Subscribe to RSS
DOI: 10.1055/s-0040-1721842
Open Fracture of the Femoral Neck in an Adult: Case Report and Surgical Solution[*]
Article in several languages: português | English
Abstract
Intracapsular proximal femoral fracture is a frequent injury in elderly patients, often associated with low-energy trauma and reduced bone mass. In young patient, it is uncommon, usually caused by high-energy trauma and accompanied by damage to the adjacent soft tissues. However, reports of open intracapsular proximal femoral fracture due to indirect trauma are rare in the orthopedic literature. In the present article, we describe a case of this injury in a 35-year-old man involved in a car accident. The proximal femur was exposed at the gluteal region due to a mechanism similar to dislocation of the posterior hip. We describe the initial treatment and subsequent management until achieving a definitive solution using total hip arthroplasty and muscle transfer to reconstruct the abductor mechanism of the hip. At 10 months of follow-up, the patient presented good functional outcome, with gradual recovery of the abductive strength and a Harris Hip Score of 91 points. In addition, a radiographic study showed that the cemented total prosthesis was well-positioned. This therapeutic strategy (total hip arthroplasty with muscle transfer to reconstruct the abductor musculature) was successful to treat an intracapsular proximal femoral fracture with bone exposure.
Introduction
Femoral neck fractures in patients younger than 50 years of age account for less than 5% of all hip fractures. These fractures result from high-energy trauma, and damage the soft tissues.[1] The pattern of the fracture pattern, the comminution in the focus of the fracture, and the degree of deviation of the fragments are associated with surgical complications, including lack of consolidation, osteosynthesis failure, and femoral head avascular necrosis.[2] When associated with a major trauma resulting in bone exposure and extensive injury to the soft tissue of the hip, this fracture becomes unique and difficult to solve.
Case Report
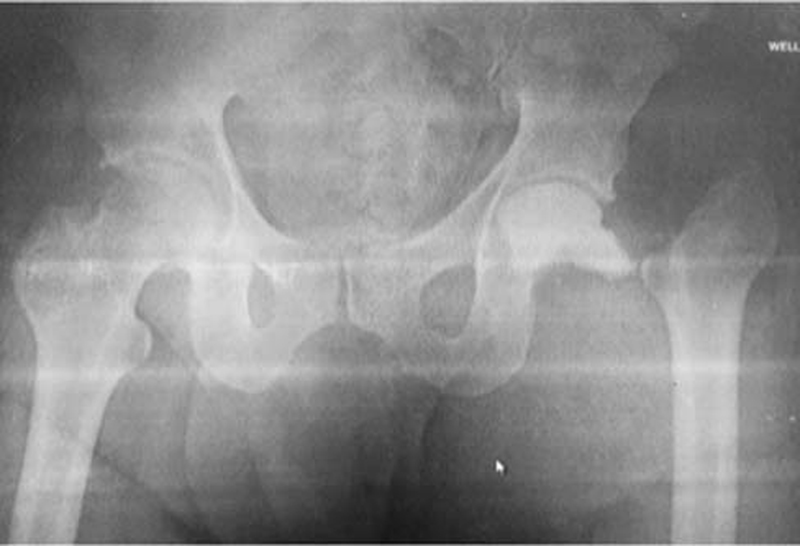
A Caucasian, single, 35-year-old male patient was involved in a car accident, and sustained typical trauma due to impact on the dashboard, resulting in a comminuted fracture at the left femoral neck with proximal migration of the diaphyseal segment, extensive injury at the gluteal musculature, and bone exposure. At the initial clinical evaluation, the patient was conscious, breathing normally, with no chest or abdominal complaints, and no signs of hemodynamic instability. Upon the physical examination, he reported severe hip pain and bleeding from a wound at the left gluteal region. The clinical examination also revealed pain and functional impairment at the ipsilateral knee, with joint instability suggesting a potential injury to the posterior cruciate ligament. A conventional radiographic study showed a comminuted, deviated fracture of the left femoral neck. Wound inspection revealed bone fragments, confirming it as an open femoral neck fracture ([Fig. 1]). At the operating room, the fracture was mechanically cleaned with a thorough wound rinse. The fracture was aligned under traction, and the wound was closed in planes. Antibiotic therapy with intravenous cefazolin and tetanus prophylaxis were started. Five days after the initial trauma, a new surgical procedure was performed through an anterolateral approach to determine the potential of direct reduction and osteosynthesis. The surgical finding was devastating, with a severe injury characterized by cephalic femoral devascularization and complete disinsertion of the iliopsoas, gluteus minimus, gluteus medius and external rotator muscles, as well as a circumferential capsulolabral lesion of the hip joint. We opted for a resection of the cephalic segment and placed a non-articulated bone cement spacer with antibiotics (vancomycin) to wait for the subsequent planning of a total hip arthroplasty ([Fig. 2]). Eight weeks later, with negative culture tests, normal erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels, the third procedure was performed. Through a posterolateral approach, the spacer was removed, and a cemented total hip arthroplasty was performed. Next, the maximum gluteus muscle was transferred to restore the hip abductor mechanism according to the technique described by Whiteside[3] in 2012 ([Fig. 3]). This technique is based on two gluteus maximus muscle flaps: the lower flap was sutured to the anterior capsule and the anterior border of the greater trochanter to emulate the function of the gluteus minimus, whereas the upper flap crossed the lower flap and was fixed at the lateral region of the greater trochanter to act as the gluteus medius ([Fig. 4]). The patient evolved uneventfully until discharge. Partial loading with support was allowed for 3 months, and physical therapy was instituted for functional recovery. The patient evolved well, with gradual recovery of the abductive strength and negative Trendelenburg signal. Ten months after surgery, he presented a Harris Hip Score of 91 points, and a conventional radiography showed that the cemented total prosthesis was well-positioned ([Fig. 5]).





Discussion
A query on the main available databases (Medline PubMed, LILACS, Scielo, Cochrane library) revealed no reports of a similar injury. There are some case reports of open anterior dislocation of the hip in adult patients,[4] [5] [6] and a single description of an open posterior dislocation in an adult who was run over on a public road.[7] Here, the trauma mechanism was knee impact on the car dashboard, which usually results only in posterior dislocation or fracture-dislocation of the hip through the posterior wall of the acetabulum, which is the most vulnerable. We believe that, at the time of trauma, the patient's hip was probably abducted, with the femoral head completely contained by the acetabular roof. Thus, the shear force vector caused the neck fracture, and the persistence of the impact energy resulted in upper migration of the proximal femur, with extensive soft tissue injury and bone exposure through the gluteal muscles. This mechanism is the same that causes femoral head fracture, which is often associated with posterior dislocation of the hip.[8] The ipsilateral knee ligament injury is also explained by this typical mechanism of knee trauma on a car dashboard during collision.
The blood supply to the femoral head is fragile and easily damaged by a deviated intracapsular fracture. The medial femoral circumflex artery supplies 82% of the femoral head and 67% of the femoral neck. The lateral femoral circumflex artery contributes to 18% and 33% respectively to the femoral head and neck vascularization. Both vessels branch off into delicate retinacular arteries spreading through the femoral neck surface up to the femoral head.[9] In our case, this vascular system was damaged due to disinsertion of the trochanteric musculature.
The therapeutic option consisting of reduction and osteosynthesis was ruled out due to the comminuted fracture focus and the risk of femoral head avascular necrosis. Thus, a total hip arthroplasty was indicated because of the biological risk of aseptic femoral head necrosis and the biomechanical risk related to the very high failure rate of an osteosynthesis at a fracture with a vertical line and posterior comminution of the femoral neck.[2] Another important aspect was the loss of the hip abductor musculature, resulting in a significant walk impairment and a potential predisposition to dislocation of the hip prosthesis. The Whiteside[3] technique enabled the stabilization of the prosthesis and minimized the walking deficit. Considering the favorable evolution of the patient, the muscle transfer described for revision of the hip prosthesis in case of loss of abductor musculature[10] was successful to treat this type of injury. Total hip arthroplasty associated with muscle transfer for the reconstruction of the abductor musculature was an efficient solution to treat open femoral neck fractures.
Conflito de Interesses
Os autores declaram não haver conflito de interesses.
* Work developed at the Teaching and Research Division of the National Institute of Traumatology and Orthopedics (INTO-RJ), Rio de Janeiro, RJ, Brazil.
Financial Support
The authors declare that they have received no financial support for the research, authorship and/or publication of the present article.
-
Referências
- 1 Robinson CM, Court-Brown CM, McQueen MM, Christie J. Hip fractures in adults younger than 50 years of age. Epidemiology and results. Clin Orthop Relat Res 1995; (312) 238-246
- 2 Liporace F, Gaines R, Collinge C, Haidukewych GJ. Results of internal fixation of Pauwels type-3 vertical femoral neck fractures. J Bone Joint Surg Am 2008; 90 (08) 1654-1659
- 3 Whiteside LA. Surgical technique: Transfer of the anterior portion of the gluteus maximus muscle for abductor deficiency of the hip. Clin Orthop Relat Res 2012; 470 (02) 503-510
- 4 Grundy M, Kumar N. Open anterior dislocation of the hip. Injury 1982; 13 (04) 315-316
- 5 Lamberti PM, Rabin SI. Open anterior-inferior hip dislocation. J Orthop Trauma 2003; 17 (01) 65-66
- 6 Oliveira AL, Machado EG. Luxação anterior exposta do quadril em adulto: relato de caso e revisão da literatura. Rev Bras Ortop 2014; 49 (01) 94-99
- 7 Hamzaoglu A, Aydinok HC, Pinar H, Asik M, Cakmak M. Open traumatic posterior dislocation of the hip. A case report. Arch Orthop Trauma Surg 1992; 111 (06) 345-347
- 8 Guimarães RP, Saeki de Souza G, da Silva Reginaldo S. et al. Study of the treatment of femoral head fractures. Rev Bras Ortop 2015; 45 (04) 355-361
- 9 Dewar DC, Lazaro LE, Klinger CE. et al. The relative contribution of the medial and lateral femoral circumflex arteries to the vascularity of the head and neck of the femur: a quantitative MRI-based assessment. Bone Joint J 2016; 98-B (12) 1582-1588
- 10 Jang SA, Cho YH, Byun YS, Gu TH. Abductor reconstruction with gluteus maximus transfer in primary abductor deficiency during total hip arthroplasty. Hip Pelvis 2016; 28 (03) 178-181
Endereço para correspondência
Publication History
Received: 08 May 2020
Accepted: 16 September 2020
Article published online:
22 March 2021
© 2021. Sociedade Brasileira de Ortopedia e Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Robinson CM, Court-Brown CM, McQueen MM, Christie J. Hip fractures in adults younger than 50 years of age. Epidemiology and results. Clin Orthop Relat Res 1995; (312) 238-246
- 2 Liporace F, Gaines R, Collinge C, Haidukewych GJ. Results of internal fixation of Pauwels type-3 vertical femoral neck fractures. J Bone Joint Surg Am 2008; 90 (08) 1654-1659
- 3 Whiteside LA. Surgical technique: Transfer of the anterior portion of the gluteus maximus muscle for abductor deficiency of the hip. Clin Orthop Relat Res 2012; 470 (02) 503-510
- 4 Grundy M, Kumar N. Open anterior dislocation of the hip. Injury 1982; 13 (04) 315-316
- 5 Lamberti PM, Rabin SI. Open anterior-inferior hip dislocation. J Orthop Trauma 2003; 17 (01) 65-66
- 6 Oliveira AL, Machado EG. Luxação anterior exposta do quadril em adulto: relato de caso e revisão da literatura. Rev Bras Ortop 2014; 49 (01) 94-99
- 7 Hamzaoglu A, Aydinok HC, Pinar H, Asik M, Cakmak M. Open traumatic posterior dislocation of the hip. A case report. Arch Orthop Trauma Surg 1992; 111 (06) 345-347
- 8 Guimarães RP, Saeki de Souza G, da Silva Reginaldo S. et al. Study of the treatment of femoral head fractures. Rev Bras Ortop 2015; 45 (04) 355-361
- 9 Dewar DC, Lazaro LE, Klinger CE. et al. The relative contribution of the medial and lateral femoral circumflex arteries to the vascularity of the head and neck of the femur: a quantitative MRI-based assessment. Bone Joint J 2016; 98-B (12) 1582-1588
- 10 Jang SA, Cho YH, Byun YS, Gu TH. Abductor reconstruction with gluteus maximus transfer in primary abductor deficiency during total hip arthroplasty. Hip Pelvis 2016; 28 (03) 178-181