

Subscribe to RSS
DOI: 10.1055/s-0036-1580613
Adaptation and Assessment of Reliability and Validity of the Greek Version of the Ohkuma Questionnaire for Dysphagia Screening
Authors
Address for correspondence
Publication History
25 June 2015
01 February 2016
Publication Date:
04 May 2016 (online)


Abstract
Introduction The Ohkuma questionnaire is a validated screening tool originally used to detect dysphagia among patients hospitalized in Japanese nursing facilities.
Objective The purpose of this study is to evaluate the reliability and validity of the adapted Greek version of the Ohkuma questionnaire.
Methods Following the steps for cross-cultural adaptation, we delivered the validated Ohkuma questionnaire to 70 patients (53 men, 17 women) who were either suffering from dysphagia or not. All of them completed the questionnaire a second time within a month. For all of them, we performed a bedside and VFSS study of dysphagia and asked participants to undergo a second VFSS screening, with the exception of nine individuals. Statistical analysis included measurement of internal consistency with Cronbach's α coefficient, reliability with Cohen's Kappa, Pearson's correlation coefficient and construct validity with categorical components, and One-Way Anova test.
Results According to Cronbach's α coefficient (0.976) for total score, there was high internal consistency for the Ohkuma Dysphagia questionnaire. Test-retest reliability (Cohen's Kappa) ranged from 0.586 to 1.00, exhibiting acceptable stability. We also estimated the Pearson's correlation coefficient for the test-retest total score, which reached high levels (0.952; p = 0.000). The One-Way Anova test in the two measurement times showed statistically significant correlation in both measurements (p = 0.02 and p = 0.016).
Conclusion The adapted Greek version of the questionnaire is valid and reliable and can be used for the screening of dysphagia in the Greek-speaking patients.
Introduction
The most comprehensive definition of dysphagia includes abnormalities in all the behavioral, sensory, and preliminary motor functions that are engaged in swallowing as well as the cognitive awareness, visual recognition of food, and the physiologic responses to the presence of food, such as increased salivation which leads to the desire and the patients' ability to feed themselves.[1] Moreover, it is a common multidimensional symptom heavily contingent on morbidity, mortality, and cost.[2]
Disability questionnaires are increasingly used as screening tools so that they will be correlated with the clinical findings, taken from the bedside examination and the clinical examination. A quantitative screening tool of dysphagia in the form of questionnaire may provide physicians with one approach for identifying individuals at risk for dysphagia.[3]
The Ohkuma questionnaire is a validated screening tool used in the detection of dysphagia among patients hospitalized in Japanese nursing homes.[4] [5] The Ohkuma questionnaire's underlying principle is the possibility to safely assess the stage of dysphagia within fifteen questions in a short period of time. It provides a comprehensive means of accurately diagnosing the presence and severity of dysphagia in patients following neurovascular disease.
The purpose of this study is to evaluate the reliability and validity of the adapted Greek version of the Ohkuma Questionnaire in potentially dysphagic patients.
Methods
This study was conducted between Autumn 2012 and Winter 2013 at the Physical Medicine and Rehabilitation Clinic, of the University Hospital of Ioannina, Greece. All patients suffering from dysphagia following cervical spine disorders,[6] brain lesions, and other allied diseases were hospitalized in the rehabilitation clinic. Based on the Ohkuma questionnaire, during the first measurement there were 39 patients suffering from dysphagia and 31 patients irrespective of dysphagia. We examined the patients' cognitive condition once upon admission to the rehabilitation clinic, prior to all other forms of evaluation using the Mini Mental State Examination (M.M.S.E.) and all patients included were capable of responding to the questions uninhibited and without external help.
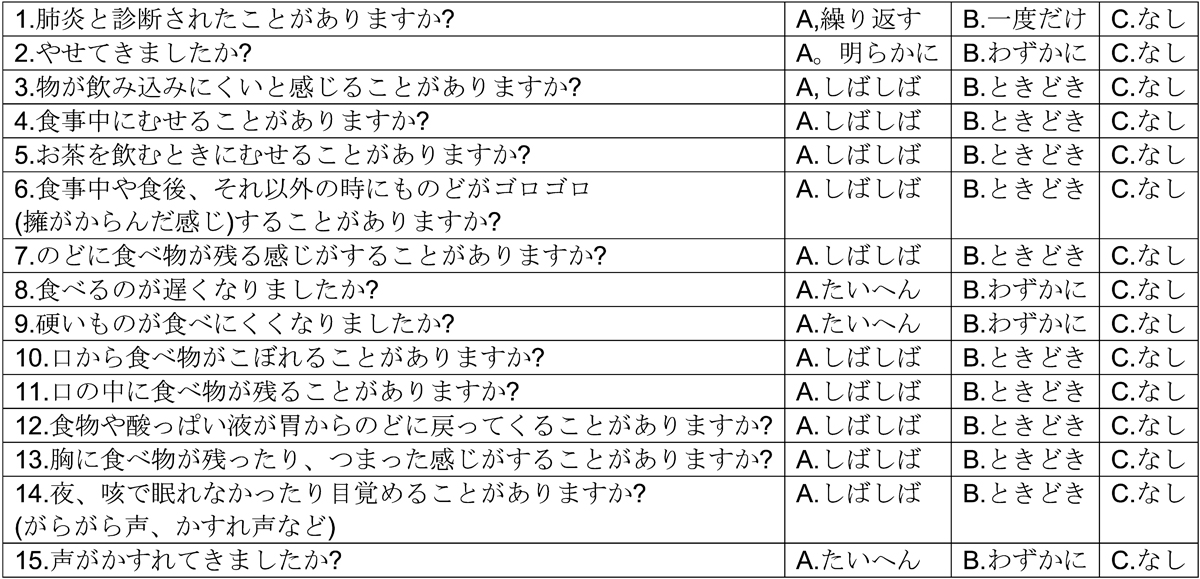
Translation of the Japanese version of the Ohkuma questionnaire into Greek and back translation to Japanese was performed by two individuals, both native speakers of Greek and highly proficient in the Japanese language. Both versions of the translation were placed under the supervision of a MD Professor at the University Hospital that is well-knowledgeable and speaks both the Greek and Japanese languages. The final translation was fixed by consensus at the final stage of the cross-cultural adaptation. All those involved in the translation and adaptation process were experts at dysphagia. An English translation from the Greek version of Ohkuma questionnaire was also performed and compared with the English Ohkuma questionnaire published by Kawashima ([Table 1]).[4]
Following Institutional Review Board (IRB) approval, the final version of the Greek Ohkuma questionnaire was given to a total of 149 patients and was later reduced to several 70 patients (53 men and 17 women) ([Fig. 1]). They were excluded because they did not meet the inclusion criteria, either because they were suffering from other ailments not consistent with the research or because they were healthy. Some of the patients who were included in the study had already been diagnosed with dysphagia where as others showed clinical indications of the symptom, under the supervision of a speech pathology team. All of them were graduates of secondary education. The mean age of the participants was 51.17 years old (SD 14.235), both male and female, and all patients signed a written consent to participate in the study.

We collected the medical records of all the patients who participated in the administration of the questionnaire to form a complete database as the clinical history record. The exclusion criteria applied to patients whose cognitive status was not deemed to be equal to the task as they could not communicate, understand, and interact, as was the case for those with psychiatric problems or unwilling to participate in the study. All patients scored between 27 and 30 in the administration of the MMSE.
The questions were clear-cut and easy to understand; therefore, there were no comprehension problems or unanswered questions. All patients were asked to complete the fifteen questions of the questionnaire by selecting one of the three given choices. Severe symptoms were rated with 1, mild symptoms with 2, and absence of symptoms with 3. The total score was based on the sum of the answers and the mean value was 45. If the patient ticked the severe box at least once, he was considered as having dysphagia. Those who did not experience severe symptoms were classified as non-dysphagic adults.[4]
The time allowed to complete the questionnaire was restricted to 8–10 minutes after all the necessary clarifications had been concluded. The time was narrowed down to 5–7 minutes when the same population answered the questionnaire again, after exactly 4 weeks. Nine of the participants were unavailable for the second administration of the VFSS, seven because of complications that arose at a later time, and two because they had died. After completing the questionnaire for the first time, the speech-language therapist (SLT), blinded to questionnaire results, assessed each patient for the presence or not of dysphagia (by a bed-side clinical examination including swallowing reflexes).
Upon admission and after the medical diagnosis, we collected information regarding the patient's medical history, pertinent medication, current method of nutrition, duration of swallowing problems, and pulmonary function.[7] All patients underwent bedside clinical examination. This mainly assessed the patient's cognitive ability, communication skills, oropharyngeal and laryngeal anatomy, swallowing reflexes, and respiratory status. The cognitive status was examined with the administration of the Mini Mental State Examination once after admission to the rehabilitation clinic. The oropharyngeal function/anatomy was checked by instructing the patients to perform certain movements of the structures that engage in the process of swallowing. We used the 3-ounce water test to screen for the risk for aspiration pneumonia.[6] [8] Finally, we placed the oximeter probe in the patients' index to record oxygen saturation (≥ 2%) while they swallowed food of varying consistencies.[9]
The oropharyngeal and oesophageal stages of swallowing were tested with the VFSS study by instructing the patients to ingest barium coated boluses or liquid barium of varying consistencies and quantities. A trained radiologist radiologically recorded the passage of the material and analyzed it. Through this exam, the physician was able to collect information about the structural and functional disabilities of the anatomic structures that are engaged in the swallowing process.[10]
We assessed the reliability of the Greek Version of the Ohkuma questionnaire with the Cronbach's α coefficient. We examined test-retest reliability with the use of Cohen's Kappa coefficient for each of the 15 items of the questionnaire and by computing the Pearsońs correlation coefficient for the total score. We evaluated construct validity through categorical principal components analysis using variable principal normalization. We then performed statistical analyses using S.P.S.S, version 20. Results with p-values < 0.05 were considered statistically significant.
As Kawashima et al[4] reported, we regarded the presence of at least one severe symptom as indicating dysphagia and, thus, it is possible to assess the risk of dysphagia even if a patient did not give positive answers to all severe symptoms. The patients with positive answers in moderate symptoms were considered suspicious dysphagic but they were pooled with the non-dysphagic (only mild symptoms in all questions) since this is a screening questionnaire for the presence of dysphagia or not. The number of severe symptoms observed for each patient was considered indicative of their dysphagia severity.
Results
The questionnaire was answered for the first time by a total number of 70 participants and everyone answered all items since they were all secondary education graduates. The distribution of responses in each of the 15 items of the questionnaire is shown in [Table 2]. Based on at least one severe symptom response of the Ohkuma questionnaire, 55.7% of the participants were screened as dysphagic patients while the remaining 44.3% were found with normal swallowing. After the second administration the percentages of patients with dysphagia decreased to 42.9%.
The reliability of the questionnaire calculated by the Cronbach's α coefficient was 0.976 for total score, 0.878 for the first questionnaire, and 0.892 for the second questionnaire, showing high internal consistency. Test-retest reliability as assessed through Pearson correlation coefficient for the total score was 0.952 (p = 0.000) and the Cohen's Kappa coefficient for each item ranged from 0.586 to 1.00, showing at least acceptable stability for the all items ([Tables 3] [4] [5] [6] [7]). To investigate a possible correlation between the VFSS study and the Ohkuma questionnaire, the One-Way Anova test was used in both measurement times. We found a statistically significant correlation both during the first evaluation (p = 0.02 < 0.05) ([Table 8]) and the second (p = 0.016 < 0.05) ([Table 9]).
** Correlation is significant at the 0.01 level (2-tailed).
|
Reliability Statistics |
||
|---|---|---|
|
Cronbach's Alpha |
Cronbach's Alpha Based on Standardized Items |
N of Items |
|
0.976 |
0.976 |
2 |
|
ANOVA |
|||||
|---|---|---|---|---|---|
|
OHKUMA.1 |
|||||
|
Sum of Squares |
df |
Mean Square |
F |
Sig. |
|
|
Between Groups |
291.324 |
2 |
145.662 |
4.161 |
0.020 |
|
Within Groups |
2345.376 |
67 |
35.006 |
||
|
Total |
2636.700 |
69 |
|||
Abbreviations: df, degrees of freedom; F, F test; Sig, significance.
|
ANOVA |
|||||
|---|---|---|---|---|---|
|
OHKUMA.2 |
|||||
|
Sum of Squares |
df |
Mean Square |
F |
Sig. |
|
|
Between Groups |
312.140 |
2 |
156.070 |
4.442 |
0.016 |
|
Within Groups |
2037.794 |
58 |
35.134 |
||
|
Total |
2349.934 |
60 |
|||
Abbreviations: df, degrees of freedom; F, F test; Sig, significance.
Discussion
The administration of the Ohkuma questionnaire was conducted with the aim of establishing a screening tool in Greek speaking patients suffering from dysphagia or not. This questionnaire had already been translated into the Italian and English language following cross cultural adaptation, which constitutes the linguistic validation of an instrument.
Severely dysphagic patients often complain that their quality of life has been heavily impaired due to their condition. Many questionnaires, such as the MD Anderson Dysphagia Inventory, which are used to evaluate the impact of dysphagia on the quality of life, and SWAL-QOL and SWAL-CARE, which gather qualitative data to patients who have already been diagnosed with dysphagia, have been implemented to measure such inhibitions.[11] Nonetheless, the Ohkuma questionnaire is instrumental in detecting dysphagia, although it does not provide an index on quality of life.
The most important screening tool in the evaluation of dysphagia and as a result of the planning of the therapeutic process is a questionnaire of proven reliability and validity in different cultures and languages so as to assess the presence of dysphagia. The difficulty that arises in establishing construct validity of a screening tool is that there is at present no single conclusive screening tool. Bed side examination is easy to use, but provides low sensitivity and specificity in detecting dysphagia.[12] Videofluoroscopy study is considered a reliable measurement tool at the physicians' disposal with the aim of establishing and evaluating the mechanical consequences of oral-pharyngeal dysphagia so as to determine the structural and functional deficiency of the anatomical formations.[6] [13] [14] [15] McCullough et al found that videofluoroscopy study not so much determined as supported Clinical Swallowing Examination (CSE) findings.[6] On the other hand, Terre & Mearin concluded that, in 90% of the cases, VFSS study was instrumental in evaluating these patients.[16] Bours et al found that a water test combined with pulse oximetry was the best method to screen patients with neurovascular disorders for dysphagia.[17] In this study even though the questionnaire's validity was not examined with the results of the videofluoroscopic study, we had clinical impression of their deglutition state by the bed-side examination.[17]
There are other validated dysphagia questionnaires that target different patient groups. The Mayo Dysphagia Questionnaire focuses mainly on esophageal dysphagia and offers a broad assessment of dysphagia covering aspects of dysphagia onset, frequency, and severity and was validated with the standard physician's interview.[18] The Sydney Swallow Questionnaire was validated in head and neck cancer patients and can only show a quantification of dysphagia,[3] offering an evaluation of swallowing difficulties in neuromyogenic, oropharyngeal dysphagia.
Belafsky et al with the 10-item Eating Assessment tool (Eat-10) found that subjective dysphagia symptoms can predict aspiration risk.[19]
The reason that the Ohkuma questionnaire was chosen is that it is brief, accurate, and easy to understand, thus it is friendlier to patients. Moreover, the questions contain all the basic indications of dysphagic patients and apply to all the stages of swallowing.
In addition to determining the frequency and duration of dysphagia,[14] the Ohkuma questionnaire helps clinicians to prevent secondary complications like aspiration pneumonia, as in patients severely affected by dysphagia, for which a thorough diagnostic examination was required before initiating therapeutic intervention methods. The main goals of the study were to distinguish dysphagic patients from normal ones; therefore, upon the completion of the questionnaire, it was evident to which category each patient belonged.
Unlike the water-swallowing test,[15] the dysphagia questionnaire does not carry a risk of aspiration. Considering all its advantages, the dysphagia questionnaire is a useful tool for determining the prevalence of dysphagia among Greek patients. The severity of dysphagia was significantly related to the level of competence. However, all of our patients were evaluated psychologically and cognitively and were found to be capable of self-response. On the other hand, the main feature of already existing questionnaires is that they are difficult to use and have been mostly designed bearing in mind patients suffering from neurological or malignant diseases in the neck region.[20]
Kawashima et al, from an elderly hospice-set population, reported dysphagia prevalence 13.8% and high reliability (Cronbach-a coefficient = 0.83).[4] Nalesso et al, in a study of Italian stroke patients, reported a great percentage of dysphagic patients (74.5%), although no reliability study was performed.[21] In this prospective study, the results showed that those patients who were under the suspicion of dysphagia were shown to have dysphagia after the administration of the questionnaire. Out of the total number of the participants, 58.5% were documented as having some inability in swallowing.[22] Our results of Ohkuma questionnaire's reliability in Greek population with 58.5% of questionnaire-confirmed dysphagia are comparable to Kawashima's (0.896). Our results show high reliability, rendering the Greek version of the Ohkuma questionnaire a reliable way to detect dysphagia in patients suffering from neurovascular diseases.
It should also be noted, though, that the dysphagia factors reported in Kawashima et al (Factor 1 related to oral and esophageal functions, Factor 2 to pharyngeal functions, Factor 3 to oral digestion, Factor 4 to airway protective function, and Factor 5 to pneumonia history) are not verified through any gold standard study (e.g., the VFSS), allowing for the possibility of a different outcome interpretation. Kawashima et al considered the dysphagia screening questionnaire to be useful for evaluating six factors: Item 1, past history of pneumonia; Item 2, nutritional state; Items 3–7 pharyngeal function; Items 8–11, oral function; Items 12–14, esophageal function; and Item 15, airway protective function. In the study of Nalesso et al., discrimination within the 15 items was only attempted on theoretical rather than statistical grounds.[21]
In our study, construct validity as examined through categorical principal components analysis showed three major factors. The first one, consisting of most items (excluding 1 and 12) accounts for 42.8% of the total variance observed ([Table 2]). The other two account for 8.6% and 7.5% of the total variance respectively. Categorization is quite clear according to the factor loadings reported. The two items comprising the two separate factors are 1 and 12. These two seem to describe “pneumonia” and “feeling of food or liquid going up into the throat from the stomach” as two different causes of dysphagia and, therefore, are discriminated in the analysis results from the rest of the items which refer to other causes of dysphagia. This result is not in accordance with the results reported by Kawashima, where different dysphagia categories derive using the principal components analysis. This discrepancy could be due to the different statistical approach adopted and to the fact that item 9 was excluded from the analysis and the items analyzed were, therefore, 14 in the Kawashima study.
The limitation to this study is the absence of a gold standard test to confirm the diagnostic accuracy of the Greek translation of Ohkuma questionnaire. However, the accuracy of this questionnaire has been shown in the Japanese population and our results showed that the questionnaire was effective in screening dysphagic symptoms in Greek speaking patients. A study to measure the sensitivity and specificity of Ohkuma questionnaire is under construction.
Conclusion
Our statistical results have confirmed that the adapted Greek version of the Ohkuma questionnaire is valid and reliable and covers a wide range of patients' perceived outcomes. The Ohkuma questionnaire is felt to be a useful tool in the screening process of dysphagic patients mainly due to the fact that it is easy to administer and does not pose any problems to the patients who can answer all the questions uninhibited and without any extra help. Moreover, as there are no such questionnaires available in Greece the validation of the Ohkuma questionnaire could be implemented to screen dysphagia and facilitate course of treatment.
-
References
- 1 Leopold NA, Kagel MC. Prepharyngeal dysphagia in Parkinson's disease. Dysphagia 1996; 11 (1) 14-22
- 2 Wallace KL, Middleton S, Cook IJ. Development and validation of a self-report symptom inventory to assess the severity of oral-pharyngeal dysphagia. Gastroenterology 2000; 118 (4) 678-687
- 3 Dwivedi RC, St Rose S, Chisholm EJ , et al. Evaluation of swallowing by Sydney Swallow Questionnaire (SSQ) in oral and oropharyngeal cancer patients treated with primary surgery. Dysphagia 2012; 27 (4) 491-497
- 4 Kawashima K, Motohashi Y, Fujishima I. Prevalence of dysphagia among community-dwelling elderly individuals as estimated using a questionnaire for dysphagia screening. Dysphagia 2004; 19 (4) 266-271
- 5 Ohkuma RFI, Kojima C, Hojo K, Takehara I, Motohashi Y. Development of a questionnaire to screen dysphagia. Jpn J Dysphagia Rehabilitation 2002; 6: 3-8
- 6 Menezes AH. Craniovertebral junction database analysis: incidence, classification, presentation, and treatment algorithms. Childs Nerv Syst 2008; 24 (10) 1101-1108
- 7 Rosenbek JC, Robbins JA, Roecker EB, Coyle JL, Wood JL. A penetration-aspiration scale. Dysphagia 1996; 11 (2) 93-98
- 8 Turner-Lawrence DE, Peebles M, Price MF, Singh SJ, Asimos AW. A feasibility study of the sensitivity of emergency physician Dysphagia screening in acute stroke patients. Ann Emerg Med 2009; 54 (3) 344-348 , 348.e1
- 9 Smith HA, Lee SH, O'Neill PA, Connolly MJ. The combination of bedside swallowing assessment and oxygen saturation monitoring of swallowing in acute stroke: a safe and humane screening tool. Age Ageing 2000; 29 (6) 495-499
- 10 Rogus-Pulia NM, Pierce M, Mittal BB, Zecker SG, Logemann J. Bolus effects on patient awareness of swallowing difficulty and swallow physiology after chemoradiation for head and neck cancer. Head Neck 2015; 37 (8) 1122-1129
- 11 Chen AY, Frankowski R, Bishop-Leone J , et al. The development and validation of a dysphagia-specific quality-of-life questionnaire for patients with head and neck cancer: the M. D. Anderson dysphagia inventory. Arch Otolaryngol Head Neck Surg 2001; 127 (7) 870-876
- 12 Shin JC, Yoo JH, Lee YS, Goo HR, Kim DH. Dysphagia in cervical spinal cord injury. Spinal Cord 2011; 49 (9) 1008-1013
- 13 Lim SH, Lieu PK, Phua SY , et al. Accuracy of bedside clinical methods compared with fiberoptic endoscopic examination of swallowing (FEES) in determining the risk of aspiration in acute stroke patients. Dysphagia 2001; 16 (1) 1-6
- 14 McElhiney J, Lohse MR, Arora AS , et al. The Mayo Dysphagia Questionnaire-30: documentation of reliability and validity of a tool for interventional trials in adults with esophageal disease. Dysphagia 2010; 25 (3) 221-230
- 15 Osawa A, Maeshima S, Tanahashi N. Water-swallowing test: screening for aspiration in stroke patients. Cerebrovasc Dis 2013; 35 (3) 276-281
- 16 Terré R, Mearin F. Oropharyngeal dysphagia after the acute phase of stroke: predictors of aspiration. Neurogastroenterol Motil 2006; 18 (3) 200-205
- 17 Bours GJ, Speyer R, Lemmens J, Limburg M, de Wit R. Bedside screening tests vs. videofluoroscopy or fibreoptic endoscopic evaluation of swallowing to detect dysphagia in patients with neurological disorders: systematic review. J Adv Nurs 2009; 65 (3) 477-493
- 18 Grudell AB, Alexander JA, Enders FB , et al. Validation of the Mayo Dysphagia Questionnaire. Dis Esophagus 2007; 20 (3) 202-205
- 19 Cheney DM, Siddiqui MT, Litts JK, Kuhn MA, Belafsky PC. The Ability of the 10-Item Eating Assessment Tool (EAT-10) to Predict Aspiration Risk in Persons With Dysphagia. Ann Otol Rhinol Laryngol 2015; 124 (5) 351-354
- 20 Skeppholm M, Ingebro C, Engström T, Olerud C. The Dysphagia Short Questionnaire: an instrument for evaluation of dysphagia: a validation study with 12 months' follow-up after anterior cervical spine surgery. Spine (Phila Pa 1976) 2012; 37 (11) 996-1002
- 21 Nalesso SSA, Bottacini M Casetta A Il paziente disfagico: studio di prevalenza in due strutture residenziali della terraferma veneziana. Societa Italiana di Gerontologia e Geriatria, 2008: 18-23
- 22 Hilari K, Byng S, Lamping DL, Smith SC. Stroke and Aphasia Quality of Life Scale-39 (SAQOL-39): evaluation of acceptability, reliability, and validity. Stroke 2003; 34 (8) 1944-1950
Address for correspondence
-
References
- 1 Leopold NA, Kagel MC. Prepharyngeal dysphagia in Parkinson's disease. Dysphagia 1996; 11 (1) 14-22
- 2 Wallace KL, Middleton S, Cook IJ. Development and validation of a self-report symptom inventory to assess the severity of oral-pharyngeal dysphagia. Gastroenterology 2000; 118 (4) 678-687
- 3 Dwivedi RC, St Rose S, Chisholm EJ , et al. Evaluation of swallowing by Sydney Swallow Questionnaire (SSQ) in oral and oropharyngeal cancer patients treated with primary surgery. Dysphagia 2012; 27 (4) 491-497
- 4 Kawashima K, Motohashi Y, Fujishima I. Prevalence of dysphagia among community-dwelling elderly individuals as estimated using a questionnaire for dysphagia screening. Dysphagia 2004; 19 (4) 266-271
- 5 Ohkuma RFI, Kojima C, Hojo K, Takehara I, Motohashi Y. Development of a questionnaire to screen dysphagia. Jpn J Dysphagia Rehabilitation 2002; 6: 3-8
- 6 Menezes AH. Craniovertebral junction database analysis: incidence, classification, presentation, and treatment algorithms. Childs Nerv Syst 2008; 24 (10) 1101-1108
- 7 Rosenbek JC, Robbins JA, Roecker EB, Coyle JL, Wood JL. A penetration-aspiration scale. Dysphagia 1996; 11 (2) 93-98
- 8 Turner-Lawrence DE, Peebles M, Price MF, Singh SJ, Asimos AW. A feasibility study of the sensitivity of emergency physician Dysphagia screening in acute stroke patients. Ann Emerg Med 2009; 54 (3) 344-348 , 348.e1
- 9 Smith HA, Lee SH, O'Neill PA, Connolly MJ. The combination of bedside swallowing assessment and oxygen saturation monitoring of swallowing in acute stroke: a safe and humane screening tool. Age Ageing 2000; 29 (6) 495-499
- 10 Rogus-Pulia NM, Pierce M, Mittal BB, Zecker SG, Logemann J. Bolus effects on patient awareness of swallowing difficulty and swallow physiology after chemoradiation for head and neck cancer. Head Neck 2015; 37 (8) 1122-1129
- 11 Chen AY, Frankowski R, Bishop-Leone J , et al. The development and validation of a dysphagia-specific quality-of-life questionnaire for patients with head and neck cancer: the M. D. Anderson dysphagia inventory. Arch Otolaryngol Head Neck Surg 2001; 127 (7) 870-876
- 12 Shin JC, Yoo JH, Lee YS, Goo HR, Kim DH. Dysphagia in cervical spinal cord injury. Spinal Cord 2011; 49 (9) 1008-1013
- 13 Lim SH, Lieu PK, Phua SY , et al. Accuracy of bedside clinical methods compared with fiberoptic endoscopic examination of swallowing (FEES) in determining the risk of aspiration in acute stroke patients. Dysphagia 2001; 16 (1) 1-6
- 14 McElhiney J, Lohse MR, Arora AS , et al. The Mayo Dysphagia Questionnaire-30: documentation of reliability and validity of a tool for interventional trials in adults with esophageal disease. Dysphagia 2010; 25 (3) 221-230
- 15 Osawa A, Maeshima S, Tanahashi N. Water-swallowing test: screening for aspiration in stroke patients. Cerebrovasc Dis 2013; 35 (3) 276-281
- 16 Terré R, Mearin F. Oropharyngeal dysphagia after the acute phase of stroke: predictors of aspiration. Neurogastroenterol Motil 2006; 18 (3) 200-205
- 17 Bours GJ, Speyer R, Lemmens J, Limburg M, de Wit R. Bedside screening tests vs. videofluoroscopy or fibreoptic endoscopic evaluation of swallowing to detect dysphagia in patients with neurological disorders: systematic review. J Adv Nurs 2009; 65 (3) 477-493
- 18 Grudell AB, Alexander JA, Enders FB , et al. Validation of the Mayo Dysphagia Questionnaire. Dis Esophagus 2007; 20 (3) 202-205
- 19 Cheney DM, Siddiqui MT, Litts JK, Kuhn MA, Belafsky PC. The Ability of the 10-Item Eating Assessment Tool (EAT-10) to Predict Aspiration Risk in Persons With Dysphagia. Ann Otol Rhinol Laryngol 2015; 124 (5) 351-354
- 20 Skeppholm M, Ingebro C, Engström T, Olerud C. The Dysphagia Short Questionnaire: an instrument for evaluation of dysphagia: a validation study with 12 months' follow-up after anterior cervical spine surgery. Spine (Phila Pa 1976) 2012; 37 (11) 996-1002
- 21 Nalesso SSA, Bottacini M Casetta A Il paziente disfagico: studio di prevalenza in due strutture residenziali della terraferma veneziana. Societa Italiana di Gerontologia e Geriatria, 2008: 18-23
- 22 Hilari K, Byng S, Lamping DL, Smith SC. Stroke and Aphasia Quality of Life Scale-39 (SAQOL-39): evaluation of acceptability, reliability, and validity. Stroke 2003; 34 (8) 1944-1950