

Subscribe to RSS
DOI: 10.1055/s-0039-1688924
Otobone®: Three-dimensional printed Temporal Bone Biomodel for Simulation of Surgical Procedures
Authors
Address for correspondence
Publication History
27 February 2019
31 March 2019
Publication Date:
31 May 2019 (online)


Abstract
Introduction The anatomy of the temporal bone is complex due to the large number of structures and functions grouped in this small bone space, which do not exist in any other region in the human body. With the difficulty of obtaining anatomical parts and the increasing number of ear, nose and throat (ENT) doctors, there was a need to create alternatives as real as possible for training otologic surgeons.
Objective Developing a technique to produce temporal bone models that allow them to maintain the external and internal anatomical features faithful to the natural bone.
Methods For this study, we used a computed tomography (CT) scan of the temporal bones of a 30-year-old male patient, with no structural morphological changes or any other pathology detected in the examination, which was later sent to a 3D printer in order to produce a temporal bone biomodel.
Results After dissection, the lead author evaluated the plasticity of the part and its similarity in drilling a natural bone as grade “4” on a scale of 0 to 5, in which 5 is the closest to the natural bone and 0 the farthest from the natural bone. All structures proposed in the method were found with the proposed color.
Conclusion It is concluded that it is feasible to use biomodels in surgical training of specialist doctors. After dissection of the bone biomodel, it was possible to find the anatomical structures proposed, and to reproduce the surgical approaches most used in surgical practice and training implants.
Introduction
The anatomy of the temporal bone is complex because of the several structures and functions present in this small bone space, which do not exist in any other region in the human body. For this reason, theoretical knowledge, along with the practical study of corpses, must be acquired to understand its structure.[1] [2]
Interest in non-cadaveric representations of the temporal bone for dissection and learning has increased, since access to cadaver body parts is increasingly restricted, and, in some parts of the world, they are difficult to obtain because of legislative, religious, or cultural reasons.[3] [4]
In the mid-1980s, the studies on stereolithography began. After a rapid evolution in these studies, the three-dimensional (3D) printer emerged; its main function was to manufacture parts for the automotive industry and to produce prototypes. Thus, testing to create the tools used in the production line commenced immediately. Since then, chocolate, pens, toys, and even spacesuits have been produced using this equipment. In the last decade, interest in this technology increased considerably in the health sector, with subsequent investment in the field.[1] [4] [5]
To improve studies on the temporal bone, and in view of its shortage in the dissection laboratory and the need for training young and experienced surgeons, the objectives of this study were:
-
To develop a technique for producing temporal bone models that maintain external and internal anatomical features identical to the natural bone in terms of density of material, plasticity, and color.
-
To reproduce in this biomodel the main anatomical structures of a natural temporal bone.
-
To reproduce the main surgical approaches to the mastoid.
Methods
This study was conducted at the Surgical Skills Laboratory of Otolaryngology, at the Faculty of Medicine, University of São Paulo.
For this study, we used a computed tomography (CT) scan of the temporal bones of a 30-year-old male patient, with no structural morphological changes or any other pathology detected during examination. The CT scan was performed using the Aquilion CXL 128 multislice CT scanner with 128 rows of detectors (Toshiba, Minato, Tokyo, Japan). Axial sections were acquired using the parameters of 120 kV and 250 mA, and opting for a reconstruction algorithm with a section thickness of 0.3 mm and field of view (FOV) directed to the left temporal bone.
Digital Imaging and Communications in Medicine (DICOM) files were imported from the InVesalius 3.0.0 software (Centro de Tecnologia da Informação Renato Archer, Campinas, SP, Brazil), which contained detailed segmentation of the regions of interest to be represented in the 3D model, and a .STL file (file format for 3D printing) was generated, representing the mastoid and all its internal details.
The final .STL file was sent to a ProJet CJP 660 Pro model 3D printer (3D Systems, Rock Hill, SC, USA) with color jet printing technology .
The material used for printing was a high yield compound with gypsum powder, sandstone, and specific binder as the base. The bone was printed in parts and subsequently welded. Blue synthetic rubber material, used to simulate the dura mater, was applied on the projection surface of the medial and posterior cranial fossae in the temporal bone. The product was submitted for patent registration with INPI (filed under number BR 10 2015 032213 5) and for trademark registration (filed under number 910502730), and was named Otobone®.
The internal structures of the carotid, jugular, and facial nerves were printed in red, blue, and yellow colors, respectively.
Five biomodels were printed and dissected by the lead author (who has 35 years of experience in administering courses on temporal bone dissection in cadaveric parts) to evaluate the plasticity of the dissected parts and to find the main anatomical structures of the temporal bone customarily used in temporal bone courses as repair points:
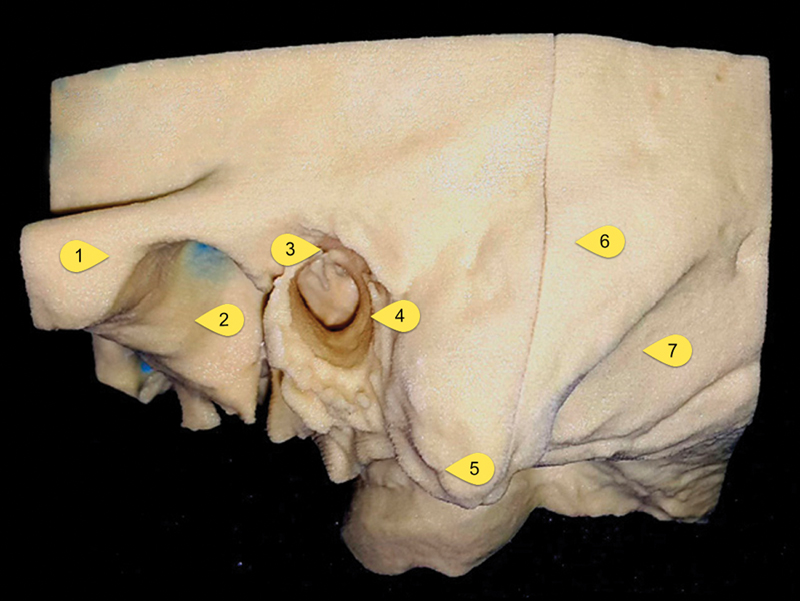
External or Lateral Surface ([Fig. 1])
-
□ zygomatic process
-
□ styloid process
-
□ glenoid cavity
-
□ tympanic bone
Posterior or Medial Surface
-
□ internal auditory meatus
-
□ dura mater of middle and posterior fossa
Ceiling or Superior Surface ([Fig. 2])
-
□ petrous crest
-
□ arcuata or arcuate eminence (projection of the superior semicircular canal in the middle fossa floor)

Base or Inferior Surface ([Fig. 3])
-
□ stylomastoid foramen, where the facial nerve emerges in the soft tissues of the neck (yellow-stained nerve)
-
□ insertion of the digastric muscle on the mastoid
-
□ mandibular fossa, where the temporomandibular joint is joined
-
□ zygomatic process before
-
□ jugular fossa
-
□ carotid canal
-
□ Jacobson channel hole (lower tympanic nerve—IX pair branch)
-
□ petrotympanic suture
-
□ passage hole of the chorda tympani nerve (canal of Huguier)
-
□ petrous apex
-
□ carotid canal
-
□ auditory tube isthmus

Dissection was performed with the same surgical instruments used in ear surgery ([Fig. 4]), Bento’s temporal bone support ([Fig. 5]) (developed at the ENT skills laboratory of FMUSP) ([Fig. 6]), Volvere VMAX high-speed motor (NSK Ltd, Shinagawa, Tokyo, Japan), 1:1 angle pen Kavo (Biberach, Baden-Württemberg, Germany) straight and angled pen, carbon drills with 5, 4, 3, 2 and 1 mm bits (Acumed, Hillsboro, OR, USA), and Zeiss surgical microscope OPMI countertop model (ZEISS, Jena, Thüringen, Germany). During dissection, a Schulz air compressor, Jet Air model (Schulz, São Paulo, Brazil), was used to disperse the particles of the material drilled in the model ([Fig. 7]).




Results
After dissection, the lead author evaluated the plasticity of the workpiece and its similarity to the drilling of a natural bone. A grade of “4” on a scale of 0 to 5 was assigned to the workpiece, with 5 being the closest to the natural bone and 0 the furthest from the natural bone. All structures proposed in the method were found, including the proposed color.
It was also observed that, with this model, it was possible to simulate surgical techniques such as mastoidectomy (open or closed), posterior tympanostomy, facial nerve decompression, cochleostomy and electrode insertion for cochlear implants, viewing of the jugular and carotid gulfs, labyrinthectomy, and access to the internal auditory meatus.
Discussion
The temporal bone produced based on CT scan data using 3D printing technology is a major milestone in the teaching and learning of the complex anatomy of the human temporal bone. Fundamental structures for dissection, such as the hammer, incus, cochlea, oval window, round window, promontory, semicircular canals, and facial nerve canal, are identifiable in the developed part, in addition to the others listed in the method.
Furthermore, it is possible to perform simple and complex surgical procedures, such as cochleostomy training and insertion of cochlear implants ([Fig. 8]).

The interaction between the bone cortex, mastoid aerated cells, and mastoid antrum, during the procedure, realistically reproduces the mechanical properties, texture, and resistance, similar to the same procedure in the cadaveric bone.[6]
With this model, we can improve the training of resident doctors in temporal bone surgical procedures in a similar manner to traditional training with cadaveric bone, but with advantages such as overcoming the constraints imposed by the unavailability of parts for students, eliminating biological hazards inherent in the handling of organic tissues (contamination with the hepatitis C virus, for example), and the possibility of producing mastoid samples that represent not only the normal anatomy, but anatomical variants and structural pathologies, based only on the availability of such samples in a CT file. For beginners, the part is useful for learning, since its main structures are colored, which allows the user to be sure where the structures. Providing them with a 3-D view of anatomical structures when they practice with a natural bone part.[1] [7]
With this technology, it is possible to customize the temporal bone for a particular patient, allowing the surgeon to practice the procedure to be performed and to familiarize himself with what he may find in the actual surgery.
This report is the starting point of a series of studies that will quantitatively assess the benefits of this type of bone simulators in the training of doctors in otorhinolaryngology and the simulation of pathological bones to predict surgical situations.
Conclusions
-
The obtained temporal bone biomodel was very similar to the natural bone.
-
It was possible to find the proposed anatomical structures.
-
It was possible to reproduce surgical approaches frequently used in surgical practice.
-
It is feasible to use biomodels for the surgical training of specialist doctors.
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
References
- 1 Pflesser B, Petersik A, Tiede U, Höhne KH, Leuwer R. Volume cutting for virtual petrous bone surgery. Comput Aided Surg 2002; 7 (02) 74-83
- 2 Webb PA. A review of rapid prototyping (RP) techniques in the medical and biomedical sector. J Med Eng Technol 2000; 24 (04) 149-153
- 3 Wiet GJ, Bryan J, Dodson E. , et al. Virtual temporal bone dissection simulation. Stud Health Technol Inform 2000; 70: 378-384
- 4 Suzuki M, Ogawa Y, Kawano A, Hagiwara A, Yamaguchi H, Ono H. Rapid prototyping of temporal bone for surgical training and medical education. Acta Otolaryngol 2004; 124 (04) 400-402
- 5 Lorensen WE, Cline HE. Marching Cubes: a high resolution 3D surface construction algorithm. Comput Graph 1987; 21: 163-169
- 6 Hochman JB, Kraut J, Kazmerik K, Unger BJ. Generation of a 3D printed temporal bone model with internal fidelity and validation of the mechanical construct. Otolaryngol Head Neck Surg 2014; 150 (03) 448-454
- 7 Pettigrew AM. . Pettigrew temporal bones. Available at: http://www.temporal-bone.com . Accessed Feb 27, 2019
Address for correspondence
-
References
- 1 Pflesser B, Petersik A, Tiede U, Höhne KH, Leuwer R. Volume cutting for virtual petrous bone surgery. Comput Aided Surg 2002; 7 (02) 74-83
- 2 Webb PA. A review of rapid prototyping (RP) techniques in the medical and biomedical sector. J Med Eng Technol 2000; 24 (04) 149-153
- 3 Wiet GJ, Bryan J, Dodson E. , et al. Virtual temporal bone dissection simulation. Stud Health Technol Inform 2000; 70: 378-384
- 4 Suzuki M, Ogawa Y, Kawano A, Hagiwara A, Yamaguchi H, Ono H. Rapid prototyping of temporal bone for surgical training and medical education. Acta Otolaryngol 2004; 124 (04) 400-402
- 5 Lorensen WE, Cline HE. Marching Cubes: a high resolution 3D surface construction algorithm. Comput Graph 1987; 21: 163-169
- 6 Hochman JB, Kraut J, Kazmerik K, Unger BJ. Generation of a 3D printed temporal bone model with internal fidelity and validation of the mechanical construct. Otolaryngol Head Neck Surg 2014; 150 (03) 448-454
- 7 Pettigrew AM. . Pettigrew temporal bones. Available at: http://www.temporal-bone.com . Accessed Feb 27, 2019