
RSS-Feed abonnieren
DOI: 10.1055/s-0040-1716429
A Review of Minimally Invasive Techniques in Thoracolumbar Trauma
- Abstract
- Introduction
- Decision Making in Choosing an Appropriate Operative Corridor
- Anterior Thoracic and Lumbar MIS Techniques
- Lateral Thoracic and Lumbar MIS Techniques
- Posterior Thoracic and Lumbar MIS Techniques
- Limitations of MIS Techniques
- Conclusions
- References
Abstract
The development of endoscopy, microscopy, and image guidance system provided the impetus for the adoption of minimally invasive surgery (MIS) techniques in the management of spinal trauma patients. The underlying drive has been an attempt to achieve the functional and biomechanical goals inherent to trauma care but through MIS techniques. Broadly the MIS techniques for spinal trauma can be divided into two categories—fusion and nonfusion methods. Fusion methods include mini-open or keyhole approaches that allow for discectomy and/or corpectomy and cage reconstruction via an anterior/lateral/posterior operative corridor. The nonfusion methods primarily include percutaneous pedicle screw fixation, kyphoplasty, and vertebroplasty, all without placement of bone graft or other attempts at inducing arthrodesis. In this review article, we have stratified the MIS techniques based on the operative corridor used and briefly described the decision-making process, technical nuances, pros, and cons of each technique.
#
Keywords
minimally invasive surgery - spinal trauma - surgical technique - operative corridor - decision-makingIntroduction
The annual incidence rate of thoracolumbar (TL) fractures is 30–40/100,000 and the majority (70%) of these fractures occurs at TL junction between T-10 and L-2 spinal levels.[1] [2] [3] [4] [5] [6] The transition of the mobile lumbar spine to stiff thoracic spine makes the TL junction more vulnerable during traumatic injuries. The basic principles of surgical management of spinal trauma include reduction, decompression, anterior-column reinforcement, reconstruction of posterior tension band, and bony fusion.[1] [2] [3] [4] [5] [6] Minimally invasive approaches do not change the underlying procedure. Instead, they offer an alternative surgical approach to the spine, with reduced trauma to soft tissues during the exposure process. The development of endoscopy, microscopy, and image guidance tools provided the impetus for the adoption of minimally invasive surgery (MIS) techniques in the management of spinal trauma patients. From a historical perspective, MIS techniques have been explored for decades, but only in the last several years have they gained serious attention.[7] The underlying drive has been an attempt to achieve the functional and biomechanical goals inherent to trauma care but through MIS techniques. These include both the general trauma care principles of early mobilization and pulmonary toilet, along with spine trauma principles of rigid stabilization, neural decompression, and anatomic bone alignment.[7]
Although many of the MIS approaches are intriguing because of their proposed benefits over traditional open approaches, their applicability in trauma surgery needs to be explored further. The potential advantages of the described minimal access approaches are a decrease in soft tissue damage during exposure of the spine, which theoretically results in decreased patient morbidity, reduced hospital stay, and thereby reduction in costs to health care system.[3] [4] [8] Also, patients with significant TL fractures often have other injuries and comorbidities. By limiting our surgical insult, these patients can be mobilized and potential pulmonary, thrombotic, and wound complications can be minimized.[3] [4] [8] Although the described procedures have a known learning curve and their own set of intraoperative and perioperative complications and risks, there are several series documenting safe and effective utilization of these approaches and each of the approaches can be converted to traditional open exposures, if necessary.
#
Decision Making in Choosing an Appropriate Operative Corridor
Recent studies have demonstrated no definite advantage of anterior over posterior approaches and vice versa.[2] [3] [4] [5] [6] [8] Traditional posterior open approaches require extensive dissection of paravertebral muscles, which leads to iatrogenic muscle denervation, elevated intramuscular pressure, consequent ischemia, infection, and increased operative site pain.[2] [3] [4] [5] [6] [8] Contrarily, anterior open approaches avoid these limitations, but may be contraindicated in morbidly obese patients with the bronchopulmonary disease. Besides anterior approaches pose a higher risk of iatrogenic respiratory, vascular and visceral complications.[2] [3] [4] [5] [6] [8] Therefore, there has been a paradigm shift toward the use of MIS techniques in the recent past. Although no strict guidelines exist so far, the choice of whether to approach the spine anteriorly in the face of significant trauma should be made based on known criteria and classification systems. The treatment planning and execution need to be tailored according to individual patient’s clinical and radiological findings, presence/absence of polytrauma, survival likelihood of the patient, and surgeon’s preference and expertise.[2] [3] [4] [5] [6] [8] [9]
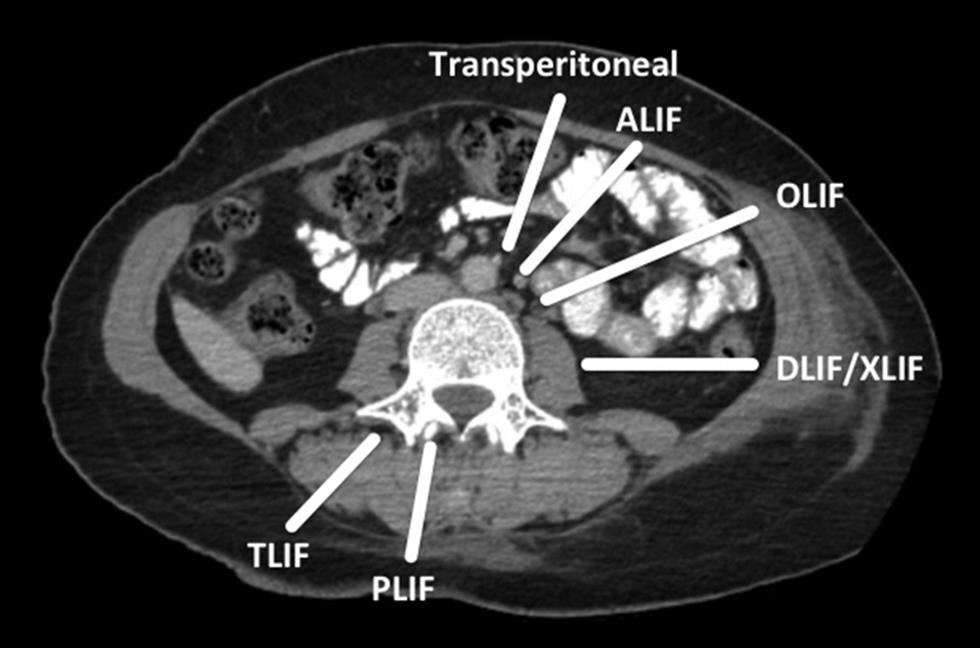
Broadly the MIS techniques for spinal trauma can be divided into two categories—fusion and nonfusion methods.[2] [3] [4] [5] [6] [8] [9] Fusion methods include mini-open or keyhole approaches that allow for discectomy and/or corpectomy and cage reconstruction via an anterior/lateral/posterior operative corridor ([Figs. 1] [2]). The nonfusion method primarily includes percutaneous pedicle screw fixation (PSF), kyphoplasty, and vertebroplasty, all without placement of bone graft or other attempts at inducing arthrodesis. Nonfusion techniques are essentially reserved for neurologically intact patients with certain specific types of TL fracture (type A3 AO spine with an intact posterior tension band—e.g., osteoporotic fractures) to restore vertebral height, stabilize the spine, or reduce fracture-associated pain.[2] [3] [4] [5] [6] [8] [9] Despite being a nonfusion method when used as a stand-alone procedure, percutaneous PSF has been shown to induce fusion in patients with diffuse idiopathic skeletal hyperostosis and ankylosing spondylitis, because of their inherent tendency to ossify. In this review article, we have stratified the MIS techniques based on the operative corridor used and briefly described the technical nuances, pros, and cons of each technique ([Tables 1] [2]).

#
Anterior Thoracic and Lumbar MIS Techniques
Several different MIS techniques have been described to access the spine using the anterior operative corridor, including endoscopic-assisted transthoracic access to the thoracic spine and TL junction using transdiaphragmatic approaches, extrapleural retroperitoneal approach to T10-L3 spine, laparoscopic-assisted transperitoneal approaches to lower lumbar segments including L4 and L5, endoscopic-assisted retroperitoneal approaches to lumbar segments L1-L5, and mini-open retroperitoneal approaches to the lumbar spine.[1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] [17]
Transthoracic (Thoracoscopic) Approach
Video-assisted thoracoscopic surgery (VATS) reduces the incidence of postoperative pulmonary morbidity, post-thoracotomy pain syndrome, intercostal neuralgia, and shoulder girdle dysfunction as compared with conventional thoracotomy.[1] [3] [9] This endoscopically assisted transthoracic transdiaphragmatic approach to the TL junction is performed by placing the patient in the lateral decubitus position and the approach is usually done on the patient’s left side. For higher thoracic levels, approach from the right side can also be done, based on vascular anatomy and surgeon’s preference. A working portal is placed directly cephalad to the fractured vertebrae and a separate portal for the endoscope is placed directly over the spine just cranial to the working portal. Additional portals for a retractor and suction can be used ventrally.
The primary limitations of VATS compared with posterior MIS approaches are the high incidence of pulmonary complications (14.1–29.4%), steep learning curve associated, requirement of special instrumentation, two separate sets of incisions (anterior and posterior) required in cases where a three column support is mandatory, and the fact that trajectory of decompression in anterior approach is toward the neural elements.[1] [3] [9] Besides, VATS can only access anterior and anterolateral aspects of the vertebrae and spinal canal. It cannot adequately expose the contralateral pedicle, posterior elements, and transverse processes.[1] [3] [9]
#
Extrapleural Retroperitoneal (Retropleural) Approach
Anterior minimally invasive extrapleural retroperitoneal (AMIER) approach can be used to access T10-L3 spinal levels.[15] Spinal angiography is a prerequisite in identifying the origin of the anterior spinal artery (vertebral level and side). The presence of the liver on the right side makes extrapleural retroperitoneal dissection more difficult; therefore, in the majority of cases, the AMIER approach is performed through the left side in the right lateral decubitus position. Subperiosteal dissection of musculature and investing endothoracic fascia (EF) over ribs is performed to avoid any injury to underlying structures such as intercostal neurovascular bundle, thoracic sympathetic chain, thoracic duct, and azygous vein, which stays in this EF, in contact with chest wall and vertebral body.[15] The contiguity of the EF, diaphragmatic lower costal origin, and the fascia transversalis allows exposure of the upper lumbar vertebral segments without entering into thoracic and abdominal cavity.[15]
The primary advantage of this technique is the avoidance of entering either of thoracic or abdominal cavities (extra-coelomic working corridor).[15] Therefore, the associated risks of ventilatory function impairment, atelectasis, and reflex ileus are significantly reduced as compared with transthoracic and transabdominal approaches. Another advantage of AMIER approach is low risk of iatrogenic large vessel injury due to its unique corridor of exposure, which displaces the vessels while being connected to retroperitoneum. However, AMIER technique is more technically challenging than its congeners, and is associated with the higher risk of lumbar plexus injury, risk to the segmental arteries, and can lead to inadequate canal decompression from this working angle.[15]
#
Transabdominal (Transperitoneal) Approach
Traditionally, video-assisted laparoscopic techniques have been used in approaching the L5-S1 level between the bifurcations of the great vessels; but laparoscopic, transperitoneal approaches to L4–5 have been fraught with problems.[2] [3] [8] [9] The incidence of vascular injury has been substantial because it requires ligation of the iliolumbar vein along with mobilization of the great vessels. In studies comparing laparoscopic versus mini-open anterior lumbar interbody fusion (ALIF) approaches and laparoscopic fusions at a variety of levels from L2-S1, there have been higher number of reported complications pertaining to deep vein thrombosis, abdominal visceral injury, damage to sympathetic plexus, ureter injury, retrograde ejaculation, great vessel injury, and postoperative intra-abdominal adhesions with the transperitoneal approach.[2] [3] [4] [8] [9] These complications inherent to the transperitoneal endoscopic approach led to the development of minimally invasive endoscopic, retroperitoneal, and mini-ALIF approaches to the lumbar spine.[2] [3] [4] [8] [9]
#
Retroperitoneal Approach
Endoscopic retroperitoneal approaches do not require CO2 insufflation, entrance into the peritoneum, or anterior dissection near the great vessels, thereby providing a safer exposure for spinal surgery. However, in some patients, inadequate surgical exposure may allow for placement of only one interbody device. Therefore, nowadays, the preference has shifted from keyhole endoscopic retroperitoneal approach to a rather mini-open procedure like mini-ALIF. The mini-ALIF procedure incorporates muscle-sparing techniques to reduce morbidity, operative time, and safer mobilization of the vascular structures.[2] [4] [8] [9] In this approach, the rectus fascia is exposed and incised transversely medially to the confluence of the rectus fascia. The preperitoneal space is entered bluntly, allowing exposure of the retroperitoneal space. The lumbar spine and the iliac vessels are then easily identified. If L5-S1 is involved, one can work below the bifurcation. If L4–5 or above is involved, the vessels will need to be mobilized and retracted medially. One to two lumbar levels can easily be exposed using this technique, making corpectomy feasible and safe.
#
#
Lateral Thoracic and Lumbar MIS Techniques
Lateral Extracavitary Approach
Minimally invasive lateral extracavitary approach provides an oblique posterolateral operative corridor to access the anterior aspect of the thoracic spine, without going through the pleural cavity or requirement of retropleural dissection.[2] [3] [8] [9] [10] This procedure can be performed in either prone or three-fourth prone position. A muscle splitting technique is employed and tubular retractor system over Kirschner wire is docked at the junction of the ipsilateral transverse process and pedicle. Subsequently the proximal rib is removed, followed by removal of costovertebral ligaments, rib head, intercostal vessels, and ipsilateral pedicle in a sequential manner. Discectomy and corpectomy are then performed with the preservation of anterior longitudinal ligament and ventral aspect of vertebral body. The primary advantage of this technique over midline posterior approaches is the preservation of posterior tension band. Nevertheless, the learning curve and patient morbidities may limit general applicability.[2] [3] [8] [9] [10]
#
Psoas Splitting Retroperitoneal Approach—Direct/Extreme Lateral Interbody Fusion
The natural progression from anterior transperitoneal and retroperitoneal minimally invasive approaches is a lateral psoas splitting approach to the anterior spine, as in the direct lateral interbody fusion (DLIF) or extreme lateral interbody fusion (XLIF) technique.[2] [3] [8] [9] [10] [12] [16] This approach, which utilizes muscle sparing at every level, has the advantage of negating retraction and dissection of the muscles of the abdominal wall. The disadvantage is that the roots of the lumbosacral plexus are at risk during blunt dissection through the muscle itself. Therefore, neuromonitoring is a mandatory component of this approach. Patients are placed in a lateral decubitus position, and the table is slightly flexed to open space between ribcage and iliac crest. A 5-cm oblique incision is fashioned directly over the disc space in line with external oblique muscle fibers. It is followed by blunt dissection through abdominal muscle layers until the retroperitoneal space is entered. The disc space is accessed through strict blunt dissection through the psoas muscle.[2] [3] [8] [9] [10] Care is used not to deviate too far anteriorly to avoid injury to major blood vessels and sympathetic chain. Also, any excessive posterior deviation may pose danger to exiting nerve roots.
Although this approach has several advantages, one significant disadvantage is the inability to access L5-S1 without creating an osteotomy through the iliac crest.[2] [3] [8] [9] [10] Biomechanical studies have shown equivalency between XLIF and anterior approaches to the lumbar spine.[2] [3] [8] [9] [10] The anterior longitudinal ligament and posterior longitudinal ligament are not violated, which afford a significant biomechanical advantage. Also, during the preparation of the disc space, any violation of the space itself with curettes, a high-speed burr, or another instrument would enter the contralateral psoas muscle rather than the spinal canal. Staying within the anterior third of psoas muscle is paramount to avoid nerve root damage, and this approach should only be attempted with appropriate neurophysiological surveillance. Complications unique to XLIF/DLIF procedure include neural injuries to lumbar plexus, psoas weakness, and thigh numbness.[2] [3] [8] [9] [10] [12] [16]
#
Nonpsoas Splitting Retroperitoneal Approach—Oblique Lateral Interbody Fusion (OLIF)
To circumvent the high complication rates of psoas splitting DLIF/XLIF approach, a nonpsoas splitting antero-oblique approach (OLIF) was innovated and conceptualized via nascent operative corridor between psoas muscle and major vessels.[13] [14] This technique provides an indirect neural decompression by distracting intervertebral disc space, and restores coronal and sagittal spine balance. Patient positioning is similar to XLIF approach; however, proceeding through left side is preferable due to easier dissection with aorta in comparison to inferior vena cava. Preoperative assessment of operative window between aorta and psoas muscle is mandatory to visualize and estimate the feasibility of OLIF procedure. In a comparative study between MIS-DLIF and MIS-OLIF, Jin et al[13] demonstrated significantly lower approach related complications in OLIF group compared with DLIF group by minimizing the risk of psoas muscle handling and iatrogenic lumbar plexus damage. They also concluded that in OLIF group, cage could be placed more posteriorly using orthogonal maneuver, thereby resulting in far superior foraminal and disc height restoration, when compared with DLIF group.
#
#
Posterior Thoracic and Lumbar MIS Techniques
Posterior approaches to the thoracic and lumbar spine after trauma are arguably the workhorse approaches.[2] [3] [5] [6] [8] [9] The ability to achieve spinal stabilization, restoration of spinal curvature, and fusion using a variety of instrumentation systems makes these approaches the most widely utilized.[2] [3] [5] [6] [8] [9] The posterior approaches are further classified into fusion and nonfusion methods.
Fusion Procedures
Minimally Invasive Posterior Transpedicular Corpectomy and Fusion of Thoracic Spine
A posterior keyhole corpectomy with percutaneous pedicle screw stabilization can be used in the surgical management of lumbar burst fractures. Indications for this technique includes AO spine subtype A.3.1 burst fractures. In patients where their comorbidities limit the use of minimally invasive transthoracic and lateral extracavitary approaches, a minimally invasive transpedicular approach has been extensively utilized. This procedure is performed in the prone position and a small 3 cm paramedian incision is given directly above the transverse process of clinically more symptomatic side. Sequential dilators and an expandable tubular retractor are then used to remove the ipsilateral transverse process, proximal lamina, and pedicle. Almost 75% of the spinal canal can be decompressed from unilateral corridor.[2] [3] [5] [8] [9] If circumferential spinal decompression is required, bilateral access may be relevant. Additional steps of rib head osteotomy, rib head disarticulation, or trap-door rib head osteotomy may augment operative corridor and can facilitate placement of the expandable cage in the thoracic spine. The primary limitation of this technique is the risk of iatrogenic spinal cord injury due to undue retraction of the thecal sac.[2] [3] [5] [8] [9]
#
Minimally Invasive Transforaminal Lumbar Interbody Fusion (MISS TLIF)
Percutaneous pedicle screw stabilization along with posterior keyhole corpectomy may be utilized in the surgical management of burst fractures of lumbar spine.[2] [3] [5] [8] [9] Denis classification subtype B or Magerl subtype A.3.1 burst fractures are common indications for this surgical technique. Advantages of TLIF approach include sparing the posterior elements and a safe decompression by using a surgical microscope.[2] [3] [5] [8] [9] Mini-TLIF offers a lower risk of injury to nerve roots and dura mater because of a more lateral entry point in comparison to mini-posterior lumbar interbody fusion (PLIF). Similarly, in a recent meta-analysis by de Kunder et al,[11] they observed that TLIF procedure has lower complication rate, surgical duration, and operative blood loss as compared with PLIF.
For mini-TLIF, patient is placed in the prone position on an adjustable surgical table to ensure optimal working trajectory by obtaining appropriate distraction and negating any excessive kyphotic deformity.[2] [3] [5] [8] [9] Skin incision is made 1.5 to 2 cm off midline on either side and they are centered appropriately at the caudal aspect of the intervertebral disc cranial to the fractured vertebrae. Using either microscopic or endoscopic view, laminar fenestration and complete facetectomy are performed to expose the nerve root, dura mater, and pedicle. It is followed by transpedicular corpectomy and interbody fusion in standard fashion with expandable interbody devices and percutaneous pedicle screws placement.[2] [3] [5] [8] [9]
#
#
Nonfusion Procedures
Percutaneous Pedicle Screw Fixation
Often placement of pedicle screws or other instrumentation in TL fractures requires extensive paraspinal muscle stripping. This requires prolonged surgical time with the patient in the prone position, and possible complications including the potential for infection, paraspinal muscular denervation with associated postoperative muscle inactivity, blood loss, muscle atrophy, and weakness.[2] [3] [6] [9] The device allows the spine to be reduced using a percutaneous pedicle screw and rod fixation, and then locked in place with setscrews. The thought process is that bluntly splitting the paraspinous muscles rather than dissecting and dividing results in less muscle atrophy, blood loss, with preservation of the normal surrounding anatomy and increased stability.[2] [3] [6] [9]
The percutaneous screw fixation technique has to be used in select subset of patients for maximum benefit and reduce the chances of implant failure. The indications of using this technique are acute type A3 AO spine fractures less than 48 to 72 hours old (which can be reduced by ligamentotaxis). Intact posterior ligamentous complex is the absolute prerequisite for performing a percutaneous procedure. The specific absolute contraindication is a three-column injury (AO spine type B and C fractures) with failure of posterior ligamentous complex, which, of course has to be supplemented with a fusion procedure also.[2] [3] [6] [9] Besides, select neurologically intact patients with TL injury classification system score of 4 can also be offered this procedure to alleviate the fracture-related pain and facilitate early mobilization ([Fig. 3]).[2] [3] [6] [9] Posterior internal stabilization can involve pedicle screws above and below the site of fracture, either two levels above and below or short-segment PSF ([Fig. 4]). Recent meta-analysis has shown the superiority of percutaneous PSF over conventional open technique, with respect to intraoperative blood loss and operative time.[4] However, there does not seem to be an apparent difference in vertebral body height, kyphosis angle, and visual analog scale pain score between open and percutaneous fixation.[4] The advantages of this procedure are decreased postoperative pain, faster postoperative mobilization, shorter length of hospitalization, shorter postoperative recovery time, and lesser disruption to paraspinal muscles and ligaments.


#
Vertebral Augmentation Procedures—Kyphoplasty and Vertebroplasty
Vertebral augmentation is a well-known minimally invasive technique utilized as a rapid and reliable way to mobilize spinal trauma patients and even provide some deformity correction ([Fig. 5]).[2] [3] [5] [6] [8] [9] There is enough evidence in the literature to suggest that symptomatic vertebral compression fractures, if left unchecked may lead to a progressive worsening in normal sagittal balance and consequent back pain and limitation of activities of daily living.[2] [3] [5] [6] [8] [9] Kyphoplasty differs from vertebroplasty by virtue of using an inflatable balloon in the vertebral body to elevate the vertebral end-plates before inserting polymethylmethacrylate (PMMA) into this cavity.[2] [3] [5] [6] [8] [9] The advantages of this procedure over vertebroplasty include more optimal vertebral body height restoration and kyphosis correction while allowing for the more controlled deposition of PMMA into the cavity.[2] [3] [5] [6] [8] [9] Theoretically this also decreases the risk of bone cement extravasation. Both procedures have been shown to reduce the back pain associated with vertebral compression fractures. The risk of cement leakage is reduced in kyphoplasty compared with vertebroplasty, because balloon-assisted cavity formation in kyphoplasty helps safer injection of cement into the vertebral body by reducing the injection pressure. Overall, the risk of spillage increases with comminution of vertebral body.[2] [3] [5] [6] [8] [9] However, a recent meta-analysis by Wang et al[17] concluded that despite the better correction of kyphotic wedge angle, lower risk of cement leakage and better restoration of vertebral height in kyphoplasty; overall clinical outcome assessed by pain scores and disability indices were similar for both kyphoplasty and vertebroplasty for osteoporotic vertebral compression fracture patients.

It is pivotal to understand that healed vertebral body fractures are stable and do not cause pain. Hence, only symptomatic fractures need surgical treatment, either via vertebroplasty or kyphoplasty. The primary aim of these augmentation procedures is to restore anatomic alignment and functionality of an individual. Fractures associated with neurologic injury, fractures with a burst component, or a fracture plane that extends into the spinal canal and healed chronic compression fractures are absolute contraindications for these percutaneous procedures. Underlying severe cardiac disease is a relative contraindication for these procedures, as PMMA contains a vasodilator agent that is rapidly absorbed systemically. Besides, vertebral augmentation can lead to increased stiffness in the treated vertebral body resulting in potentially altering the relative force distribution in the adjacent vertebral levels and predisposing them for additional osteoporotic compression fractures. However, data regarding adjacent-segment fractures after percutaneous augmentation procedures are limited.[2] [3] [5] [6] [8] [9]
#
#
#
Limitations of MIS Techniques
Despite several advances toward successful MIS for the treatment of spinal trauma, considerable limitations still exist. There is a dearth of literature on long-term follow-up of well-designed randomized controlled trials comparing open versus MIS techniques. Besides, MIS techniques can take care of a limited number of spinal levels at a time, because of the inability to contour rods for larger lengths along the normal curvature of the spine. Lastly, there is a lot of scope in the improvement in MIS techniques, especially when dealing with complex traumatic dislocations such as bilateral locked facets, which fail to reduce with traction.
#
Conclusions
Ideal management of spinal trauma patients, especially with intact neurology, is an enigmatic problem. This dilemma is faced by many neurosurgeons on daily basis. MIS is a treatment modality, which can bridge the gap between operative and conservative management for such patients. The technological advances and patient preference have led to an inevitable evolution of refined MIS techniques in spinal trauma. Using MIS principles, the patients can be mobilized earlier since the soft tissue dissection is performed to a lesser extent, further adding to faster recovery and early rehabilitation. Furthermore, current evidence points toward a reduction in operative blood loss and operative time with MIS techniques, which translates into shorter hospitalization and cost-effective utilization of the health care system. Current literature does not favor one MIS approach over the other, and the surgical approach chosen should be tailored according to the patient’s clinical and radiological findings, presence/absence of polytrauma, the likelihood of survival of patient, and surgeon’s preference and expertise.
#
#
Note
The manuscript has not been published in part or full at any online or print publication site/journal. The manuscript has been reviewed, edited, and approved by all authors before submission.
Conflict of Interest
None declared.
-
References
- 1 Amini A, Beisse R, Schmidt MH. Thoracoscopic spine surgery for decompression and stabilization of the anterolateral thoracolumbar spine. Neurosurg Focus 2005; 19 (06) E4
- 2 Dhall SS, Wadhwa R, Wang MY, Tien-Smith A, Mummaneni PV. Traumatic thoracolumbar spinal injury: an algorithm for minimally invasive surgical management. Neurosurg Focus 2014; 37 (01) E9
- 3 Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus 2014; 37 (01) E11
- 4 McAnany SJ, Overley SC, Kim JS, Baird EO, Qureshi SA, Anderson PA. Open versus minimally invasive fixation techniques for thoracolumbar trauma: a meta-analysis. Global Spine J 2016; 6 (02) 186-194
- 5 Smith JS, Ogden AT, Fessler RG. Minimally invasive posterior thoracic fusion. Neurosurg Focus 2008; 25 (02) E9
- 6 Zairi F, Court C, Tropiano P. et al; French Society of Spine Surgery. Minimally invasive management of thoraco-lumbar fractures: combined percutaneous fixation and balloon kyphoplasty. Orthop Traumatol Surg Res 2012; 98 (Suppl. 06) S105-S111
- 7 Thongtrangan I, Le H, Park J, Kim DH. Minimally invasive spinal surgery: a historical perspective. Neurosurg Focus 2004; 16 (01) E13
- 8 Oh T, Scheer JK, Fakurnejad S, Dahdaleh NS, Smith ZA. Minimally invasive spinal surgery for the treatment of traumatic thoracolumbar burst fractures. J Clin Neurosci 2015; 22 (01) 42-47
- 9 Lall RR, Smith ZA, Wong AP, Miller D, Fessler RG. Minimally invasive thoracic corpectomy: surgical strategies for malignancy, trauma, and complex spinal pathologies. Minim Invasive Surg 2012; 2012: 213791
- 10 Arnold PM, Anderson KK, McGuire Jr RA. The lateral transpsoas approach to the lumbar and thoracic spine: a review. Surg Neurol Int 2012; 3 (Suppl. 03) S198-S215
- 11 de Kunder SL, van Kuijk SMJ, Rijkers K. et al. Transforaminal lumbar interbody fusion (TLIF) versus posterior lumbar interbody fusion (PLIF) in lumbar spondylolisthesis: a systematic review and meta-analysis. Spine J 2017; 17 (11) 1712-1721
- 12 Epstein NE. Review of risks and complications of extreme lateral interbody fusion (XLIF). Surg Neurol Int 2019; 10: 237
- 13 Jin J, Ryu KS, Hur JW, Seong JH, Kim JS, Cho HJ. Comparative study of the difference of perioperative complication and radiologic results: MIS-DLIF (minimally invasive direct lateral lumbar interbody fusion) versus MIS-OLIF (minimally invasive oblique lateral lumbar interbody fusion). Clin Spine Surg 2018; 31 (01) 31-36
- 14 Li R, Li X, Zhou H, Jiang W. Development and application of oblique lumbar interbody fusion. Orthop Surg 2020; 12 (02) 355-365
- 15 Litré CF, Duntze J, Benhima Y. et al. Anterior minimally invasive extrapleural retroperitoneal approach to the thoraco-lumbar junction of the spine. Orthop Traumatol Surg Res 2013; 99 (01) 94-98
- 16 Scherman DB, Rao PJ, Phan K, Mungovan SF, Faulder K, Dandie G. Outcomes of direct lateral interbody fusion (DLIF) in an Australian cohort. J Spine Surg 2019; 5 (01) 1-12
- 17 Wang B, Zhao CP, Song LX, Zhu L. Balloon kyphoplasty versus percutaneous vertebroplasty for osteoporotic vertebral compression fracture: a meta-analysis and systematic review. J Orthop Surg Res 2018; 13 (01) 264
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
23. Februar 2021
© 2021. Neurotrauma Society of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Amini A, Beisse R, Schmidt MH. Thoracoscopic spine surgery for decompression and stabilization of the anterolateral thoracolumbar spine. Neurosurg Focus 2005; 19 (06) E4
- 2 Dhall SS, Wadhwa R, Wang MY, Tien-Smith A, Mummaneni PV. Traumatic thoracolumbar spinal injury: an algorithm for minimally invasive surgical management. Neurosurg Focus 2014; 37 (01) E9
- 3 Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus 2014; 37 (01) E11
- 4 McAnany SJ, Overley SC, Kim JS, Baird EO, Qureshi SA, Anderson PA. Open versus minimally invasive fixation techniques for thoracolumbar trauma: a meta-analysis. Global Spine J 2016; 6 (02) 186-194
- 5 Smith JS, Ogden AT, Fessler RG. Minimally invasive posterior thoracic fusion. Neurosurg Focus 2008; 25 (02) E9
- 6 Zairi F, Court C, Tropiano P. et al; French Society of Spine Surgery. Minimally invasive management of thoraco-lumbar fractures: combined percutaneous fixation and balloon kyphoplasty. Orthop Traumatol Surg Res 2012; 98 (Suppl. 06) S105-S111
- 7 Thongtrangan I, Le H, Park J, Kim DH. Minimally invasive spinal surgery: a historical perspective. Neurosurg Focus 2004; 16 (01) E13
- 8 Oh T, Scheer JK, Fakurnejad S, Dahdaleh NS, Smith ZA. Minimally invasive spinal surgery for the treatment of traumatic thoracolumbar burst fractures. J Clin Neurosci 2015; 22 (01) 42-47
- 9 Lall RR, Smith ZA, Wong AP, Miller D, Fessler RG. Minimally invasive thoracic corpectomy: surgical strategies for malignancy, trauma, and complex spinal pathologies. Minim Invasive Surg 2012; 2012: 213791
- 10 Arnold PM, Anderson KK, McGuire Jr RA. The lateral transpsoas approach to the lumbar and thoracic spine: a review. Surg Neurol Int 2012; 3 (Suppl. 03) S198-S215
- 11 de Kunder SL, van Kuijk SMJ, Rijkers K. et al. Transforaminal lumbar interbody fusion (TLIF) versus posterior lumbar interbody fusion (PLIF) in lumbar spondylolisthesis: a systematic review and meta-analysis. Spine J 2017; 17 (11) 1712-1721
- 12 Epstein NE. Review of risks and complications of extreme lateral interbody fusion (XLIF). Surg Neurol Int 2019; 10: 237
- 13 Jin J, Ryu KS, Hur JW, Seong JH, Kim JS, Cho HJ. Comparative study of the difference of perioperative complication and radiologic results: MIS-DLIF (minimally invasive direct lateral lumbar interbody fusion) versus MIS-OLIF (minimally invasive oblique lateral lumbar interbody fusion). Clin Spine Surg 2018; 31 (01) 31-36
- 14 Li R, Li X, Zhou H, Jiang W. Development and application of oblique lumbar interbody fusion. Orthop Surg 2020; 12 (02) 355-365
- 15 Litré CF, Duntze J, Benhima Y. et al. Anterior minimally invasive extrapleural retroperitoneal approach to the thoraco-lumbar junction of the spine. Orthop Traumatol Surg Res 2013; 99 (01) 94-98
- 16 Scherman DB, Rao PJ, Phan K, Mungovan SF, Faulder K, Dandie G. Outcomes of direct lateral interbody fusion (DLIF) in an Australian cohort. J Spine Surg 2019; 5 (01) 1-12
- 17 Wang B, Zhao CP, Song LX, Zhu L. Balloon kyphoplasty versus percutaneous vertebroplasty for osteoporotic vertebral compression fracture: a meta-analysis and systematic review. J Orthop Surg Res 2018; 13 (01) 264