
Subscribe to RSS
DOI: 10.1055/s-0042-106392
More to be Learned about Cotyledonoid Dissecting Leiomyoma
Publication History
Publication Date:
20 June 2016 (online)
Introduction
Cotyledonoid dissecting leiomyoma, also known as a “grape-like” myoma or Sternberg tumor, is a particularly uncommon variant of uterine fibroma that imitates malignant gross characteristics; however this tumor is a benign neoplasm clinically and pathologically. The name cotyledonoid leiomyoma originates from the characteristic macroscopic appearance, which includes extrauterine dark red-brown, spongy, bulbous, exophytic masses, resembling the maternal face of the placenta [Smith CC et al. Int J Surg Pathol 2012; 20: 330–341].
Clinically, most cases occur in women of reproductive age, presenting abnormal uterine bleeding and symptoms related to the presence of a pelvic mass. Preoperative diagnosis either by 2D ultrasound or magnetic resonance images (MRI) is usually inaccurate and very frequently raises the suspicion for a malignant process [Raga F et al. Cotyledonoid dissecting leiomyoma of the uterus. Fertil Steril 2009; 91: 1269–1270].
Although this tumor is a benign neoplasm, gross appearance and unusual growth pattern may mimic a malignant process. Consequently, to avoid aggressive surgery it is essential to recognize it preoperatively.
#
Case Description
A 28-year-old nulliparous Caucasian female visited our outpatient clinic with the complaints of menorrhagia, dysmenorrhea and intense asthenia of several months duration, despite the use of oral contraceptives. Major laboratory findings at admission were a hematocrit level of 27.2%, hemoglobin of 8.2 g/dL and a ferritin of 10 ng/mL. Moreover, she had no significant personal or family medical history.
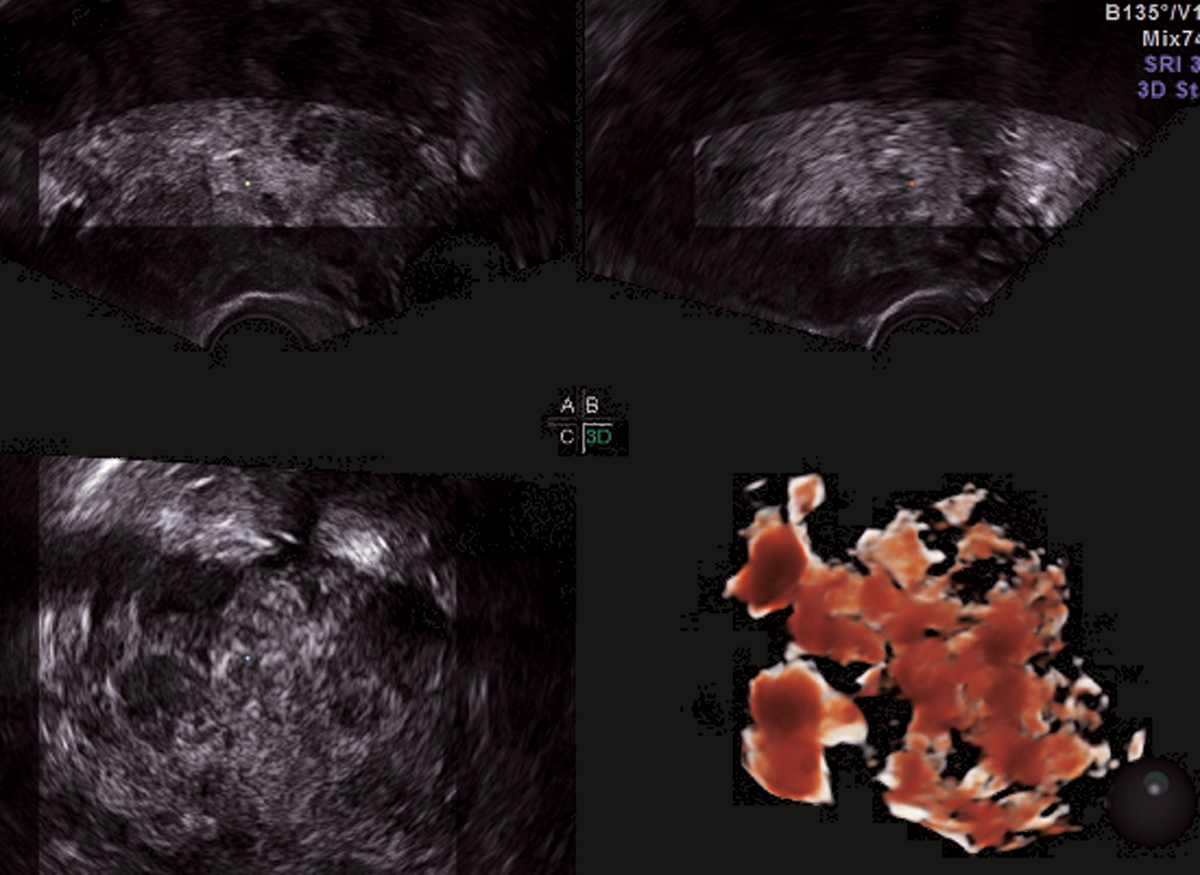
Transvaginal ultrasound revealed a large solid non-uniform diffuse uterine mass with irregular margins measuring 15.1×9.8×9.6 cm according to the Morfological Uterus Sonographic Assesment (MUSA) group [Van den Bosch T, et al. Ultrasound Obstet Gynecol 2015; 46: 284–298]. The minimum distance from the lesion to the endometrium (inner lesion-free margin) was 12 mm. Additionally, Doppler ultrasound revealed low resistance vessels within the uterine tumor. Pelvic magnetic resonance imaging (MRI) was performed for further evaluation.; T2-weighted sequences displayed an irregular uterine mass composed of many incompletely confluent nodules ([Fig. 1]). At this time, the differential diagnosis included leiomyomas with unusual growth patterns. In an attempt to specify the diagnosis more exactly, a three-dimensional HDlive (High Definition) ultrasound (Voluson E8, GE Healthcare, Madrid, Spain) was performed, revealing a uterine tumor that despite its irregular appearance had sharp edges. Additionally, when the light source was positioned in the posterior setting of the uterine tumor, the interior of the tumor appeared composed of many partially-confluent patchy nodules of different sizes, resembling the cotyledons of the maternal face of the placenta ([Fig. 2]). Additionally, estimation of tumor volume (759 mm3) and power Doppler vascularization index (VI: 0.8%), flow index (FI: 41.9) and vascularization flow index (VFI: 0.5) were generated using the software Virtual Organ Computer-aided AnaLysis (VOCAL). On the basis of these findings, a cotyledonoid dissecting leiomyoma was considered.

The patient was informed regarding the different possible treatments. After counseling, the patient opted for conservative uterine surgery intended to preserve fertility. The patient was prescribed ulipristal acetate (UPA) (Esmya®) 5 mg/day and iron supplements for 3 months in order to control uterine bleeding and to restore hemoglobin and hematocrit levels before the surgery. At completion of UPA therapy, the patient presented in our outpatient clinic for a pre-surgical US examination. She reported amenorrhea and slight pelvic pain during the entire treatment. Transvaginal 3D US examination revealed a significant reduction in tumor volume (471 mm3) and Doppler vascularization index (VI: 0.4%, FI: 31.5,VFI: 0.2). Likewise, the anemia had been corrected. At the time of laparotomy, a normal uterus was seen and a soft irregular lesion was observed at the fundus of the uterus. To maintain fertility, the tumor was excised by myomectomy ([Fig. 3]).

#
Discussion
Uterine leiomyomas may exhibit a diversity of growth patterns other than the typical appearance of a well-circumscribed, uniformly expansile tumor. Myomas with such unusual growth pattern include diffuse leiomyomatosis of the uterus, leiomyoma with vascular invasion, intravenous leiomyomatosis, benign metastasizing leiomyoma, parasitic leiomyoma, disseminated peritoneal leiomyoma, dissecting leiomyoma and leiomyomas with perinodular hydropic degeneration [Ip PP, et al. Adv Anat Pathol 2010; 17: 91–112].
Cotyledoniod dissecting leiomyoma is a distinctive variant of dissecting leiomyoma that is characterized by reddish, exophytic, placenta-like gross appearance and by its frequent extrauterine extension into the adjacent tissues and pelvic cavity [Smith CC. Int J Surg Pathol 2012; 20: 330–341]. The ultrasonographic and radiological (MRI) features of cotyledoniod dissecting leiomyoma are not particularly different from those of typical myomas. Nevertheless, the 3D ultrasound reconstruction of this uterine tumor seems to be more specific, as it is depicted by one or more large and lobulated masses with many partially confluent patchy nodules of different sizes, delimited by an irregular capsule [Raga F et al. Cotyledonoid dissecting leiomyoma of the uterus. Fertil Steril 2009; 91: 1269–1270]. The recent advent of HDlive technology into prenatal diagnosis, gynecology and reproductive medicine has enhanced 3D/4D ultrasound diagnosis [Raga F, et al. Ultrasound Obstet Gynecol 2016; doi: 0.1002/uog.15727]. In our case, HDlive imaging proved to be a valuable tool for lucidly investigates this uncommon uterine tumor, establishing an accurate diagnosis.
The most common treatment for this type of tumor to date has been hysterectomy, obviously influenced by its macroscopic appearance. In isolated reported cases there has been performed a partial resection (myomectomy). There is no precedent for medical treatment in this type of tumor [Smith CC. Int J Surg Pathol 2012; 20: 330–41]. Conversely, the potential therapeutic role of selective progesterone-receptor modulators (SPRMs), an additional class of progesterone-receptor (PR) ligands displaying tissue-selective agonist/antagonist/mixed activity, has been introduced into clinical practice for the treatment of conventional uterine leiomyomas. Ulipristal acetate (UPA) is an orally active synthetic SPRM, characterized by a tissue-specific partial progesterone antagonist effect. As a progesterone antagonist, UPA both inhibits the proliferation of leiomyoma cells, as well as induces apoptosis. Moreover, UPA regulates the expression of angiogenic growth factors, matrix metalloproteinases and collagen deposition in the extracellular spaces, which, consequently, impairs fibroid tissue integrity by reducing vascularization, cell proliferation and survival in leiomyoma [Courtoy GE, et al. Fertil Steril 2015; 104: 426–434].
UPA has been shown to be useful for several clinical conditions. It might be administered to patients waiting for surgery in order to achieve clinical control of the symptoms (in particular, because it prevents the worsening of anemia). Furthermore, a reduction in uterine fibroid volume is achieved. Finally, UPA may be a good option for women seeking pregnancy. Since it reduces the invasiveness of surgery, it expands woman’s fertility and improves the obstetric outcome [Donnez J, et al. Fertil Steril 2015; 103: 519–527]. Additionally, a significant reduction in fibroid vascularization has been recently described by means of 3D power Doppler ultrasound after 3 months of UPA treatment [Czuczwar P, et al. Ultrasound Obstet Gynecol 2015; 45: 744–750].
In our case, we have witnessed a response to ulipristal acetate similar to that previously described for conventional leiomyomas, both in reducing the tumor volume and vascularization. Therefore, the present report provides us with valuable information on both the diagnostic and therapeutic approach of this singular smooth muscle tumor of the uterus.
F. Raga, S. Cholvi, C. Pascual, D. Boigues, C. Sanchez, A. Cano; Spain
#
#