
Subscribe to RSS
DOI: 10.1055/s-0035-1564829
Yolk Sac Tumor of the Temporal Lobe: Case Report
Article in several languages: English | portuguêsAddress for correspondence
Publication History
29 May 2015
31 August 2015
Publication Date:
05 October 2015 (online)


Abstract
Germ cell tumors of the central nervous system (CNS) are usually located along the midline. Yolk sac tumor is a rare germ cell tumor very uncommonly located outside the midline, and, in such cases, it can be mistaken with other primary tumors. We report a case of a 32-year-old male patient who presented with a right temporal lobe tumor suggestive of a high grade glioma. He was submitted to a right temporal lobectomy with complete tumor removal. The histological exam revealed a germ cell tumor (later confirmed to be a yolk sac tumor). The search for a primary tumor outside of the CNS (including a positron emission tomography scan) was negative, making this a primary temporal lobe yolk sac tumor. The patient was submitted to chemotherapy and radiotherapy, but died 7 months after the surgery.
Introduction
Central nervous system (CNS) germ cell tumors account for 2 to 3% of the primary intracranial tumors, and are usually located in the midline (in the pineal or sellar regions).[1] The yolk sac tumor is a relatively rare germ cell tumor.[2] [3] The occurrence of this type of tumor outside the midline is an exception, with very few cases described in the literature.[1] [2] [4] [5] [6] When they occur in atypical locations, they are usually lesions with a cystic component and poor prognosis.[5]
Case Report
A 32-year-old male patient, who sought the emergency department with a headache with 2 weeks of evolution and papillary stasis. No other focal neurological signs were observed.
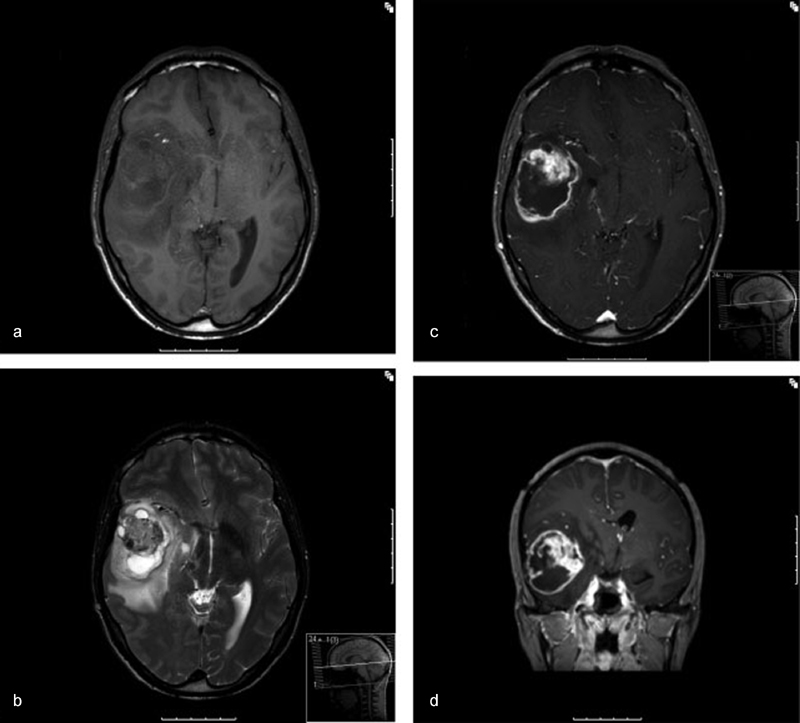
The imaging investigation revealed a right temporal intra-axial lesion with heterogeneous contrast uptake and a cystic/necrotic area ([Fig. 1]). The hypothesis of the diagnosis was high-grade glioma (HGG).
The patient underwent a right frontotemporal craniotomy with a temporal lobectomy encompassing the lesion in its entirety ([Fig. 2]). The lesion had a hard, vascularized consistency, and a cystic area of yellowish content, macroscopically similar to an HGG.

Clinically, the patient improved postoperatively, without headaches or focal deficits.
The neuropathological examination revealed a germ cell tumor forming, in some places, tubular structures composed of cells with prominent nuclei, and numerous mitoses were observed. The immunocytochemical examination was positive for both α-fetoprotein and glypican 3,([Fig. 3]), and negative for glial fibrillary acidic protein (GFAP), human chorionic gonadotropin (HCG), and epithelial markers. In this sense, a systemic investigation including a positron emission tomography (PET) scan was performed to investigate a possible primary tumor (assuming that, from the location of the brain lesion, it would be metastatic). The investigation was negative, and no other tumor was found. The study of the neuraxis also revealed no other lesions.

The patient was directed to four cycles of chemotherapy – ifosfamide + cisplatin + etoposide (ICE), which would be followed by holocranial brain radiotherapy.
At 3 months, during the third cycle of chemotherapy, a magnetic resonance imaging (MRI) exam revealed intracranial meningeal metastases. At this time, the patient remained clinically stable. A decision was made to continue with the fourth cycle of chemotherapy and subsequent radiotherapy. At an MRI exam performed at 5 months, the patient maintained the metastases already known ([Fig. 4]). Three weeks after this examination, already under radiotherapy, there was an important neurological deterioration, revealing a marked growth of metastases in the computerized axial tomography (CAT) scan, as well as new lesions ([Fig. 5]). Due to the lack of response to the treatment, the radiotherapy was discontinued. The patient deteriorated rapidly to a comatose state, dying 3 weeks later, ∼ 7 months after surgery.


Discussion
Germ cell tumors are divided into two major groups: germ cell and non-germ cell tumors (yolk sac tumor, choriocarcinoma, embryonal carcinomas, and teratomas).[7] The latter group has a worse prognosis.[6] [7]
In the presence of a tumor located in the midline, in a child or young adult, the hypothesis of a germ cell tumor should be considered. A search for tumor markers (α-fetoprotein and β-HCG) in the blood and/or in the cerebrospinal fluid (CSF) should be performed.
Germinomas are the most common tumors of this group; and, in this case, the markers are usually negative, and the diagnosis requires histological confirmation through biopsy.[7] Since this type of tumor has an excellent response to radiotherapy, with long-term regression rates of ∼ 90%, excision surgery does not lead to an improvement in the outcome.[7]
On the other hand, the positivity of α-fetoprotein labeling will determine the diagnosis of yolk sac tumor without the need of histological confirmation for therapeutic orientation.[7] In the case described in the present report, this hypothesis was never raised due to the location of the lesion, which is why this study was not performed preoperatively.
The temporal location of a yolk sac tumor is extremely rare. To our knowledge, there are 19 cases reported in the literature[6] [8] on the occurrence of this tumor outside the midline, with only 4 located in the cerebral lobes – the remaining reported cases occurred in the lateral ventricles, in the fourth ventricle, in the thalamus/basal ganglia, in the cerebellum, or in the rachis)[6] [8] ([Table 1]).
|
Site |
Author |
Gender |
Age (years) |
Treatment |
Survival (months) |
|---|---|---|---|---|---|
|
Spine |
Kurisaka et al. |
Female |
1 |
Surgery + CT |
8b |
|
Spine |
Kan et al. |
Female |
25 |
Surgery + RT + CT |
22b |
|
Cerebellum |
Takeda et al. |
Male |
4 |
Surgery + RT |
8a |
|
Cerebellum |
Tajika et al. |
Male |
3 |
Surgery + CT |
4a |
|
Cerebellum |
Tsukamoto et al. |
Male |
3 |
Surgery + RT + CT |
18a |
|
Cerebellum |
Nakase et al. |
Male |
5 |
Surgery + CT |
12a |
|
Cerebellum |
Wada et al. |
Male |
6 |
Surgery + CT |
5b |
|
Cerebellum |
Cheon et al. |
Male |
3 |
Surgery + CT |
48a |
|
Basal ganglia |
Masuzawa et al. |
Male |
10 |
Surgery + RT |
NAb |
|
Basal ganglia |
Oshita et al. |
Female |
8 |
Surgery + RT + CT |
NAb |
|
Basal ganglia |
Wang et al. |
Female |
7 |
Surgery + RT + CT |
NAb |
|
Lateral ventricle |
Murovic et al. |
Female |
2 |
Surgery + RT |
42a |
|
Lateral ventricle |
Tsugu et al. |
Female |
13 |
Surgery + RT + CT |
7b |
|
Fourth ventricle |
Nakagawa et al. |
Male |
18 |
Surgery + RT |
5a |
|
Frontal lobe |
Sugawara et al. |
Female |
18 |
Surgery + RT + CT |
3a |
|
Frontal lobe |
Netalkar et al. |
Female |
15 |
Surgery + CT |
36a |
|
Frontal lobe |
Honda et al. |
Male |
1 |
Surgery + CT |
9b |
|
Middle fossa + orbit |
Dragan et al. |
NA |
15 |
Surgery + CT |
5a |
|
Temporoparietal lobe |
Abdennebi et al. |
Female |
1 |
Surgery + RT |
NAb |
|
Temporal lobe |
Present case |
Male |
32 |
Surgery + CT + RT |
7b |
The definitive diagnosis and correct orientation of a case like this requires an exhaustive study for the exclusion of an extracerebral primary tumor. In our case, this study included a thoracoabdominopelvic CAT scan, a testicular echography, and a PET scan, which were negative.
Germinomas are undifferentiated and aggressive tumors, with a poor response to the complementary treatment. Given the rarity of non-germ cell germ cell tumors histologies, in literature reviews of prognosis and survival these are often grouped in the same category,[7] with a 45% survival rate at 2 years for this subgroup of tumors. From the 19 cases described outside the midline[1] [6] at the time of the respective publications, 4 patients had died in less than 1 year (in 4 cases, the survival was not described). Regarding the modalities of complementary treatment, 12 patients from the 19 cases were submitted to chemotherapy programs (5 in conjunction with radiotherapy).[6] [8] Two patients underwent the same scheme of the case presented here. Three patients received vinblastine + cisplatin + bleomycin. Two patients received carboplatin + etoposide + bleomycin. One patient received vincristine + cisplatin + bleomycin. One patient received etoposide + cisplatin + bleomycin. One patient received carboplatin + vinblastine + etoposide. One patient received intrathecal methotrexate and cytosine + carboplatin + bleomycin. And one patient received vinblastine + bleomycin + cisplatin + etoposide.[6]
Conclusion
The tumor of the yolk sac of the CNS is a germ cell tumor with aggressive characteristics and poor prognosis. The present case reinforces the notion that, although rare, this tumor may occur outside the midline. Having no imaging characteristics that clearly distinguish it from other primary malignant CNS tumors, namely HGGs, it should be maintained as a diagnostic hypothesis in young individuals, since the therapeutic and prognostic orientation are markedly different for this type of tumor.
No conflict of interest has been declared by the author(s).
-
References
- 1 Tsugu H, Oshiro S, Ueno Y. , et al. Primary yolk sac tumor within the lateral ventricle. Neurol Med Chir (Tokyo) 2009; 49 (11) 528-531
- 2 Lazzareschi I, Furfaro IF, Coccia P, Puma N, Riccardi R. Extragonadal yolk sac tumor outside of the midline of the body: a case report of a child with a yolk sac tumor of the pontocerebellar angle. Tumori 2009; 95 (06) 840-842
- 3 Verma R, Malone S, Canil C, Jansen G, Lesiuk H. Primary skull-based yolk-sac tumour: case report and review of central nervous system germ cell tumours. J Neurooncol 2011; 101 (01) 129-134
- 4 Frank TC, Anand VK, Subramony C. Yolk sac tumor of the temporal bone: report of a case. Ear Nose Throat J 2000; 79 (03) 183 , 187–188, 191–192 passim
- 5 Utsuki S, Oka H, Tanizaki Y, Kondo K, Fujii K. Radiological features of germinoma arising from atypical locations. Neurol Med Chir (Tokyo) 2005; 45 (05) 268-271
- 6 Wang CH, Hsu TR, Yang TY. , et al. Primary yolk sac tumor of bilateral basal ganglia. J Chin Med Assoc 2010; 73 (08) 444-448
- 7 Odgen AT, Bruce JN. Pineal Region Tumors. In: Bernstein M. Neuro-oncology - The essentials. New York: Thieme Publishers; 2008: 299-305
- 8 Schmidek H. Schmidek and Sweet Operative Neurosurgical Techniques. Philadelphia: Elsevier; 2000: 908-915
Address for correspondence
-
References
- 1 Tsugu H, Oshiro S, Ueno Y. , et al. Primary yolk sac tumor within the lateral ventricle. Neurol Med Chir (Tokyo) 2009; 49 (11) 528-531
- 2 Lazzareschi I, Furfaro IF, Coccia P, Puma N, Riccardi R. Extragonadal yolk sac tumor outside of the midline of the body: a case report of a child with a yolk sac tumor of the pontocerebellar angle. Tumori 2009; 95 (06) 840-842
- 3 Verma R, Malone S, Canil C, Jansen G, Lesiuk H. Primary skull-based yolk-sac tumour: case report and review of central nervous system germ cell tumours. J Neurooncol 2011; 101 (01) 129-134
- 4 Frank TC, Anand VK, Subramony C. Yolk sac tumor of the temporal bone: report of a case. Ear Nose Throat J 2000; 79 (03) 183 , 187–188, 191–192 passim
- 5 Utsuki S, Oka H, Tanizaki Y, Kondo K, Fujii K. Radiological features of germinoma arising from atypical locations. Neurol Med Chir (Tokyo) 2005; 45 (05) 268-271
- 6 Wang CH, Hsu TR, Yang TY. , et al. Primary yolk sac tumor of bilateral basal ganglia. J Chin Med Assoc 2010; 73 (08) 444-448
- 7 Odgen AT, Bruce JN. Pineal Region Tumors. In: Bernstein M. Neuro-oncology - The essentials. New York: Thieme Publishers; 2008: 299-305
- 8 Schmidek H. Schmidek and Sweet Operative Neurosurgical Techniques. Philadelphia: Elsevier; 2000: 908-915




