

Subscribe to RSS
DOI: 10.1055/s-0034-1366074
Imaging of Appendicitis in Adults
Bildgebung der Appendizitis beim ErwachsenenAuthors
Correspondence
Publication History
18 October 2013
20 December 2013
Publication Date:
23 April 2014 (online)

Abstract
Three imaging modalities are available for the diagnosis of acute appendicitis: ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI). Transabdominal ultrasound should be the first-line imaging test. Abdominal CT is superior to US and is required immediately in patients with atypical clinical presentation of appendicitis and suspected perforation. However, low-dose unenhanced CT is equal to standard-dose CT with intravenous contrast agents in the detection of five signs of acute appendicitis (thickened appendiceal wall more than 2 mm, cross-sectional diameter greater than 6 mm, periappendicitis, abscess, and appendicolith). MRI is necessary in pregnant women and young adults. This review illustrates the principles of state-of-the-art imaging techniques and their clinical relevance.
Key Points:
• US is the basic diagnostic method in case of suspected appendicitis.
• CT is necessary in patients with atypical presentation of appendicitis.
• MRI should be the first-line imaging test in pregnant women.
Citation Format:
• Karul M, Berliner C, Keller S et al. Imaging of Appendicitis in Adults. Fortschr Röntgenstr 2014; 186: 551 – 558
Zusammenfassung
Zur Akutdiagnostik der Appendizitis stehen drei radiologische Verfahren zur Verfügung: 1. Ultraschall (US); 2. Computertomografie (CT); 3. Magnetresonanztomografie (MRT). Während der transabdominelle Ultraschall zur Basisdiagnostik zählt, sollte die diagnostisch überlegene CT bei atypischen klinischen Appendizitiszeichen und Perforationsverdacht unverzüglich erfolgen. Besonders hervorzuheben ist die native Niedrigdosis-CT, die der Standarddosis-CT nach intravenöser Kontrastmittelapplikation in der Detektion von fünf Appendizitiszeichen (Wandverdickung größer 2 mm, vergrößerter Appendixdurchmesser mehr als 6 mm, Periappendizitis, Abszessformation und Appendicolith) ebenbürtig ist. Die MRT kommt bei Schwangeren und jungen Erwachsenen zum Einsatz. Diese Übersichtsarbeit stellt die Prinzipien der modernen Untersuchungstechniken sowie ihre klinischen Implikationen dar.
Introduction
Acute abdomen is a life-threatening condition requiring prompt diagnosis and often emergency surgery. Acute appendicitis is the most common cause of acute abdomen [1] [2] [3]. The risk of developing acute appendicitis over the course of a lifetime is approximately 7 % [4]. The appendiceal lumen is often obstructed due to lymph node hyperplasia (e. g. in gastroenteritis), coprolites, or parasites [4] [5]. The clinical diagnosis is made on the basis of the classic anamnesis (positive signs of appendicitis, such as Blumberg’s, Rovsing’s, obturator, and psoas sign in the physical examination, fever and elevated inflammation values in lab tests). An increase in the C-reactive protein (CRP) correlates with the severity of the disease and is a possible surrogate parameter for perforation with peritonitis and abscess formation. Leukocytosis is more sensitive for the detection of early-stage appendicitis [6].
Preoperative imaging can be decisive for diagnosis. Three modalities are available for radiological diagnosis: 1. Ultrasound (US); 2. Computed tomography (CT); 3. Magnetic resonance imaging (MRI). CT holds a special position among these methods since it can deliver the exact diagnosis within minutes. Since the start of the new millennium, CT has been the gold standard for diagnosing appendicitis in the United States [7]. In Europe the initial concerns regarding this method due to radiation exposure have been allayed thanks to the continually improving technical means of dose reduction. However, despite this trend it is still necessary for the justifying indication to be closely reviewed by a physician with radiation protection qualification in accordance with § 23 of the X-Ray Ordinance.
The present study provides an overview of radiological examination methods for the diagnosis of acute appendicitis and discusses their implications for the clinical routine. The individual examination methods are first described under consideration of the particular indication/contraindication, technical implementation, morphological imaging criteria for appendicitis, and study results. The advantages and disadvantages of all three methods are then discussed. The resulting conclusions are shown graphically as a diagnostic algorithm in the case of suspicion of appendicitis.
Ultrasound (US)
Indication/contraindication
Transabdominal ultrasound is the basic diagnostic method in the case of suspected appendicitis and is the continuation of the clinical examination [8]. The cost-effective examination is immediately and readily available in the emergency situation. It does not require patient preparation, is noninvasive, and can be repeated at any time. It can be performed quickly and does not entail any patient discomfort.
There are no contraindications. However, the diagnostic information is limited particularly in the case of overlying intestinal gas, existing peritonitic reaction with guarding, or adiposity since the appendix region cannot be sufficiently assessed. Even in the case of an atypical position of the vermiform appendix, an ultrasound examination can be easily interpreted as false negative [9].
Transvaginal US is suitable for verifying or ruling out common diseases of the female genitalia, such as adnexitis, symptomatic ovarian cysts, or ectopic pregnancy, as well as for diagnosing appendicitis if the preceding transabdominal ultrasound scan did not yield a definitive diagnosis.
Method
After complete examination of the abdomen with a convex probe (2 – 5 MHz), targeted sonography of the appendix using a high-resolution linear probe (7.5 – 14 MHz) should be performed. The examiner uses the patient’s pain for orientation and looks for the ileocecal pole. The intraperitoneal appendix can normally be visualized on the medial side of the ileocecal pole or less frequently in a retrocecal position. The normal appendix appears in the longitudinal section as a blind, tubular structure without peristalsis. The organ diameter is less than 6 mm and the appendix can be compressed when pressure is applied via the probe [10] [11].
Morphological imaging criteria of appendicitis
The diagnostic criterion of an inflamed appendix is direct visualization of the pathologically changed vermiform appendix ([Fig. 1]). The classic sign on US is a pathological cockade in the cross section. A target structure comprised of concentric layers with a diameter of more than 6 mm can be seen. The hypoechoic wall is greater than 2 mm thick and the normal wall layering is no longer present particularly in the case of necrosis [10] [12]. An appendicolith with typical dorsal acoustic shadowing can be diagnosed as the cause of the inflammation. Free pericecal and/or retrovesical fluid is a further sign of acute appendicitis. A hyperechogenic reaction of the surrounding tissue is an indication of infiltration of the adjoining adipose tissue [10] [12]. In some cases wall thickening of the adjacent cecum and terminal ileum can be detected. Slightly enlarged, locoregional, reactive lymph nodes are also able to be detected. Additional color-coded duplex sonography can detect increased perfusion of the appendiceal wall as a sign of an inflammatory reaction. The appendix contour is interrupted in the case of a perforated appendix with a perityphlitic abscess [10].

Results
The sensitivity and specificity of transabdominal US are highly examiner-dependent and are often limited ([Table 1]). Combined transabdominal and transvaginal US in the case of suspected appendicitis has a sensitivity/specificity of 97.3 % and 91 %, respectively [9].
|
study |
n = number of patients |
sensitivity in % |
specificity in % |
|
Nasiri et al. 2012 [14] |
75 |
71.2 |
83.3 |
|
Carroll et al. 2012 [15] |
1268 |
92 |
96 |
|
Al Ajerami et al. 2012 [16] |
180 |
84.8 |
83.3 |
During pregnancy, acute appendicitis is the most common cause of an acute abdomen [13]. While US achieves good diagnostic results in the 1st and 2nd trimester, the examination conditions in the 3rd trimester are very limited due to the changed anatomy [13]. The appendix is displaced from the lower right quadrant to the upper right quadrant over the course of pregnancy due to the enlargement of the uterus and is also displaced by the ventral abdominal wall. Irritation of the parietal peritoneum resulting in localized pain is no longer present.
Computed tomography (CT)
Indication/contraindication
If anamnesis, physical examination, lab parameters (C-reactive protein/leukocytes), and transabdominal US did not yield a definitive diagnosis of appendicitis and pregnancy has been ruled out, CT examination of the abdomen should be performed particularly in the case of limited sonographic evaluation options and patients with atypical signs of appendicitis or suspected perforation. Atypical signs of appendicitis are present in approx. 1/3 of all patients [17].
CT is not absolutely contraindicated in pregnant women with suspected appendicitis [18]. However, due to the potential risk of radiation-induced teratogenesis and carcinogenesis [19], it should not be used as the primary examination method, particularly if MRI can be promptly performed. Young adults and women of childbearing age also should not undergo CT examination for radiation hygiene reasons.
Method
The optimal CT protocol for appendicitis diagnosis is a controversial topic of discussion. Variable parameters are the possible enteric and intravenous administration of iodine-containing contrast agent and the effective dose: Low or standard dose. Under consideration of these parameters, we recommend specific CT protocols in the following sections.
Unenhanced CT
Since patients receive neither enteric nor intravenous contrast agent, unenhanced CT to diagnose appendicitis does not require patient preparation. To limit the examination area on the basis of anatomical landmarks, a topogram of the abdomen is first performed. It must be ensured that the patient’s arms are not in the examination area and that the topogram is not selected to be shorter than the examination area. A CT scan is then performed during inspiration from the diaphragm to the head of the femur. Non-overlapping, transverse images with a slice thickness of 5 mm are reconstructed from the CT volume datasets. Moreover, overlapping thin-slice images with a slice thickness of 3 mm and an increment of 1 mm are generated as three-dimensional multiplanar reconstructions.
Morphological imaging criteria of appendicitis
When evaluating CT images, the radiologist performing the examination should pay attention to 5 signs of appendicitis [20] [21] [22]: 1. Enlarged appendix diameter of more than 6 mm (most important parameter in the absence of perforation), 2. Appendiceal wall more than 2 mm thick ([Fig. 2]), 3. Inflammatory compression of the adjoining adipose tissue, 4. Abscess formation in the right lower abdomen, 5. Calcified appendicolith.

The presence of all of the first three criteria indicates non-perforated acute appendicitis. Given the presence of perityphlitic abscess in the case of appendiceal perforation, detection of a calcified appendicolith is not definitive for acute appendicitis [20].
Contrast-enhanced CT
The venous contrast agent phase (automatic start delay of approximately 110 s after intravenous contrast agent application of approx. 130 ml of iodine-containing contrast agent) is highly suitable for appendicitis diagnosis because the indicated appendicitis signs can be best evaluated in this phase. In addition to the above criteria, contrast-enhanced CT shows an appendix with wall thickening and ring-shaped contrast enhancement ([Fig. 3]) that is pathognomonic for the diagnosis. A further advantage of intravenous contrast agent application is the exact visualization of complications. Therefore, for example in the case of appendix perforation, an encapsulated, parietal contrast-enhanced abscess in the right lower abdomen can be better evaluated in comparison to unenhanced CT ([Fig. 4]).


Contrast agent should be used in compliance with the recommendations of the ESUR (European Society of Urogenital Radiology) [23]. The known contraindications for intravenous contrast agent application are for example contrast agent allergy, renal insufficiency, untreated hyperthyroidism, and plasmacytoma.
Enteric contrast agent application (per os and/or rectal) in addition to intravenous contrast agent application is considered unnecessary by some authors since it does not significantly improve the sensitivity/specificity [24] [25] [26] and results in a longer duration of stay in the emergency room. For these reasons we do not perform enteric contrast enhancement in our clinic.
CT dose
Both the unenhanced and contrast-enhanced effective CT dose is significant in the case of suspected appendicitis. Accordingly, it should be as low as possible while maintaining constant diagnostic quality and follow the ALARA principle. Possible means of dose reduction are the reduction of both the tube current (mAs) and the tube voltage (kV) while using fully automatic dose modulation techniques and the implementation of iterative reconstruction methods [27]. [Table 2] shows typical examination protocols using the low-dose and standard-dose technique in a normal-weight patient.
Results
In a retrospective study Coursey et al. evaluated the preoperative use of CT in patients with suspected appendicitis and the effect on the negative appendectomy rate. The authors showed that the number of preoperative CT examinations in a 10-year period increased from 18.5 % to 93.2 % causing the rate of negative appendectomies to drop from 16.7 % to 8.7 % [28].
Multiple studies compared the diagnostic accuracy of low-dose CT and standard-dose CT in the case of suspected appendicitis [21] [29] [30] [31]. The authors came to the conclusion that low-dose CT is equally suitable for diagnosing appendicitis. For example, Kim et al. determined the rates of unnecessary appendectomies in 890 patients after standard-dose CT and low-dose CT in a randomized prospective study and compared the results [21]. The patients were divided into two groups. In the first group, 438 patients underwent low-dose CT (average DLP = 116 mGy × cm) and in the second group, 441 patients underwent standard-dose CT (average DLP = 521 mGy × cm). Contrast agent was administered intravenously to all patients. Acute appendicitis was histopathologically verified in 37.9 % of the patients in group 1 and in 40.8 % in group 2. The rate of unnecessary appendectomies after low-dose CT was 3.5 % (6/172 patients) and 3.2 % (6/186 patients) after standard-dose CT.
Seo et al. demonstrated that low-dose CT even without contrast agent is equivalent to standard-dose CT after intravenous contrast agent application [30]. They examined 207 adults with clinical suspicion of appendicitis. Of the patients included in the retrospective study, 78 had histopathologically verified acute appendicitis. Two blinded radiologists interpreted the images: The sensitivity and specificity were 98.7 % and 95.3 %, respectively, for unenhanced low-dose CT and 100 % and 93 %, respectively, for standard-dose CT after intravenous contrast agent application for the first radiologist and 100 % in each case for unenhanced low-dose CT and 96.9 % in each case for standard-dose CT after intravenous contrast agent application for the second radiologist ([Table 3]).
|
study |
n = number of patients |
sensitivity in % |
specificity in % |
|
Kim et al. 2012 [21] |
440 SD iv 433 ND iv |
95.0 94.5 |
93.8 93.3 |
|
Seo et al. 2009 [30] |
207 SD iv 207 ND unenhanced |
100/100 98/100 |
93/96 95/96 |
|
Kim et al. 2011 [29] |
44 SD iv 55 ND iv |
89 90 |
89 90 |
|
Platon et al. 2009 [31] |
86 SD iv 86 ND o |
100/100 100/100 |
98/98 98/98 |
Magnetic resonance imaging (MRI)
Indication/contraindication
MRI in the case of suspicion of appendicitis is indicated in patients with special radiation protection requirements, e. g. young adults (in particular women of childbearing age), women in whom a pregnancy cannot be ruled out in the emergency situation, and pregnant women. Early diagnosis of acute appendicitis during pregnancy limits the complications that could endanger the life of the mother and the unborn child [32].
Due to the longer examination times, the higher costs, and the limited availability, MRI of the abdomen is not the first choice method in the case of clinical suspicion of appendicitis. General contraindications include a pacemaker, claustrophobia, metal splinters/vascular clips, or large tattoos located in the examination area.
Method
MRI of the abdomen in suspected appendicitis does not require any targeted evacuation measures or other patient preparation. Intravenous administration of butylscopolamine bromide under consideration of contraindications (pregnancy, known sensitivity to the drug, narrow-angle glaucoma, tachycardia arrhythmia, retention of urine, mechanical stenoses of the GI tract, myasthenia gravis) reduces peristalsis resulting in improved image quality.
Unenhanced MRI
Unenhanced MRI of the abdomen has high soft tissue contrast and is capable of providing excellent visualization of the appendix [33]. Some authors recommend additional sagittal sequences for localizing the appendix [34]. However, the acquisition of transverse and coronal sequences is sufficient [35] [36] [37]. For optimum visualization of both the peritoneal fat and the appendix, T1-weighted sequences (hypointense appendiceal wall) and fat-saturated T2-weighted sequences (hyperintense appendiceal wall) are necessary ([Fig. 5]). The fat saturation allows excellent visualization of the intramural edema and the periappendiceal inflammation.

Diffusion-weighted sequences can be created to assess the diffusion movement of water molecules (Brown’s molecular movement) in the appendiceal wall. The apparent diffusion coefficient (ADC) was developed to be able to quantify the signals of these sequences. Diffusion-weighted MRI is evaluated automatically via ADC mapping.
Contrast-enhanced MRI
Contrast agent administration is not absolutely necessary in the case of suspicion of appendicitis. If the diagnosis cannot be definitively made in the unenhanced examination, intravenous contrast agent application is indicated under consideration of the individual risks, particularly for pregnant women [38]. Due to the fact that clinical data regarding contrast agent application in pregnancy is only available on a limited basis, multiple factors (e. g. chemical background and teratogenicity) must be taken into consideration in the risk-benefit analysis. After intravenous contrast agent application, there is significant signal enhancement in the appendiceal wall and a periappendicitic reaction in the surround tissue in the T1-weighted sequences after fat saturation.
Morphological imaging criteria of appendicitis
An enlarged appendix diameter of more than 7 mm, edematous compression of the surrounding mesenterial adipose tissue, limited diffusion in the thickened appendiceal wall and abscess formation in the right lower abdomen after appendix perforation are signs of appendicitis [39]. The first three signs are particularly specific. The probability of appendicitis is 88 % if only one of these three signs can be detected, 94 % in the case of two signs, and 96 % in the case of the combination of all of the first three signs [39].
Results
The sensitivity and specificity of conventional MRI (T1 / T2-weighted sequences and T1-weighted sequences after intravenous contrast agent application) for the diagnosis of acute appendicitis are between 90 % and 100 % as in the case of CT ([Table 4]).
|
study |
n = number of patients |
Sensitivity in % |
Specificity in % |
|
Pedrosa et al. 2009 [41] |
148 |
100 |
93 |
|
Heverhagen et al. 2012 [35] |
52 |
85 |
97 |
|
Oto et al. 2009 [33] |
118 |
90 |
98 |
|
Avcu et al. 2013 [40] |
60 |
97.5 |
100 |
Research is increasingly focused on the use of diffusion-weighted sequences [39] [40]. Leeuwenburgh et al. discovered limited diffusion in the appendiceal wall as a reliable indicator of acute inflammation [39]. Avcu et al. also examined whether the ADC value plays a role in the differentiation between perforated and non-perforated appendicitis [40]. 60 adults with suspected appendicitis were included in this prospective study. The diagnosis of acute appendicitis was correctly made via MRI in 44 cases. The findings were normal in the remaining patients. A perforation was histopathologically confirmed in 12 cases of the 40 patients with acute appendicitis. The other 28 patients had non-perforated appendicitis.
The average ADC value in patients with non-perforated appendicitis was lower than in a control group (1.01 × 10-3 mm2/s vs. 1.85 × 10-3 mm2/s) or the value in patients with perforated appendicitis was lower than in patients with non-perforated appendicitis (0.79 × 10-3 mm2/s vs. 1.11 × 10-3 mm2/s). The authors concluded that diffusion-weighted MRI including the calculated ADC values can be effectively used for diagnosing appendicitis and appendiceal perforations could be reliably detected in the same breath.
Discussion
Acute appendicitis is the most common reason for legal disputes with patients in the emergency setting [17]. A delay in diagnosis and necessary treatment can have major consequences. Therefore, radiological diagnosis is very important and requires a high level of expertise on the part of the radiologist. [Table 5] shows advantages and disadvantages of the three imaging modalities for the diagnosis of acute appendicitis.
Transabdominal US should be routinely performed in the case of suspicion of appendicitis. Targeted examiner training ensures quality standards and results in high diagnostic accuracy. The examination is cost-effective when performed properly. However, if it does not yield a definitive diagnosis, additional comparatively more expensive examinations must be performed.
Due to the high regional availability as well as the more constant examination quality and reproducibility of CT compared to US, the use of CT for diagnosis in the case of suspicion of appendicitis has increased considerably. CT can quickly provide the correct diagnosis. In a literature review, 671 patients were examined with US and then via CT. The sensitivity and specificity in the diagnosis of histopathologically verified acute appendicitis were 91 % and 90 %, respectively, for CT and 78 % and 83 %, respectively, for US [42]. The early use of CT lowers the mortality rate since it shows impending vital complications consequently resulting in shorter durations of inpatient care [8].
If acute appendicitis cannot be detected, other pathological findings can be determined. The most common differential diagnoses are summarized in [Table 6] [2] [8]. In the case of a non-pathological finding, the patient can be discharged immediately after the examination resulting in a savings for the hospital.
|
MRI currently plays a secondary role. However, due to the tendency toward increasingly fast sequences, it remains to be seen whether MRI will be used more frequently to diagnose acute appendicitis. The higher costs compared to the other modalities are put into perspective when it is taken into consideration that the correct diagnosis can be made via MRI. It is not necessary to perform further examinations. In a current multicenter study [43], the three examination methods were performed in a total of 230 patients with suspected appendicitis. After transabdominal US examination, contrast-enhanced CT of the abdomen (115 patients) was performed if the US finding was negative or not definitively pathological. All patients then underwent unenhanced MRI. The appendicitis diagnosis was histopathologically confirmed in 118 patients. The sensitivity and specificity of MRI and CT for detecting appendicitis were comparatively high. Under consideration of the young patient age (average age: 35 years) and in light of the fact that 60 % of the patients were female, the authors concluded that unenhanced MRI should be used to a greater extent for diagnosing appendicitis.
Conclusion
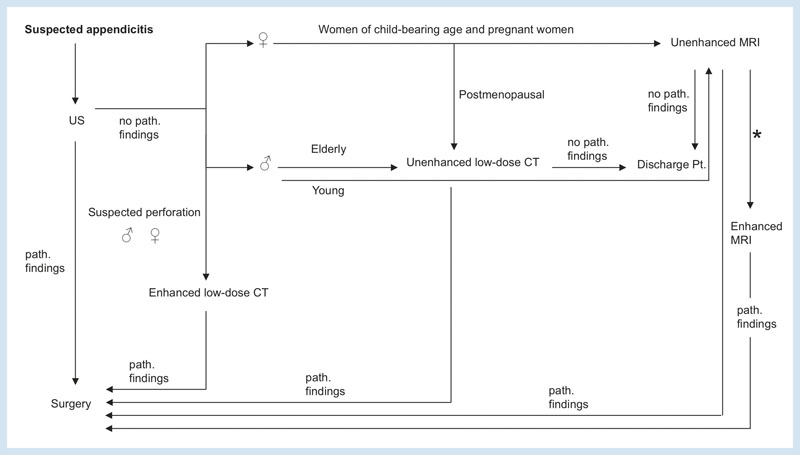
Transabdominal US is the first choice examination method in the case of suspicion of appendicitis. If a definitively pathological finding could not be determined and the patient presented during the clinical examination with atypical appendicitis signs (lack of at least one of the classic signs: fever, wandering pain, pain on palpation of McBurney’s point or elevated inflammation values in lab tests), further diagnostic methods must be performed. Unenhanced low-dose CT should be performed in postmenopausal women. Unenhanced MRI should be performed in women of childbearing age, pregnant women, or in women in whom a pregnancy cannot be ruled out in the emergency situation.
Young men should undergo unenhanced low-dose CT or unenhanced MRI if available. In the case of significantly elevated CRP values and suspicion of perforation, CT with intravenous contrast agent application should be performed in men and women (excluding pregnant women) for time reasons to rule out perityphlitic abscess. The flowchart in [Fig. 6] shows possible steps for diagnosing acute appendicitis.
-
References
- 1 Marincek B. Akutes Abdomen: Bildgebung heute. Dtsch Arztebl 2002; 99: 3010-3017
- 2 Kreis ME, Koch FEv, Jauch KW et al. Abklärung des rechtsseitigen Unterbauchschmerzes. Dtsch Arztebl 2009; 2: 42a
- 3 Petroianu A. Diagnosis of acute appendicitis. Int J Surg 2012; 10: 115-119
- 4 Hardin JR M. Acute Appendicitis: Review and Update. Am Fam Physician 1999; 60: 2027-2034
- 5 Mysorekar VV, Chanda S, Dandeka CP. Mast cells in surgically resected appendices. Indian J Pathol Microbiol 2006; 49: 229-233
- 6 Kim HC, Yang DM, Lee CM et al. Acute appendicitis: relationships between CT determined severities and serum white blood cell counts and C-reactive protein levels. Br J Radiol 2011; 84: 1115-1120
- 7 Reich B, Zalut T, Weiner SG. An international evaluation of ultrasound vs. computed tomography in the diagnosis of appendicitis. Int J Emerg Med 2011; 29: 68
- 8 Lankisch PG, Mahlke R, Lübbers H. Das akute Abdomen aus internistischer Sicht. Dtsch Arztebl 2009; 2: 46a
- 9 Bondi M, Miller R, Zbar A et al. Improving the diagnostic accuracy of ultrasonography in suspected acute appendicitis by the combined transabdominal and transvaginal approach. Am Surg 2012; 78: 98-103
- 10 Ultraschall-Kurs. Dietrich CF. (ed.) Köln: Deutscher Ärzte-Verlag; 2012: 215-216
- 11 Koichi Y, Toshizo K, Shigeru S et al. Sonographic appearance of the normal appendix in adults. J Ultrasound Med 2007; 27: 37-43
- 12 Sonographische Appendizitisdiagnostik. Möglichkeit und Grenzen. Hans Marseille Verlag GmbH München Chir Praxis 2001; 58: 587-598
- 13 Lim HK, Bae SH, Seo GS. Diagnosis of acute appendicitis in pregnant women: value of sonography. Am J Roentgenol 1992; 159: 539-542
- 14 Nasiri S, Mohebbi F, Sodagari N et al. Diagnostic values of ultrasound and the Modified Alvarado Scoring System in acute appendicitis. Int J Emerg Med 2012; 5: 26
- 15 Carroll PJ, Gibson D, El-Faedy O et al. Surgeon-performed ultrasound at the bedside for the detection of appendicitis and gallstones: systematic review and meta-analysis. Am J Surg 2013; 205: 102-108
- 16 Al-Ajerami Y. Sensitivity and specificity of ultrasound in the diagnosis of acute appendicitis. East Mediterr Health J 2012; 18: 66-69
- 17 MRT in der Gastroenterologie. Adamek HE, Lauenstein TC, (eds.) Stuttgart, New York: Thieme; 2009: 168-182
- 18 Ames CM, Shipp TD, Castro EE et al. The use of helical computed tomography in pregnancy for the diagnosis of acute appendicitis. Am J Obstet Gynecol 2001; 184: 954-957
- 19 Chen MM, Coakley FV, Kaimal A et al. Guidelines for computed tomography and magnetic resonance imaging use during pregnancy and lactation. Obstet Gynecol 2008; 112: 333-340
- 20 Karul M, Avanesov M, Yamamura J. Acute appendicitis: a clinical diagnosis?. Radiologe 2012; 52: 1089-1090
- 21 Kim K, Kim YH, Kim SY et al. Low-dose abdominal CT for evaluating suspected appendicitis. N Engl J Med 2012; 366: 1596-1605
- 22 Lai V, Chan WC, Lau HY et al. Diagnostic power of various computed tomography signs in diagnosing acute appendicitis. Clin Imaging 2012; 36: 29-34
- 23 Stacul F, van der Molen AJ, Reimer P et al. Contrast Media Safety Committee of European Society of Urogenital Radiology (ESUR). Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines. Eur Radiol 2011; 21: 2527-2541
- 24 Hekimoglu K, Yildirim UM, Karabulut E et al. Comparison of combined oral and i.v. contrast-enhanced versus single i.v. contrast-enhanced CT for the detection of acute appendicitis. JBR-BTR 2011; 94: 278-282
- 25 Kepner AM, Bacasnot JV, Stahlman BA. Intravenous contrast alone vs intravenous and oral contrast computed tomography for the diagnosis of appendicitis in adult ED patients. Am J Emerg Med 2012; 30: 1765-1773
- 26 Latifi A, Labruto F, Kaiser S et al. Does enteral contrast increase the accuracy of appendicitis diagnosis?. Radiol Technol 2011; 82: 294-299
- 27 Laqmani A, Buhk JH, Henes FO et al. Impact of a 4th Generation Iterative Reconstruction Technique on Image Quality in Low-Dose Computed Tomography of the Chest in Immunocompromised Patients. Fortschr Röntgenstr 2013; 185: 749-757
- 28 Coursey CA, Nelson RC, Patel MB et al. Making the diagnosis of acute appendicitis: do more preoperative CT scans mean fewer negative appendectomies? A 10-year study. Radiology 2010; 254: 460-468
- 29 Kim SY, Lee KH, Kim TY et al. Acute appendicitis in young adults: low- versus standard-radiation-dose contrast-enhanced abdominal CT for diagnosis. Radiology 2011; 260: 437-445
- 30 Seo H, Lee KH, Kim HJ et al. Diagnosis of acute appendicitis with sliding slab ray-sum interpretation of low-dose unenhanced CT and standard-dose i.v. contrast-enhanced CT scans. Am J Roentgenol 2009; 193: 96-105
- 31 Platon A, Jlassi H, Rutschmann OT et al. Evaluation of al low-dose CT protocol with oral contrast for assessment of acute appendicitis. Eur Radiol 2009; 19: 446-454
- 32 Dabir D, Fürst G, Blondin D. MRI in acute appendicitis in pregnancy. Fortschr Röntgenstr 2010; 182: 1010-1011
- 33 Oto A, Ernst RD, Ghulmiyyah LM et al. MR imaging in the triage of pregnant patients with acute abdominal and pelvic pain. Abdom imaging 2009; 34: 243-250
- 34 Nikolaidis P, Hammond N, Marko J et al. Incidence of visualization of the normal appendix on different MRI sequences. Emerg Radiol 2006; 12: 223-226
- 35 Heverhagen JT, Pfestroff K, Heverhagen AE et al. Diagnostic accuracy of magnetic resonance imaging: a prospective evaluation of patients with suspected appendicitis (diamond). J Magn Reson Imaging 2012; 35: 617-623
- 36 Cobben L, Groot I, Kingma L et al. A simple MRI protocol in patients with clinically suspected appendicitis: results in 138 patients and effect on outcome of appendectomy. Eur Radiol 2009; 19: 1175-1183
- 37 Incesu L, Coskun A, Selcuk MB et al. Acute appendicitis: MR imaging and sonographic correlation. Am J Roentgenol 1997; 168: 669-674
- 38 Fröhlich JM, Kubik-Huch RA. Röntgen-, MR- oder Ultraschallkontrastmittel während der Schwangerschaft oder Stillzeit: Was ist zu beachten?. Fortschr Röntgenstr 2013; 185: 13-25
- 39 Leeuwenburgh MM, Jensch S, Gratama JW et al. MRI features associated with acute appendicitis. Eur Radiol 2013; Epub ahead of print
- 40 Avcu S, Cetin FA, Arslan H et al. The value of diffusion-weighted imaging and apparent diffusion coefficient quantification in the diagnosis of perforated and nonperforated appendicitis. Diagn Interv Radiol 2013; 19: 106-110
- 41 Pedrosa I, Lafornara M, Pandharipande PV et al. Having acute appendicitis: effects of MR imaging on negative laparatomy rate and appendiceal perforation rate. Radiology 2009; 250: 749-757
- 42 van Randen A, Bipat S, Zwinderman AH et al. Acute appendicitis: meta-analysis of diagnostic performance of CT and graded compression US related to prevalence of disease. Radiology 2008; 249: 97-106
- 43 Leeuwenburgh MM, Wiarda BM, Wiezer MJ et al. Comparison of imaging strategies with conditional contrast-enhanced CT and unenhanced MR imaging in patients suspected of having appendicitis: a multicenter diagnostic performance study. Radiology 2013; 268: 135-143
Correspondence
-
References
- 1 Marincek B. Akutes Abdomen: Bildgebung heute. Dtsch Arztebl 2002; 99: 3010-3017
- 2 Kreis ME, Koch FEv, Jauch KW et al. Abklärung des rechtsseitigen Unterbauchschmerzes. Dtsch Arztebl 2009; 2: 42a
- 3 Petroianu A. Diagnosis of acute appendicitis. Int J Surg 2012; 10: 115-119
- 4 Hardin JR M. Acute Appendicitis: Review and Update. Am Fam Physician 1999; 60: 2027-2034
- 5 Mysorekar VV, Chanda S, Dandeka CP. Mast cells in surgically resected appendices. Indian J Pathol Microbiol 2006; 49: 229-233
- 6 Kim HC, Yang DM, Lee CM et al. Acute appendicitis: relationships between CT determined severities and serum white blood cell counts and C-reactive protein levels. Br J Radiol 2011; 84: 1115-1120
- 7 Reich B, Zalut T, Weiner SG. An international evaluation of ultrasound vs. computed tomography in the diagnosis of appendicitis. Int J Emerg Med 2011; 29: 68
- 8 Lankisch PG, Mahlke R, Lübbers H. Das akute Abdomen aus internistischer Sicht. Dtsch Arztebl 2009; 2: 46a
- 9 Bondi M, Miller R, Zbar A et al. Improving the diagnostic accuracy of ultrasonography in suspected acute appendicitis by the combined transabdominal and transvaginal approach. Am Surg 2012; 78: 98-103
- 10 Ultraschall-Kurs. Dietrich CF. (ed.) Köln: Deutscher Ärzte-Verlag; 2012: 215-216
- 11 Koichi Y, Toshizo K, Shigeru S et al. Sonographic appearance of the normal appendix in adults. J Ultrasound Med 2007; 27: 37-43
- 12 Sonographische Appendizitisdiagnostik. Möglichkeit und Grenzen. Hans Marseille Verlag GmbH München Chir Praxis 2001; 58: 587-598
- 13 Lim HK, Bae SH, Seo GS. Diagnosis of acute appendicitis in pregnant women: value of sonography. Am J Roentgenol 1992; 159: 539-542
- 14 Nasiri S, Mohebbi F, Sodagari N et al. Diagnostic values of ultrasound and the Modified Alvarado Scoring System in acute appendicitis. Int J Emerg Med 2012; 5: 26
- 15 Carroll PJ, Gibson D, El-Faedy O et al. Surgeon-performed ultrasound at the bedside for the detection of appendicitis and gallstones: systematic review and meta-analysis. Am J Surg 2013; 205: 102-108
- 16 Al-Ajerami Y. Sensitivity and specificity of ultrasound in the diagnosis of acute appendicitis. East Mediterr Health J 2012; 18: 66-69
- 17 MRT in der Gastroenterologie. Adamek HE, Lauenstein TC, (eds.) Stuttgart, New York: Thieme; 2009: 168-182
- 18 Ames CM, Shipp TD, Castro EE et al. The use of helical computed tomography in pregnancy for the diagnosis of acute appendicitis. Am J Obstet Gynecol 2001; 184: 954-957
- 19 Chen MM, Coakley FV, Kaimal A et al. Guidelines for computed tomography and magnetic resonance imaging use during pregnancy and lactation. Obstet Gynecol 2008; 112: 333-340
- 20 Karul M, Avanesov M, Yamamura J. Acute appendicitis: a clinical diagnosis?. Radiologe 2012; 52: 1089-1090
- 21 Kim K, Kim YH, Kim SY et al. Low-dose abdominal CT for evaluating suspected appendicitis. N Engl J Med 2012; 366: 1596-1605
- 22 Lai V, Chan WC, Lau HY et al. Diagnostic power of various computed tomography signs in diagnosing acute appendicitis. Clin Imaging 2012; 36: 29-34
- 23 Stacul F, van der Molen AJ, Reimer P et al. Contrast Media Safety Committee of European Society of Urogenital Radiology (ESUR). Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines. Eur Radiol 2011; 21: 2527-2541
- 24 Hekimoglu K, Yildirim UM, Karabulut E et al. Comparison of combined oral and i.v. contrast-enhanced versus single i.v. contrast-enhanced CT for the detection of acute appendicitis. JBR-BTR 2011; 94: 278-282
- 25 Kepner AM, Bacasnot JV, Stahlman BA. Intravenous contrast alone vs intravenous and oral contrast computed tomography for the diagnosis of appendicitis in adult ED patients. Am J Emerg Med 2012; 30: 1765-1773
- 26 Latifi A, Labruto F, Kaiser S et al. Does enteral contrast increase the accuracy of appendicitis diagnosis?. Radiol Technol 2011; 82: 294-299
- 27 Laqmani A, Buhk JH, Henes FO et al. Impact of a 4th Generation Iterative Reconstruction Technique on Image Quality in Low-Dose Computed Tomography of the Chest in Immunocompromised Patients. Fortschr Röntgenstr 2013; 185: 749-757
- 28 Coursey CA, Nelson RC, Patel MB et al. Making the diagnosis of acute appendicitis: do more preoperative CT scans mean fewer negative appendectomies? A 10-year study. Radiology 2010; 254: 460-468
- 29 Kim SY, Lee KH, Kim TY et al. Acute appendicitis in young adults: low- versus standard-radiation-dose contrast-enhanced abdominal CT for diagnosis. Radiology 2011; 260: 437-445
- 30 Seo H, Lee KH, Kim HJ et al. Diagnosis of acute appendicitis with sliding slab ray-sum interpretation of low-dose unenhanced CT and standard-dose i.v. contrast-enhanced CT scans. Am J Roentgenol 2009; 193: 96-105
- 31 Platon A, Jlassi H, Rutschmann OT et al. Evaluation of al low-dose CT protocol with oral contrast for assessment of acute appendicitis. Eur Radiol 2009; 19: 446-454
- 32 Dabir D, Fürst G, Blondin D. MRI in acute appendicitis in pregnancy. Fortschr Röntgenstr 2010; 182: 1010-1011
- 33 Oto A, Ernst RD, Ghulmiyyah LM et al. MR imaging in the triage of pregnant patients with acute abdominal and pelvic pain. Abdom imaging 2009; 34: 243-250
- 34 Nikolaidis P, Hammond N, Marko J et al. Incidence of visualization of the normal appendix on different MRI sequences. Emerg Radiol 2006; 12: 223-226
- 35 Heverhagen JT, Pfestroff K, Heverhagen AE et al. Diagnostic accuracy of magnetic resonance imaging: a prospective evaluation of patients with suspected appendicitis (diamond). J Magn Reson Imaging 2012; 35: 617-623
- 36 Cobben L, Groot I, Kingma L et al. A simple MRI protocol in patients with clinically suspected appendicitis: results in 138 patients and effect on outcome of appendectomy. Eur Radiol 2009; 19: 1175-1183
- 37 Incesu L, Coskun A, Selcuk MB et al. Acute appendicitis: MR imaging and sonographic correlation. Am J Roentgenol 1997; 168: 669-674
- 38 Fröhlich JM, Kubik-Huch RA. Röntgen-, MR- oder Ultraschallkontrastmittel während der Schwangerschaft oder Stillzeit: Was ist zu beachten?. Fortschr Röntgenstr 2013; 185: 13-25
- 39 Leeuwenburgh MM, Jensch S, Gratama JW et al. MRI features associated with acute appendicitis. Eur Radiol 2013; Epub ahead of print
- 40 Avcu S, Cetin FA, Arslan H et al. The value of diffusion-weighted imaging and apparent diffusion coefficient quantification in the diagnosis of perforated and nonperforated appendicitis. Diagn Interv Radiol 2013; 19: 106-110
- 41 Pedrosa I, Lafornara M, Pandharipande PV et al. Having acute appendicitis: effects of MR imaging on negative laparatomy rate and appendiceal perforation rate. Radiology 2009; 250: 749-757
- 42 van Randen A, Bipat S, Zwinderman AH et al. Acute appendicitis: meta-analysis of diagnostic performance of CT and graded compression US related to prevalence of disease. Radiology 2008; 249: 97-106
- 43 Leeuwenburgh MM, Wiarda BM, Wiezer MJ et al. Comparison of imaging strategies with conditional contrast-enhanced CT and unenhanced MR imaging in patients suspected of having appendicitis: a multicenter diagnostic performance study. Radiology 2013; 268: 135-143