
RSS-Feed abonnieren
DOI: 10.1055/s-0040-1716435
Possible Novel Treatment Modality for Non Ossifying Fibroma Neck of Femur
Source(s) of Support Nil


Abstract
Nonossifying fibromas (NOFs) are benign bone tumors occurring in the second decade of life. Most of the NOFs are diagnosed incidentally on the basis of its presentation on plain radiographs where they typically appear as small, cortical osteolytic lesions with sclerotic margin. They are mostly asymptomatic but can result in pathologic fractures if the lesion involves more than 50% of bone diameter. They are mostly treated with curettage and bone grafting. But in challenging situations where the classical surgery has failed or there is impending fracture of the neck of femur, bone structural support is needed. We are discussing two cases diagnosed as NOFs of intracapsular femoral neck. Both cases underwent curettage of tumor followed by free vascularized fibular graft. Results in both the cases were very gratifying, with complete resolution of symptoms during 1 year of follow-up.
Introduction
Nonossifying fibromas (NOFs) are benign bone tumors accounting for 2% of all primary bone tumors that mostly occur during the second decade of life with male predominance. They were first described by Jaffe and Lichtenstein in 1942. They are commonly located at distal femur, distal tibia, and proximal tibia. Etiologically, it is supposed to arise from bone marrow cell lineage or from the physis, thus making them more of a developmental bone defect.[1] They are mostly asymptomatic with spontaneous regression by 20 to 25 years but can result in pathologic fractures if the lesion involves more than 50% of bone diameter.[2] They are mostly diagnosed incidentally on plain radiographs, appearing as cortical osteolytic lesions with sclerotic margin.[3] The standard treatment is curettage and cancellous bone graft. In cases of impending fracture or fracture, bony fixation or even arthroplasty is required.[4]
Case report
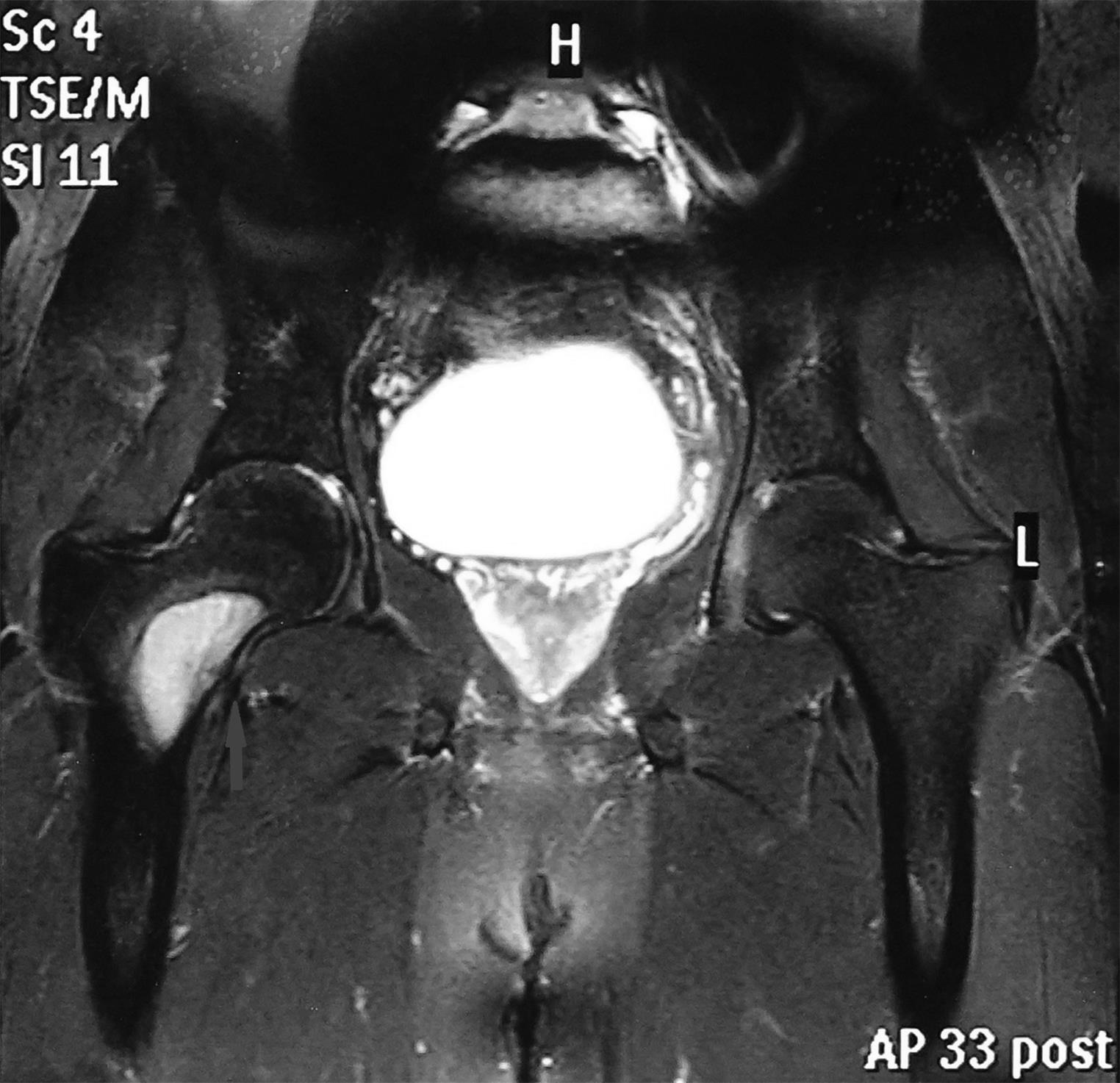
Case 1–A 35-year-old male presented with complaints of insidious, dull aching, and gradually increasing pain in the right hip, with difficulty in walking for past 6 months without history of trauma, fever, anorexia or weight loss. There was no swelling or deformity in the right hip. He had complete range of motion in the joint with pain. Tenderness was present on deep pressure over greater tronchanter. X-ray of the right hip showed osteolytic lesion with smooth sclerotic margins in the inferior part of right neck of femur, involving more than 50% of the neck diameter ([Fig. 1]). MRI showed eccentric osteolytic lesion at the medial aspect of neck of right femur, with breach in cortex coupled with sharp zone of transition and no periosteal reaction ([Fig. 2]). The patient underwent open biopsy with curettage of tumor. Histopathology confirmed diagnosis of NOF. Surgical options available were curettage with bone grafting, arthroplasty, or surgery with regenerative potential. Since the patient was an active young adult with impending pathological fracture, the last option was selected. The patient was managed with vascularized fibula, providing strong mechanical support and early healing of fracture due to its robust vascularity.

Watson incision was developed between tensor fascia lata and gluteus medius in lateral position. Transverse branch of lateral circumflex artery was followed proximally. Reaming of neck of femur was done up to 18 mm of diameter toward the greater trochanter and 14 mm for 3 cm toward the head of femur. Ipsilateral fibula was harvested simultaneously. Fibula sliver was removed from one side to make the contour more circular ([Fig. 3]). A total of 7.5 cm free fibula was placed into the cored-out neck of femur as snug fit without using any K wire, as shown in intraoperative C arm image PA view ([Fig. 4]). Microvascular anastomosis was done between peroneal artery and lateral circumflex artery and associated venae comitantes, as shown in figure with schematic diagram of the surgery ([Fig. 5]). The postoperative period was uneventful. Weight-bearing was prohibited for 1 month and full-weight bearing allowed after 3 months. Patient was asymptomatic during 1 year of follow-up.



Case 2–A 16-year-old male was an old diagnosed case of NOF of left neck of femur, who presented with complaints of pain in the left hip on walking and difficulty in weight-bearing since 30 months He had undergone multiple surgeries including curettage, followed by autogenous corticocancellous bone grafting done 2 years back. Six months after that surgery, the patient became symptomatic and was found to have a fractured neck of femur which was fixed with hip plate. The patient still had instability in the hip joint, with pain on motion and difficulty in bearing weight. X-ray of the hip 6 months after the second surgery showed a nonunited, fractured neck of left femur ([Fig. 6]). The patient underwent vascularized free fibula transfer to left neck of femur in a similar manner with good recovery. Complete weight-bearing was allowed after 3 months ([Fig. 7]). PET-CT scan performed 4 months postoperatively showed viable graft in the left neck of femur with FDG avidity likely due to reparative phase ([Fig. 8]). Patient remained asymptomatic during follow-up.



Discussion
NOF predominantly occurs in the lower extremities, especially around the knee. Only very few cases of NOFs located in femoral neck have been reported, which were treated with curettage and nonvascularized bone grafting.[5] We are discussing two difficult cases of NOF of intracapsular femoral neck treated with vascularized free fibula graft, which proved to be successful treatment modality under these conditions.
Most patients are asymptomatic, presenting as incidental radiological finding of lucent lesion, with the margins ranging from being densely sclerotic or scalloped to being hazy and indistinct. The cortex may be thinned, and in some cases, it is expanded.[6] Rarely, it may result in pathologic fractures. Surgical intervention is considered when the lesion leads to pathological fracture or there is potential risk for the same.[4] Arata et al described that a lesion involving more than 50% of the transverse diameter or measuring 33 mm carries the risk of pathologic fracture.[2]
Both our patients were symptomatic. One patient had pathological fracture with nonunion even after two surgeries.
For this challenging situation with paucity of options, patients were planned for vascularized fibular graft. This not only provides mechanical cortical support but also has regenerative potential.
A fibular graft is a preferred source of vascularized bone, as it provides suitable length and cortical support.[7] Osteocytes and osteoblasts within the graft remain viable. The rich vascularity and biological potential of this graft allows callus formation from the deliberately exposed cortex and the periosteal cambial layer of the cephalad end of the graft to the cancellous bone and the remaining subchondral bone.[8]
In both these cases, the results were very gratifying with complete recovery in 1 year of follow-up.
Conclusion
Although wide curettage and bone grafting provide excellent results in symptomatic NOFS, vascularized fibular graft is the new possible modality for treatment in more challenging situations, as it has regenerative potential and provides better mechanical stability.
Conflicts of Interest
None declared.
-
References
- 1 Goldin A, Muzykewicz DA, Dwek J, Mubarak SJ. The aetiology of the non-ossifying fibroma of the distal femur and its relationship to the surrounding soft tissues. J Child Orthop 2017; 11 (05) 373-379
- 2 Arata MA, Peterson HA, Dahlin DC. Pathological fractures through non-ossifying fibromas. review of the Mayo Clinic experience. J Bone Joint Surg Am 1981; 63 (06) 980-988
- 3 Ritschl P, Karnel F, Hajek P. Fibrous metaphyseal defects–determination of their origin and natural history using a radiomorphological study. Skeletal Radiol 1988; 17 (01) 8-15
- 4 Betsy M, Kupersmith LM, Springfield DS. Metaphyseal fibrous defects. J Am Acad Orthop Surg 2004; 12 (02) 89-95
- 5 Havitçioğlu H, Biçen Ç, Hapa O, Balcı A. Treatment of intracapsular femoral neck lesions: aggressive or conservative surgery?. Musculoskelet Surg 2014; 98 (03) 251-254
- 6 Kumar R, Madewell JE, Lindell MM, Swischuk LE. Fibrous lesions of bones. Radiographics 1990; 10 (02) 237-256
- 7 Gilbert A. Free vascularized bone grafts. Int Surg 1981; 66 (01) 27-31
- 8 Korompilias AV, Lykissas MG, Beris AE, Urbaniak JR, Soucacos PN. Vascularised fibular graft in the management of femoral head osteonecrosis: twenty years later. J Bone Joint Surg Br 2009; 91 (03) 287-293
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
07. September 2020
© 2020. Association of Plastic Surgeons of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Goldin A, Muzykewicz DA, Dwek J, Mubarak SJ. The aetiology of the non-ossifying fibroma of the distal femur and its relationship to the surrounding soft tissues. J Child Orthop 2017; 11 (05) 373-379
- 2 Arata MA, Peterson HA, Dahlin DC. Pathological fractures through non-ossifying fibromas. review of the Mayo Clinic experience. J Bone Joint Surg Am 1981; 63 (06) 980-988
- 3 Ritschl P, Karnel F, Hajek P. Fibrous metaphyseal defects–determination of their origin and natural history using a radiomorphological study. Skeletal Radiol 1988; 17 (01) 8-15
- 4 Betsy M, Kupersmith LM, Springfield DS. Metaphyseal fibrous defects. J Am Acad Orthop Surg 2004; 12 (02) 89-95
- 5 Havitçioğlu H, Biçen Ç, Hapa O, Balcı A. Treatment of intracapsular femoral neck lesions: aggressive or conservative surgery?. Musculoskelet Surg 2014; 98 (03) 251-254
- 6 Kumar R, Madewell JE, Lindell MM, Swischuk LE. Fibrous lesions of bones. Radiographics 1990; 10 (02) 237-256
- 7 Gilbert A. Free vascularized bone grafts. Int Surg 1981; 66 (01) 27-31
- 8 Korompilias AV, Lykissas MG, Beris AE, Urbaniak JR, Soucacos PN. Vascularised fibular graft in the management of femoral head osteonecrosis: twenty years later. J Bone Joint Surg Br 2009; 91 (03) 287-293