Keywords
arteries - aorta - multidetector computed tomography - inferior phrenic artery - celiac
artery - chemoembolization - hemoptysis
Introduction
Inferior phrenic arteries (IPAs) are small caliber paired arteries supplying diaphragm
with small branches to the liver, adrenal glands, and gastroesophageal junction. Though
the right inferior phrenic artery (RIPA) and the left inferior phrenic artery (LIPA)
commonly originate from the aorta or celiac artery, they frequently show variations
in their origins.[1] IPA is involved in various pathologic conditions like hemoptysis due to lower lobe
lung abnormality, bleeding due to diaphragm/liver trauma, bleeding from gastroesophageal
pathologies like Mallory-Weiss tear or tumor.[2]
[3]
[4]
[5]
[6] The RIPA is the most common extrahepatic blood supply to hepatocellular carcinoma
(HCC), especially those located near the bare area of the liver and exophytic lesions
abutting the undersurface of the diaphragm.[7] Knowledge of the variations helps to achieve effective treatment of HCC by transarterial
chemoembolization (TACE) and other pathologies related to IPA. We undertook this study
to document the frequency and pattern of variations in the origins of IPA.
Aim
The study aims to evaluate the frequency and pattern of variations in the origins
of RIPA and LIPA on 256 slice multidetector computed tomography (MDCT).
Materials and Methods
Study Population
An institutional review board approved this retrospective study. Informed consent
was taken before the CT scans. Between January 2018 and November 2019, abdominal CT
angiography (CTA) images of 600 patients (male:female = 344:256; mean age 56.45 ±
12.96 years) who underwent technically successful multiphase CT for cirrhosis without
HCC or hepatic vascular disease, mesenteric ischemia, gastrointestinal bleed, peripheral
arterial disease, donor patients for renal/liver transplantation, renal artery stenosis,
and aortic aneurysms were included. None of the patients included in the study had
primary or metastatic hepatic neoplasm, pleural or diaphragmatic disease, at the time
of the CT scan. Images of patients who had severe atherosclerosis, and/or movement
artifacts preventing assessment of the IPAs were also excluded from the study ([Fig. 1]).
 Fig. 1 Diagram showing included and excluded patients in the study. CT, computed tomography;
HCC, hepatocellular carcinoma; IPA, inferior phrenic artery; MDCT, multidetector computed
tomography.
Fig. 1 Diagram showing included and excluded patients in the study. CT, computed tomography;
HCC, hepatocellular carcinoma; IPA, inferior phrenic artery; MDCT, multidetector computed
tomography.
CT Technique
Multiphase computed tomography was performed with a 256-section multidetector CT scanner
(Philips 256 slice ICT, Philips Healthcare). Scanning parameters are shown in [Table 1]. Contrast-enhanced images were obtained in the bolus-triggered arterial phase and
delayed venous phases. A region of interest was placed over the descending thoracic
aorta, 2 cm proximal to the diaphragm, and the scanning was initiated 6 seconds after
the threshold of 150 HU was reached. Patients were scanned at 120 kV with an active
dose reduction index (DRI-20).
Table 1
Multidetector computed tomography parameters used for scanning patients
|
Parameter
|
Comment
|
|
Abbreviations: AP, arterial phase; DRI, dose reduction index; HU, Hounsfield; IV,
intravenous; ROI, region of interest.
|
|
Peak voltage (kVp)
|
120 kVP
|
|
Effective (mAs)
|
150–350 mAs (DRI-20)
|
|
Rotation time (s)
|
0.5 s
|
|
Detector collimation
|
128 × 0.625 mm
|
|
Pitch
|
0.914
|
|
Matrix
|
512 × 512
|
|
Reconstruction slice thickness
|
1.0 mm
|
|
Reconstruction method
|
iDose-4
|
|
IV contrast
|
Omnipaque 350 (iohexol); volume: 1.5 mL/kg; rate: 4–6 mL/s.
|
|
Scan delay
|
Hepatic AP: 15 s; other AP: 6 s (bolus tracking; ROI—descending aorta, 2 cm above).
|
Image Interpretation
The image analysis was done on dedicated workstations (Philips Healthcare) which allowed
three-dimensional postprocessing with multiplanar image reformatting and maximum intensity
projections. Arterial phase CT images with 1-mm slice thickness were used to assess
the IPA. All images were reviewed by a radiologist with 10 years of experience in
abdominal CT imaging. The IPAs were assessed with emphasis on their origins and results
analyzed.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics 20.0 software (IBM Corp.).
The data was analyzed using descriptive statistical methods. Quantitative variables
were expressed as mean values and standard deviations.
Results
Both IPA origins were documented in all patients. IPAs were divided into two groups:
those originating from a common trunk and those originating independently from different
sources without a truncus. Both RIPA and LIPA originated from a common trunk in 128
(21.3%) patients ([Fig. 2]). The truncus originated from the aorta in 68 (11.3%) patients and from the celiac
artery in 58 (9.6%) patients ([Fig. 3]). Both RIPA and LIPA originated from a common trunk in one patient (0.2%) each from
the left renal artery and left gastric artery ([Figs. 4]
[5]). The RIPA and the LIPA originated independently in 472 (78.6%) patients ([Figs. 6]
[7]). The RIPA most commonly originated from the abdominal aorta in 225 (37.5%) patients,
followed by the celiac artery in 177 (29.5%), right renal artery in 59 (9.8%), left
gastric artery in 9 (1.5%), and 1 (0.2%) each from common hepatic artery (CHA) and
superior mesenteric artery (SMA), respectively ([Figs. 8]
[9]
[10]
[11]). The LIPA most commonly originated from the celiac artery in 278 (46.3%) followed
by the abdominal aorta in 181 (30.1%), left renal artery in 7 (1.1%), and splenic
artery in 6 (1.0%) ([Figs. 8]
[9]
[10]
[12]
[13]). In patients with IPA originating from the aorta, the origins were from the anterior,
lateral. or posterior aspect of the aorta. The least frequently detected IPA variations
were RIPA originating from the CHA and SMA. We also observed that in patients with
multiple renal arteries, IPA originated from the uppermost renal artery ([Fig. 11]).
 Fig. 2 Schematic representation of origin of inferior phrenic arteries with common trunk.
CA, celiac artery, CHA, common hepatic artery; LGA, left gastric artery; LIPA, left
inferior phrenic artery; LRA, left renal artery; RIPA, right inferior phrenic artery;
RRA, right renal artery; SA, splenic artery; SMA, superior mesenteric artery.
Fig. 2 Schematic representation of origin of inferior phrenic arteries with common trunk.
CA, celiac artery, CHA, common hepatic artery; LGA, left gastric artery; LIPA, left
inferior phrenic artery; LRA, left renal artery; RIPA, right inferior phrenic artery;
RRA, right renal artery; SA, splenic artery; SMA, superior mesenteric artery.
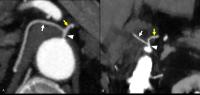 Fig. 3 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) and left IPA (A, B
yellow arrow) originating from aorta (A
arrowhead) and celiac artery (B
arrowhead) as common trunk. IPA, inferior phrenic artery.
Fig. 3 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) and left IPA (A, B
yellow arrow) originating from aorta (A
arrowhead) and celiac artery (B
arrowhead) as common trunk. IPA, inferior phrenic artery.
 Fig. 4 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) and left IPA (A, B
yellow arrow) originating from left renal artery (A, B
arrowhead) as common trunk. IPA, inferior phrenic artery.
Fig. 4 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) and left IPA (A, B
yellow arrow) originating from left renal artery (A, B
arrowhead) as common trunk. IPA, inferior phrenic artery.
 Fig. 5 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) and left IPA (A, B
yellow arrow) originating from left gastric artery (A, B
arrowhead) as common trunk. IPA, inferior phrenic artery.
Fig. 5 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) and left IPA (A, B
yellow arrow) originating from left gastric artery (A, B
arrowhead) as common trunk. IPA, inferior phrenic artery.
 Fig. 6 Schematic representation of origin of RIPAs from different sources without common
trunk. CA, celiac artery; CHA, common hepatic artery; LGA, left gastric artery; LRA,
left renal artery; RIPA, right inferior phrenic artery; RRA, right renal artery; SA,
splenic artery; SMA, superior mesenteric artery.
Fig. 6 Schematic representation of origin of RIPAs from different sources without common
trunk. CA, celiac artery; CHA, common hepatic artery; LGA, left gastric artery; LRA,
left renal artery; RIPA, right inferior phrenic artery; RRA, right renal artery; SA,
splenic artery; SMA, superior mesenteric artery.
 Fig. 7 Schematic representation of origin of LIPAs from different sources without common
trunk. CA, celiac artery; CHA, common hepatic artery; LGA, left gastric artery; LIPA,
left inferior phrenic artery; LRA, left renal artery; RRA, right renal artery; SA,
splenic artery; SMA, superior mesenteric artery.
Fig. 7 Schematic representation of origin of LIPAs from different sources without common
trunk. CA, celiac artery; CHA, common hepatic artery; LGA, left gastric artery; LIPA,
left inferior phrenic artery; LRA, left renal artery; RRA, right renal artery; SA,
splenic artery; SMA, superior mesenteric artery.
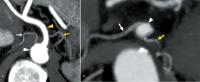 Fig. 8 (A, B) Multidetector computed tomography arterial phase maximum intensity projection images
show right inferior phrenic artery (RIPA, white arrow) and left inferior phrenic artery (LIPA, yellow arrow) originating separately without common truncus. (A) RIPA originates from aorta (white arrowhead) and LIPA from celiac artery (yellow arrowhead). (B) Both RIPA and LIPA originate from celiac artery (white arrowhead).
Fig. 8 (A, B) Multidetector computed tomography arterial phase maximum intensity projection images
show right inferior phrenic artery (RIPA, white arrow) and left inferior phrenic artery (LIPA, yellow arrow) originating separately without common truncus. (A) RIPA originates from aorta (white arrowhead) and LIPA from celiac artery (yellow arrowhead). (B) Both RIPA and LIPA originate from celiac artery (white arrowhead).
 Fig. 9 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) originating from the celiac artery (A, B
arrowhead) and left IPA (B, C
yellow arrow) originating from left renal artery (B, C
yellow arrowhead). IPA, inferior phrenic artery.
Fig. 9 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) originating from the celiac artery (A, B
arrowhead) and left IPA (B, C
yellow arrow) originating from left renal artery (B, C
yellow arrowhead). IPA, inferior phrenic artery.
 Fig. 10 (A, B) Multidetector computed tomography arterial phase maximum intensity projection images
show right inferior phrenic artery (RIPA, white arrow) and left inferior phrenic artery (LIPA, yellow arrow) originating separately without common truncus. (A) RIPA originates from left gastric artery (white arrowhead) and LIPA from aorta (yellow arrowhead). (B) LIPA originates from left gastric artery (yellow arrowhead).
Fig. 10 (A, B) Multidetector computed tomography arterial phase maximum intensity projection images
show right inferior phrenic artery (RIPA, white arrow) and left inferior phrenic artery (LIPA, yellow arrow) originating separately without common truncus. (A) RIPA originates from left gastric artery (white arrowhead) and LIPA from aorta (yellow arrowhead). (B) LIPA originates from left gastric artery (yellow arrowhead).
 Fig. 11 Multidetector computed tomography arterial phase maximum intensity projection images
show right inferior phrenic artery (RIPA; A, B
white arrow) originating separately without common truncus. (A) RIPA originates from right renal artery (white arrowhead); (B) RIPA originates from accessory superior right renal artery (white arrowhead).
Fig. 11 Multidetector computed tomography arterial phase maximum intensity projection images
show right inferior phrenic artery (RIPA; A, B
white arrow) originating separately without common truncus. (A) RIPA originates from right renal artery (white arrowhead); (B) RIPA originates from accessory superior right renal artery (white arrowhead).
 Fig. 12 Multidetector computed tomography arterial phase maximum intensity projection images
show left inferior phrenic artery (LIPA; A, B
yellow arrow) originating separately without common truncus. (A) LIPA originates from thoracic aorta (yellow arrowhead). (B) LIPA originates from splenic artery (yellow arrowhead).
Fig. 12 Multidetector computed tomography arterial phase maximum intensity projection images
show left inferior phrenic artery (LIPA; A, B
yellow arrow) originating separately without common truncus. (A) LIPA originates from thoracic aorta (yellow arrowhead). (B) LIPA originates from splenic artery (yellow arrowhead).
 Fig. 13 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) originating from the left gastric artery (A, B
white arrowhead) and left IPA (B, yellow arrow) originating from celiac artery (B
yellow arrowhead). IPA, inferior phrenic artery.
Fig. 13 Multidetector computed tomography arterial phase maximum intensity projection images
show right IPA (A, B
white arrow) originating from the left gastric artery (A, B
white arrowhead) and left IPA (B, yellow arrow) originating from celiac artery (B
yellow arrowhead). IPA, inferior phrenic artery.
Discussion
Advances in CT technology have expanded its role in vascular imaging. Faster scanning
and multiplanar reconstruction capabilities allow clear visualization of smaller arteries
in different parts of the body. This, in turn, helps in studying vascular anatomy,
variations, anomalies, and various vascular pathologies. Though digital subtraction
angiography (DSA) is the gold standard for vascular imaging, because of wide variations
associated with the origins of the small abdominal visceral arteries, overlapping
structures during DSA, poor breath-hold of the patients, and bowel gas artifacts,
it is not always easy to detect the arterial anatomy/pathology on DSA. MDCT with three-dimensional
reconstruction capability helps in delineating the anatomy and detecting the pathology
accurately.[1]
[8] CTA prior to the vascular interventional procedure helps in identifying the culprit
artery and its variations allowing us to draw up a clear strategy and plan the embolization
technique to be used. These in turn significantly reduce the procedure time, contrast
usage, and radiation exposure. IPA are millimetric sized arteries and not always easy
to visualize. The appropriately timed arterial phase is required for the adequate
visualization of the IPA. We had obtained contrast-enhanced images using bolus triggering
technique which helps in adequate opacification of arteries. Studies have shown that
a higher rate of injection of the contrast improves the detection in gastrointestinal
bleed patients which indirectly means better visualization of the smaller arteries
like IPA.[9] Technically inadequate CT scans and those with movement artifacts pose a challenge
in the assessment of the IPA origins. Severe atherosclerotic calcification of the
aorta or occlusion of the aorta and celiac artery also makes the interpretation of
the origins of IPA difficult.[1]
[10] Ozbulbul et al in their study of 200 patients had shown the importance of arterial-phase
images for demonstrating the origins of IPAs in a population without liver disease.[10] In our study, we had a heterogeneous patient population including cirrhotic patients
without HCC (33.3%). We were able to document the origins of both the RIPA and LIPA
in all patients.
Variations in the Origins of IPA and the Embryological Basis
The origin of IPAs can be from the aorta, celiac artery, or from other visceral arteries.[1]
[11] In the study conducted by Basile et al the authors reported 13 different variations
in the origin of IPA using MDCT. However, this study did not separately mention the
origin from a common trunk.[12] Loukas et al conducted a study on cadavers and classified the origins of LIPA and
RIPA into five groups.[11] In both these studies, the most common site of origin of IPA was the celiac artery.
Ozbulbul et al reported the variations in IPA origin in 200 patients without liver
disease on CTA.[10] The authors have reported the rare origin of RIPA from the proper hepatic artery.
Aslaner et al also studied the variations in the IPA origins on CTA in 1,000 patients.[13] The authors reported common trunk of IPA origin in 295 (29.5%) patients, with common
trunk originating in most of the cases from the aorta (16.4%) followed by celiac artery
(12.6%), right renal artery (0.4%), and left gastric artery (0.1%), in descending
order. Our study is one of the larger studies in the printed literature in terms of
the number of patients analyzed for IPA origin variations. We found 12 different types
of variations in the origins of RIPA and LIPA ([Table 2]). In our study, both RIPA and LIPA originated from a common trunk in 128 (21.3%)
patients. As in the previous study, common trunk originated from the aorta in most
patients (128, 21.3%), followed by the celiac artery in 58 (9.6%) patients. We also
found the rare origins of the common trunk from the left gastric artery (1, 0.2%)
and left renal artery (1, 0.2%) in our patients ([Figs. 4]
[5]). In fact, the common truncus from the left renal artery has not been reported in
the previous studies ([Fig. 4]). However, we did not observe a rare common trunk originating from the right renal
artery as reported by the previous authors.[13] The RIPA and the LIPA originated independently in 472 (78.6%) patients. In patients
without a common trunk, RIPA most commonly originated from the aorta (225, 37.5%)
and LIPA from a celiac artery (278, 46.3%). This contrasts with the previous studies
which have observed that RIPA most commonly originates from the celiac artery.[11]
[12] We observed that 46.3% of LIPA originated from the celiac artery. This observation
is similar to other studies.[12]
[13] We discovered a RIPA originating from SMA (0.2%) and LIPA originating from the splenic
artery (1.0%), which have not been described in prior studies. As documented previously,
in our study also, most of the IPAs originated from a segment of the aorta between
the diaphragm and the renal arteries consistently.[13] However, in one patient, the LIPA originated from the left lateral wall from the
lower thoracic aorta just above the level of diaphragm ([Fig. 12]).
Table 2
Variations in the origins of RIPA and LIPA
|
N = 600
|
|
Common origin
|
RIPA+LIPA
|
|
Abbreviations: LIPA, left inferior phrenic artery; RIPA, right inferior phrenic artery;
SMA, superior mesenteric artery.
|
|
Aorta
|
68 (11.3%)
|
|
Celiac
|
58 (9.6%)
|
|
Left gastric artery
|
1 (0.2%)
|
|
Left renal artery
|
1 (0.2%)
|
|
Separate origin
|
RIPA
|
LIPA
|
|
Aorta
|
225 (37.5%)
|
181 (30.1%)
|
|
Celiac artery
|
177 (29.5%)
|
278 (46.3%)
|
|
Right renal artery
|
59 (9.8%)
|
0
|
|
Left renal artery
|
0
|
7 (1.1%)
|
|
Left gastric artery
|
9 (1.5%)
|
0
|
|
Common hepatic artery
|
1 (0.2%)
|
0
|
|
Splenic artery
|
0
|
6 (1.0%)
|
|
SMA
|
1 (0.2%)
|
0
|
It is essential to understand the embryological development of IPA to appreciate the
anatomical logic behind the variations of IPA origin. Various theories have been proposed
to explain the variations in IPA origin. Three groups of branches arise from the primitive
dorsal aortae: the ventral, dorsal, and dorsolateral groups. Most of the primitive
branches disappear and the ventral splanchnic arteries persist as a celiac artery,
SMA, and inferior mesenteric artery to supply the foregut, midgut, and hindgut structures,
respectively. The lateral splanchnic arteries persist as renal, suprarenal, phrenic,
and gonadal arteries and supply the structures from intermediate mesoderm. The dorsolateral
group of arteries persists as intercostal and lumbar arteries. According to “Felix’s
ladder theory,” IPAs are said to be formed by the cranial group of lateral splanchnic
arteries called “Rete arteriosus Urogenitale,” which can explain the variations in
origin between other lateral branches like renal and gonadal arteries.[14] However, this theory does not explain IPA origin from celiac artery and a common
trunk of origin from the abdominal aorta which is observed in majority of the patients.
During fetal development, most primitive arteries from the ventral, lateral, and dorsal
group disappear. The persistence of longitudinal channels between these ventral, lateral,
and dorsal primitive vessels could explain the fact that IPAs can originate from the
celiac artery and aorta with common truncus.[15] According to another theory proposed by Isogai et al, the adrenal primordium (cranial
half of paraaortic ridge) is supplied by few branches from the gonadal artery and/or
abdominal aorta, during day 14 of embryonic life. The most cranial part of these adrenal
arteries, which are the prospective IPAs, establishes their definitive branching pattern
of the adult by day 15.[16] This theory provides an explanation for the celiac origin of IPA as well as its
origin as a common trunk from the aorta.
Knowing the origins of IPA is useful in various clinical scenarios. TACE is an important
treatment option for unresectable HCC. It improves the prognosis of the patient by
local tumor control and serves as a bridging procedure prior to a liver transplant.[17] HCCs are mainly supplied by hepatic arterial branches. However, depending on the
size and location, it can recruit extrahepatic collateral blood supply. Identifying
these collateral arteries and targeting them is important to achieve complete embolization.
RIPA is the most common extrahepatic artery supplying the HCCs, especially the ones
located in the peripheral posterior segments of the right lobe and near the bare area
of the liver.[7] Prior to TACE, a detailed analysis of the arterial supply to the tumor is needed
to achieve effective embolization. Visualization of the distal ascending portion of
the IPA near the liver surface on CT may be an indicator of the extrahepatic supply
of HCC by IPA.[18] This warrants an IPA angiogram during TACE. IPAs are involved in transpleural systemic-pulmonary
artery anastomosis. In inflammatory lower lung pathologies, there is a compensatory
increase in the systemic circulation, which may result in rupture of these systemic
communications and hemoptysis.[2]
[3]
[19] Occasionally, IPAs might be the only source of hemoptysis, especially in lower lobe
lung pathologies. Hence, locating the IPA and treating it becomes critical for patient
management. IPA may be the source of bleeding secondary to diaphragmatic or hepatic
trauma or post liver transplant procedure due to inadequate ligation.[4]
[20] LIPA is involved in anastomosis with the left anterior descending coronary artery,
which may be of importance in patients with atherosclerotic ischemic heart diseases.[21] LIPA supplies gastroesophageal junction and could be a source of bleed in post-gastrectomy
patients (especially if IPA arises from the LGA).[5]
[6]
[22] LIPA is involved in the anastomosis with pericardiophrenic arteries and may be a
source of traumatic pericardial tamponade, which can be managed effectively by LIPA
embolization.[21]
Having a thorough knowledge of the vascular anatomy and being familiar with variations
of IPA help to bail out the interventional radiologists from difficult situations
faced on day-to-day basis. IPA should be an inherent part of the checklist while reporting
or doing an interventional procedure in that region.
Our study had a few limitations. First is the retrospective nature of the study and
second is the lack of confirmation of the variations detected on CTA images with DSA.
We did not obtain DSA images of the patients as it was not indicated.
Conclusion
MDCT demonstrates the IPA origins very well, enabling planning of interventional procedures
related to IPA. Without common trunk, RIPA most commonly originates from aorta and
LIPA from the celiac artery. IPAs with common trunk most commonly originate from aorta.
Being familiar with the variations of IPA origins is of great clinical relevance.






