Keywords
3D knee MRI - isotropic resolution - multiplanar reconstruction - cartilage imaging
Although two-dimensional (2D) multiplanar fast spin-echo (FSE) acquisitions have been
the cornerstone of knee magnetic resonance imaging (MRI) for many decades, three-dimensional
(3D) MRI has been increasingly incorporated into clinical protocols as the technology
has evolved.[1]
[2]
[3]
[4]
[5]
[6]
[7]
[8]
[9]
[10] Knee MRI has often been at the forefront of evolving musculoskeletal (MSK) MRI research
and trends. The development of new 3D sequences that provide benefits over 2D acquisitions
for various applications, such as cartilage, bone, and hardware imaging, in addition
to new acceleration techniques that allow images to be acquired more quickly, has
made 3D imaging more applicable for routine knee MRI evaluation.[11]
[12]
Although most clinical protocols still use multiplanar 2D FSE imaging for primary
knee joint assessment, many practices add a single 3D isotropic or near-isotropic
acquisition, often reconstructed into multiple planes with multiplanar reconstructions
(MPRs). First used with a focus on evaluating articular cartilage to detect small
chondral lesions prone to partial volume averaging on 2D imaging, newer 3D FSE sequences
are now increasingly being performed to assess other structures, such as menisci,
ligaments, tendons, and nerves.[2]
[13]
[14]
[15] Three-dimensional sequences are especially beneficial for these evaluations because
nonorthogonal MPRs can be performed along or perpendicular to the course of these
structures.[3]
[15]
[16]
Aside from providing value in reducing partial volume averaging and offering the ability
to perform MPRs, various 3D sequences afford additional benefits for specific applications.
Three-dimensional spatially encoded MRI has a central role in many metal artifact
reduction sequences used throughout the MSK system, including the knee.[11] Compositional and quantitative MRI techniques increasingly use 3D MRI and are typically
developed for imaging of knee cartilage, usually in the research setting.[9]
[17]
[18]
[19]
[20] However, as acceleration and automation technologies continue to evolve, these advanced
imaging techniques should become more practical in a clinical workflow.[12]
[17]
[21]
[22]
[23]
[24]
[25]
[26]
[27]
In this review, we discuss 3D MRI sequences currently available for the knee, as well
as the advantages and limitations of 3D MRI relative to routine 2D knee MRI. We also
describe emerging techniques for 3D MRI, including acceleration and automated quantification
techniques.
Current Techniques
Three-dimensional spatially encoded MRI is performed by excitation of the entire imaged
volume rather than the slice-by-slice method used for 2D imaging. The typical frequency
and phase encoding are used for the in-plane resolution (voxel dimension along the
x-axis and y-axis) of the image. However, phase encoding is also used in the slice
direction (voxel dimension along the z-axis) and determines slice thickness. Three-dimensional
isotropic spatial resolution refers to the acquired resolution of the volume and indicates
that slice thickness is at or near in-plane resolution with no or little gap between
slices, allowing MPRs to be created in any desired imaging plane without substantial
loss of image resolution.
Many 3D MRI sequences have been created and investigated for MSK evaluation of the
knee ([Table 1]).[3]
[9]
[28]
[29] The availability of these various 3D sequences depends on the scanner strength and
vendor. Many of the sequences first developed for 3D knee MRI were gradient-recalled
echo (GRE) techniques because more commonly used spin-echo and FSE techniques could
not be performed in a reasonable length of time before the introduction of newer technologies.[30]
[31]
[32] Although useful for evaluating articular cartilage, GRE sequences have contrast
properties that are not well suited for evaluating other structures, such as menisci,
tendons, ligaments, and bones. GRE sequences are still commonly used in clinical practice,
however, because they are commercially available on most scanners including scanners
with lower magnetic field strengths. Advances in scanner and coil technology have
since allowed for the development of 3D FSE sequences that can achieve signal characteristics
similar to 2D FSE proton-density (PD) or T2 weighting, increasing the clinical utility
of 3D acquisitions.[33]
[34] Although these sequences allow for complete joint evaluation, their availability
is limited on older scanners, and they work best on 3-T scanners.[9]
Table 1
Summary of imaging applications of 3D imaging and types of 3D sequences used for each
application
|
Imaging application
|
3D sequences
|
|
Morphological cartilage assessment
|
3D FSE, bright fluid 3D GRE, dark fluid 3D GRE
|
|
Meniscus assessment
|
3D FSE
|
|
Nerve assessment
|
3D FSE, DW-PSIF, diffusion tensor imaging
|
|
Whole joint assessment
|
3D FSE
|
|
Metal artifact reduction[a]
|
SEMAC, MAVRIC
|
|
Segmentation
|
3D FSE, bright fluid 3D GRE, dark fluid 3D GRE
|
|
Compositional cartilage assessment[a]
[b]
|
T1ρ, T2, T2*, dGEMRIC, DWI, sodium 23
|
Abbreviations: 2D, two-dimensional; 3D, three-dimensional; dGEMRIC, delayed gadolinium-enhanced
MRI of cartilage; DW-PSIF, diffusion-weighted reversed fast imaging with steady-state
precession; FSE, fast spin-echo; GRE, gradient-recalled echo; MAVRIC, multi-acquisition
variable-resonance image combination; SEMAC, slice encoding for metal artifact correction.
a These sequences are typically nonisotropic 3D spatially encoded sequences.
b Compositional sequences typically have both 3D and 2D spatially encoded acquisition
options.
3D Gradient-recalled Echo for Morphological Assessment
Although early 3D GRE sequences had lower nonisotropic resolutions, high-resolution
isotropic or near-isotropic voxels amenable to MPRs have been available for many years.[3]
[28]
[30] Although various 3D GRE acquisitions with different types of contrast weighting
are available from different vendors, the sequences can be broadly classified into
two categories: dark fluid signal sequences and bright fluid signal sequences. Because
GRE sequences do not have a refocusing pulse, they are predisposed to susceptibility
artifacts that can limit evaluation after surgery and reduce conspicuity of bone marrow
edema signal. Additionally, the typically short echo times make these sequences subject
to magic angle artifact that limits the evaluation of low-signal curving structures
such as menisci, ligaments, and tendons. As a result, research on bright and dark
fluid GRE sequences in knee MRI has focused mainly on cartilage evaluation because
there is typically good contrast between fluid, articular cartilage, and bone.
Both bright and dark fluid 3D GRE sequences can be advantageous for the morphological
assessment of knee cartilage.[3]
[32] Many early studies found that dark fluid GRE sequences such as the 3D spoiled GRE
sequence could be used to measure articular cartilage volume and thickness with good
accuracy.[8] These high-resolution isotropic dark fluid GRE morphological sequences have often
been considered the standard for cartilage morphology assessment in the research setting,
but they can have long scan times and a compromise of resolution or quality when optimized
for clinically feasible acquisition times ([Fig. 1]). Bright fluid high-resolution 3D GRE sequences, such as the 3D double-echo steady-state
sequence, offer faster acquisition times and favorable fluid-to-cartilage contrast,
resulting in improved assessment of the cartilage surface ([Fig. 2]).[8]
[29] Many clinical practices, including our own, therefore use 3D GRE acquisitions, more
often bright fluid techniques, in addition to multiplanar 2D FSE sequences, to assess
articular cartilage on MRI scanners that do not have clinically feasible 3D FSE sequences
available (typically older systems and those with lower field strengths).
 Fig. 1 (a) Displaced intra-articular cartilage fragment (arrow) from a lateral femoral condylar
full-thickness chondral defect (not shown) is easily identified on the dark fluid
three-dimensional gradient-recalled echo sagittal image due to the large contrast
difference between the high signal of cartilage fragment and the dark fluid. (b) Two-dimensional proton-density fast spin-echo sagittal image also demonstrates the
fragment (arrow), but it is slightly less distinct because it is partially averaged
with adjacent synovial proliferation of similar intensity and is somewhat less distinct
in bright fluid.
Fig. 1 (a) Displaced intra-articular cartilage fragment (arrow) from a lateral femoral condylar
full-thickness chondral defect (not shown) is easily identified on the dark fluid
three-dimensional gradient-recalled echo sagittal image due to the large contrast
difference between the high signal of cartilage fragment and the dark fluid. (b) Two-dimensional proton-density fast spin-echo sagittal image also demonstrates the
fragment (arrow), but it is slightly less distinct because it is partially averaged
with adjacent synovial proliferation of similar intensity and is somewhat less distinct
in bright fluid.
 Fig. 2 A large osteochondral lesion of the medial femoral condyle with bright fluid (white
arrowhead) undercutting an intra-articular osteochondral fragment is well visualized
(a) on the sagittal fat-saturated two-dimensional (2D) proton-density (PD) fast spin-echo
(FSE) and (b) on the bright fluid three-dimensional (3D) gradient-recalled echo (GRE) double-echo
steady-state sequences. Associated bone marrow edema (white arrow) is prominent (a)
on the 2D PD FSE image but is less conspicuous (b) on the 3D GRE image.
Fig. 2 A large osteochondral lesion of the medial femoral condyle with bright fluid (white
arrowhead) undercutting an intra-articular osteochondral fragment is well visualized
(a) on the sagittal fat-saturated two-dimensional (2D) proton-density (PD) fast spin-echo
(FSE) and (b) on the bright fluid three-dimensional (3D) gradient-recalled echo (GRE) double-echo
steady-state sequences. Associated bone marrow edema (white arrow) is prominent (a)
on the 2D PD FSE image but is less conspicuous (b) on the 3D GRE image.
3D Fast Spin Echo for Morphological Assessment
Most vendors now offer 3D FSE sequences that use techniques such as parallel imaging,
variable flip angles, long echo trains, and partial k-space filling to achieve clinically
feasible imaging times.[33]
[34] Because 3D FSE acquisitions rely on acceleration techniques that decrease image
signal-to-noise ratio (SNR) to reduce acquisition times, these techniques perform
better on 3-T systems because they produce images with inherently higher signal than
lower strength MRI systems and can therefore better compensate for signal loss or
noise. The reported diagnostic performance of 3D FSE, including for cartilage, has
been lower on 1.5-T systems than on 3-T systems.[1]
[2]
[4]
[5]
[35]
Three-dimensional FSE sequences can be performed using a variety of image contrast
techniques. Intermediate-weighted 3D FSE acquisitions can produce images with signal
properties similar to those seen with the PD-weighted sequences typically used for
2D knee MRI. This allows for the use of 3D FSE sequences to assess not only cartilage
but also structures such as bone marrow, menisci, tendons, and ligaments while still
providing high-resolution isotropic or near-isotropic evaluation. As a result, 3D
FSE sequences provide a more global joint assessment, an important advantage over
3D GRE sequences.[1]
[2] These isotropic 3D FSE sequences also maintain the ability to minimize partial volume
averaging while allowing MPRs to be performed ([Fig. 3]).
 Fig. 3 A high-grade patellar chondral fissure (arrow) is well visualized (a) on the fat-saturated sagittal three-dimensional fast spin-echo (FSE) sequence (0.6-mm
slice thickness) but is not as well visualized on (b) a corollary two-dimensional proton-density FSE sequence (2.8-mm slice thickness)
because of partial volume averaging.
Fig. 3 A high-grade patellar chondral fissure (arrow) is well visualized (a) on the fat-saturated sagittal three-dimensional fast spin-echo (FSE) sequence (0.6-mm
slice thickness) but is not as well visualized on (b) a corollary two-dimensional proton-density FSE sequence (2.8-mm slice thickness)
because of partial volume averaging.
Many studies have therefore evaluated the feasibility of replacing traditional multiplanar
2D sequences with a single 3D FSE acquisition for a faster diagnostic global knee
joint assessment.[4]
[5]
[6]
[7]
[36]
[37] Although most of these studies have shown that the diagnostic abilities of 3D FSE
sequences are for the most part similar to those of 2D FSE sequences, we are not aware
of any large institution that has replaced its 2D protocol with a single 3D FSE sequence.
Rather, evolving MRI acceleration techniques for both 2D and 3D sequences now allow
for acquisition of both multiplanar 2D sequences and high-resolution 3D FSE knee MRI
sequences in a feasible time. At our institution, our routine knee protocol on 3-T
scanners consists of five 2D FSE sequences and a 3D FSE sequence obtained using parallel
imaging in a total acquisition time of ∼ 10 minutes.
Compositional Knee MRI
Compositional cartilage imaging is one of the most studied applications of 3D MRI
techniques in the knee.[9]
[17]
[19]
[38] Most often performed in the research setting, compositional imaging involves creating
a cartilage parameter map based on measurements of specific MR parameters over time
that can then be used (depending on the compositional sequence employed) to infer
the intrinsic biochemical properties of the articular cartilage, including water content,
glycosaminoglycan and proteoglycan content, and type II collagen network integrity.
Essentially all compositional techniques, including T2* maps, T1ρ, delayed gadolinium-enhanced
MRI of cartilage (dGEMRIC), diffusion-weighted imaging (DWI), T2, and sodium 23 MRI,
have been investigated with 3D spatially encoded acquisitions.[9]
[17]
[19]
Typically, a high-resolution isotropic 3D GRE or 3D FSE sequence is obtained alongside
a compositional map sequence, which can be a 3D or 2D spatially encoded acquisition.[23]
[39]
[40] Cartilage segmentation is then performed, usually using the high-resolution isotropic
3D sequence, and the segmentation is registered to the compositional map that typically
consists of thicker slices because of SNR or acquisition limitations. For T2* mapping,
however, high-resolution isotropic maps can often be obtained.[9]
[41] Of these compositional techniques, only T2, T2*, and T1 (dGEMRIC) maps are currently
available for clinical systems. The long acquisition times of these compositional
sequences and the manual or semi-manual cartilage segmentation required have prevented
more widespread clinical adoption of these techniques. However, new accelerated imaging
techniques and automated cartilage segmentation using machine learning show promise
for future clinical integration.
Metal Artifact Suppression
Another rapidly expanding clinical application for these 3D encoded techniques is
the reduction of metal artifacts when scanning a patient with hardware such as knee
arthroplasties. Advanced metal artifact reduction techniques use 3D spatially encoded
MRI techniques to reduce through-plane artifact. For instance, the multi-acquisition
variable-resonance image combination (MAVRIC) sequence directly uses 3D excitation
and 3D readout pulses.[11]
[26] Slice encoding for metal artifact correction (SEMAC), in contrast, uses a 2D excitation
pulse with a 3D readout pulse.[11] These sequences have been shown to reduce hardware artifact markedly when compared
with traditional techniques to reduce metal artifact (e.g., using FSE sequences and
increasing receiver bandwidth). Given the increased magnetization of hardware at higher
field strengths, these sequences are most effective when employed on 1.5-T systems
rather than on 3-T systems. The long acquisition time required is the primary limitation
of this technique, although new acceleration techniques using compressed sensing can
substantially reduce imaging times.[26]
MRI Neurography
Three-dimensional MRI techniques can also be useful for assessing peripheral nerves,
including nerves around the knee.[14]
[15]
[42] T2-weighted isotropic 3D FSE MRI sequences with various fat-suppression techniques
are increasingly being incorporated into clinical peripheral neurography protocols.
Although not specifically optimized for neurography, isotropic 3D FSE sequences commonly
included in clinical knee MRI protocols are often acquired with similar fluid-sensitive
weighting and fat suppression that allow for high-resolution assessment of the nerves
and the ability to perform MPRs ([Fig. 4]). Vessel signal suppression is a technique often used in MRI neurography sequences
to isolate signal from the nerves within the neurovascular bundle.[43]
 Fig. 4 (a) For a patient with peroneal nerve symptoms after an injury, the entire course of
the common peroneal nerve is visualized on a single image with a curved multiplanar
reconstruction (MPR) using a three-dimensional fast spin-echo sequence acquired as
part of a standard knee protocol, demonstrating segmental nerve fascicle enlargement
and increased signal (white arrowheads) proximal to the fibula relative to the normal
signal and caliber of the more proximal and distal portion of the nerve (black arrows),
consistent with neuritis. (b) The subacute healing nondisplaced proximal fibular fracture (white arrow) is also
well depicted on a thick nonorthogonal MPR along the long axis of the fibula, oblique
to the routine sagittal plane; the fracture was occult on radiographs at the time
of the trauma. A reference image (top right corner) is provided to demonstrate the
referenced nonorthogonal planes used to create an optimized MPR. Fe, femur; Fi, fibula.
Fig. 4 (a) For a patient with peroneal nerve symptoms after an injury, the entire course of
the common peroneal nerve is visualized on a single image with a curved multiplanar
reconstruction (MPR) using a three-dimensional fast spin-echo sequence acquired as
part of a standard knee protocol, demonstrating segmental nerve fascicle enlargement
and increased signal (white arrowheads) proximal to the fibula relative to the normal
signal and caliber of the more proximal and distal portion of the nerve (black arrows),
consistent with neuritis. (b) The subacute healing nondisplaced proximal fibular fracture (white arrow) is also
well depicted on a thick nonorthogonal MPR along the long axis of the fibula, oblique
to the routine sagittal plane; the fracture was occult on radiographs at the time
of the trauma. A reference image (top right corner) is provided to demonstrate the
referenced nonorthogonal planes used to create an optimized MPR. Fe, femur; Fi, fibula.
Although 3D FSE sequences intrinsically suppress signal in high-flow velocity vessels,
such as arteries, due to low refocusing pulses that are sensitive to motion, the venous
signal usually remains predominantly bright and may obscure or confound nerve assessment.
Dedicated 3D FSE peripheral neurography protocols use fat-suppressed T2-weighted sequences
with dedicated pulse techniques or T1 shortening intravenous gadolinium contrast to
further suppress blood signal from veins.[13]
[42] Three-dimensional DWI techniques can also be used to suppress the vascular signal
and enhance the nerve signal, allowing these techniques to be employed for isotropic
peripheral neurography protocols; however, these DWI techniques are limited by sensitivity
to field inhomogeneities and motion.[43] Diffusion tensor imaging, which uses anisotropy of diffusion that occurs along a
nerve to visualize the course of the nerve (fiber tractography), is another 3D technique
that can be used for MR neurography, but this technique requires considerable optimization
and postprocessing time to yield productive images, thus limiting its clinical use
([Fig. 5]).
 Fig. 5 Rendered magnetic resonance diffusion tensor imaging of the sciatic nerve demonstrates
and differentiates between disrupted nerve fibers (arrows) and intact nerve fibers
in a patient with a gunshot injury of the thigh.
Fig. 5 Rendered magnetic resonance diffusion tensor imaging of the sciatic nerve demonstrates
and differentiates between disrupted nerve fibers (arrows) and intact nerve fibers
in a patient with a gunshot injury of the thigh.
Advantages
Decreased Partial Volume Averaging
A primary advantage of high-resolution 3D MRI when compared with 2D FSE MRI is a reduction
in partial volume averaging artifacts in the slice direction.[3]
[28] Isotropic or near-isotropic resolution 3D sequences have cube-shaped voxels with
a slice thickness that is nearly or completely equivalent to the in-plane resolution.
Two-dimensional sequences, in contrast, have rectangular-shaped voxels with a slice
thickness that is typically five to nine times greater in the slice direction than
the in-plane resolution. These larger voxels result in a predisposition to partial
volume averaging of MR signal along the slice direction. Although this averaging has
the benefit of increasing SNR in thicker 2D images, it can also blend together different
anatomical structures and signals that can obscure potentially clinically relevant
pathology or artifactually create the appearance of pathology in otherwise normal
anatomy. This is particularly true for small structures with curved or anatomically
oblique orientations, such as articular cartilage or menisci in the knee.[16]
Morphological assessment of articular cartilage is the most common reason for including
a 3D acquisition in knee MRI examinations in both the clinical and research settings.
Both 3D GRE and 3D FSE sequences can be helpful in evaluating articular cartilage,
due in large part to decreased partial volume averaging. Numerous studies have evaluated
cartilage assessment using a variety of 3D FSE sequences from different vendors, and
a comprehensive meta-analysis of these studies in 2018 found that 3D FSE sequences
were more sensitive and specific than multiplanar 2D FSE protocols for cartilage assessment.[1] Although 3D FSE sequences have advantages over 3D GRE sequences for cartilage assessment,
the contrast difference between articular cartilage and fluid, especially on bright
fluid GRE sequences, was shown to increase sensitivity for detecting superficial partial-thickness
cartilage lesions.[8]
[29]
Three-dimensional GRE sequences have also been found to increase specificity when
used as a supplement to 2D FSE sequences. However, 3D GRE sequences have lower sensitivity
for the detection of cartilage lesions overall when compared with 2D FSE sequences
alone, in part because of poor conspicuity of subchondral marrow signal changes (an
important secondary marker of adjacent chondral pathology) ([Fig. 2]).[1]
[8]
Decreased partial volume averaging can also be a benefit when evaluating other structures
in the knee, such as menisci. Most studies have found that 3D FSE and 2D sequences
offer comparable diagnostic accuracy for detecting meniscus pathology.[2] Thus 3D imaging can be particularly helpful in detecting small radial tears that
can be obscured by partial volume averaging on 2D images but are more apparent on
3D images.[3]
[25] Similarly, 3D imaging can be helpful in diagnosing normal meniscal flounce, which
can mimic a tear on 2D images because of partial volume averaging. At our institution,
we routinely obtain a high-resolution 3D FSE sequence (when available) or a 3D GRE
sequence that is typically bright fluid to assess articular cartilage and menisci.
Multiplanar Reconstructions
Another important advantage of high-resolution isotropic 3D knee MRI is the ability
to create MPRs in any imaging plane without a substantial loss of in-plane image resolution,
thus obviating the need to acquire multiple sequences in different imaging planes,
as required with 2D imaging. These 3D sequences can be used to either replace 2D multiplanar
sequences or to supplement them. With the advent of 3D FSE sequences and their ability
to provide contrast similar to that of 2D FSE sequences, multiple studies have evaluated
knee MRI protocols consisting of only one or two 3D FSE sequences.[4]
[36] The main advantage of such a protocol is that it can substantially reduce acquisition
time when compared with standard protocols consisting of multiple 2D FSE sequences
in the axial, coronal, and sagittal planes. Using isotropic 3D acquisitions would
also eliminate difficulties or the need for repeat acquisitions due to incorrect imaging
plane prescriptions by technologists, a problem especially common in the setting of
oblique or radial planes.
Although studies have shown that the diagnostic performance for this type of 3D FSE
protocol is similar to that of standard 2D protocols, we are unaware of any institution
that has replaced its 2D sequences in favor of one or two 3D sequences with MPR reformations,
likely because of the disadvantages associated with a 3D protocol, discussed later.
Instead, 3D MRI with MPRs more commonly supplement 2D sequences obtained in standard
planes. One of the most common uses of 3D MPRs is to generate images along nonorthogonal
planes to better depict anatomical structures coursing in oblique or radial orientations
that otherwise would necessitate additional 2D acquisitions.[16] These reconstructions can be created with any desired slice thickness to optimize
the balance of SNR lost from thinner slices with the partial volume averaging artifacts
that result from thicker slices. Most clinical picture archive and communication systems
offer the radiologist the option to manipulate and view the 3D data set interactively
with MPRs to optimally display and highlight pathology for the particular study at
hand without the need to explicitly export additional images.
For articular cartilage, nonstandard planes can be of particular utility in analyses
of the trochlea and posterior femoral condyles. Studies have demonstrated that 1-mm-thick
radial reformats of 3D FSE acquisitions for evaluation of the curved surface of the
femoral condyles can improve the accuracy of articular cartilage evaluation when compared
with 2D sequences and orthogonal 3D FSE reconstructions ([Fig. 6]).[16]
 Fig. 6 (a) A moderate-sized full-thickness chondral fissure/defect in the lateral trochlea
(arrow) is well visualized and characterized on a thin three-dimensional (3D) fast
spin-echo (FSE) axial oblique multiplanar reconstruction (MPR) due to optimal orientation
of the imaging plane perpendicular to the curved articular surface of the trochlea
at the site of the defect. (b) The same lesion (arrow) is suboptimally characterized on the two-dimensional (2D)
T2-weighted FSE standard axial sequence due to partial volume averaging with adjacent
cartilage as a result of thicker slices and oblique orientation of the imaging plane
through the defect. A sagittal reference image (a, lower right corner) demonstrates
the thinner 3D MPR plane (thin line) and the thicker standard axial 2D plane (thick
dashed line).
Fig. 6 (a) A moderate-sized full-thickness chondral fissure/defect in the lateral trochlea
(arrow) is well visualized and characterized on a thin three-dimensional (3D) fast
spin-echo (FSE) axial oblique multiplanar reconstruction (MPR) due to optimal orientation
of the imaging plane perpendicular to the curved articular surface of the trochlea
at the site of the defect. (b) The same lesion (arrow) is suboptimally characterized on the two-dimensional (2D)
T2-weighted FSE standard axial sequence due to partial volume averaging with adjacent
cartilage as a result of thicker slices and oblique orientation of the imaging plane
through the defect. A sagittal reference image (a, lower right corner) demonstrates
the thinner 3D MPR plane (thin line) and the thicker standard axial 2D plane (thick
dashed line).
The menisci can be similarly assessed with nonorthogonal MPRs. Radial reconstructions
of 3D FSE sequences perpendicular to the curved course of the menisci can supplement
assessment and characterization of meniscal tears and meniscal extrusion, particularly
in regions that are suboptimally assessed in standard imaging planes, such as the
root or the junctions of the body with the posterior and anterior horns ([Fig. 7]).[3]
[25] Additionally, some tear types, particularly radial tears, can be best appreciated
on 3D isotropic MPRs oriented axially to the meniscal curvature that may not match
the plane of orthogonal 2D axial images.
 Fig. 7 Radial multiplanar reconstructions (MPRs) perpendicular to the entire semicircular
course of the menisci generated using a three-dimensional (3D) viewer tool available
on the picture archive and communication system from a 3D fast spin-echo (FSE) acquisition
demonstrates (a) a posterior root meniscus tear (arrow) with (b) early meniscal extrusion (arrow) optimally compared with standard orthogonal coronal
and sagittal two-dimensional planes (not shown). A reference image (b, top left corner)
is provided to demonstrate the referenced nonorthogonal planes used to create the
optimized radial MPRs.
Fig. 7 Radial multiplanar reconstructions (MPRs) perpendicular to the entire semicircular
course of the menisci generated using a three-dimensional (3D) viewer tool available
on the picture archive and communication system from a 3D fast spin-echo (FSE) acquisition
demonstrates (a) a posterior root meniscus tear (arrow) with (b) early meniscal extrusion (arrow) optimally compared with standard orthogonal coronal
and sagittal two-dimensional planes (not shown). A reference image (b, top left corner)
is provided to demonstrate the referenced nonorthogonal planes used to create the
optimized radial MPRs.
Three-dimensional MPRs can also help assess ligaments and tendons of the knee that
often course in nonorthogonal planes. For example, some institutions obtain oblique
sagittal images along the course of the anterior cruciate ligament to improve visualization
of the ligament; however, this protocol is not ideal for evaluating the femoral condyle
cartilage, thereby necessitating the acquisition of two 2D sagittal sequences. With
a 3D FSE sequence, both sagittal oblique and axial oblique MPR images along the course
of the anterior cruciate ligament can be generated if needed. Similarly, MPRs or curved
reconstructions along the long or short axis of a coursing tendon can be used to optimize
visualization of tendon pathology.
At our institution, we acquire 3D FSE or GRE sequences with submillimeter voxels in
the sagittal plane and create 1-mm-thick straight sagittal, straight coronal, and
oblique axial reformats to balance the improved resolution of the thinner slices with
the improved SNR of the thicker slices. Axial oblique images oriented perpendicular
to the trochlea simultaneously improve the visualization of the trochlear cartilage,
the anterior cruciate ligament, and the meniscal roots that are all oriented along
a similar plane.
Segmentation and Quantitative Assessment
Isotropic 3D morphological sequences are also well suited for segmentation, particularly
for volumetric analyses or surface rendering.[23]
[32]
[39]
[44]
[45] Additionally, isotropic resolution for segmentation minimizes registration errors
and eliminates the need to segment the same anatomy in multiple planes.
The high out-of-plane resolution of isotropic 3D FSE or GRE sequences is particularly
well suited for segmentation of small or thin anatomical structures, such as articular
cartilage, given the many curved surfaces of the knee prone to partial volume averaging.
Segmentation not only allows for measurement of cartilage thickness and volume but
is also a prerequisite step for compositional analysis of articular cartilage.[39] As such, these isotropic sequences are often used alongside 2D or 3D spatially encoded
compositional map acquisitions. Although compositional articular cartilage sequences
are currently not used in most clinical environments because of the time-consuming
process required to segment articular cartilage, the development of fully automated
segmentation techniques is bringing these sequences closer to implementation in routine
clinical practice.[23]
[39]
Along the same lines, segmentation and surface rendering of bones using 3D imaging
are increasingly being used for preoperative planning.[3] Traditionally, computed tomography (CT) was used to generate bone models. Recent
studies, however, have shown that several isotropic or near-isotropic 3D MRI sequences
can be used instead of CT. Using these 3D MRI sequences not only eliminates the need
to perform an additional study but also the need to expose patients to ionizing radiation.
At our institution, for example, we have found that a 3D two-point Dixon sequence
is interchangeable with CT for preoperative planning for femoroacetabular surgery
in the hip, although we currently do not explicitly use 3D MRI for this purpose in
the knee. Nonetheless, optimized MPRs can allow for excellent diagnostic assessment
of osseous structures, particularly with 3D FSE sequences for obliquely oriented anatomy
([Fig. 4]).
Metal Artifact Reduction
Three-dimensional MRI sequences can also be used to reduce metal artifact.[11] Although traditional 2D FSE optimization techniques, such as increasing receiver
bandwidth, are helpful in reducing in-plane distortions caused by metal hardware,
they do not correct for through-plane distortions along the slice direction. New advanced
metal artifact reduction sequences, such as MAVRIC and SEMAC, in contrast, use 3D
spatial encoding techniques to correct not only for in-plane distortions but also
for through-plane distortions. The use of these 3D MRI sequences for metal artifact
reduction was shown to improve the detection of hardware complications such as osteolysis,
periprosthetic fractures, fluid collections, and soft tissue masses. These sequences
can also be helpful for assessing intra-articular structures, such as articular cartilage,
menisci, and ligaments, that would otherwise be obscured by metal artifact in the
setting of a unicompartmental knee arthroplasty ([Fig. 8]). These 3D metal artifact reduction sequences, now available through multiple vendors,
are replacing standard 2D FSE sequences for imaging joints in patients with metal
hardware. At our institution, we routinely use SEMAC sequences instead of standard
2D sequences when imaging patients with knee arthroplasties or metal hardware around
the knee.
 Fig. 8 (a) Metal artifact from a patellofemoral compartment arthroplasty obscures visualization
of the metal–bone interface (arrow) of the trochlear implant on a two-dimensional
high-bandwidth short tau inversion recovery (STIR) sagittal image. (b) A corollary sagittal STIR image from an advanced three-dimensional metal artifact
reduction sequence using slice encoding for metal artifact correction (SEMAC) allows
clear visualization of the metal–bone interface (arrow) due to reduction of through-plane
metal artifact.
Fig. 8 (a) Metal artifact from a patellofemoral compartment arthroplasty obscures visualization
of the metal–bone interface (arrow) of the trochlear implant on a two-dimensional
high-bandwidth short tau inversion recovery (STIR) sagittal image. (b) A corollary sagittal STIR image from an advanced three-dimensional metal artifact
reduction sequence using slice encoding for metal artifact correction (SEMAC) allows
clear visualization of the metal–bone interface (arrow) due to reduction of through-plane
metal artifact.
Imaging of Nerves
The high spatial resolution of isotropic 3D sequences is also beneficial when evaluating
peripheral nerves that are typically small in caliber and course in nonorthogonal
planes. Isotropic 3D FSE sequences have shown particular promise for the evaluation
of nerves ([Fig. 4]). Three-dimensional FSE sequences, despite being optimized for the evaluation of
articular cartilage, ligaments, and tendons, are similar to 3D FSE protocols optimized
for dedicated MR neurography techniques used to evaluate peripheral nerves. Dedicated
3D MR neurography sequences, such as diffusion-weighted reversed fast imaging with
steady-state precession, can suppress signal from vessels to highlight the nerves
and provide excellent assessment of peripheral nerves around the knee.[13]
[42] Regardless of the type of 3D sequence used, optimized MPRs can be of use for assessing
the sciatic nerve and branches, as well as the common peroneal nerve and branches
along the curved course around the fibular head. These MPRs can also be used to create
thicker maximum intensity projection slabs to visualize a large segment of a nerve
on a single image. At our institution, we use a near-isotropic 3D FSE sequence as
part of our MR neurography protocol; from this sequence, nonorthogonal and curved
MPRs can be generated along the course of the nerve of interest.
Limitations
Time Limitations
One of the biggest barriers to incorporating 3D knee MRI sequences into routine clinical
practice is the long acquisition time.[10]
[30] This is particularly true in the case of high-resolution submillimeter isotropic
or near-isotropic 3D FSE acquisitions that can take > 8 minutes to acquire. This is
a substantially longer acquisition time than required for a single 2D FSE acquisition.
Because 3D sequences are currently most often used to augment rather than replace
2D sequences, the incorporation of a 3D sequence into the routine protocol results
in added imaging time. Long acquisition times can also increase the potential for
motion artifacts, and it may be problematic if repeat acquisition is necessary. As
a result, many practices do not routinely obtain a 3D sequence as part of the knee
protocol. Emerging techniques to accelerate 3D image acquisition hold the promise
to lower this barrier; these techniques are discussed later.
MPRs also require additional postprocessing time either by the technologist or by
the radiologist. Additionally, although thinner slices result in decreased volume
averaging, they also result in many more images that need interpretation. The image
count can increase from twofold to fivefold, depending on the thickness of the MPR
images and the number of reconstruction planes generated, which can increase interpretation
time.
Contrast Weighting and Single Acquisition
One of the main advantages of standard multiple-plane 2D knee MRI protocols is that
they include sequences with different image contrast weightings. Most protocols include
sequences with PD weighting for optimized evaluation of menisci and cartilage, T2
weighting for optimized evaluation of tendons and ligaments, and T1 weighting for
optimized evaluation of marrow. Along the same lines, most standard 2D protocols include
both fat-saturated sequences to increase conspicuity of edema and non–fat-saturated
sequences to improve anatomical detail.
In contrast, a 3D sequence with MPRs is limited to a single contrast-weighting and
fat-suppression technique. Although 3D FSE sequences can reproduce PD weighting, T2
weighting, and T1 weighting, the use of just one contrast-weighting technique limits
the ability of this sequence to optimally evaluate all of the structures in the knee.
Furthermore, in the case of 3D GRE sequences, the contrast-weighting technique is
dissimilar to PD-weighted, T2-weighted, and T1-weighted sequences in that there is
more T2* dependence, and so the use of this sequence is limited for global joint assessment.
Similarly, images with fat saturation and without fat saturation offer distinct advantages
and disadvantages, depending on the pathology. Although most studies have found that
a single 3D FSE sequence protocol with MPRs has diagnostic performance similar to
that of a standard multiple-plane 2D protocol, some studies have shown decreased sensitivity
of both 3D GRE sequences and, in a few studies, 3D FSE sequences for detecting meniscal
tears, likely related to suboptimal contrast weighting ([Fig. 9]).[2]
[5]
[37]
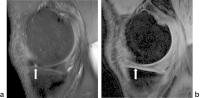 Fig. 9 (a) Sagittal proton-density-weighted two-dimensional sequence clearly demonstrates a
radial tear (arrow) in the anterior inner margin of the medial meniscus. (b) This tear (arrow) is not well visualized on a corollary three-dimensional gradient-recalled
echo sequence because of poor meniscus–fluid contrast.
Fig. 9 (a) Sagittal proton-density-weighted two-dimensional sequence clearly demonstrates a
radial tear (arrow) in the anterior inner margin of the medial meniscus. (b) This tear (arrow) is not well visualized on a corollary three-dimensional gradient-recalled
echo sequence because of poor meniscus–fluid contrast.
Although a single 3D sequence protocol may therefore not be the answer to replace
2D sequences, studies showed it may be more feasible to use a protocol with two accelerated
3D FSE sequences in lieu of 2D sequences.[36] At this time, however, we are not aware of any large practice that has replaced
its standard knee protocol with a protocol consisting only of 3D sequences.
Diagnostic and Quality Limitations of Isotropic 3D MRI
Apart from imaging time and contrast weighting, there are other diagnostic limitations
to isotropic 3D knee MRI imaging for both GRE and FSE sequences. Although the out-of-plane
spatial resolution of 3D sequences is much higher than that of 2D sequences, the in-plane
resolution of 3D sequences is usually slightly lower than for 2D sequences.[4]
[5] Additionally, the smaller voxels, due to thinner slices in 3D acquisitions, result
in overall decreased signal in each voxel that reduces SNR. SNR is often further reduced
due to undersampling acceleration techniques that are often required to obtain 3D
FSE sequences within a feasible time. Although these limitations can be partially
overcome by using 3-T systems and by creating MPRs with thicknesses that optimize
the balance between SNR and partial volume averaging, the image quality of 2D sequences
is often still superior to that of 3D sequences.[12]
Additionally, for 3D GRE sequences, susceptibility artifact from the absence of a
refocusing pulse limits the ability of these sequences to evaluate areas prone to
this artifact, such as in the presence of hardware or in the bone marrow ([Fig. 2]).[32] Decreased bone marrow edema signal on GRE images not only limits the ability of
these sequences to identify bone pathology but also affects their ability to evaluate
articular cartilage. The decreased conspicuity of subtle subchondral marrow signal
changes that can help identify overlying cartilage abnormalities has been hypothesized
as the reason why 3D GRE sequences are less sensitive for identifying cartilage lesions
than 2D sequences, despite having thinner slices with less partial volume averaging.[3] Short echo times with 3D GRE sequences can also result in magic angle artifacts
when evaluating obliquely coursing structures such as tendons.
Because of these limitations with 3D GRE sequences, most practices have replaced 3D
GRE sequences with 3D FSE sequences when available. However, 3D FSE sequences also
have limitations, including image blurring, caused by the long echo train lengths
and undersampling techniques used to reduce acquisition time.[32] Meta-analyses showed that only articular cartilage evaluation is improved with the
use of 3D FSE sequences, whereas evaluations of other structures, such as menisci,
ligaments, and bone marrow, remain comparable with evaluations with 2D sequences.[1]
[2] Some studies have demonstrated marginally better performance for some meniscal tear
subtypes with multiplanar 2D sequences than with 3D FSE sequences, although these
findings have not been consistent and have not demonstrated any measurable differences
in meta-analyses.[5]
[37] Interestingly, it remains unclear whether 3D FSE sequences reconstructed with thicker
slices (similar to those used in 2D sequences) also have a diagnostic performance
similar to that of 2D sequences. As a result of these limitations, 3D FSE sequences
are typically used in addition to 2D FSE rather than as a replacement.
Emerging Techniques
Recent advances in MRI acceleration technologies and techniques have been instrumental
to the advancement of 3D knee MRI. Compared with 2D acquisition, 3D acquisition is
better suited for acceleration techniques such as parallel imaging and compressed
sensing.[12]
[25]
[27]
[38] This has influenced the growth and adoption of 3D FSE sequences over the past decade,
and more recently, this has expanded to other applications such as compressed sensing
metal artifact reduction sequences.[26] Broadly, all acceleration techniques rely on undersampling of data that results
in a decrease in SNR and an increase in artifacts. The primary challenge in the development
of accelerated sequences is maintaining diagnostic image quality. As in 2D imaging,
sequence optimization in 3D imaging often depends on identifying parameters that balance
the acquisition time, image resolution, and SNR to suit the clinical needs. As such,
although acceleration techniques are often considered successful when continuing to
yield diagnostic images with shorter acquisition times, they can also ultimately be
used to obtain images with similar scan times but with more optimized parameters,
such as higher resolution.
The most widely used acceleration technique currently is parallel imaging, a key component
of 3D FSE sequences.[12] Parallel imaging reduces acquisition time by decreasing the number of phase-encoding
steps acquired and using the spatial sensitivity of multichannel surface coils to
unfold the resultant aliased signal.[38] This unfolding can be performed in the image domain, termed sensitivity encoding,
or in the k-space domain, termed generalized autocalibrating partial parallel acquisition
(GRAPPA). Although both techniques have their unique advantages and disadvantages,
they are largely interchangeable. One of the main advantages of the parallel imaging
technique is that it is applicable to a broad range of acquisition types, including
FSE and GRE sequences, 2D and 3D acquisitions, and compositional imaging techniques.
The biggest drawback of this technique is that it results in a reduction in the SNR
by a factor roughly the square root of the acceleration factor. To minimize the effect
of this SNR loss on image quality, it is highly beneficial to start with high SNR
images, such as those obtained on 3-T systems. Even at 3 T, however, the loss in SNR
usually prohibits acquisition acceleration beyond a factor of 2.
Submillimeter isotropic 3D FSE sequences using parallel imaging with an acceleration
factor of 2 can have acquisition times too long for clinical protocols, sometimes
requiring ≥ 8 minutes. More recently, however, a parallel imaging technique with an
acceleration factor of 4 became available for 3D FSE techniques, termed CAIPIRINHA
(Controlled Aliasing in Parallel Imaging Results in Higher Acceleration).[46] CAIPIRINHA takes advantage of the fact that phase encoding occurs in two directions
in a 3D acquisition, skipping phase-encoding steps in both directions while minimizing
the loss in SNR that typically occurs with fourfold acceleration by incorporating
a phase shift to the k-space sampling. With CAIPIRINHA, acquisition times can be reduced
to 5 minutes for a submillimeter isotropic 3D FSE acquisition with diagnostic image
quality. This shorter acquisition time provides the ability to obtain multiple 3D
FSE sequences with different contrast weightings and fat saturation techniques in
a clinically feasible time, thus partially addressing the limitations of the single-sequence
3D protocol discussed earlier. A 2018 study evaluated a 10-minute knee protocol consisting
of two 3D FSE CAIPIRINHA sequences, one with fat saturation and one without, and demonstrated
diagnostic performance comparable with that of a multiplanar 2D protocol with an acquisition
time twice as long for global joint assessment at both 1.5 T and 3 T.[36] At our institution, although we continue to use a 3D FSE sequence with standard
time optimizations and an acceleration factor of 2 for our clinical cases, we have
begun evaluating a CAIPIRINHA 3D FSE sequence with an acceleration factor of 4 in
some research studies.
Compressed sensing is another undersampling technique that has been successfully applied
to 3D FSE sequences and metal artifact reduction sequences with acceleration factors > 2.
This technique is based on the same principles used in digital image compression algorithms
that exploit inherent sparsity (lack of information) on mathematical transformations
of image data to reduce digital image size while maintaining perceived quality. Compressed
sensing uses a similar process in reverse, undersampling k-space in a pseudo-random
manner while preserving the essential data in the center of k-space, transforming
the k-space data into a domain where there is data sparsity, and then iteratively
reconstructing the data back into the image domain.[12] Like parallel imaging techniques, compressed sensing techniques are more suited
for 3D sequences that inherently have greater data sparsity than 2D sequences; this
is especially the case with metal artifact reduction sequences such as SEMAC. Compressed
sensing 3D FSE sequences have demonstrated SNR and diagnostic image quality comparable
with the SNR and image quality of standard 3D FSE sequences in the knee, although
some studies have noted image blurring as a diagnostic issue with compressed sensing.[12]
[25] Compressed sensing SEMAC sequences can substantially reduce imaging time while still
providing metal artifact reduction similar to that provided by standard SEMAC sequences.[26] At our institution, when imaging patients with arthroplasties, we have begun using
compressed sensing SEMAC sequences when available, resulting in a reduction in imaging
times.
Compressed sensing acceleration can also be applied to nonmorphological sequences,
such as some compositional cartilage imaging techniques.[47] Compositional cartilage imaging sequences, such as T2 mapping and T1ρ, traditionally
require long acquisition times (> 10 minutes), which has been a barrier to the incorporation
of these techniques into routine clinical practice. At our institution, we developed
a compressed sensing 3D T1ρ sequence with up to eightfold acceleration that permits
a whole-knee relaxometry map acquisition in 3 to 4 minutes ([Fig. 10]). Like other acceleration techniques, compressed sensing is not without its limitations.
The iterative reconstruction required for compressed sensing increases computational
hardware processing requirements and time, and the undersampling and iterative reconstruction
methods can lead to loss of details and edge sharpness.[12]
 Fig. 10 Compressed sensing can be used to decrease acquisition time of a three-dimensional
T1ρ sequence without a clinically significant difference in accuracy. Reference acquisition
using parallel imaging with an acceleration factor (AF) = 2 and a time of acquisition
(TA) = 13:43 can be reduced to TA = 6:37 (AF = 4), TA = 4:24 (AF = 6), and TA = 3:18
(AF = 8), with < 4% difference in the average coefficients of variation between reference
and accelerated sequences for all AFs. Top: whole image within field of view; bottom:
zoomed-in images.
Fig. 10 Compressed sensing can be used to decrease acquisition time of a three-dimensional
T1ρ sequence without a clinically significant difference in accuracy. Reference acquisition
using parallel imaging with an acceleration factor (AF) = 2 and a time of acquisition
(TA) = 13:43 can be reduced to TA = 6:37 (AF = 4), TA = 4:24 (AF = 6), and TA = 3:18
(AF = 8), with < 4% difference in the average coefficients of variation between reference
and accelerated sequences for all AFs. Top: whole image within field of view; bottom:
zoomed-in images.
Acceleration techniques using artificial intelligence (AI) algorithms are also on
the horizon, and these techniques may be the most promising of all. Two recent studies
demonstrated that deep learning acceleration can be used successfully for knee MRIs
with acceleration factors ≥ 4.[21]
[22] In both of these studies, the deep learning algorithms were trained on retrospectively
undersampled k-space from 2D sequences using different types of convolutional neural
networks. For AI acceleration techniques, although model training is an iterative
process that can be time intensive and computationally demanding, once the model is
fully trained, image reconstruction is fast and can be performed without the need
for special reconstruction hardware. Another advantage of AI acceleration is that
it may be possible to create highly accelerated images without the loss in image quality
seen with the other imaging techniques. In fact, the AI-accelerated images were actually
preferred over the standard images in one of these recent studies.[21] The main drawback of AI acceleration, as with other AI applications, is that a large
amount of training data are needed, and the methodology behind the algorithm is a
black box. To our knowledge, no 3D AI acceleration sequences are currently available
for clinical use. However, we have developed a combined T1ρ and T2 map sequence with
acquisition AI acceleration factors as high as 12, resulting in acquisition times
approaching 1 minute and with quantitative values comparable with those of a fully
sampled multiecho sequence ([Fig. 11]).
 Fig. 11 A deep learning algorithm can be used to accelerate a combined T1ρ and T2 three-dimensional
sequence without a clinically significant difference in accuracy. T1ρ (top) and T2
(bottom) maps with acceleration factors (AFs) of 4, 8, and 12 were obtained from retrospective
undersampling of the reference T1ρ and T2 maps (acquisition time = 13:43) from eight
fully sampled echoes. The deep network exploits both the spatial correlation among
pixels and the temporal correlation between the selected echoes while algorithmically
learning the complicated nonlinear relationship between the subsampled T1ρ/T2-weighted
images and the T1ρ/T2 maps. NMSE, normalized means squared error.
Fig. 11 A deep learning algorithm can be used to accelerate a combined T1ρ and T2 three-dimensional
sequence without a clinically significant difference in accuracy. T1ρ (top) and T2
(bottom) maps with acceleration factors (AFs) of 4, 8, and 12 were obtained from retrospective
undersampling of the reference T1ρ and T2 maps (acquisition time = 13:43) from eight
fully sampled echoes. The deep network exploits both the spatial correlation among
pixels and the temporal correlation between the selected echoes while algorithmically
learning the complicated nonlinear relationship between the subsampled T1ρ/T2-weighted
images and the T1ρ/T2 maps. NMSE, normalized means squared error.
Thus far, we have primarily focused on the advantages and limitations of 3D MRI techniques
for morphological imaging, but 3D MRI techniques are also an integral part of quantitative
MRI protocols, such as compositional cartilage imaging. Aside from the long acquisition
times required to obtain these compositional sequences, another barrier to the adoption
of these techniques into routine clinical practice is the postprocessing required
that is time consuming and traditionally was performed either entirely manually or
semi-manually. As a result, these sequences have been relegated almost entirely to
the research setting. Recent studies, however, showed that the postprocessing needed
for these compositional techniques can be fully automated using AI algorithms. One
of the most tedious postprocessing tasks often required for quantification of spatial
or pixel information is image segmentation, which is typically performed on isotropic
3D MRI sequences. Segmentation is a complex task, and commonly used automation methods
often still require substantial user input. However, recently developed segmentation
techniques using deep learning convolutional neural networks and generative adversarial
networks can segment knee articular cartilage and menisci in a fully automated fashion
with accuracy comparable with that seen with segmentation performed by humans ([Fig. 12]).[23]
[44]
 Fig. 12 Fully automatic segmentation of cartilage and meniscus using a deep learning generative
adversarial network (Unet-cGAN)-based model and three-dimensional gradient-recalled
echo double-echo steady-state images from the Osteoarthritis Initiative, with accuracy
comparable with that seen with manual segmentation.
Fig. 12 Fully automatic segmentation of cartilage and meniscus using a deep learning generative
adversarial network (Unet-cGAN)-based model and three-dimensional gradient-recalled
echo double-echo steady-state images from the Osteoarthritis Initiative, with accuracy
comparable with that seen with manual segmentation.
With these advances in postprocessing techniques and emerging acceleration techniques,
the ability to incorporate quantitative MRI techniques into routine clinical protocols
is now becoming feasible. As a consequence, the inclusion of 3D sequences as part
of a routine knee MRI protocol is only likely to increase, given that these compositional
techniques can directly use 3D acquisitions and are often paired with a morphological
3D sequence.
Conclusion
Three-dimensional sequences are being increasingly incorporated into knee MRI protocols
due to the availability of new sequences such as 3D FSE, advanced metal artifact reduction
techniques, and quantitative cartilage imaging with coincident advances in MRI acceleration
techniques, such as parallel imaging, compressed sensing, and deep learning. Although
3D sequences are still primarily being used in addition to 2D sequences for morphological
imaging, 3D sequences are increasingly replacing 2D sequences in certain applications,
such as MR neurography and metal artifact reduction imaging. Furthermore, reductions
in acquisition times of 3D compositional sequences, such as T1ρ and T2 maps with compressed
sensing and machine learning acceleration techniques, in addition to fully automated
segmentation algorithms, now make it feasible to incorporate these sequences clinically.
As further advances and refinements in knee MRI acceleration, automation, and quantification
techniques occur, 3D knee MRI will continue to become more accessible and valuable
to clinical practices.





