

Subscribe to RSS
DOI: 10.1055/s-0040-1718989
Rare Clinical Onset of Nontraumatic Intracavernous Aneurysm of the Internal Carotid Artery: A Diagnostic and Therapeutic Challenge
Authors


Abstract
While the so-called pseudoaneurysms can result from arterial injury during trans-sphenoidal surgery or after a trauma, spontaneous aneurysms of cavernous–internal carotid artery (CICA) are rare. Symptoms vary and the differential diagnosis with other, more frequent, sellar lesions is difficult. We describe three cases of misdiagnosed CICA spontaneous aneurysm. In two cases the onset was with neuro-ophthalmological manifestations, classifiable as “cavernous sinus syndrome.” The emergency computed tomography scan did not show CICA aneurysm and the diagnosis was made by surgical exploration. The third patient came to our attention with a sudden severe unilateral epistaxis; endonasal surgery revealed also in this case a CICA aneurysm, eroding the wall and protruding into the sphenoidal sinus. When the onset was with a cavernous sinus syndrome, misdiagnosis exposed two patients to potential serious risk of bleeding, while the patient with epistaxis was treated with embolization, using coils and two balloons. Intracavernous nontraumatic aneurysms are both a diagnostic and therapeutic challenge, because of their heterogeneous onset and risk of rupture, potentially lethal. Intracavernous aneurysms can be managed with radiological follow-up, if asymptomatic or clinically stable, or can be surgically treated with endovascular or microsurgical techniques.
Introduction
The cavernous part of the internal carotid artery (ICA) is in the form of a siphon that is twisted and torqued in three dimensions.[1] It is the most medial structure within the cavernous sinus, so it leans directly against the lateral surface of the body of the sphenoid bone, where bone can be absent in 4% of cases or a very thin space (< 1 mm) can be seen in 66%.[2]
Prevalence of intracranial saccular aneurysms varies in the literature, from 0.4% to 6%, with a preponderance in female patients (92%).[3] They are most commonly localized in ICA (42%).[4] Nakagawa and Hashi found an incidence of 3.7% of cavernous–internal carotid artery (CICA) aneurysms among all asymptomatic, unruptured intracranial aneurysms in 400 volunteers.[5]
Symptoms of CICA include optic nerve compression with mild-to-severe visual changes, severe headaches, isolated third or sixth nerve palsy, cavernous sinus syndrome, and rarely epistaxis. Three cases referring different clinical onset are described.
Case Series
Case 1
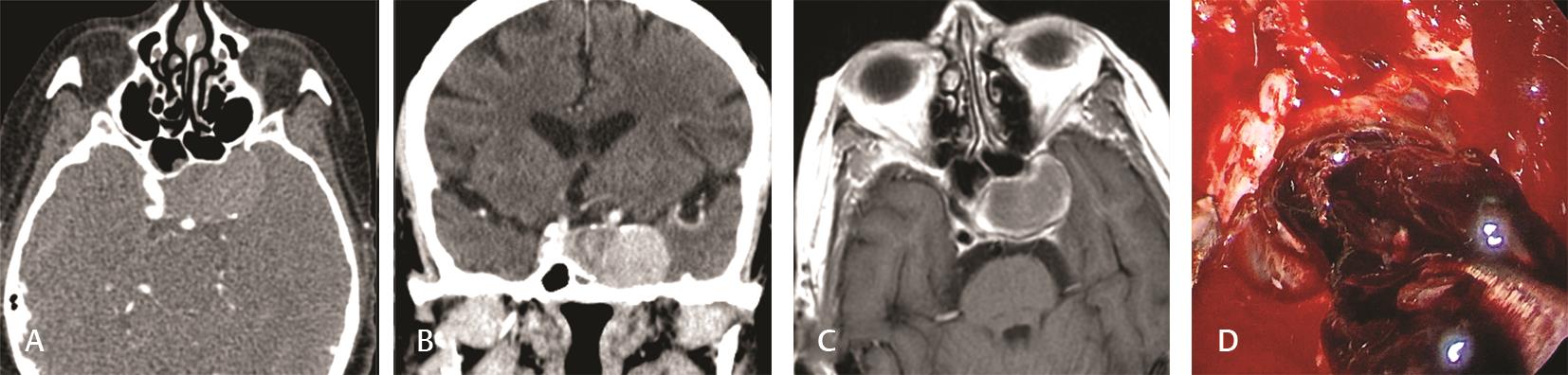
A 69-year-old female patient was admitted to the Department of Neurology for a progressive left pulsating frontotemporal and retro-orbital headache, associated to nausea, vomiting, and phonophobia for 1 week, and a sudden diplopia on left lateral gaze. An emergency head computed tomography (CT) showed a hyperdense voluminous intracavernous lesion (20 × 24 × 36 mm) extending to sella turcica and a CT angiography (CTA) evidenced an occlusion of the left carotid artery at the origin on the aortic arch ([Figs. 1A] [B]). The patient was obese and had a severe chronic obstructive pulmonary disease and arterial hypertension; some years before, she underwent breast quadrantectomy for fibrocystic mastopathy. A magnetic resonance angiography (MRA) described a sellar mass located in the left paramedian region without postcontrastographic enhancement and with no cleavage from the pituitary gland that was displaced; the bone of the sella appeared sclerotic ([Fig. 1C]). The pituitary function was normal. Following a discussion of the case, the patient was transferred to the Department of Otorhinolaryngology with the diagnosis of cavernous left sinus syndrome due to a sellar mass (strongly suggestive for parenchymal nature of the lesion, like a pituitary adenoma or a meningioma), and an extended endoscopic endonasal approach was planned, to access the lesion. After drilling out the anterior sellar wall, large intrasellar coated material was noted ([Fig. 1D]) and was sent to pathologist who confirmed its fibrous nature. The coated cavernous aneurysm was left untreated and the patient was discharged with deficit of third and sixth left cranial nerves. At 2 months of follow-up, the patient had stable neurological deficits, and CT scan demonstrated no complications after surgery.
Case 2
A 79-year-old female patient presented with gradual onset of intermittent diffuse headache of moderate-to-severe intensity for the past 2 months and right decreased visual acuity. The headache was generalized, not associated to vomiting, with exacerbation in retro-orbital region and irradiated to the area of distribution of ophthalmic and maxillary branches of the fifth cranial nerve.
The patient underwent ophthalmologic and neurologic evaluation; a CT scan and MRA were reported as normal by radiologist, concluding for trigeminal neuralgia. As she referred right blindness in the following days, she was admitted to the Department of Neurology, and, supposing first a right temporal arteritis and then an ischemic neuropathy, corticosteroid and anticoagulant therapies were prescribed, without results.
A mycotic sphenoidal sinusitis was suspected, based on a new facial CT scan ([Fig. 2A]) and a new MRA ([Fig. 2B]), even if both exams were again referred as negative by radiologist. In office videorhinoscopy, mixed mucous-bloody secretions originating by the right sphenoethmoidal recess were noted. An endonasal endoscopic surgery highlighted a dark red sphenoidal formation with a bloody pulsating mass ([Fig. 2C]) below it causing hemorrhage, which was interrupted by plugging with hemostatic material.

On suspicion of an aneurysm, an emergency head CTA was performed, showing a complete thrombosis of the right ICA. After evaluation with the neurosurgeon, it was decided that the patient did not need further therapy and she was discharged. After 2 months, the patient was readmitted to the Department of Neurology for confusion and right ptosis. Meningoencephalitis was diagnosed, but after 1 week she developed right hemisyndrome for a complete occlusion of the right ICA and after 2 days she died.
Case 3
A 41-year-old female patient presented to our institution with severe left epistaxis. She suffered from several episodes of epistaxis during the last months. She underwent an emergency endoscopic cauterization of the left sphenopalatine artery and sphenoidectomy under general anesthesia. During the surgery, left sphenoidal hemosinus was found. An emergency CTA revealed a 4 mm medial cavernous aneurysm on the left ICA, eroding the wall and protruding into the sphenoidal sinus ([Fig. 2D]). The balloon occlusion test showed good collateral flow through both the anterior and posterior communicating arteries; thus, embolization was performed using coils and two detachable Gold Balloons 2 deployed in the petrous left ICA. No new neurological deficit developed after this procedure, even if cerebral diffusion-weighted imaging MRA, performed 10 hours after embolization, showed small left semioval center infarction. The postprocedure treatment was with Aspirin/Enoxaparin combination for 1 month. At 6 years of follow-up, the patient has no neurological deficits and the MRA demonstrates stable outcome.
Discussion
The onset of two of the three cases described of CICA aneurysms was represented by neuro-ophthalmological manifestations, visual changes and pain, classifiable as the cavernous sinus syndrome, and mimicking pituitary apoplexy. The first case concerned progressive unilateral pulsating frontotemporal and retro-orbital headache and diplopia, due to vulnerable third, fourth, and sixth cranial nerves. The second case concerned a decreased unilateral visual acuity till blindness, caused by involvement of the optic nerves, and generalized headache with exacerbation in retro-orbital region and trigeminal neuralgia. In both cases the emergency imaging was not diriment. In the first patient, emergency CT scan demonstrated a sellar mass, better characterized, even if only partially, by the following MRA; indeed, the radiologist concluded for a difficult differential diagnosis between a pituitary tumor and a parasellar meningioma. In the second case, despite the radiological examination, nobody suspected sellar lesion, up to the evidence on the operatory room of a pulsating lateral sphenoidal formation. The definitive diagnosis was made for both patients during surgery and misdiagnosis exposed them to potential serious hemorrhagic risk.
Differential diagnosis of sellar masses is not straightforward because of the various potential etiologies, and because many of these lesions may mimic the clinical, endocrinologic, and radiographic presentations of pituitary adenomas that represent the most common sellar lesion.[6] In 9% of cases, the mass is within a broad spectrum of diagnosis, including, for example, cell rest tumors (craniopharyngioma), germ cell tumors, benign lesions (meningiomas), metastatic tumors, vascular lesions, and inflammatory processes. Confusion is due to the fact that the incidence of CICA aneurysms associated with pituitary adenoma is ~0.5 to 7% among pituitary adenoma patients[7] and in particular for growth hormone-secreting pituitary adenoma.[8] Another reason of confusion is that cases of “intra-adenoma,” embedded, aneurysm are described.[9]
MRA and CTA, used in combination, help to make differential diagnosis of sellar masses and provide the information for presurgical planning of cerebral aneurysms.[10] Because of the significant percentage of false positive on MRA and CTA, conventional digital subtraction angiography has a diagnostic role in small aneurysms detected on noninvasive imaging, while for large aneurysms its role is guiding surgical or endovascular treatment approaches.[11]
The third case presented to our institution with severe unilateral epistaxis. Diagnosis was made by surgeon because, during endoscopic cauterization, a hemosinus and clots in the sphenoidal sinus were found, confirmed by an emergency angiography. The bony structures were eroded and the small aneurysm (4 mm) extended into the sphenoid sinus, causing epistaxis, instead of subarachnoid hemorrhage. Lehmann et al reviewed the literature since 1956 and found 36 true CICA aneurysms that revealed with epistaxis. They represent a rare, but potentially fatal situation, with a mortality rate of 22.2%, which increases to 71.4% when not treated.[12]
Various management strategies have been proposed, but no consensus or guideline exists in the literature because of the rarity of the condition, so the treatment depends on clinical onset and on the severity of the situation. Ranabir and Baruah suggested that significant neuro-ophthalmic signs or reduced level of consciousness indicate the need for surgical therapy,[13] otherwise patients have to be monitored clinically and radiologically. Stiebel-Kalish et al gave indication to surgical treatment in cases of carotid cavernous fistula caused by the rupture of aneurysm, debilitating pain, visual loss from compression, or diplopia, or in patients with risk factors for major complications. Regarding cavernous aneurysm revealed by epistaxis, different types of strategies are used in the literature: no treatment, surgery, and endovascular treatment.
Endovascular technique includes balloon occlusion of the parent vessel, superficial temporal artery bypass to the middle cerebral artery followed by balloon occlusion, balloon occlusion with ICA preservation, Guglielmi detachable coils into the aneurysm, balloon in the parent vessel, and carotid stent. Patients can be treated surgically with trapping and clamping.
Intracavernous nontraumatic aneurysms are both a diagnostic and therapeutic challenge, because they are a rare but potentially lethal condition, when rupture occurs, and because their onset is various, from cavernous sinus syndrome to severe epistaxis. Differential diagnosis of a sellar mass needs a careful evaluation with MRA and CTA, even if angiography represents an efficient diagnostic and therapeutic technique at the same time. Rupture revealed by epistaxis and significant neuro-ophthalmologic signs or reduced level of consciousness represent an indication for treatment. Intracavernous aneurysms can be treated by both endovascular and microsurgical techniques.
Conflict of Interest
None declared.
-
References
- 1 Vijaywargiya M, Deopujari R, Athavale SA. Anatomical study of petrous and cavernous parts of internal carotid artery. Anat Cell Biol 2017; 50 (03) 163-170
- 2 Fujii K, Chambers SM, Rhoton AL Jr. Neurovascular relationships of the sphenoid sinus. A microsurgical study. J Neurosurg 1979; 50 (01) 31-39
- 3 Stiebel-Kalish H, Kalish Y, Bar-On RH. et al. Presentation, natural history, and management of carotid cavernous aneurysms. Neurosurgery 2005; 57 (05) 850-857
- 4 Rinkel GJE, Djibuti M, Algra A. van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke 1998; 29 (01) 251-256
- 5 Nakagawa T, Hashi K. The incidence and treatment of asymptomatic, unruptured cerebral aneurysms. J Neurosurg 1994; 80 (02) 217-223
- 6 Freda PU, Post KD. Differential diagnosis of sellar masses. Endocrinol Metab Clin North Am 1999; 28 (01) 81-117, vi
- 7 Pant B, Arita K, Kurisu K, Tominaga A, Eguchi K, Uozumi T. Incidence of intracranial aneurysm associated with pituitary adenoma. Neurosurg Rev 1997; 20 (01) 13-17
- 8 Curto L, Squadrito S, Almoto B. et al. MRI finding of simultaneous coexistence of growth hormone-secreting pituitary adenoma with intracranial meningioma and carotid artery aneurysms: report of a case. Pituitary 2007; 10 (03) 299-305
- 9 Suzuki M, Haginomori SI, Terada T. et al. Large intracavernous carotid artery aneurysm. Otol Neurotol 2017; 38 (06) e188-e189
- 10 Kouskouras C, Charitanti A, Giavroglou C. et al. Intracranial aneurysms: evaluation using CTA and MRA. Correlation with DSA and intraoperative findings. Neuroradiology 2004; 46 (10) 842-850
- 11 Rustemi O, Alaraj A, Shakur SF. et al. Detection of unruptured intracranial aneurysms on noninvasive imaging. Is there still a role for digital subtraction angiography?. Surg Neurol Int 2015; 6: 175
- 12 Lehmann P, Saliou G, Page C, Balut A, Le Gars D, Vallée JN. Epistaxis revealing the rupture of a carotid aneurysm of the cavernous sinus extending into the sphenoid: treatment using an uncovered stent and coils. Review of literature. Eur Arch Otorhinolaryngol 2009; 266 (05) 767-772
- 13 Ranabir S, Baruah MP. Pituitary apoplexy. Indian J Endocrinol Metab 2011; 15 (Suppl. 03) S188-S196
Address for correspondence
Publication History
Article published online:
19 December 2020
© 2020. Neurological Surgeons’ Society of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Vijaywargiya M, Deopujari R, Athavale SA. Anatomical study of petrous and cavernous parts of internal carotid artery. Anat Cell Biol 2017; 50 (03) 163-170
- 2 Fujii K, Chambers SM, Rhoton AL Jr. Neurovascular relationships of the sphenoid sinus. A microsurgical study. J Neurosurg 1979; 50 (01) 31-39
- 3 Stiebel-Kalish H, Kalish Y, Bar-On RH. et al. Presentation, natural history, and management of carotid cavernous aneurysms. Neurosurgery 2005; 57 (05) 850-857
- 4 Rinkel GJE, Djibuti M, Algra A. van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke 1998; 29 (01) 251-256
- 5 Nakagawa T, Hashi K. The incidence and treatment of asymptomatic, unruptured cerebral aneurysms. J Neurosurg 1994; 80 (02) 217-223
- 6 Freda PU, Post KD. Differential diagnosis of sellar masses. Endocrinol Metab Clin North Am 1999; 28 (01) 81-117, vi
- 7 Pant B, Arita K, Kurisu K, Tominaga A, Eguchi K, Uozumi T. Incidence of intracranial aneurysm associated with pituitary adenoma. Neurosurg Rev 1997; 20 (01) 13-17
- 8 Curto L, Squadrito S, Almoto B. et al. MRI finding of simultaneous coexistence of growth hormone-secreting pituitary adenoma with intracranial meningioma and carotid artery aneurysms: report of a case. Pituitary 2007; 10 (03) 299-305
- 9 Suzuki M, Haginomori SI, Terada T. et al. Large intracavernous carotid artery aneurysm. Otol Neurotol 2017; 38 (06) e188-e189
- 10 Kouskouras C, Charitanti A, Giavroglou C. et al. Intracranial aneurysms: evaluation using CTA and MRA. Correlation with DSA and intraoperative findings. Neuroradiology 2004; 46 (10) 842-850
- 11 Rustemi O, Alaraj A, Shakur SF. et al. Detection of unruptured intracranial aneurysms on noninvasive imaging. Is there still a role for digital subtraction angiography?. Surg Neurol Int 2015; 6: 175
- 12 Lehmann P, Saliou G, Page C, Balut A, Le Gars D, Vallée JN. Epistaxis revealing the rupture of a carotid aneurysm of the cavernous sinus extending into the sphenoid: treatment using an uncovered stent and coils. Review of literature. Eur Arch Otorhinolaryngol 2009; 266 (05) 767-772
- 13 Ranabir S, Baruah MP. Pituitary apoplexy. Indian J Endocrinol Metab 2011; 15 (Suppl. 03) S188-S196