

Subscribe to RSS
DOI: 10.1055/s-0040-1712917
Ectopic Cerebellar Tissue in the Occipital Bone: A Case Report
Authors
Funding Not applicable.
Address for correspondence
Publication History
25 March 2019
28 September 2019
Publication Date:
08 August 2020 (online)


Abstract
Ectopic cerebellar tissue has only been described in isolated case reports, with only two reported cases in adult patients. We report the case of a 63-year-old woman with progressive, medically refractory headaches. A scan showed an intraosseous lesion of the midline occipital bone. Surgical resection of the soft tissue lesion was undertaken. Her headaches ceased postoperatively. Histopathological analysis revealed cerebellar cortical tissue with a surrounding meningothelial cell layer, characteristic of cerebellar ectopia. This is the second reported case of an intraosseous location of this lesion, and only the third case described in an adult patient. Our findings illustrate a rare cause of headaches and support the therapeutic roles of surgical treatment for this extremely rare condition.
Keywords
ectopic cerebellar tissue - glioneuronal ectopia - intraosseous lesion - headache - occipital bone - craniectomyIntroduction
Ectopic cerebellar tissue is an extremely uncommon finding, occurring as both an isolated finding and in conjunction with other neurological disorders. The condition remains poorly understood due to its rarity and diverse clinical presentations. Only two cases have previously been described in adults, and only one in an intraosseous location.[1] We describe the case of an adult patient presenting with headaches which were found to be associated with a small nodule of ectopic cerebellar tissue in the midline occipital bone. Cessation of the headaches upon removal of the lesion suggests a causative relationship. We present clinical, operative, radiographic, and histopathologic findings and their implications for our understanding of this rare lesion.
Case Report
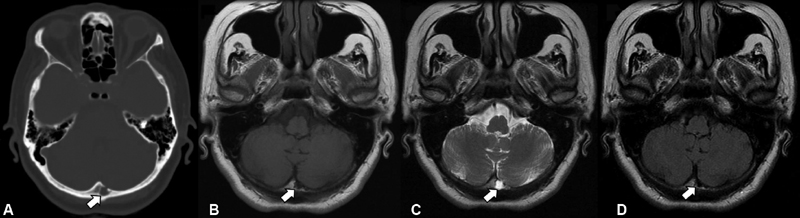
A 63-year-old Hispanic woman with no significant past medical or neurological history presented with several years of progressive, medically refractory occipital headaches. The pain was of a pounding quality and associated with nausea. Symptoms occurred daily, without obvious aggravating or alleviating factors. Work-up of primary and secondary headache disorders, with empiric medication trials where appropriate, had been negative over the preceding 2 years. Noncontrast computed tomography (CT) and magnetic resonance imaging (MRI) of the brain showed a 1-cm, well-demarcated spherical lesion in the occipital bone just to the left of midline There was a small opening into the posterior fossa. The lesion appeared to be lytic on CT without obvious abnormalities in the surrounding bone. It paralleled cerebrospinal fluid (CSF) on all MRI sequences ([Fig. 1]).
An exploratory suboccipital craniectomy for resection of the lesion was undertaken. Upon removal of the outer cortical bone overlying the lesion, a smooth-walled bony cavity was found. Inside the cavity laid a small mass of red and off-white friable tissue with a thin translucent surrounding membrane. The inner cortical bone was eroded revealing the underlying cerebellar dura. The dura appeared intact, and the lesion was confirmed to be anatomically isolated from the dura or brain. The lesion was carefully resected en bloc with a curette. The patient tolerated the procedure without any complications and returned home on the first postoperative day. Her headaches substantially decreased in frequency and intensity immediately postoperatively and remained controlled at the last follow-up 9 months later.
Histopathological analysis showed non-neoplastic cerebellar cortex comprising molecular and granular layers with a small number of Purkinje cells. A thin layer of fibrous tissue with overlying meningothelial cells was also noted. The surrounding bone demonstrated reactive changes and benign spindle cells with immunohistochemical staining positive for epithelial membrane antigen, supporting meningothelial origin ([Fig. 2]).

Discussion
Ectopic cerebellar tissue, also known as cerebellar ectopia, was first reported in 1973 by Billings and Danziger, in a 9-month-old infant presenting with hydrocephalus, macrocephaly, and developmental delay. The patient was found to have a 1-cm focus of ectopic cerebellar tissue in the roof of the fourth ventricle that was resected successfully.[2] To our knowledge, this condition has been documented in only two previous adult cases and 14 pediatric cases, without obvious gender predilection.[1] [3] [4] The anatomic location of the ectopic tissue in prior cases is extremely heterogeneous, including the orbit,[5] [6] anterior fossa,[7] suprasellar region,[8] [9] posterior fossa,[10] [11] and even the spinal cord.[4] [12] [13]
The diagnosis of ectopic cerebellar tissue requires a high degree of suspicion due to its protean clinical manifestations. The lesion may be associated with abnormalities such as teratoma, intracranial cysts, Chiari I malformation, or spinal dysraphism. In these situations, presenting symptoms are likely due to the associated abnormality, and the cerebellar tissue is discovered intraoperatively and/or upon histopathological examination. In other cases, the lesion may be an incidental finding in screening studies or the work up of other conditions. Alternatively, ectopic tissue may cause symptoms related to mass effect (proptosis, hydrocephalus, syringohydromyelia, etc.), impingement on structures such as the optic nerve, or cortical irritation causing epilepsy.[1] The radiographic appearance of the lesion may resemble gray matter and/or CSF when occurring in isolation, or the surrounding pathology when associated with other abnormalities.
The pathogenesis of ectopic cerebellar tissue is not known, but may relate to abnormal cell migration or differentiation during development, such as in other forms of glioneuronal ectopia and heterotopia.[14] The condition has also been hypothesized to arise from herniation of mature tissue through a pial defect.[1] Given the surrounding meningothelial cell layer in our case, it is also possible these lesions could represent congenital meningoencephaloceles or cystic intraosseous arachnoid granulations/diverticula that subsequently disconnect later in life. We propose that these hypotheses may not be mutually exclusive; the underlying mechanism may instead depend upon the anatomical location and associated pathologies, converging upon histologically identical differentiated cerebellar tissue.
Only two prior reports have documented headache in association with ectopic cerebellar tissue; the patients were 5 and 15 years of age, respectively. Interestingly, in both cases the ectopic tissue was in the supracerebellar region and connected to the cerebellum via a stalk, without associated hydrocephalus or other abnormalities. Surgical resection was both diagnostic and therapeutic in the former case,[11] while the diagnosis was made by diffusion tensor imaging and the lesion managed expectantly in the latter.[3] Our report thus represents the first case of an adult presenting with headache in this condition.
Similarly, there are only two prior reports of ectopic cerebellar tissue in adults. Matyja et al described a 25-year-old woman with complex partial seizures; midline deformities including hypertelorism, low-set hairline, and nose deformations; and a large mass at the base of the mesial frontal lobes. Resection of the mass disclosed ectopic cerebellar and heterogenous neuroglial tissue and scattered thin-walled, dilated vessels.[7] Subsequently, Kawashima et al described the case of a 46-year-old woman who was incidentally found to have a small lesion in the right side of the occipital bone, which was excised during suboccipital craniotomy for hemifacial spasm. This is also the only prior report of an intraosseous location of ectopic cerebellar tissue. The radiographic, gross, and histopathological characteristics were quite similar to the findings in our case.[1]
Given that the lesion was asymptomatic in the other intraosseous case, it may be possible that our patient's headaches were due to a different cause and abated independently of surgical resection. However, the mechanism underlying pain in this condition remains unknown, and the prior report of surgical resection curing a pediatric patient's headache[11] must also be taken into account. Indeed, it is possible that slow growth of the lesion over time caused it to become symptomatic and accounted for the delayed presentation in our patient.
The pathogenesis, natural history, and symptoms associated with ectopic cerebellar tissue remain poorly understood. However, this condition must remain in the differential diagnosis of isolated intraosseous masses in adults. Surgical resection plays a critical role in providing definitive tissue diagnosis to distinguish the lesion from intraosseous neoplasms such as meningioma, lymphoma, dermoid cyst, and hemangioma.
Conflict of Interest
The authors have no conflicts of interest to declare.
Acknowledgment
Not applicable.
-
References
- 1 Kawashima M, Kobayashi M, Ishizawa K, Fujimaki T. Ectopic cerebellar tissue in the occipital bone: a case report. J Med Case Rep 2017; 11 (01) 231
- 2 Billings KJ, Danziger FS. Cerebellar heterotopia. Case report. J Neurosurg 1973; 38 (02) 218-220
- 3 Algin O, Ozmen E. Ectopic anterior cerebellum (ala lobule centralis). Neuroradiol J 2015; 28 (03) 278-280
- 4 Kumar R, Prakash M. Unusual split cord with neurenteric cyst and cerebellar heterotopia over spinal cord. Childs Nerv Syst 2007; 23 (02) 243-247
- 5 Call NB, Baylis HI. Cerebellar heterotopia in the orbit. Arch Ophthalmol 1980; 98 (04) 717-719
- 6 Kagotani Y, Takao K, Nomura K, Imai Y, Hashimoto K. Intraorbital cerebellar heterotopia associated with Chiari I malformation. J Pediatr Ophthalmol Strabismus 1996; 33 (05) 262-265
- 7 Matyja E, Grajkowska W, Marchel A, Rysz A, Majkowska-Zwolinska B. Ectopic cerebellum in anterior cranial fossa: report of a unique case associated with skull congenital malformations and epilepsy. Am J Surg Pathol 2007; 31 (02) 322-325
- 8 Chang AH, Kaufmann WE, Brat DJ. Ectopic cerebellum presenting as a suprasellar mass in infancy: implications for cerebellar development. Pediatr Dev Pathol 2001; 4 (01) 89-93
- 9 Takhtani D, Melhem ER, Carson BS. A heterotopic cerebellum presenting as a suprasellar mass with associated nasopharyngeal teratoma. AJNR Am J Neuroradiol 2000; 21 (06) 1119-1121
- 10 Gunbey HP, Bilgici MC, Aslan K, Aygün C, Celik H. Ectopic cerebellar tissue of the posterior cranial fossa: diffusion tensor tractography and MR spectroscopy findings. Childs Nerv Syst 2016; 32 (01) 195-198
- 11 Nagaraj U, Boue DR, Humphrey B, Martin LC. Ectopic cerebellum in the posterior cranial fossa. Pediatr Radiol 2012; 42 (11) 1391-1394
- 12 Chung CJ, Castillo M, Fordham L, Mukherji S, Boydston W, Hudgins R. Spinal intradural cerebellar ectopia. AJNR Am J Neuroradiol 1998; 19 (05) 897-899
- 13 Suneson A, Kalimo H. Myelocystocele with cerebellar heterotopia. Case report. J Neurosurg 1979; 51 (03) 392-396
- 14 Muzumdar D, Michaud J, Ventureyra EC. Anterior cranial base glioneuronal heterotopia. Childs Nerv Syst 2006; 22 (03) 227-233
Address for correspondence
-
References
- 1 Kawashima M, Kobayashi M, Ishizawa K, Fujimaki T. Ectopic cerebellar tissue in the occipital bone: a case report. J Med Case Rep 2017; 11 (01) 231
- 2 Billings KJ, Danziger FS. Cerebellar heterotopia. Case report. J Neurosurg 1973; 38 (02) 218-220
- 3 Algin O, Ozmen E. Ectopic anterior cerebellum (ala lobule centralis). Neuroradiol J 2015; 28 (03) 278-280
- 4 Kumar R, Prakash M. Unusual split cord with neurenteric cyst and cerebellar heterotopia over spinal cord. Childs Nerv Syst 2007; 23 (02) 243-247
- 5 Call NB, Baylis HI. Cerebellar heterotopia in the orbit. Arch Ophthalmol 1980; 98 (04) 717-719
- 6 Kagotani Y, Takao K, Nomura K, Imai Y, Hashimoto K. Intraorbital cerebellar heterotopia associated with Chiari I malformation. J Pediatr Ophthalmol Strabismus 1996; 33 (05) 262-265
- 7 Matyja E, Grajkowska W, Marchel A, Rysz A, Majkowska-Zwolinska B. Ectopic cerebellum in anterior cranial fossa: report of a unique case associated with skull congenital malformations and epilepsy. Am J Surg Pathol 2007; 31 (02) 322-325
- 8 Chang AH, Kaufmann WE, Brat DJ. Ectopic cerebellum presenting as a suprasellar mass in infancy: implications for cerebellar development. Pediatr Dev Pathol 2001; 4 (01) 89-93
- 9 Takhtani D, Melhem ER, Carson BS. A heterotopic cerebellum presenting as a suprasellar mass with associated nasopharyngeal teratoma. AJNR Am J Neuroradiol 2000; 21 (06) 1119-1121
- 10 Gunbey HP, Bilgici MC, Aslan K, Aygün C, Celik H. Ectopic cerebellar tissue of the posterior cranial fossa: diffusion tensor tractography and MR spectroscopy findings. Childs Nerv Syst 2016; 32 (01) 195-198
- 11 Nagaraj U, Boue DR, Humphrey B, Martin LC. Ectopic cerebellum in the posterior cranial fossa. Pediatr Radiol 2012; 42 (11) 1391-1394
- 12 Chung CJ, Castillo M, Fordham L, Mukherji S, Boydston W, Hudgins R. Spinal intradural cerebellar ectopia. AJNR Am J Neuroradiol 1998; 19 (05) 897-899
- 13 Suneson A, Kalimo H. Myelocystocele with cerebellar heterotopia. Case report. J Neurosurg 1979; 51 (03) 392-396
- 14 Muzumdar D, Michaud J, Ventureyra EC. Anterior cranial base glioneuronal heterotopia. Childs Nerv Syst 2006; 22 (03) 227-233