner
ligament between the volar surface of the trapezium, near the attachment of the flexor
retinaculum to the base of the first metacarpal and is often not well delineated on
conventional magnetic resonance imaging (MRI). (C and D) Serial sagittal fat suppressed proton density (PDFS) MR image shows DRL (thick green
arrow, C) deep to the APL (white arrow heads, C) and the AOL (yellow arrows, C and D). The POL (thin arrow) is seen, ulnar to DRL and is seen on the sagittal section
where APL is no longer visible, but extensor polices tendon (white arrow) is seen.
(E) The oblique coronal reformatted PDFS MR image of a different patient demonstrates
the IML (green arrowheads).
Fig. 5 Ligaments and tendons around the trapeziometacarpal joint. (A) Diagrammatic representation of thumb in coronal plane shows the components of dorsal
first carpometacarpal ligaments. The dorsoradial ligament (DRL) is a capsular thickening
between the dorsal surface of the trapezium (T) to the dorsoradial surface of the
base of the first metacarpal (m1) deep to the abductor pollicis longus (APL) tendon.
The posterior oblique ligament (POL) is also a capsular ligament between the trapezium
and base of first metacarpal, positioned more ulnar to the attachment of the DRL.
The intermetacarpal ligament (IML) extends from the ulnar side of the base of first
metacarpal (m1) to the radial side of the base of the second metacarpal (m2). (B) Diagrammatic representation of thumb in coronal plane shows components of volar
first carpometacarpal ligaments. The thicker anterior oblique ligament (AOL) has superficial
and deep components, extending from the volar tubercule of trapezium (T) to the volar
tubercle of the first metacarpal (m1). The ulnar collateral ligament (UCL) is a thinner
ligament between the volar surface of the trapezium, near the attachment of the flexor
retinaculum to the base of the first metacarpal and is often not well delineated on
conventional magnetic resonance imaging (MRI). (C and D) Serial sagittal fat suppressed proton density (PDFS) MR image shows DRL (thick green
arrow, C) deep to the APL (white arrow heads, C) and the AOL (yellow arrows, C and D). The POL (thin arrow) is seen, ulnar to DRL and is seen on the sagittal section
where APL is no longer visible, but extensor polices tendon (white arrow) is seen.
(E) The oblique coronal reformatted PDFS MR image of a different patient demonstrates
the IML (green arrowheads).
Table 3
Comparative analysis of the tarsometatarsal joint and the carpometacarpal joint
|
Great toe: Tarsometatarsal joint
|
Thumb: Carpometacarpal joint
|
|
Ligaments
|
Dorsomedial ligament
(dC1-M1)
Dorsal Lisfranc's ligament
(dC1-M2)
Dorsal intercuneiform ligament
(dC1-C2)
Planter tarsometatarsal ligament
(pC1-M1)
Plantar Lisfranc's ligament complex (pC1-M2/M3)
|
Dorsal carpometacarpal ligament complex—DRL and POL
Intermetatarsal ligament
UCL-AOL
|
|
Tendons
|
At distal end of medial cuneiform:
Peroneus longus
Tibialis anterior
At base of first metatarsal:
Peroneus longus
Tibialis anterior
|
At trapezium: Nil
At base of first metacarpal: APL
|
Abbreviations: AOL, anterior oblique ligament; APL, abductor pollicis longus; DRL,
dorsoradial Ligament; POL, posterior oblique ligament; UCL, ulnar collateral ligament.
Metatarsophalangeal/Metacarpophalangeal Joints
Great Toe
The first MTP joint is an ellipsoid joint between the head of first metatarsal and
base of first proximal phalanx that allows flexion, extension, limited adduction,
abduction, rotation, and circumduction. There exists a “plantar plate complex” that
stabilizes and protects the joint, aiding in propulsion while walking and maintaining
balance. It comprises the sesamoido-capsulo-ligamentous complex and a musculo-tendinous
complex.[8]
There are two sesamoid bones, medial and lateral, articulating in the respective grooves
present on the plantar surface of the first metatarsal head. They function as a pulley
system, providing attachment and smooth movement of tendons as well as protection
to the underlying joint. The sesamoids are connected to each other by the intersesamoid
ligament (ISL), to the base of proximal phalanx by the paired sesamoidophalangeal
ligaments (SPL) and to the plantar aspect of first metatarsal neck by the paired metatarsosesamoid
ligaments. The SPLs are thicker and serve as the main stabilizer against hyperextension.
There is a fibrocartilaginous pad, visible between the two SPLs that invest the sesamoid
bones and is inseparable from the plantar capsule and above-described ligaments. The
ligaments between the lateral and medial aspect of the proximal phalanx and the head
of metatarsal are the lateral and medial collateral ligaments, respectively, that
typically are not considered part of the “plantar plate complex” and protect against
varus and valgus forces, respectively[3]
[8] ([Figs. 6] and [7]).
 Fig. 6 Ligamentous attachments around the first metatarsophalangeal (MTP) joint representing
the plantar plate complex. (A) Diagrammatic representation of the first MTP joint shows the medial (M) and lateral
(L) sesamoids and their paired attachments to the plantar surface of the base of proximal
phalanx—the sesamoidophalangeal ligaments (SPL), paired metatarsosesamoid ligaments
(MSL) between the respective sesamoid and neck of first metatarsal. Medial (M) and
lateral (L) collateral ligaments are obliquely oriented, from the head of metatarsal
on each side to the plantar surface of the base of proximal phalanx. The intersesamoid
ligament (ISL) is between the two sesamoids. (B) Axial fat suppressed proton density weighted (PDFS) magnetic resonance (MR) image
and (D) sagittal T2-weighted imaging (T2WI) shows the lateral SPL (yellow arrow heads) as
thick ligament extending from the lateral (L)sesamoid to the base of proximal phalanx,
deep to the conjoint tendon of the adductor hallucis (yellow arrow). Similarly, (B) axial PDFS and (E) sagittal T2WI show the medial SPL (green arrow heads) as thick ligament extending
from the medial (M) sesamoid to the base of proximal phalanx. (C) The subsequent T1W axial image shows the abductor hallucis (green arrow), which
is superficial to the medial SPL. (F and G) Sequential PDFS axial MR image shows the medial collateral ligament (MCL) (bent
green arrow) and lateral collateral ligament (LCL) (bent yellow arrow) extending from
the base of proximal phalanx to the head of first metatarsal on each side. Note the
discontinuity and preligamentous edema at the metatarsal attachment of MCL suggestive
of a tear.
Fig. 6 Ligamentous attachments around the first metatarsophalangeal (MTP) joint representing
the plantar plate complex. (A) Diagrammatic representation of the first MTP joint shows the medial (M) and lateral
(L) sesamoids and their paired attachments to the plantar surface of the base of proximal
phalanx—the sesamoidophalangeal ligaments (SPL), paired metatarsosesamoid ligaments
(MSL) between the respective sesamoid and neck of first metatarsal. Medial (M) and
lateral (L) collateral ligaments are obliquely oriented, from the head of metatarsal
on each side to the plantar surface of the base of proximal phalanx. The intersesamoid
ligament (ISL) is between the two sesamoids. (B) Axial fat suppressed proton density weighted (PDFS) magnetic resonance (MR) image
and (D) sagittal T2-weighted imaging (T2WI) shows the lateral SPL (yellow arrow heads) as
thick ligament extending from the lateral (L)sesamoid to the base of proximal phalanx,
deep to the conjoint tendon of the adductor hallucis (yellow arrow). Similarly, (B) axial PDFS and (E) sagittal T2WI show the medial SPL (green arrow heads) as thick ligament extending
from the medial (M) sesamoid to the base of proximal phalanx. (C) The subsequent T1W axial image shows the abductor hallucis (green arrow), which
is superficial to the medial SPL. (F and G) Sequential PDFS axial MR image shows the medial collateral ligament (MCL) (bent
green arrow) and lateral collateral ligament (LCL) (bent yellow arrow) extending from
the base of proximal phalanx to the head of first metatarsal on each side. Note the
discontinuity and preligamentous edema at the metatarsal attachment of MCL suggestive
of a tear.
 Fig. 7 Ligamentous attachments around the first metatarsophalangeal (MTP) joint. (A,
C) Axial diagrammatic representation and (B, D) corresponding fat suppressed proton density (PDFS) axial magnetic resonance image
at the level of first metatarsal head and base of proximal phalanx shows the medial
collateral ligament (bent green arrows) and lateral collateral ligaments (yellow bent
arrows). The lateral sesamoidophalangeal ligament (MTS, curved arrow in a, straight
arrows in B) is seen extending between the lateral sesamoid and metatarsal head, merging
with the collateral ligaments. The medial MTS ligament (curved green arrow in A) is seen between medial sesamoid and adjacent metatarsal head; the corresponding
axial PDFS image (B) shows fluid signal (green arrow) and absence of T2 hypointense signal at the location
of the ligament suggesting tear of the medial MTS ligament. The sesamoidophalangeal
ligaments are seen at the level of base of proximal phalanx (C, D; medial—green arrowhead,
lateral—yellow arrowhead). The adductor hallucis tendon (yellow arrow) and abductor
halluces tendon (green arrow) are seen superficial to the ligaments, ultimately merging
with it.
Fig. 7 Ligamentous attachments around the first metatarsophalangeal (MTP) joint. (A,
C) Axial diagrammatic representation and (B, D) corresponding fat suppressed proton density (PDFS) axial magnetic resonance image
at the level of first metatarsal head and base of proximal phalanx shows the medial
collateral ligament (bent green arrows) and lateral collateral ligaments (yellow bent
arrows). The lateral sesamoidophalangeal ligament (MTS, curved arrow in a, straight
arrows in B) is seen extending between the lateral sesamoid and metatarsal head, merging
with the collateral ligaments. The medial MTS ligament (curved green arrow in A) is seen between medial sesamoid and adjacent metatarsal head; the corresponding
axial PDFS image (B) shows fluid signal (green arrow) and absence of T2 hypointense signal at the location
of the ligament suggesting tear of the medial MTS ligament. The sesamoidophalangeal
ligaments are seen at the level of base of proximal phalanx (C, D; medial—green arrowhead,
lateral—yellow arrowhead). The adductor hallucis tendon (yellow arrow) and abductor
halluces tendon (green arrow) are seen superficial to the ligaments, ultimately merging
with it.
The musculo-tendinous complex provides dynamic stabilization to the joint. The flexor
hallucis longus (FHL) tendon runs beneath ISL, in the groove between the two sesamoids
and finally attaches to the base of the distal phalanx. The paired flexor hallucis
brevis attaches to the respective sesamoid bones. On the medial aspect, abductor hallucis
tendon attaches to the medial sesamoid with extensions to the capsule-ligamentous
complex and medial aspect of the base of the proximal phalanx. Similarly, on the lateral
aspect, conjoint tendon of the oblique and transverse heads of adductor hallucis attach
to the lateral sesamoid with extensions to the capsule-ligamentous complex and lateral
aspect of the base of the proximal phalanx[3]
[8] ([Figs. 8] and [9]).
 Fig. 8 Musculotendinous attachments around the first metacarpophalangeal (MCP) joint. (A) Diagrammatic representation and (B) corresponding axial T1-weighted magnetic resonance (MR) image show the adductor
hallucis muscle attaching to the lateral sesamoid (L) and to the base of proximal
phalanx and adjoining capsule-ligamentous complex (not shown here), the medial and
lateral heads of the flexor hallucis brevis (FHB) attaching to the respective sesamoids,
and the tendon of abductor hallucis (green arrow) is seen attaching to the medial
sesamoid (M). (C) Coronal fat suppressed proton density MR image shows transverse head of adductor
hallucis and its tendon (yellow arrow), lateral and medial FHB and its tendons (white
arrows) and in the medial most aspect, tendon of abductor hallucis (green arrow).
Fig. 8 Musculotendinous attachments around the first metacarpophalangeal (MCP) joint. (A) Diagrammatic representation and (B) corresponding axial T1-weighted magnetic resonance (MR) image show the adductor
hallucis muscle attaching to the lateral sesamoid (L) and to the base of proximal
phalanx and adjoining capsule-ligamentous complex (not shown here), the medial and
lateral heads of the flexor hallucis brevis (FHB) attaching to the respective sesamoids,
and the tendon of abductor hallucis (green arrow) is seen attaching to the medial
sesamoid (M). (C) Coronal fat suppressed proton density MR image shows transverse head of adductor
hallucis and its tendon (yellow arrow), lateral and medial FHB and its tendons (white
arrows) and in the medial most aspect, tendon of abductor hallucis (green arrow).
 Fig. 9 Plantar plate complex. The serial sagittal T2-weighted magnetic resonance images
show the components of the plantar plate complex of the first metatarsal joint with
corresponding level of section (shown in the inset). (A) The medial most section shows attachment of the abductor halluces (green arrow)
to the medial sesamoid and capsuloligamentous structures attaching to the medial side
of the base of the first metatarsal. (B) The next section shows medial sesamoidophalangeal ligament (SPL; bent green arrow)
between the medial sesamoid (M) and plantar surface of the base of the base of the
first proximal phalanx and the medial head of flexor halluces brevis (FHB) attaching
to the medial sesamoid (M). (C) The section through the midline of the metatarsophalangeal (MTP) joint, shows the
flexor halluces longus (FHL) tendon (blue arrows) passing over the fibrocartilage
part of the plantar plate (white asterisk) and inseparable from the intersesamoid
ligament (thin white arrow). (D) The sagittal section at the level of the lateral sesamoid (L) shows the lateral
SPL (bent yellow arrow) between the lateral sesamoid(L) and plantar surface of the
base of the base of the first proximal phalanx and the lateral head of FHB attaching
to lateral sesamoid (L). (E) The lateral most section through the first MTP joint shows the conjoint tendon of
adductor halluces (yellow arrow) attaching to the lateral sesamoid, adjacent capsuloligamentous
complex, and lateral surface of the base of proximal phalanx.
Fig. 9 Plantar plate complex. The serial sagittal T2-weighted magnetic resonance images
show the components of the plantar plate complex of the first metatarsal joint with
corresponding level of section (shown in the inset). (A) The medial most section shows attachment of the abductor halluces (green arrow)
to the medial sesamoid and capsuloligamentous structures attaching to the medial side
of the base of the first metatarsal. (B) The next section shows medial sesamoidophalangeal ligament (SPL; bent green arrow)
between the medial sesamoid (M) and plantar surface of the base of the base of the
first proximal phalanx and the medial head of flexor halluces brevis (FHB) attaching
to the medial sesamoid (M). (C) The section through the midline of the metatarsophalangeal (MTP) joint, shows the
flexor halluces longus (FHL) tendon (blue arrows) passing over the fibrocartilage
part of the plantar plate (white asterisk) and inseparable from the intersesamoid
ligament (thin white arrow). (D) The sagittal section at the level of the lateral sesamoid (L) shows the lateral
SPL (bent yellow arrow) between the lateral sesamoid(L) and plantar surface of the
base of the base of the first proximal phalanx and the lateral head of FHB attaching
to lateral sesamoid (L). (E) The lateral most section through the first MTP joint shows the conjoint tendon of
adductor halluces (yellow arrow) attaching to the lateral sesamoid, adjacent capsuloligamentous
complex, and lateral surface of the base of proximal phalanx.
On the dorsal aspect of the MTP joint, the extensor hallucis brevis and extensor hallucis
longus (EHL) pass over the dorsal plate to finally attach on the dorsal aspect of
the base of the proximal and distal phalanx, respectively. The extensor tendons are
anchored to the underlying bones by the medial and lateral sagittal bands[3]
[8] ([Fig. 10]).
 Fig. 10 Extensor and flexor compartment muscles of the great toe. (A) Sagittal schematic diagram and (B) sagittal fat suppressed proton density (PDFS) shows that the flexor halluces longus
(FHL) (blue arrows) attaches to the base of the distal phalanx on the plantar aspect,
passing over the plantar plate of distal interphalangeal (DIP) and plantar plate complex
of metatarsophalangeal (MTP) (white asterisks). The extensor hallucis brevis (EHB)
(short green arrow) attaches to the dorsal aspect of the base of the proximal phalanx
and the extensor hallucis longus (EHL) (long green arrow) goes on to attach on the
dorsal aspect of the base of the distal phalanx, passing over the dorsal plates (yellow
asterisks) at the level of intervening joints. (C) Axial schematic diagram and (D) corresponding axial PDFS magnetic resonance image at the level of proximal phalanx
shows the EHL (green arrow) is secured to the underlying bone through thin sagittal
bands (white arrows).
Fig. 10 Extensor and flexor compartment muscles of the great toe. (A) Sagittal schematic diagram and (B) sagittal fat suppressed proton density (PDFS) shows that the flexor halluces longus
(FHL) (blue arrows) attaches to the base of the distal phalanx on the plantar aspect,
passing over the plantar plate of distal interphalangeal (DIP) and plantar plate complex
of metatarsophalangeal (MTP) (white asterisks). The extensor hallucis brevis (EHB)
(short green arrow) attaches to the dorsal aspect of the base of the proximal phalanx
and the extensor hallucis longus (EHL) (long green arrow) goes on to attach on the
dorsal aspect of the base of the distal phalanx, passing over the dorsal plates (yellow
asterisks) at the level of intervening joints. (C) Axial schematic diagram and (D) corresponding axial PDFS magnetic resonance image at the level of proximal phalanx
shows the EHL (green arrow) is secured to the underlying bone through thin sagittal
bands (white arrows).
Thumb
The first MCP joint is also an ellipsoid joint that allows flexion, extension, limited
adduction, abduction, rotation, and circumduction. Analogous to the plantar plate
complex, there exists a similar “volar plate complex” comprising the radial and ulnar
sesamoids, embedded within the fibrocartilaginous volar plate with a gamut of ligamentous
and musculo-tendinous attachments. Its ligamentous support is less robust, allowing
more mobility and less stability compared with the MTP joint that plays a pivotal
role in weight bearing and walking.
The radial and ulnar collateral ligaments attach proximally on the volar aspect of
the metacarpal head laterally and distally to the dorsolateral aspect of the base
of the proximal phalanx. The accessory collateral ligaments attach to the metacarpal
head (volar to proper collateral ligaments), connecting it to the respective sesamoids
and the volar plate[6]
[9] ([Figs. 11] and [12]).
 Fig. 11 Ligamentous and tendinous attachments around the first metacarpophalangeal joint
(MCP). (A) Schematic diagram shows the ligamentous and tendonous attachments around the first
MCP. The radial (RCL) and ulnar collateral ligaments (UCL) are seen extending obliquely
from the palmer aspect of head of metacarpal to the base of proximal phalanx on the
radial and ulnar aspect respectively. The adductor pollicis (AdP) attaches to the
ulnar sesamoid (U), with aponeurotic extension to the base of proximal phalanx. While
the tendon of flexor polices longus (FPL) passes across the MCP joint in between the
two sesamoid bones, the flexor polices brevis (FPB) attaches on the radial sesamoid
(R). The abductor pollicis brevis (AbPB) attaches directly to the base of radial aspect
of proximal phalanx. (B–E) Serial coronal fat suppressed proton density magnetic resonance imaging showing
the radial (R) and ulnar (U) sesamoid bones and FPL tendon (long green arrow) in (B). FHB tendon (short green arrows; c) is seen attaching on the radial sesamoid and base of proximal phalanx. The RCL (blue
arrow heads; D–E) lies deep to the AbPB(blue arrows; D), whereas the UCL(yellow arrow heads; D–E) lies deep to the AdP aponeurosis(yellow arrows; D–E), attaching distally to the base of proximal phalanx on its radial and ulnar aspect,
respectively.
Fig. 11 Ligamentous and tendinous attachments around the first metacarpophalangeal joint
(MCP). (A) Schematic diagram shows the ligamentous and tendonous attachments around the first
MCP. The radial (RCL) and ulnar collateral ligaments (UCL) are seen extending obliquely
from the palmer aspect of head of metacarpal to the base of proximal phalanx on the
radial and ulnar aspect respectively. The adductor pollicis (AdP) attaches to the
ulnar sesamoid (U), with aponeurotic extension to the base of proximal phalanx. While
the tendon of flexor polices longus (FPL) passes across the MCP joint in between the
two sesamoid bones, the flexor polices brevis (FPB) attaches on the radial sesamoid
(R). The abductor pollicis brevis (AbPB) attaches directly to the base of radial aspect
of proximal phalanx. (B–E) Serial coronal fat suppressed proton density magnetic resonance imaging showing
the radial (R) and ulnar (U) sesamoid bones and FPL tendon (long green arrow) in (B). FHB tendon (short green arrows; c) is seen attaching on the radial sesamoid and base of proximal phalanx. The RCL (blue
arrow heads; D–E) lies deep to the AbPB(blue arrows; D), whereas the UCL(yellow arrow heads; D–E) lies deep to the AdP aponeurosis(yellow arrows; D–E), attaching distally to the base of proximal phalanx on its radial and ulnar aspect,
respectively.
 Fig. 12 Ligamentous and tendinous attachments around the first metacarpophalangeal (MCP)
joint. (A) Schematic diagram and (B) axial T1-weighted imaging at the level of the head of the first metacarpal joint
showing the ligamentous attachments around the first MCP joint. The proper radial
(p-RCL, A; dark blue arrow heads, B) and proper ulnar (p-UCL, A; dark blue arrow heads, B) collateral ligament proximally attach to the metacarpal head, whereas the accessory
radial (p-RCL, A; light blue arrow heads, B) and accessory ulnar (a-UCL, A; light blue arrow heads, B) collateral ligaments attach to the radial (R) and ulnar (U) sesamoid bones, respectively.
The volar plate (asterisk) is between the two sesamoid bones, with the flexor pollicis
longus (FPL) tendon running along its volar aspect. The abductor pollicis brevis tendon
(AbPb, blue arrow) and the adductor pollicis aponeurosis (AdP, yellow arrows) lie
superficial to the respective collateral ligaments, attaching distally to the base
of the proximal phalanx (not shown).
Fig. 12 Ligamentous and tendinous attachments around the first metacarpophalangeal (MCP)
joint. (A) Schematic diagram and (B) axial T1-weighted imaging at the level of the head of the first metacarpal joint
showing the ligamentous attachments around the first MCP joint. The proper radial
(p-RCL, A; dark blue arrow heads, B) and proper ulnar (p-UCL, A; dark blue arrow heads, B) collateral ligament proximally attach to the metacarpal head, whereas the accessory
radial (p-RCL, A; light blue arrow heads, B) and accessory ulnar (a-UCL, A; light blue arrow heads, B) collateral ligaments attach to the radial (R) and ulnar (U) sesamoid bones, respectively.
The volar plate (asterisk) is between the two sesamoid bones, with the flexor pollicis
longus (FPL) tendon running along its volar aspect. The abductor pollicis brevis tendon
(AbPb, blue arrow) and the adductor pollicis aponeurosis (AdP, yellow arrows) lie
superficial to the respective collateral ligaments, attaching distally to the base
of the proximal phalanx (not shown).
The radial and ulnar sesamoids provide attachments to flexor pollicis brevis (FPB)
and adductor pollicis, respectively. The aponeurosis of adductor pollicis extends
further to attach on the ulnar aspect of the base of the proximal phalanx. The tendon
of abductor pollicis brevis is however attached only to the radial aspect of base
of proximal phalanx[6]
[9] ([Figs. 11] and [12]).
The flexor pollicis longus (FPL) tendon passes over the volar plate in the groove
between the sesamoid bones to finally attach to the base of the distal phalanx ([Fig. 13]). FPL is anchored to the underlying bones by the annular pulley system that prevents
bow-stringing of the tendon during flexion. The pulley system of the thumb differs
from the rest of the digits as there are no transverse pulleys, but only annular pulleys
as described in [Fig. 14].[6]
[9]
 Fig. 13 Muscles of the flexor and extensor compartment of the great toe. (A) Sagittal schematic diagram and (B, C) serial sagittal fat suppressed proton density (PDFS) shows that the flexor pollicis
longus (FPL; green arrows) attaches to the base of the distal phalanx on the volar
aspect, passing over the volar plates (white asterisks) at the level of metacarpophalangeal
(MCP) and distal interphalangeal (DIP) joints. The extensor pollicis brevis (EPB;
short white arrow) attaches to the dorsal aspect of the base of the proximal phalanx
and the extensor pollicis longus (EPL) (long white arrow) goes on to attach on the
dorsal aspect of the base of the distal phalanx, passing over the dorsal plates (yellow
asterisks) at the level of intervening joints. Note that there is a synovial recess
(yellow arrow, B) at the proximal attachment of the volar plate, which should not be misinterpreted
as a tear. (D) Sagittal schematic diagram and (E) serial sagittal PDFS shows the attachment of the flexor pollicis brevis (FPB; short
green arrows) on the radial sesamoid (R) and volar aspect of the base of proximal
phalanx.
Fig. 13 Muscles of the flexor and extensor compartment of the great toe. (A) Sagittal schematic diagram and (B, C) serial sagittal fat suppressed proton density (PDFS) shows that the flexor pollicis
longus (FPL; green arrows) attaches to the base of the distal phalanx on the volar
aspect, passing over the volar plates (white asterisks) at the level of metacarpophalangeal
(MCP) and distal interphalangeal (DIP) joints. The extensor pollicis brevis (EPB;
short white arrow) attaches to the dorsal aspect of the base of the proximal phalanx
and the extensor pollicis longus (EPL) (long white arrow) goes on to attach on the
dorsal aspect of the base of the distal phalanx, passing over the dorsal plates (yellow
asterisks) at the level of intervening joints. Note that there is a synovial recess
(yellow arrow, B) at the proximal attachment of the volar plate, which should not be misinterpreted
as a tear. (D) Sagittal schematic diagram and (E) serial sagittal PDFS shows the attachment of the flexor pollicis brevis (FPB; short
green arrows) on the radial sesamoid (R) and volar aspect of the base of proximal
phalanx.
 Fig. 14 Pulley system around the flexor pollicis longus (FPL) tendon. (A) Coronal schematic diagram showing the positions of annular pulleys (shaded in green):
A1 and A2 are along the metacarpophalangeal (MCP) and distal interphalangeal (DIP)
joints, respectively. The oblique pulley (Ao) is along the diaphysis of proximal phalanx
and oriented obliquely. The variable pulley (Av) is between the A1 and A2. (B) Axial schematic diagram showing the position of annular pulleys in relation to the
FPL tendon. The pulleys (green line) surround the FPL tendon, attaching to the palmer
aspect of the phalanges, preventing bowstringing of FPL. (C–F) Corresponding axial magnetic resonance T1-weighted images are shown in the panel
on the right with the pulleys marked with green arrows. To merge either A1 and A2
pulleys are seen to merge with the underlying volar plates.
Fig. 14 Pulley system around the flexor pollicis longus (FPL) tendon. (A) Coronal schematic diagram showing the positions of annular pulleys (shaded in green):
A1 and A2 are along the metacarpophalangeal (MCP) and distal interphalangeal (DIP)
joints, respectively. The oblique pulley (Ao) is along the diaphysis of proximal phalanx
and oriented obliquely. The variable pulley (Av) is between the A1 and A2. (B) Axial schematic diagram showing the position of annular pulleys in relation to the
FPL tendon. The pulleys (green line) surround the FPL tendon, attaching to the palmer
aspect of the phalanges, preventing bowstringing of FPL. (C–F) Corresponding axial magnetic resonance T1-weighted images are shown in the panel
on the right with the pulleys marked with green arrows. To merge either A1 and A2
pulleys are seen to merge with the underlying volar plates.
Similar to the MTP joint, extensor pollicis brevis (EPB) and extensor pollicis longus
(EPL) tendons pass over the dorsal plate of the MCP joint and finally attach to the
dorsal aspect of the base of the proximal and distal phalanx, respectively ([Fig. 13]). EPB, being a muscle of the first extensor compartment of the forearm, is visualized
more radial to the EPL, a muscle of the third compartment. The extensor tendons are
anchored to the underlying bones by the medial and lateral sagittal bands[6]
[9]([Fig. 15] and [Table 4]).
 Fig. 15 Extensor muscles of the thumb. (A) Coronal and (C) axial schematic diagram, (B) coronal fat suppressed proton density magnetic resonance (MR) images and (D) axial T1-weighted MR images at the level of first metacarpal bone show that the
extensor shows that the extensor pollicis brevis (EPB, short white arrow) lies radial
to the extensor pollicis longus (EPL, long white arrow). Note that even at the level
of distal forearm and wrist, the EPB is more on the radial aspect as it belongs to
the first compartment and EPL belongs to the third compartment of the extensor group
of muscle. The tendons are held in central position by the sagittal bands (shaded
in gray in a, black arrows in C–D), in and around the metacarpophalangeal (MCP) joint, whereas more distally, it is
supported by a faint triangular expansion (shaded in purple), which is not well appreciated
on imaging.
Fig. 15 Extensor muscles of the thumb. (A) Coronal and (C) axial schematic diagram, (B) coronal fat suppressed proton density magnetic resonance (MR) images and (D) axial T1-weighted MR images at the level of first metacarpal bone show that the
extensor shows that the extensor pollicis brevis (EPB, short white arrow) lies radial
to the extensor pollicis longus (EPL, long white arrow). Note that even at the level
of distal forearm and wrist, the EPB is more on the radial aspect as it belongs to
the first compartment and EPL belongs to the third compartment of the extensor group
of muscle. The tendons are held in central position by the sagittal bands (shaded
in gray in a, black arrows in C–D), in and around the metacarpophalangeal (MCP) joint, whereas more distally, it is
supported by a faint triangular expansion (shaded in purple), which is not well appreciated
on imaging.
Table 4
Comparative analysis of the first metatarsophalangeal (MTP) joint of foot and metacarpophalangeal
(MCP) joint of thumb
|
Great Toe: First MTP joint
|
Thumb: First MCP joint
|
|
Ligaments
|
Plantar plate—fibrocartilage pad[a]
Medial and lateral SPL[a]
Intersesamoid ligament[a]
MCL
LCL
Medial and lateral MTSL[a]
Dorsal plate
Medial and lateral sagittal bands
|
Volar plate
Intersesamoid ligament
RCL
UCL supported by adductor aponeurosis
Accessory UCL and RCL
Dorsal plate
Radial and ulnar sagittal bands
Pulleys
|
|
Tendons
|
Lateral sesamoid: FHB (lateral head), adductor hallucis
Medial sesamoid: FHB (medial head), abductor hallucis
FHL
EHL
EHB
|
Ulnar sesamoid: adductor pollicis
Radial sesamoid: FPB
Base of first metacarpal radial aspect: abductor pollicis brevis
FPL
EPL
EPB
|
Abbreviations: EHB, extensor hallucis brevis; EHL, extensor hallucis longus; EPB,
extensor pollicis brevis; EPL, extensor pollicis longus; FHB, flexor hallucis brevis;
FHL, flexor hallucis longus; FPL, flexor pollicis longus; LCL, lateral collateral
ligament; MCL, medial collateral ligament; MTSL, metatarsosesamoid ligament; RCL,
radial collateral ligament; SPL, sesamoidophalangeal ligament; UCL, ulnar collateral
ligament.
a Forms part of the “planter plate complex.”
Interphalangeal Joints
The IP joint in both great toe and thumb is a hinge joint, allowing only flexion and
extension movement.
Paired collateral ligaments are present on the medial and lateral aspect of the joint
extending between the distal end of proximal phalanx to the base of the distal phalanx.
The respective EPL/EHL and FPL/FHL attach to the base of the distal phalanx of the
dorsal and volar/plantar aspect, respectively. The volar/plantar plates and dorsal
plates are also present at the IP joint that allow the tendons to glide over smoothly[9] ([Figs. 16] and [17]) ([Table 5]).
 Fig. 16 Ligamentous and tendinous attachments near the distal interphalangeal (DIP) joint
of the great toe. (A) Coronal schematic diagram and (B) coronal fat suppressed proton density (PDFS) magnetic resonance (MR) image at the
level of DIP joint show the lateral (LCL) and medial (MCL) collateral ligaments (blue
arrows) extending from the lateral and medial aspects of distal end of proximal phalanx
to the proximal end of distal phalanx, respectively. (C) Coronal schematic diagram and (D) axial PDFS MR image at the level of base of distal phalanx show LCL and MCL (blue
arrows), extensor hallucis longus (EHL; long white arrow) and flexor hallucis longus
(FHL; long green arrow) attached to the dorsal aspect and volar aspect respectively.
The prominent volar plate is deep to the FHL tendon and is marked with white asterisk.
The dorsal plate (yellow asterisk) is small.
Fig. 16 Ligamentous and tendinous attachments near the distal interphalangeal (DIP) joint
of the great toe. (A) Coronal schematic diagram and (B) coronal fat suppressed proton density (PDFS) magnetic resonance (MR) image at the
level of DIP joint show the lateral (LCL) and medial (MCL) collateral ligaments (blue
arrows) extending from the lateral and medial aspects of distal end of proximal phalanx
to the proximal end of distal phalanx, respectively. (C) Coronal schematic diagram and (D) axial PDFS MR image at the level of base of distal phalanx show LCL and MCL (blue
arrows), extensor hallucis longus (EHL; long white arrow) and flexor hallucis longus
(FHL; long green arrow) attached to the dorsal aspect and volar aspect respectively.
The prominent volar plate is deep to the FHL tendon and is marked with white asterisk.
The dorsal plate (yellow asterisk) is small.
 Fig. 17 Ligamentous and tendinous attachments near the distal interphalangeal (DIP) joint
of the thumb. (A) Coronal schematic diagram and (B) coronal fat suppressed proton density (PDFS) MR image at the level of DIP joint
show the radial (RCL) and ulnar (UCL) collateral ligaments (blue arrows) extending
from the radial and ulnar aspects of distal end of proximal phalanx to the proximal
end of distal phalanx, respectively. (C) Axial schematic diagram and the (D) axial PDFS MR image at the level of base of distal phalanx show the radial and ulnar
collateral ligaments (blue arrow) attached laterally, extensor pollicis longus (EPL;
long white arrow) and flexor pollicis longus (FPL; long green arrow) attached to the
dorsal aspect and volar aspect, respectively. The prominent volar plate is deep to
the FPL tendon and is marked with white asterisk, while the A2(small green arrows)
pulley covers the FPL on its superficial aspect. The sagittal bands (small white arrow)
are thin linear bands that secure the EPL tendon.
Fig. 17 Ligamentous and tendinous attachments near the distal interphalangeal (DIP) joint
of the thumb. (A) Coronal schematic diagram and (B) coronal fat suppressed proton density (PDFS) MR image at the level of DIP joint
show the radial (RCL) and ulnar (UCL) collateral ligaments (blue arrows) extending
from the radial and ulnar aspects of distal end of proximal phalanx to the proximal
end of distal phalanx, respectively. (C) Axial schematic diagram and the (D) axial PDFS MR image at the level of base of distal phalanx show the radial and ulnar
collateral ligaments (blue arrow) attached laterally, extensor pollicis longus (EPL;
long white arrow) and flexor pollicis longus (FPL; long green arrow) attached to the
dorsal aspect and volar aspect, respectively. The prominent volar plate is deep to
the FPL tendon and is marked with white asterisk, while the A2(small green arrows)
pulley covers the FPL on its superficial aspect. The sagittal bands (small white arrow)
are thin linear bands that secure the EPL tendon.
Table 5
Comparative analysis of interphalangeal (IP) joints of great toe and thumb
|
Great toe: IP joint
|
Thumb: IP joint
|
|
Ligaments
|
MCL
LCL
Plantar plate
Dorsal plate
|
RCL
UCL
Volar plate
Dorsal plate
|
|
Tendons
|
FHL
EHL
|
FPL
EPL
|
Abbreviations: EHL, extensor hallucis longus; EPL, extensor pollicis longus; FHL,
flexor hallucis longus; FPL, flexor pollicis longus; LCL, lateral collateral ligament;
MCL, medial collateral ligament; RCL, radial collateral ligament; UCL, ulnar collateral
ligament.
Conclusion
The evolutionary development of human limbs facilitated their feet and hands to assume
functional roles of stability and mobility, respectively, and hence they have many
similarities with few dissimilarities in their anatomy. Evaluating their MRI anatomy
in correlation allows a comprehensive understanding to a radiologist, enabling them
to develop a systematic approach to read the MRI scans thereof.






