Subscribe to RSS
DOI: 10.1055/s-0041-1728737
Extended Anterolateral Approach and Rim Plate Fixation for Posterolateral Fragments in Tibial Plateau Fractures
Article in several languages: español | English
Abstract
Posterolateral fragments (PLFs) are commonly seen in tibial plateau fractures, but their reduction and fixation are challenging. There is no consensus about the ideal approach to fix this particular fragment. Even though an anterolateral approach is a safe option, it may impair a correct reduction. The posterolateral and posterior approaches offer direct visualization of the fragment, and enable a fixation with a biomechanical advantage; however, they are more demanding and expose the patient to a higher risk if morbidity. The following technical note describes the reduction and fixation of PLFs with a rim plate through an extended anterolateral approach using the paralateral collateral ligament space.
Introduction
The concept of column fixation in tibial plateau fractures was described by Luo et al.[1] 10 years ago. However, the decision to fixate posterior fragments through a posterior approach is still controversial.[2] According to the current AO Foundation/Orthopaedic Trauma Association (AO/OTA) classification modified by Kfuri and Schatzker,[3] the posterolateral fragment (PLF) is located at the lateral plateau, posterior to the tip of the fibula.[3] [4] Although FPLs are more frequent than previously thought (36% to 80%),[5] [6] [7] a malreduction rate between 50% and 70% has been described.[7]
There is no consensus on how to approach PLFs.[8] [9] Although the anterolateral approach is safe and widely known, it has proven to be insufficient for proper visualization, reduction and fixation of these fragments.[9] The posterolateral and posterior approaches provide direct visualization, enabling fixation with a biomechanical advantage,[10] [11] but they are technically demanding and expose the patient to increased morbidity.[12] Posterolateral and posterior approaches increase the risk of damage to the common peroneal nerve, the anterior tibial artery, and the sciatic-popliteal bundle.[13] [14] [15] This is especially true for posterior approaches which require operating the patient in prone position; if a fracture anterior to the midline of the plateau is found, the position of the patient needs to be changed during the procedure, increasing the surgical time and the risk of infection.[16]
The present is a technical note on PLF reduction and fixation with a rim plate using an extended anterolateral approach and the paralateral collateral ligament space.
Patient and Surgical Technique
Patient
A 75-year-old male patient with hypertension was run over on a public road and sustained a left tibial plateau fracture classified as AO/OTA 43C3.1 (t, u), that is, a multifragmentary fracture of the lateral tibial plateau with anterolateral and posterolateral traces ([Figure 1]). The physical examination revealed swelling of soft tissue and valgus alignment of the affected knee.

The patient was duly informed before and after surgery, and agreed to participate in the present research by signing an informed consent form.
Extended Anterolateral Approach
On a radiolucent operating table, the patient was placed in supine position, with the affected knee in 20° to 30° of flexion and a lift at the level of the ipsilateral gluteus. The following anatomical landmarks for the approach were indicated: the proximal tibial anterolateral (Gerdy) tubercle, the anterolateral rim of the tibia, the fibular head, the lateral joint line, the proximal tibial anterior tubercle, and the patellar tendon. A curvilinear incision was made from the Gerdy tubercle (GT) towards the lateral joint line, extending proximally and distally over the anterolateral rim of the tibia as required. Subcutaneous tissue elevation in a flap continued until exposing the iliotibial band (ITB) and its attachment into the GT. The femoral fascia and ITB were then incised distally up to the subperiosteal elevation of the tibialis anterior muscle. Although the original article[13] on this approach stated that the ITB should be incised in its midline, we recommend an individual evaluation according to the fracture pattern and the presence of more fragments. In this case, we decided to incise the fascia at its most anterior point (leaving a 3-mm to 5-mm remnant for posterior closure) for better exposure of the anterolateral fragment. With the anterolateral fragment exposed, a submeniscal arthrotomy was added, and the lateral meniscus next to the capsule was elevated with lace-like sutures, enabling the proper visualization of the articular surface and the meniscus. A controlled varus maneuver is recommended to increase visualization.
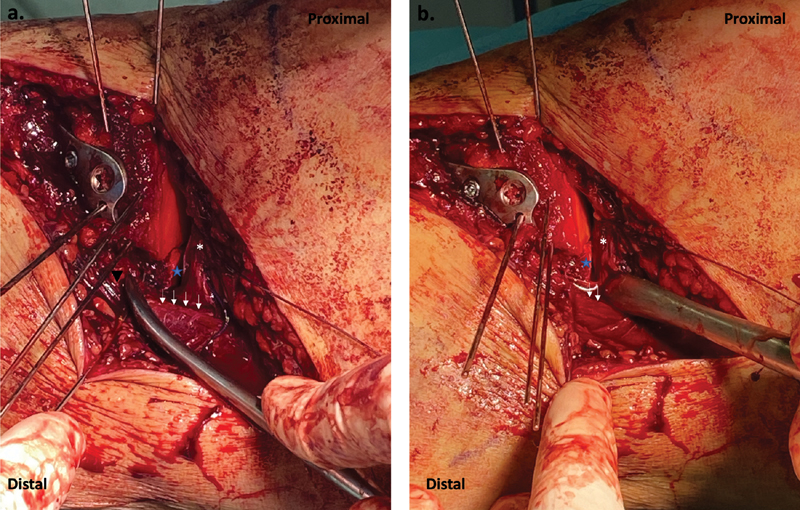
Next, we continued the extension towards the posterolateral portion of the tibia through the space called “parafibular collateral ligament space” by Cho et al.,[17] that is, the paralateral collateral space ([Figure 2]). The lateral collateral ligament (LCL) was identified with the knee flexed at 90° to relax the common peroneal nerve and the LCL.[17] Using a retractor at the paralateral collateral space, the LCL was retracted laterally, and then, the tissue of the bone capsule tissue of the lateral plateau rim was dissected to expose the PLF ([Figure 3A]). Finally, the extended approach enables the separation of the para-LCL space with a Hohmann retractor, and the fragment may be reduced in flexion or extension ([Figure 3B]).


Reduction Sequence and Use of the Rim Plate
In this case, the anterolateral line and diastasis were used to elevate those depressed fragments at the described central comminution and the PLF. Using Kirschner wires, the height of the fragments was maintained, and the anterolateral fracture was reduced. The reduction was complemented with anteroposterior wires to consolidate both fragments; next, it was stabilized with a proximal lateral tibial locked plate with variable angle (Peri-loc VLP, Smith & Nephew, Watford, England, UK), directing one of the screws towards the PLF. Since the FPL remained unstable, the anterolateral approach was extended through the para-LCL space for detailed visualization of the fragment, enabling proper reduction and stabilization with a rim plate. This was a 2.7-mm trefoil-shaped locked plate, with variable angle, from the mid/forefoot system (LCP®, DePuy Synthes, Raynham, MA, US).
The plate must be molded according to the anatomy of the patient ([Figure 4]). It is important to mold the plate hole after hole for correct shaping; in addition, it is advisable to ensure that the end is in contact with the bone. [Figure 5] shows the positioning of the rim plate through the extended anterolateral approach, leaving the trefoil-shaped segment posteriorly, and providing FPL fixation for further reduction. For the fixation of the rim plate, it is advisable to use a reduction forceps at the posterior segment of the plate, and begin by inserting a cortical screw at the first hole for proper apposition between plate and bone. As many screws as possible were inserted, ensuring an adequate direction to maintain the reduction and central comminutionof the PLF. Stabilization can be increased with anteroposterior screws. Fixation was finalized by placing the screws of the proximal tibial side plate ([Figures 6] and [7]).




Rehabilitation
The authors of the present study recommend a discharge protocol supporting the operated limb with canes or a walker for 6 to 8 weeks, followed by progressively increasing loads according to the degree of comminution of the fracture. Passive-active joint range exercises should start early to avoid stiffness, along with isometric quadriceps and hamstrings exercises. Then, according to the patient's symptoms, concentric exercises in closed chain are allowed, followed by open chain exercises when adequate neuromuscular control is resumed.
Discussion
Detection of FPLs in tibial plateau fractures is more frequent than previously thought. While Partenheimer et al.[18] described a rate of 7%, the current literature[5] [6] [7] reports a detection rate of up to 80%, with a malreduction rate ranging from 50% to 70%. These fragments are difficult to reduce mainly because of the obstruction by the fibular head and the components of the posterolateral corner.[19]
The anatomical reduction and stabilization of tibial plateau fractures has shown good long-term outcomes; FPL malreduction has been associated with knee instability during flexion.[17] [19] However, there is no consensus on how these FPLs should be managed.[8] [9] In fractures with joint separation (split fractures), support (buttress) plates are preferred to counteract the shear force of the axial load.[3] [11] [20] [21] Ideally, these plates should be placed parallel to the fracture and supported on the apex of the lesion.[3] [21] Several approaches have been described for fractures with a posterior apex to achieve satisfactory reduction and stabilization.[19] [21] [22] [23] In these cases, there is a tendency to prefer direct posterior approaches in prone position, especially when the joint fracture is at the coronal plane with a posterior apex. However, a fracture anterior to the midline of the plate would require repositioning the patient during the procedure, increasing the surgical time and the risk of infection.[16] Additionally, there is a risk of damaging neurovascular structures, such as the anterior tibial artery,[14] and the physiological consequences of keeping an anesthetized patient in prone position.
Therefore, in the presence of a non-shearing FPL, it is important to assess whether a direct posterior approach is really necessary. The present article illustrates a surgical approach that allows the patient to be operated in supine position and an optimal stabilization method for comminuted, depressed FPLs requiring fixation. Cho et al.[13] were the first to describe this approach and fixation method, and they stated the following advantages: 1) full exposure of the lateral and posterolateral portions of the lateral plate, allowing enough space to avoid a fibular head osteotomy; 2) patient positioned in supine recumbency; 3) fracture reduction and fixation under direct visualization; 4) the approach enables the simultaneous fixation of the anterolateral and posterolateral columns with plates; 5) simultaneous visualization of the FPL and the articular surface, which would not be possible with the direct posterior approach; 6) it can be performed by less experienced surgeons, reducing the potential limitation of the direct posterior approaches; 7) the removal of osteosynthesis material is simpler and less risky; and 8) it does not require the identification of the common peroneal nerve or posterolateral vascular structures. Moreover, the authors[13] also said that this is a safe option, with no reported ligament or neurovascular complications.
It is important to mention that the rim plate does not function as a buttress; therefore, we believe that this approach and reduction method would be insufficient for shear fractures at the coronal plane with the apex at the posterolateral region. [Box 1] describes tips and pitfalls of the surgical technique.
|
Tips |
Pitfalls |
|---|---|
|
1. When dissecting the paralateral collateral ligament (LCL) space, flex the knee at 90° to relax the LCL and the common peroneal nerve. 2. Fold the rim plate in stages (space after space), and make sure to bend the previous tip to avoid protrusions. 3. Place a pointed reduction forceps through the rim plate, ideally into one of the holes from the trefoil segment, to ensure its adhesion to the posterior cortex. |
1. Consider that all the posterolateral fragments of the tibial plateau can be successfully reduced from a standard anterolateral approach or using anteroposterior screws. 2. Extend the dissection of the para-LCL space proximal to the joint line. This may result in damage to the popliteal tendon, leading to iatrogenic instability. 3. Place the proximal lateral tibia (subchondral) plate too proximally, preventing the use of the rim plate. 4. Bending the rim plate with an unsuitable material risks deforming the holes and preventing the screws from locking. |
Conclusion
The extended anterolateral approach through the para-LCL space and fixation with a rim plate is an optimal surgical technique for the visualization, reduction, and fixation of comminuted FPLs and depressed joints requiring fixation.
Conflicto de intereses
Dr. F. Figueroa relata que es miembro editor de la Acta Ortopedica Mexicana. Los otros autores declaron no haber conflicto de intereses.
Acknowledgments
We would like to thank Karen Illesca, technician in nursing and surgical instrumentation, for being an essential part of the surgical team, and Arielle Ergas, for providing the illustration.
-
Referencias
- 1 Luo CF, Sun H, Zhang B, Zeng BF. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma 2010; 24 (11) 683-692
- 2 Rossmann M, Fensky F, Ozga AK. et al. Tibial plateau fracture: does fracture classification influence the choice of surgical approach? A retrospective multicenter analysis. Eur J Trauma Emerg Surg 2020; ;(0123456789): 1-7
- 3 Kfuri M, Schatzker J. Revisiting the Schatzker classification of tibial plateau fractures. Injury 2018; 49 (12) 2252-2263
- 4 Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and Dislocation Classification Compendium-2018. J Orthop Trauma 2018; 32 (9781461479864, Suppl 1) S1-S170
- 5 Zhai Q, Luo C, Zhu Y. et al. Morphological characteristics of split-depression fractures of the lateral tibial plateau (Schatzker type II): a computer-tomography-based study. Int Orthop 2013; 37 (05) 911-917
- 6 Adams Jr JD, Della Rocca GJ. Management of Posterior Articular Depression in Tibial Plateau Fractures. J Knee Surg 2016; 29 (01) 28-33
- 7 Meulenkamp B, Martin R, Desy NM. et al. Incidence, Risk Factors, and Location of Articular Malreductions of the Tibial Plateau. J Orthop Trauma 2017; 31 (03) 146-150
- 8 Warner BT, Moulton SG, Cram TR, LaPrade RF. Anatomic Reconstruction of the Proximal Tibiofibular Joint. Arthrosc Tech 2016; 5 (01) e207-e210
- 9 Yi Z, Hui S, Binbin Z. et al. A new strategy to fix posterolateral depression in tibial plateau fractures: Introduction of a new modified Frosch approach and a “Barrel hoop plate” technique. Injury 2020; 51 (03) 723-734
- 10 Solomon LB, Stevenson AW, Lee YC, Baird RPV, Howie DW. Posterolateral and anterolateral approaches to unicondylar posterolateral tibial plateau fractures: a comparative study. Injury 2013; 44 (11) 1561-1568
- 11 Zhang W, Luo CF, Putnis S, Sun H, Zeng ZM, Zeng BF. Biomechanical analysis of four different fixations for the posterolateral shearing tibial plateau fracture. Knee 2012; 19 (02) 94-98
- 12 Hangody L, Dobos J, Baló E, Pánics G, Hangody LR, Berkes I. Clinical experiences with autologous osteochondral mosaicplasty in an athletic population: a 17-year prospective multicenter study. Am J Sports Med 2010; 38 (06) 1125-1133
- 13 Cho JW, Samal P, Jeon YS, Oh CW, Oh JK. Rim Plating of Posterolateral Fracture Fragments (PLFs) Through a Modified Anterolateral Approach in Tibial Plateau Fractures. J Orthop Trauma 2016; 30 (11) e362-e368
- 14 Heidari N, Lidder S, Grechenig W, Tesch NP, Weinberg AM. The risk of injury to the anterior tibial artery in the posterolateral approach to the tibia plateau: a cadaver study. J Orthop Trauma 2013; 27 (04) 221-225
- 15 Chen WT, Zhang YQ, Chang SM. Posterolateral approach for plating of tibial plateau fractures and the risk of injury to the anterior tibial vessels. J Orthop Trauma 2013; 27 (09) e228-e229
- 16 Colman M, Wright A, Gruen G, Siska P, Pape HC, Tarkin I. Prolonged operative time increases infection rate in tibial plateau fractures. Injury 2013; 44 (02) 249-252
- 17 Cho JW, Kim J, Cho WT. et al. Approaches and fixation of the posterolateral fracture fragment in tibial plateau fractures: a review with an emphasis on rim plating via modified anterolateral approach. Int Orthop 2017; 41 (09) 1887-1897
- 18 Partenheimer A, Gösling T, Müller M. et al. [Management of bicondylar fractures of the tibial plateau with unilateral fixed-angle plate fixation]. Unfallchirurg 2007; 110 (08) 675-683
- 19 Frosch KH, Balcarek P, Walde T, Stürmer KM. A new posterolateral approach without fibula osteotomy for the treatment of tibial plateau fractures. J Orthop Trauma 2010; 24 (08) 515-520
- 20 Wang Y, Luo C, Zhu Y. et al. Updated Three-Column Concept in Surgical Treatment for Tibial Plateau Fractures - A Prospective Cohort Study of 287 Patients. Vol 47. Elsevier Ltd; 2016.
- 21 Kfuri M, Schatzker J, Castiglia MT, Giordano V, Fogagnolo F, Stannard JP. Extended Anterolateral Approach for Complex Lateral Tibial Plateau Fractures. J Knee Surg 2017; 30 (03) 204-211
- 22 Carlson DA. Posterior bicondylar tibial plateau fractures. J Orthop Trauma 2005; 19 (02) 73-78
- 23 Garner MR, Warner SJ, Lorich DG. Surgical Approaches to Posterolateral Tibial Plateau Fractures. J Knee Surg 2016; 29 (01) 12-20
Address for correspondence
Publication History
Received: 21 July 2020
Accepted: 21 January 2021
Article published online:
02 June 2021
© 2021. Sociedad Chilena de Ortopedia y Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referencias
- 1 Luo CF, Sun H, Zhang B, Zeng BF. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma 2010; 24 (11) 683-692
- 2 Rossmann M, Fensky F, Ozga AK. et al. Tibial plateau fracture: does fracture classification influence the choice of surgical approach? A retrospective multicenter analysis. Eur J Trauma Emerg Surg 2020; ;(0123456789): 1-7
- 3 Kfuri M, Schatzker J. Revisiting the Schatzker classification of tibial plateau fractures. Injury 2018; 49 (12) 2252-2263
- 4 Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and Dislocation Classification Compendium-2018. J Orthop Trauma 2018; 32 (9781461479864, Suppl 1) S1-S170
- 5 Zhai Q, Luo C, Zhu Y. et al. Morphological characteristics of split-depression fractures of the lateral tibial plateau (Schatzker type II): a computer-tomography-based study. Int Orthop 2013; 37 (05) 911-917
- 6 Adams Jr JD, Della Rocca GJ. Management of Posterior Articular Depression in Tibial Plateau Fractures. J Knee Surg 2016; 29 (01) 28-33
- 7 Meulenkamp B, Martin R, Desy NM. et al. Incidence, Risk Factors, and Location of Articular Malreductions of the Tibial Plateau. J Orthop Trauma 2017; 31 (03) 146-150
- 8 Warner BT, Moulton SG, Cram TR, LaPrade RF. Anatomic Reconstruction of the Proximal Tibiofibular Joint. Arthrosc Tech 2016; 5 (01) e207-e210
- 9 Yi Z, Hui S, Binbin Z. et al. A new strategy to fix posterolateral depression in tibial plateau fractures: Introduction of a new modified Frosch approach and a “Barrel hoop plate” technique. Injury 2020; 51 (03) 723-734
- 10 Solomon LB, Stevenson AW, Lee YC, Baird RPV, Howie DW. Posterolateral and anterolateral approaches to unicondylar posterolateral tibial plateau fractures: a comparative study. Injury 2013; 44 (11) 1561-1568
- 11 Zhang W, Luo CF, Putnis S, Sun H, Zeng ZM, Zeng BF. Biomechanical analysis of four different fixations for the posterolateral shearing tibial plateau fracture. Knee 2012; 19 (02) 94-98
- 12 Hangody L, Dobos J, Baló E, Pánics G, Hangody LR, Berkes I. Clinical experiences with autologous osteochondral mosaicplasty in an athletic population: a 17-year prospective multicenter study. Am J Sports Med 2010; 38 (06) 1125-1133
- 13 Cho JW, Samal P, Jeon YS, Oh CW, Oh JK. Rim Plating of Posterolateral Fracture Fragments (PLFs) Through a Modified Anterolateral Approach in Tibial Plateau Fractures. J Orthop Trauma 2016; 30 (11) e362-e368
- 14 Heidari N, Lidder S, Grechenig W, Tesch NP, Weinberg AM. The risk of injury to the anterior tibial artery in the posterolateral approach to the tibia plateau: a cadaver study. J Orthop Trauma 2013; 27 (04) 221-225
- 15 Chen WT, Zhang YQ, Chang SM. Posterolateral approach for plating of tibial plateau fractures and the risk of injury to the anterior tibial vessels. J Orthop Trauma 2013; 27 (09) e228-e229
- 16 Colman M, Wright A, Gruen G, Siska P, Pape HC, Tarkin I. Prolonged operative time increases infection rate in tibial plateau fractures. Injury 2013; 44 (02) 249-252
- 17 Cho JW, Kim J, Cho WT. et al. Approaches and fixation of the posterolateral fracture fragment in tibial plateau fractures: a review with an emphasis on rim plating via modified anterolateral approach. Int Orthop 2017; 41 (09) 1887-1897
- 18 Partenheimer A, Gösling T, Müller M. et al. [Management of bicondylar fractures of the tibial plateau with unilateral fixed-angle plate fixation]. Unfallchirurg 2007; 110 (08) 675-683
- 19 Frosch KH, Balcarek P, Walde T, Stürmer KM. A new posterolateral approach without fibula osteotomy for the treatment of tibial plateau fractures. J Orthop Trauma 2010; 24 (08) 515-520
- 20 Wang Y, Luo C, Zhu Y. et al. Updated Three-Column Concept in Surgical Treatment for Tibial Plateau Fractures - A Prospective Cohort Study of 287 Patients. Vol 47. Elsevier Ltd; 2016.
- 21 Kfuri M, Schatzker J, Castiglia MT, Giordano V, Fogagnolo F, Stannard JP. Extended Anterolateral Approach for Complex Lateral Tibial Plateau Fractures. J Knee Surg 2017; 30 (03) 204-211
- 22 Carlson DA. Posterior bicondylar tibial plateau fractures. J Orthop Trauma 2005; 19 (02) 73-78
- 23 Garner MR, Warner SJ, Lorich DG. Surgical Approaches to Posterolateral Tibial Plateau Fractures. J Knee Surg 2016; 29 (01) 12-20