

RSS-Feed abonnieren
DOI: 10.1055/s-0035-1549224
Subdural Metastasis of Prostate Cancer
Autoren
Address for correspondence
Publikationsverlauf
13. November 2014
10. Februar 2015
Publikationsdatum:
13. Mai 2015 (online)


Abstract
Dural metastasis from prostate cancer is rare and may mimic a subdural hematoma (SDH). Preoperatively diagnosis may be difficult and only reveal its presence during surgery. We present such a case and review the literature to identify common characteristics. A 65-year-old man presented with headache, confusion, and progressive right upper limb weakness. Past history included a prostate adenocarcinoma with bone metastasis 3 years earlier. Head computed tomography (CT) scan without contrast revealed a multinodular bilateral hyperdense extra-axial lesion interpreted as acute SDH. At surgery planned for SDH drainage no blood was found; instead there was an en plaque subdural yellowish tumor. Histopathologic examination was consistent with metastatic adenocarcinoma of the prostate. We found 11 cases reported as dural metastasis of prostate cancer mimicking SDH. Surgery was performed on nine cases with no suspicion of dural metastasis. On preoperative nonenhanced CT scan images, three types of image patterns can be described: a nodule in SDH, multinodular metastasis surrounded by SDH, and large en plaque subdural tumor. The latter group consists of those cases where no blood but rather an en plaque subdural tumor was found at surgery. Even though rare, dural metastasis should be considered among the differential diagnoses in a patient known for prostate cancer.
Introduction
Carcinomatous infiltration of the dura from nonneurologic cancer is rare. It has been found at autopsy in 8 to 9% of cases of extraneural malignancy.[1] Laigle-Donadey et al[2] found in a series of 198 cases of dural metastasis that the tumor types metastasizing to the dura mater are cancers of the prostate (19.5%), breast (16.5%), lung (11%), and stomach (7.5%); thus prostate cancer is evidently more susceptible to spread to the dura. Tremont-Luktas et al[3] reported that in 118 cases of brain metastasis of prostate cancer, 19 spread to the dura. In a few cases, the diagnosis of dural metastasis was made following subdural bleeding. However, in other cases no blood was found during surgery, thus revealing the mimicking appearance of the subdural metastasis. Recognition of this latter occurrence may help determine the best management for each individual case.
Material and Methods
We report a case of dural metastasis of prostate cancer mimicking subdural hematoma (SDH). We reviewed the English and French literature for cases presenting with suspected SDH to ascertain common clinical and imagery characteristics of metastasis mimicking SDH.
Results
Illustrative Case
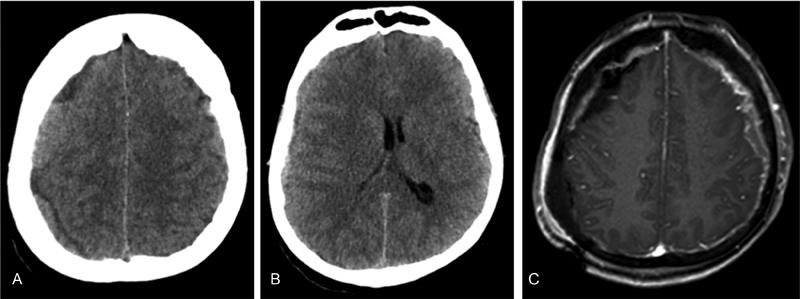
A 65-year-old man was admitted to the emergency department presenting with headache, confusion, and progressive right upper limb weakness. He also reported a recent fall at home. Past history included a metastatic prostate adenocarcinoma 3 years earlier, for which he underwent hormonal therapy. His prostate-specific antigen (PSA) fell from 377 to 190 μg/L. Pelvic lymph nodes and bone metastasis were diagnosed 3 years ago. On initial examination he was mildly confused, with a drift of his left upper limb. Computed tomography (CT) scan of the head without contrast revealed a multinodular bilateral hyperdense extra-axial lesion ([Fig. 1A]) with a midline shift of 4 mm to the right ([Fig. 2B]). This image was interpreted as acute SDH. The patient was initially observed. The next day he became more confused and progressively nonresponsive. A second CT scan showed progress of the midline shift to 7.8 mm. A left parietal burr hole was performed for SDH drainage. Upon opening the dura, no blood was found. Instead there was an obvious subdural tumor. A craniotomy was performed, revealing an en plaque frontoparietal temporal subdural yellowish tumor, with no cortical involvement. The bone had an abnormal appearance, suggesting bone metastasis. The tumor was excised as much as possible including the adjacent dura. The involved bone was not replaced. Postoperative magnetic resonance imaging (MRI) showed prominent irregular enhancing tissue along the dura consistent with bilateral dural metastasis ([Fig. 1C]). The patient progressively recovered and left the hospital at day 15 with little weakness of the arm. Retrospectively, we suspect that the clinical deterioration and the rapid increase of the midline shift might be due to an impaired brain venous drainage secondary to the extensive dural metastasis. Histopathologic examination of the obtained tissue was consistent with metastatic adenocarcinoma of the prostate. Due to the extensive generalized bone metastasis that was nonresponsive to previous chemotherapy, no further treatment was undertaken. The patient died 5 months later.

Review of Reported Cases
In the literature we found 11 cases[4] [5] [6] [7] [8] [9] [10] [11] ([Table 1]) reported as dural metastasis of prostate cancer presenting as or mimicking an SDH. Between the first diagnosis of prostate cancer and the discovery of the dural metastasis, the time ranged from 3 months to 7 years (mean: 33 months); the mean age of these patients was 64.5 years. All patients (when data were known) presented in the advanced stage with metastasis. No correlation was found between an anterior history of head trauma and the finding of blood on surgery. Two cases were not operated on because of the obvious evidence of dural metastasis, seen on CT scan and MRI. In all the other cases surgery was performed with no suspicion of dural metastasis. In five cases no blood was found; there was an en plaque subdural tumor. In these cases the burr hole or craniotomy that had been preoperatively planned had to be converted into a larger craniotomy. When reviewing the preoperative nonenhanced CT scan images of all of the 11 patients, we can describe three types of image patterns ([Fig. 2A–C]): a nodule in SDH (two cases),[4] [9] multinodular metastasis surrounded by SDH (three cases),[4] [7] [8] and large en plaque subdural tumor (six cases).[5] [6] [10] [11] [12] [13] This latter group consists of those cases where no blood was found at surgery.
|
Study |
Age, y |
History of trauma |
Clinical signs |
SDH description |
CT scan |
MRI |
Other locations |
Surgery |
Surgery finding |
Pathologic diagnosis |
Type of image pattern[a] |
Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Meara et al[9] |
62 |
No |
Epistaxis; cognitive impairment |
Acute on chronic |
Nodular hyperdense and hypodense extra-axial collection |
No |
NA |
Burr hole; collection evacuation |
Hematoma and thickening of dura |
On dura matter |
A |
Death 4 d postoperatively |
|
George et al[8] |
72 |
No |
Confusion |
Chronic |
Hypodense lentiform extra-axial collection |
Dural enhancement; nodular lesion |
NA |
Burr hole; collection evacuation |
Hematoma |
On hematoma membrane |
B |
Death 7 d postoperatively |
|
Yu et al[11] |
62 |
No |
Upper limbs weakness; convulsion |
Acute |
Bilateral hyperdense to isodense extraaxial collection |
Diffuse enhanced meningeal thickening; nodular areas; enhancing bilateral dural soft tissues |
Bone, lung, liver |
No surgery |
– |
– |
C |
NA |
|
Dorsi et al[7] |
71 |
Yes |
Headaches; word-finding; instability; apraxia |
Chronic |
Hypodense lentiform extra-axial collection |
Extensive dural enhancement; nodular lesions |
NA |
Craniotomy; tumor resection; collection evacuation |
Yellow fluid under high pressure; thickening of dura with nodularity |
On dura matter |
B |
NA |
|
Dols et al[6] |
54 |
No |
Headaches; nausea; Facial palsy |
Acute on chronic |
Isodense extraaxial collection and edema |
Extensive dural enhancement |
Bone |
No surgery |
– |
– |
C |
Death at day 3 of hospitalization |
|
Patil et al[10] |
71 |
Yes |
Headaches; dizziness |
Subacute on chronic |
Isodense to hypodense collection |
Postoperatively: homogeneous enhanced subdural lesion |
NA |
Burr hole transformed in craniotomy; tumor biopsy |
En plaque diffuse subdural tumor; no blood |
On subdural tumor |
C |
25 mo |
|
Cheng et al[5] |
72 |
No |
Headaches; hemiparesis |
Chronic |
Hypodense extraaxial collection and edema |
Postoperatively: enhancing lesion along the dura matter, extending bilaterally from the skull base |
Bone |
Surgery for hematoma (no precision) |
Diffuse thickening; yellowish tumor; no blood |
On subdural tumor and dura matter |
C |
4 mo |
|
Tomlin and Alleyne[13] |
61 |
Yes |
Headaches; cognitive impairment |
Subacute |
Isodense extraaxial collection |
Postoperatively: enhancing lesion along the dura matter |
Bone, lymph node |
Burr hole transformed in craniotomy; tumor biopsy |
Diffuse thickening of dural; confluent epidural and subdural tumor; no blood |
On subdural tumor and dura matter |
C |
3 mo |
|
Oka et al[12] |
60 |
No |
Headaches; cognitive impairment; hemiparesis |
Acute |
Hypodense multilobular crescent |
No |
Bone |
Craniotomy for acute hematoma |
Subdural yellowish tumor; no blood |
On subdural tumor |
C |
NA |
|
Bucci and Farhat[4] |
62 |
No |
Headaches; confusion |
Subacute |
Isodense fluid collection |
No |
NA |
Craniotomy for subacute hematoma |
Thin membrane-covered hematoma |
On hematoma membrane |
B |
Dead at 4 d postoperatively |
|
63 |
No |
Confusion; lower limbs weakness |
Chronic |
Hypodense subdural collection |
No |
Bone |
Craniotomy for chronic hematoma |
Hematoma with membrane |
On hematoma membrane |
A |
NA |
|
|
Our case |
65 |
Yes |
Confusion; upper limb weakness |
Subacute |
Bilateral multinodular hyperdense extra-axial collection |
Postoperatively: prominent enhancing lesion along the dura matter |
Bone |
Burr hole transformed in craniotomy |
Diffuse thickening; yellowish tumor; no blood |
On subdural tumor, dura matter, and bone |
C |
5 mo |
Abbreviations: CT, computed tomography; NA, not available; NMR, nuclear magnetic resonance; SDH, subdural hematoma.
a A, single nodular; B, multinodular; C, en plaque.
Discussion
Brain metastasis secondary to prostate cancer is rare, as is dural metastasis. However, prostate cancer appears to be the most common origin of dural metastases.[2] [14] In their large series on dural metastases, Laigle-Donadey et al[2] observed that dural metastasis originated from the direct extension of skull metastasis in 57% of cases and from a hematogenous route in 43% of cases. Another potential mechanism for skull and subdural metastases of prostate cancer could be retrograde spread through the vertebral venous plexus. It is also known that dural metastasis can present as, or mimic, SDH.[4] [5] [7] [8] [9] [10] [12] [13] Including the present case, 12 cases have been reported.[4] [5] [6] [7] [8] [9] [10] [12] [13] Of the 10[4] [5] [7] [8] [9] [10] [12] [13] operated cases, the preoperative diagnosis of subdural metastasis was missed. In five cases[5] [10] [11] [12] [13] no blood was found during surgery; instead there was an en plaque subdural tumor. All 12 cases were known for prostate cancer with most of them in an advanced stage with bone or lymph node metastasis. In fact, as shown in [Table 1], prognosis was grim in all cases regardless of whether there was trauma or not, with survival ranging from a few days to 5 months, except for one patient who survived for 25 months.
The time between the first diagnosis of prostate cancer and the discovery of the dural metastasis was highly variable ranging from 3 months to 7 years.
The preoperative appearance on the CT scan of the subdural collection was nodular or multinodular, associated at times with brain edema. The bone views often revealed diffuse sclerotic changes of the skull suggestive of bone metastasis. Including our case, only one other case[11] was bilateral. Also, on postoperative MRI, there were diffuse pachymeningeal thickening with enhancement and areas of nodular enhancing soft tissues.
Reexamining the CT scans provided in the literature of these 12 cases, we identified three patterns ([Fig. 2]) that could lead us to a more accurate diagnosis upon admission: (1) a nodule in an SDH[4] [9] ([Fig. 2A]), (2) multinodular metastasis surrounded by an SDH[4] [7] [8] ([Fig. 2B]), and (3) an extensive en plaque subdural tumor[5] [6] [10] [11] [12] [13] ([Fig. 2C]) as in our case. Types 1 and 2 may be particularly misleading because a burr hole to drain the blood may miss the tumor. In type 3 cases, where unexpectedly no blood is found, a larger craniotomy reveals an extensive tumor not amenable to surgical treatment.
Knowing these imagery features in advance helps us to be more vigilant and thus make a more accurate diagnosis to choose the right course of treatment and possibly avoid unnecessary surgery. Indeed, of the 10 patients who underwent surgery, 6 died within 4 days to 3 months.[4] [5] [8] [9] [10] This suggests that dural metastasis secondary to prostate cancer occurs at an end stage of advanced disease.
Conclusion
Although rare, dural metastasis should be considered among the differential diagnoses in a patient known for prostate cancer, particularly with bone metastasis. The nodular features of the subdural collection on a nonenhanced CT scan should alert us to the possibility of subdural metastasis and prompt us to investigate further. This can lead to better management and possibly avoid unnecessary surgery. Simply being aware of the possibility that dural metastasis may mimic hematoma in cases of metastatic prostate cancer may help evaluate the indication for surgery, especially in this group of patients often harboring a poor prognosis.
-
References
- 1 Meyer PC, Reah TG. Secondary neoplasms of the central nervous system and meninges. Br J Cancer 1953; 7 (4) 438-448
- 2 Laigle-Donadey F, Taillibert S, Mokhtari K, Hildebrand J, Delattre JY. Dural metastases. J Neurooncol 2005; 75 (1) 57-61
- 3 Bobustuc G, Lagos GK, Lolas K, Kyritsis AP, Puduvalli VK. Brain metastasis from prostate carcinoma: The M.D. Anderson Cancer Center experience. Cancer 2003; 98 (2) 363-368
- 4 Bucci MN, Farhat SM. Metastatic adenocarcinoma of the prostate as a cause of subdural hematoma. J Urol 1986; 135 (4) 803-804
- 5 Cheng YK, Wang TC, Yang JT, Lee MH, Su CH. Dural metastasis from prostatic adenocarcinoma mimicking chronic subdural hematoma. J Clin Neurosci 2009; 16 (8) 1084-1086
- 6 Dols MC, Calle SG, Chamorro EV, Díaz IA, Pino AM, García JA. Dural metastases with subdural hematoma from prostate cancer. Oncologia 2005; 28 (8) 407-411
- 7 Dorsi MJ, Zenonos G, Hsu W, Huang J. Dural prostate adenocarcinoma metastasis with subdural hematoma mimicking the appearance of an epidural hematoma. Clin Neurol Neurosurg 2010; 112 (6) 501-504
- 8 George KJ, Lau A, Ellis M, Kiehl TR, Fehlings MG. Metastatic coagulopathic subdural hematoma: A dismal prognosis. Surg Neurol Int 2012; 3: 60
- 9 Meara ACO, Mahasneh T, Wilson P, Ons BI, Alkhawaja D. Dural prostate metastasis resembling a chronic subdural haematoma. J Surg Case Rep 2012; 5: 7
- 10 Patil S, Veron A, Hosseini P , et al. Metastatic prostate cancer mimicking chronic subdural hematoma: a case report and review of the literature. J La State Med Soc 2010; 162 (4) 203-205
- 11 Yu W, Sitt C, Cheung TCY. Dural metastases from prostate cancer mimicking acute sub-dural hematoma. Emerg Radiol 2012; 19 (6) 549-552
- 12 N'Dri Oka D, Varlet G, Boni N, Broalet E, Boukassa L, Zeze VBA. Métastase durale d'un adénocarcinome sous-dural aigu intracrânien à propos d'une observation. J Neuroradiol 2013; 27 (4) 282-284
- 13 Tomlin JM, Alleyne CH. Transdural metastasis from adenocarcinoma of the prostate mimicking subdural hematoma: case report. Surg Neurol 2002; 58 (5) 329-331 ; discussion 331
- 14 Nayak L, Abrey LE, Iwamoto FM. Intracranial dural metastases. Cancer 2009; 115 (9) 1947-1953
Address for correspondence
-
References
- 1 Meyer PC, Reah TG. Secondary neoplasms of the central nervous system and meninges. Br J Cancer 1953; 7 (4) 438-448
- 2 Laigle-Donadey F, Taillibert S, Mokhtari K, Hildebrand J, Delattre JY. Dural metastases. J Neurooncol 2005; 75 (1) 57-61
- 3 Bobustuc G, Lagos GK, Lolas K, Kyritsis AP, Puduvalli VK. Brain metastasis from prostate carcinoma: The M.D. Anderson Cancer Center experience. Cancer 2003; 98 (2) 363-368
- 4 Bucci MN, Farhat SM. Metastatic adenocarcinoma of the prostate as a cause of subdural hematoma. J Urol 1986; 135 (4) 803-804
- 5 Cheng YK, Wang TC, Yang JT, Lee MH, Su CH. Dural metastasis from prostatic adenocarcinoma mimicking chronic subdural hematoma. J Clin Neurosci 2009; 16 (8) 1084-1086
- 6 Dols MC, Calle SG, Chamorro EV, Díaz IA, Pino AM, García JA. Dural metastases with subdural hematoma from prostate cancer. Oncologia 2005; 28 (8) 407-411
- 7 Dorsi MJ, Zenonos G, Hsu W, Huang J. Dural prostate adenocarcinoma metastasis with subdural hematoma mimicking the appearance of an epidural hematoma. Clin Neurol Neurosurg 2010; 112 (6) 501-504
- 8 George KJ, Lau A, Ellis M, Kiehl TR, Fehlings MG. Metastatic coagulopathic subdural hematoma: A dismal prognosis. Surg Neurol Int 2012; 3: 60
- 9 Meara ACO, Mahasneh T, Wilson P, Ons BI, Alkhawaja D. Dural prostate metastasis resembling a chronic subdural haematoma. J Surg Case Rep 2012; 5: 7
- 10 Patil S, Veron A, Hosseini P , et al. Metastatic prostate cancer mimicking chronic subdural hematoma: a case report and review of the literature. J La State Med Soc 2010; 162 (4) 203-205
- 11 Yu W, Sitt C, Cheung TCY. Dural metastases from prostate cancer mimicking acute sub-dural hematoma. Emerg Radiol 2012; 19 (6) 549-552
- 12 N'Dri Oka D, Varlet G, Boni N, Broalet E, Boukassa L, Zeze VBA. Métastase durale d'un adénocarcinome sous-dural aigu intracrânien à propos d'une observation. J Neuroradiol 2013; 27 (4) 282-284
- 13 Tomlin JM, Alleyne CH. Transdural metastasis from adenocarcinoma of the prostate mimicking subdural hematoma: case report. Surg Neurol 2002; 58 (5) 329-331 ; discussion 331
- 14 Nayak L, Abrey LE, Iwamoto FM. Intracranial dural metastases. Cancer 2009; 115 (9) 1947-1953